
Abstract
We pilot tested a multiple health behavior change (MHBC) intervention to improve breastfeeding rates, healthy eating/active living, and depression prevention among pregnant and parenting adolescent mothers. We also assessed utility of the MHBC mHealth approach by examining health behavior coaction and intervention acceptability. We used a longitudinal randomized controlled trial to compare the tablet-delivered momHealth to a control condition (usual care). Delivered between 32 weeks of pregnancy and one month postpartum, momHealth included nine multi-media education modules, simultaneous daily educational text messaging, and weekly videoconferences for individual and group support. Main outcomes included “any” and “exclusive” breastfeeding initiation and continuation for 5 weeks and 3 months postpartum; number of fruit and vegetable servings; minutes of moderate/vigorous physical activity per day; and depressive symptoms. Sixty-two adolescents aged 16–19 having their first baby were randomized. Compared to Control, more momHealth participants were still breastfeeding at 5 weeks (chi-square = 3.91, df = 1, P = .048). Mothers who breastfed for 3 months were more likely to eat adequate daily fruits/vegetables. Participants positively rated the intervention. momHealth positively affected early breastfeeding continuation and trended toward positive outcomes in healthy living and depressive symptoms. A fully powered trial is planned to test the intervention more effectively.
Keywords
“The Multiple Health Behavior Change (MHBC) paradigm offers a unique approach to intervene with childbearing adolescents by promoting change in multiple health behaviors simultaneously”
Teenage pregnancy in the United States has declined greatly over the past two decades but remains a significant public health problem. 1 In 2016, 209,809 babies were born to mothers 15–19 years of age, for a live birth rate of 20.3 per 1000 women in this age group. 2 Multiple health issues impact pregnant and parenting adolescent mothers; they are less likely to initiate breastfeeding than older mothers, 3 more likely to begin formula supplements in the hospital, and have lower rates of exclusive breastfeeding (EBF; human milk only), 3 as well as shorter breastfeeding duration.4,5 Adolescent mothers tend toward excess pregnancy weight gain 6 and postpartum weight retention,7-9 engage in less healthy eating10-12 and physical activity after giving birth, 13 and are at higher risk for postpartum depression.14,15 These problems occur for adolescent mothers around the world10-12 and are related to barriers such as socioeconomic status, 16 stress, motivation, and convenience. 17
The Multiple Health Behavior Change (MHBC) paradigm offers a unique approach to intervene with childbearing adolescents by promoting change in multiple health behaviors simultaneously.18,19 Evidence has supported the potential for the MHBC approach to have a greater impact on health than single-behavior interventions. A recent meta-analysis of 150 MHBC intervention studies demonstrated that these interventions were more effective than those addressing just one health behavior, or those targeting 4 or more health behaviors. 20 Furthermore, influencing three key behaviors through simultaneous interventions offers the potential for synergistic effects. Additionally, by maximizing limited resources, MHBC interventions capitalize upon behavioral change momentum 19 and reinforce shared behavior change strategies.
Also important to this area of study and target population are mobile technologies to support the achievement of health objectives (ie, mHealth), which allow delivery of interventions, either synchronously or asynchronously, in an engaging, timely manner. Teen access to smartphones is near ubiquitous, with most teens (84%) owning smartphones 21 ; and the majority of adolescents like to receive interventions via technology. 22 The mHealth approach uses low-cost mobile technology to increase support opportunities to underserved youth at home, enhancing research retention, 23 and uses evidence that adolescents prefer in-home research involvement.24,25
Despite the significance of adolescent childbearing and the behavioral health issues noted, no studies have attempted to address multiple health issues among adolescent mothers. 26 Thus, we designed an mHealth MHBC intervention called momHealth, assessed feasibility of its components, 27 and in the current study examined the initial indications of effectiveness of this approach.
Aims and Hypotheses
The primary aim of this pilot study was to compare momHealth to a usual care group (Control) in pregnant/parenting adolescents in the areas of breastfeeding, healthy eating/active living, and depression prevention. We hypothesized momHealth would result in 1. higher rates of any and exclusive breastfeeding at post-birth hospital discharge, 5 weeks, and 3 months postpartum and significantly longer duration of breastfeeding to 3 months; 2. greater number of fruits/vegetable servings per day and more minutes of moderate/vigorous physical activity per day at 5 weeks and 3 months postpartum; and 3. fewer postpartum depressive symptoms at 5 weeks and 3 months postpartum.
