
Abstract
Approximately 10 million individuals in the United States have osteoporosis and 44 million have low bone mineral density which puts them at risk for bone breaks. This presents a large burden on our health care system since about one-quarter of hip fracture patients never regain full function, need nursing care, and, for those over age 50, 24% die within one year. Oral bisphosphonates are often used as first-line therapy for the treatment of osteoporosis; however, patients frequently experience significant side effects. In addition, bisphosphonates inhibit bone loss by initiating apoptosis in osteoclasts that remove old bone, thus allowing old bone to accumulate and slowing the activity of osteoblasts that create new bone, thereby affecting bone quality. As an alternative, a bone-friendly lifestyle, including calcium and vitamin D consumption, exercise, smoking cessation, and a decrease in alcohol intake, may reduce bone loss. This case report describes lifestyle changes that included diet and exercise that increased bone mineral density in two years in a post-menopausal woman with no negative side effects.
“An integrated lifestyle modification plan that included diet and exercise led to a gain in BMD.”
Introduction
According to the National Institutes of Health, the most common risk factors for osteoporosis are gender, age, body size, ethnicity, and family history. 1 Individuals often lose 0.5 to 1% of their bone mineral density per year after the age of 50.2,3 This increases for post-menopausal women to 1 to 3% bone loss for five to 10 years and then resumes at the lower rate. 4 About half of all American adults 50+ years old have osteopenia or osteoporosis, leading to an increased risk of hip and vertebral fractures. 5 Osteopenia is bone mineral density (BMD) that is 1.1 to 2.4 standard deviations (SD) and osteoporosis is > 2.5 SD below the mean that of a young adult BMD. 6 Bisphosphonates are often prescribed for the treatment of osteoporosis because they may reduce the risk of fracture for some patients. But bisphosphonates have many toxicities that make them less appealing to patients, including reflux, esophagitis, esophageal ulcers and cancer, diarrhea, abdominal pain, musculoskeletal pain, impaired kidney function, and osteonecrosis and avascular necrosis of the jaw. 6 Chronic use of bisphosphonates allows old bone to accumulate, slows the activity of osteoblasts that create new bone, and potentially compromises bone quality. 7
Lifestyle changes that include nutrition and exercise may slow the loss of BMD.8-10 Eating an anti-inflammatory Mediterranean-style whole-foods-based diet and eliminating highly processed food is beneficial for reducing the risk of many chronic diseases. 11 The recommendations include adding several servings of vegetables and some fruits, omega-3 fatty acids (from fatty fish, seeds, and nuts), and enough protein to maintain or increase muscle mass. 11 Dietary sources of calcium such as yogurt, kefir, kale, bok choy, sardines with bones, bone broth, and nettle tea are beneficial.12-14 Some calcium-rich foods high in oxalic acid, such as spinach, Swiss chard, beets, almonds, and rhubarb, may prevent calcium from being absorbed by the body and therefore should be decreased in the diet.12-14 Contrary to earlier advice, protein-rich diets are beneficial for BMD.15,16 Additionally, nutrients that are difficult to get from dietary sources, like vitamin D-3, may be taken as supplements.12-14
The International Osteoporosis Foundation and the Bone Health and Osteoporosis Foundation also recommend weight-bearing exercises to improve bone health. Low-impact activities, such as walking, may be beneficial for maintaining BMD. 17 In contrast, high-impact osteogenic loading activities, such as tennis and jumping, stress the bones and thus potentially accelerate bone-building.18-23 Another way to stress bones is wearing a weight belt or vest while doing low-impact activities. 24 In addition, strength training with weights and isometric exercises will build muscle and improve BMD.21,22,25,26 Tai chi, qigong, and yoga are good for balance and may reduce the risk of falls, while core-training exercises like Pilates help with balance.21,22
This case report highlights a personalized nutrition and exercise approach that increased BMD in a primary osteoporosis post-menopausal female in two years.