A second aim was to assess the utility of the MHBC approach through examining health behavior coaction, 28 that is, would individuals who succeed on one behavior be more likely to succeed on one or both other behaviors. Third, within the momHealth group, we examined the acceptability of the intervention, participation rate, perceived technology ease of use, and program satisfaction.
Methods
This was a pilot longitudinal randomized controlled trial with rolling recruitment. Individual participant activities took place over a 20-week period commencing around 32 weeks of pregnancy. In-home data collection visits were conducted at 32 weeks (Baseline), 5 weeks postpartum (Postpartum), and 3 months postpartum (Follow-Up). An intent-to-treat (ITT) analysis strategy was used with the participants who consented, completed baseline measures, and were randomized. Participant recruitment, enrollment, and activities took place between December 2017 and May 2020.
Participants
Participants were pregnant English-speaking females between age 15 and 19 years—11 months; screened at 27–31 weeks of pregnancy; experiencing a low-risk pregnancy; giving birth to their first child; and intending to parent the newborn. Exclusion criteria included multiple gestation pregnancy; development of pregnancy complications; and/or other severe health concerns of mother, fetus, or newborn. As a depression prevention program, women with active untreated mental health conditions were excluded (eg, clinical affective, substance use, or anxiety disorders). A clinical interview based on the DSM-5 was used for screening participants, 29 and those with a positive screen were referred to their health care provider.
Setting
Adolescents were recruited from local and regional obstetric and family medicine clinics and community or school-based health service settings. Recruitment strategies were active (clinic recruitment and phone calls) and passive (brochures distributed to local clinics and high schools). Research team members included nurses, psychologists, dietitians, and trainees in these areas, all of whom were trained in study procedures. Relevant institutional review boards approved the protocol.
Enrollment Procedures, Informed Consent, and Randomization
Informed consent took place at the recruitment site or the participant’s home during the baseline data collection; no parental assent was required. Following consent and completion of baseline measures, randomization was conducted by the study statistician independent of the study staff, with equal numbers assigned to each group.
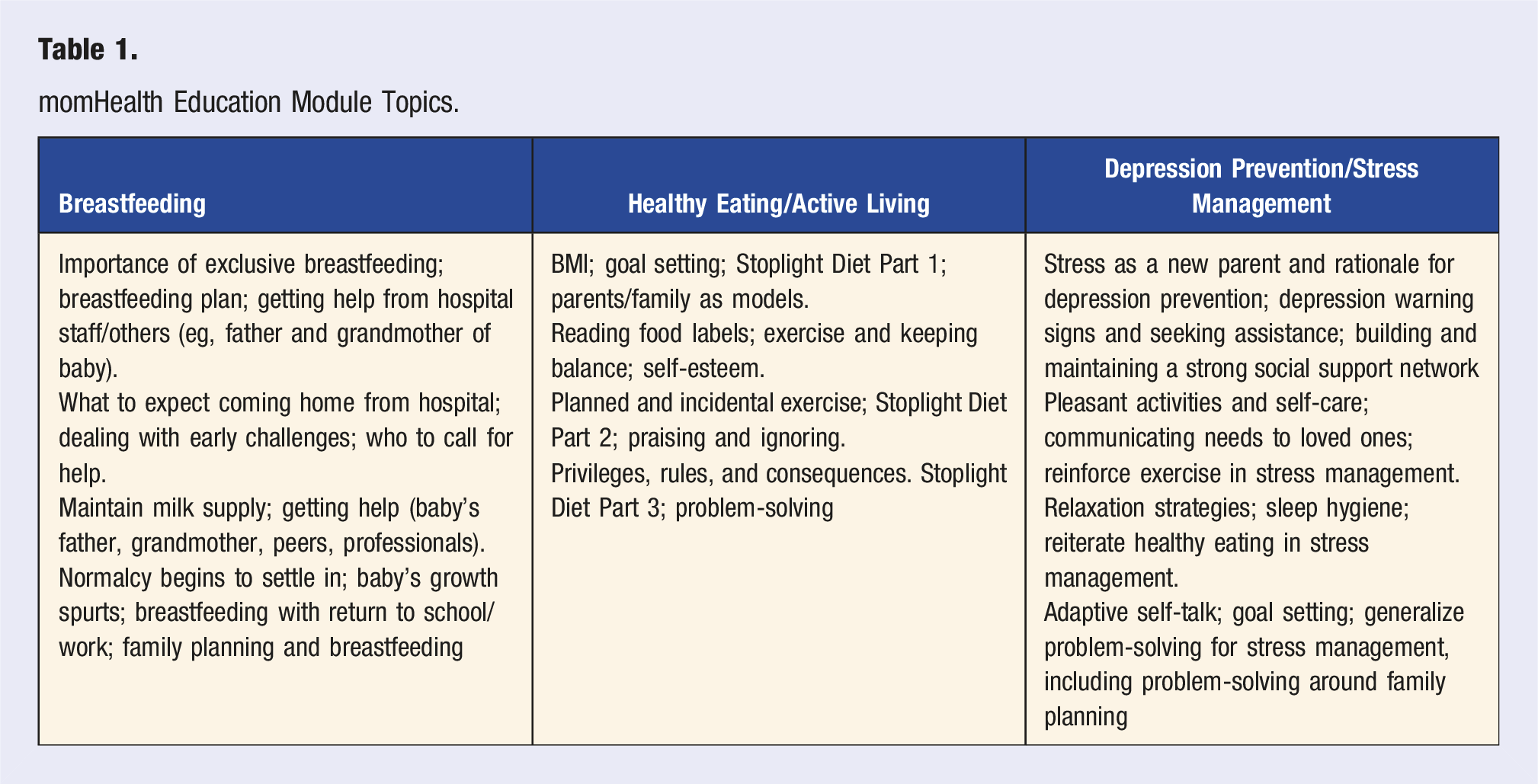
momHealth Intervention
momHealth Education Module Topics.
Control Group
Control group participants received standard health care from their prenatal providers during clinic visits on healthy lifestyle, breastfeeding and postpartum lactation support through hospital “warm lines” and pediatric providers. Programs available in our urban setting, outside of typical obstetrical care, included a school-based teen pregnancy program at two local high schools and a health department program. Provider feedback indicated high drop-out rates and infrequent attendance for most participants in these supplemental programs. The control participants did not receive a study-issued iPad and were given the choice to complete study surveys via their personal device or telephone.
Study Measures
momHealth Measures Timeline.
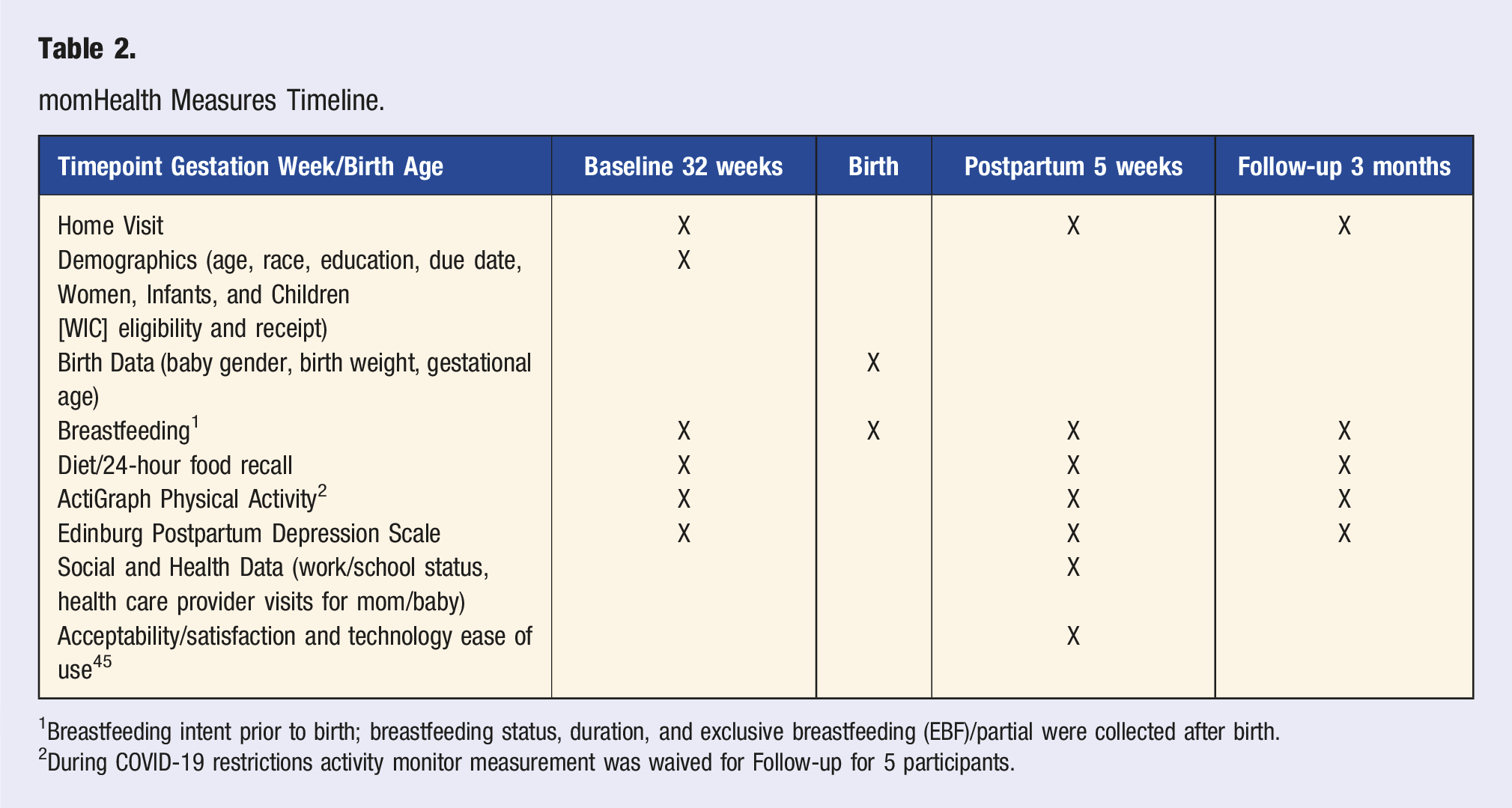
1Breastfeeding intent prior to birth; breastfeeding status, duration, and exclusive breastfeeding (EBF)/partial were collected after birth.
2During COVID-19 restrictions activity monitor measurement was waived for Follow-up for 5 participants.
Breastfeeding Outcomes
Intention to breastfeed and intention to exclusively breastfeed were collected using a 5-point rating scale at baseline. Following birth, each participant reported if she initiated breastfeeding and if she was EBF vs partial breastfeeding (human milk plus infant formula) in hospital and at home each week.