Case Narrative
A 56-year-old physically active post-menopausal female, who went through menopause at the age of 50 and did not take hormone replacement therapy, was diagnosed with osteopenia, based on data from a dual-energy X-ray absorptiometry (DXA) scan in 2011 (Figure 1Longitudinal DXA Scans). In 2013, a DXA scan indicated that the spine L1-L4, total hip left and total hip right scores declined further (Figure 1 Longitudinal DXA Scans). In 2013, the patient made several lifestyle changes to reduce the risk of further bone loss. Changes in diet included the consumption of more calcium-rich vegetables and snacks (Table 1). Pre-diagnosis, she was active but lacked a consistent exercise regimen. Post-diagnosis, she developed a workout routine including strength training exercises (two times per week), sculpting exercises (two to three times per week), and aerobic exercise for 40 to 60 minutes (min) per day (one time per week). Strength training exercises included kettlebells and dumbbells, and TRX suspension training. Specifically, strength training included upper and lower multi-joint exercises such as lunges, squats, rows, biceps curls, tricep extensions, and overhead and chest presses. Sculpting exercises included bodyweight exercises such as ballet, barre, Pilates, and yoga. Cardiovascular exercises included biking, boxing, canoeing, cross-country skiing, dancing, elliptical, hiking, jogging, kayaking, and table tennis. Longitudinal DXA Scans. Results of four bone density (DXA) measurements performed on the same GE Medical Systems Lunar Prodigy Advance. The top and bottom red dashed lines represent the cut-off values for osteopenia (top) and osteoporosis (bottom). X-axis is the date of the DXA scan (year-monthday) and Y-axis is the T-score. Lifestyle Changes. The Main Changes in Nutrition Comparing Pre- and Post-osteoporosis Diagnosis Were in the Breakfast and Snack Meals. The Two-Serving Size for Each Component of the Smoothie is Provided in the Table. The Serving Size of the Snacks, Lunch, and Dinner Foods Varied Daily and Therefore it is not Included in the Table. Heavier Weights Were Used During Strength Training Post-Osteoporosis Diagnosis, and a Weighted Vest was Worn When Strength Training and Sculpting. Italic Text Indicates Components Changed. Indicates Eliminated bIndicates Added Abbreviations: C, cup; IU, International Units; lbs, Pounds; mcg, Micrograms; mg, Milligrams; min, Minutes tbs, Tablespoon.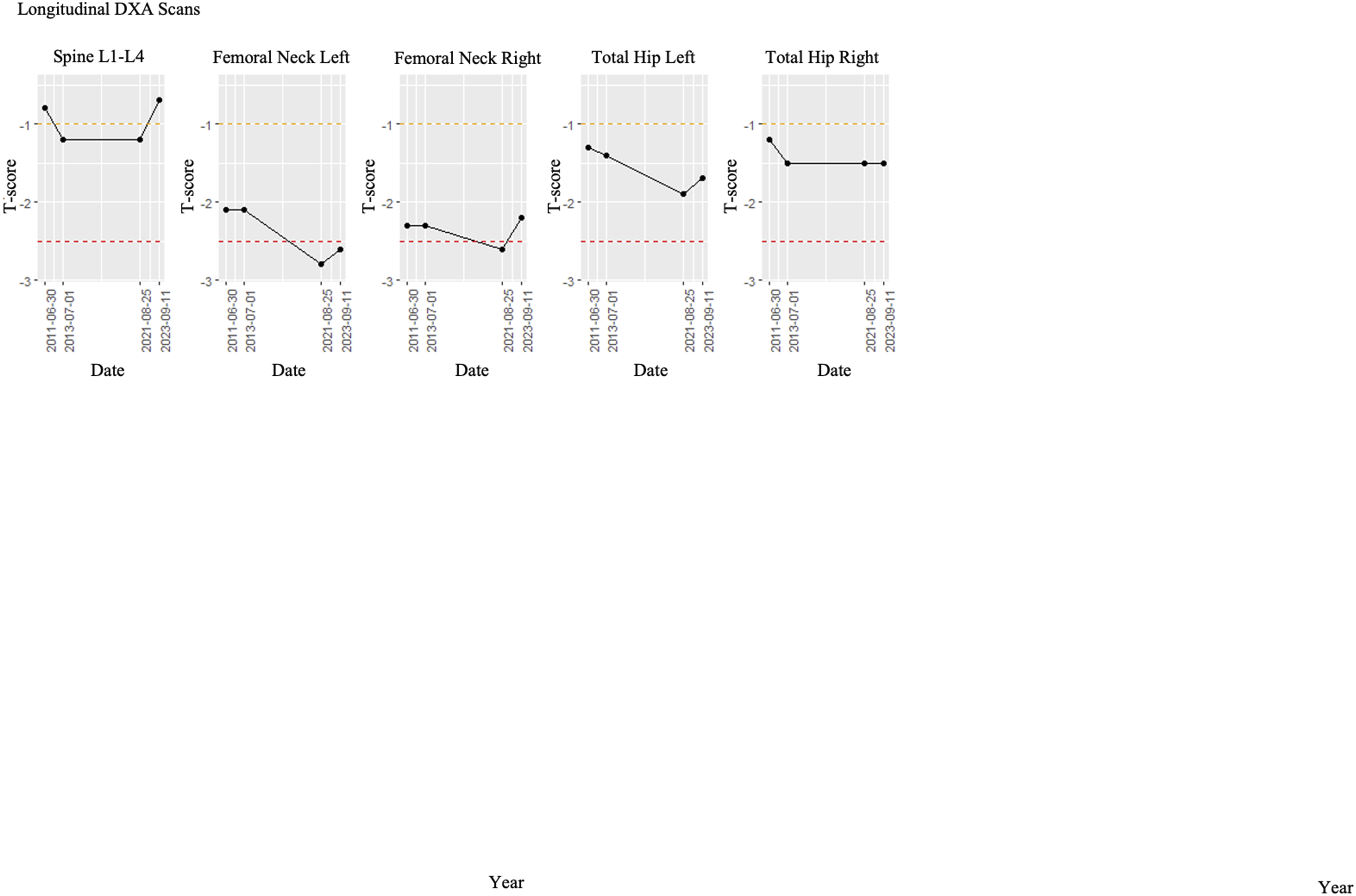
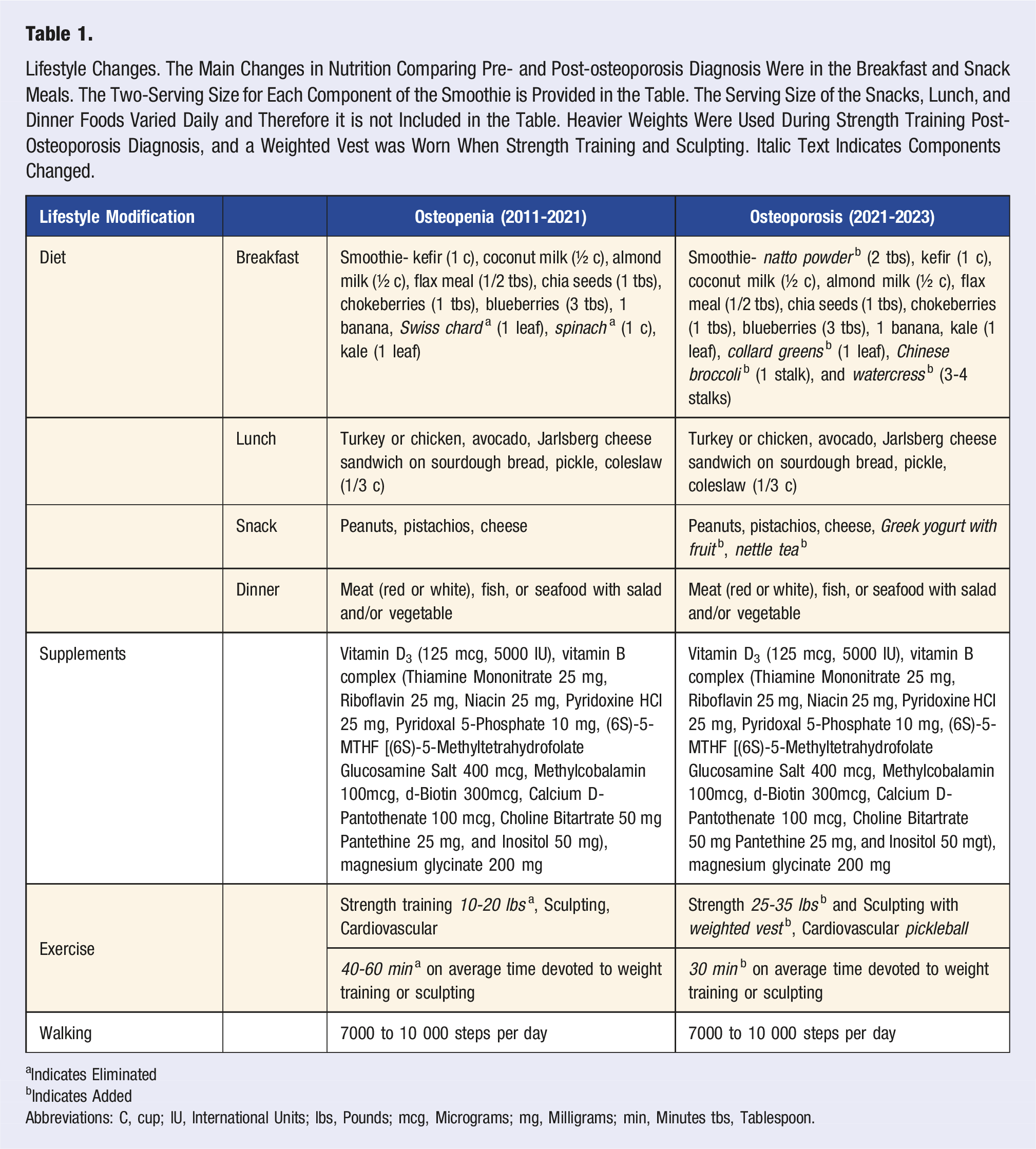
Despite the efforts, a DXA scan in 2021 revealed the 66-year-old post-menopausal patient had progressed to osteoporosis in the right and left femoral neck (Figure 1 Longitudinal DXA Scans). The patient decided not to take medication for her bone loss and instead opted for additional lifestyle modifications to prevent further loss of BMD. A reassessment of the patient’s diet revealed a high intake of foods containing oxalic acid. The main modification she made to her diet was changing the breakfast smoothie. Vegetables high in oxalic acid (spinach and Swiss chard) were replaced with calcium-rich vegetables low in oxalic acid including kale, collard greens, Chinese broccoli, and watercress (Table 1). In addition, natto powder, rich in vitamin K2, was added to the smoothie and she began drinking nettle tea regularly.
In addition to the dietary changes, the patient continued her exercise program with a few noteworthy changes. She began wearing a weighted vest (from three to six pounds (lb)) for 30 min, five days per week, while strength training (30 min, 3 days per week), toning (30 min, 2 days per week), and taking tai chi (60 min, 1 day per week) and yoga (30 min, 1 day per week) classes. In addition, the patient slowly increased the resistance of the weights used in strength training from 10-20 to 25-35 lbs. Additionally, the patient increased aerobic activity, playing pickleball (60 min, 3 to 5 days per week) in 2023.
The most recent 2023 DXA scan revealed that all T-score values improved on the 2023 DXA scan except one which remained the same without further deterioration. The patient still has osteoporosis according to the lowest calculated T-score in the femoral neck left (Figure 1 Longitudinal DXA Scans).
Discussion
The present case describes a reversal of BMD loss in a patient diagnosed with osteoporosis. An integrated lifestyle modification plan that included diet and exercise led to a gain in BMD. The main change in diet included replacing high oxalic acid calcium-rich foods with low oxalic acid calcium-rich foods. Oxalic acid found in some leafy plants can bind with calcium to form insoluble oxalate. Thus, oxalic acid is considered an antinutrient that reduces calcium absorption. 27 By removing antinutrients from the diet, the patient improved calcium absorption. 27 Another significant change to the diet was the addition of natto powder to the breakfast smoothie. Natto is a fermented soybean dish that is rich in proteins, cellulose, calcium, iron, potassium, and vitamins B2, B6, B12, E and K, which is often eaten in Japan and China. 28 Natto is a good source of vitamin K2, which contains the menaquinones MK4 and MK7. 28 These menaquinones are needed to protect bone sheath flexibility, deposit calcium in the bone matrix, and remove calcium from the arteries and joints.13,28 In addition, the patient also started drinking nettle tea regularly. One cup of tea contains 125 milligrams (mg) of calcium, 75 mg of magnesium, 450 international units (iu) of vitamin A, and 4.1 gram (g) of protein.13,29 Nettle tea also provides other bone-strengthening ingredients including iron, vitamins B, C, A, D, and K, trace minerals, potassium, zinc, copper, sulfur, and boron.13,29 Caution is advised when drinking nettle tea as it may cause sweating, fluid retention, mild gastrointestinal disturbances, and diarrhea. 30 While there are no known contraindications or drug interactions with nettle tea., further studies are needed to determine if it may interact with antiplatelet, anticoagulant, high blood pressure, diuretic, diabetes, lithium, and nonsteroidal anti-inflammatory drugs. 30
The patient exercises daily including strength training, toning, balance, and aerobics. After the diagnosis of osteoporosis, she began wearing a weighted vest while exercising five days per week while weight lifting, and taking barre or tai chi classes. During strength training, she slowly increased the weight from 10-20 to 25-35 lbs. Barre and tai chi classes are promoted for their toning and balance benefits, respectively. The weighted vest provided an osteogenic load to these classes. Another major change she made during this period was playing pickleball. A review of 22 studies that examined the effect of tennis on bone health revealed that bone mineral content and BMD were greater in the hip and lumbar spine regions of tennis players compared to nonplayers. 31 In both tennis and pickleball, many rapid accelerations and decelerations put an osteogenic load on bones; therefore, it is likely that the observations made on bone health for tennis may apply to pickleball players.
This case report highlights simple lifestyle changes that are beneficial for increasing BMD in a patient with osteoporosis. The integrated multi-modal approach included dietary and exercise modifications that reversed bone loss in two years. There were no negative side effects associated with the management plan. Previous studies suggested that diet and exercise may improve BMD, although no single study has examined incorporating both lifestyle changes in patients with osteoporosis. Due to the limited number of case-control studies addressing lifestyle modifications that may be used to build BMD in patients with osteopenia and osteoporosis, this case report provides a valuable approach that health care providers and nutritionists can use for clinical application.
Limitations
When using a multi-modal clinical approach to treat osteoporosis, it is not possible to conclude if all the interventions were essential for improving BMD. Modifying the diet or the exercise plan alone may have increased BMD. A case report using only diet or exercise as an intervention would be useful to assess the effectiveness of each therapy properly. Additionally, this case report may describe a causal relationship between nutrition, exercise, and BMD; however, it does not exclude the possibility of a chance association between these lifestyle changes and the observed benefits. Finally, the results from a single case study may not represent a larger genetically diverse population. Future clinical studies that involve a large number of participants would be warranted to better evaluate the role of nutrition and exercise in increasing BMD.
Conclusion
This case demonstrates the safe and effective use of a personalized multi-modal integrated lifestyle approach to increasing BMD in a post-menopausal woman in two years. The approach included diet modifications that enriched for nutrients needed to build BMD and eliminated high oxalic acid-rich foods. In addition, an exercise plan that included a weighted vest that increased the osteogenic load on bones was implemented. The patient had no problems with implementing and remaining compliant with the plan.
There are very few case-control studies addressing lifestyle methods for building BMD in patients with osteopenia and osteoporosis. Animal and observational human studies for increasing bone mass are the basis of the lifestyle plan implemented in this case report. The personalized program described in this report provides a novel simple approach for treating patients with no negative clinical outcomes. More studies addressing this issue would be useful for providing opportunities to patients who may choose not to take the currently available drugs for treating osteoporosis.
Footnotes
Acknowledgments
J.A.P. is a Professor of Cellular and Molecular Pharmacology at Chicago Medical School, Rosalind Franklin University of Medicine and Science. N.K. is a Senior Biostatistician and Data Resource Core Lead of the Michael Reese Foundation Center for Health Equity Research, Rosalind Franklin University of Medicine and Science.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.