Dietary Outcomes
Dietary intake was assessed with the Automated Self-Administered 24-hour Recall™ (ASA24™), versions 2016 and 2020. 36 Diet recalls with caloric consumption below 912 or above 3971 calories/day required the participant to repeat the recall for each out-of-range day. 37 If unable to complete 3 days independently within the valid range, the diet recall was conducted by telephone and data were entered into ASA24 system by study staff. The primary outcome was number of servings of fruits/vegetables per day.
Physical Activity
Physical activity was measured using ActiGraph Physical Activity Monitors (ActiGraph LLC, Pensacola, FL). These reliable, small, lightweight accelerometers were worn on an adjustable belt over the non-dominant hip; each monitor was programmed for start time and data collection intervals (15 seconds), and data were downloaded for analysis. Participants wore their monitor for 7 consecutive days each timepoint. For analyses, a “valid” data point was defined as at least 10 hours of wear time in 24 hours for a minimum of 4 days. 38 Participants not meeting criteria were asked to repeat the monitoring. Primary outcome was minutes of moderate to vigorous physical activity (MVPA) per day.
Depressive Symptoms Outcome
The Edinburgh Postnatal Depression Scale (EPDS) is a widely used self-report 10-item questionnaire for postpartum depression with established psychometric properties 39 ; it is validated for use in identifying both prenatal and postpartum depression in adolescents.40-42 Each question response is coded from 0 to 3 and the maximum total score is 30. The recommended cut score of 10 or greater indicates a major depressive disorder with sensitivity of >90% and specificity >80%. 41 Internal consistency reliability for this sample was .765 at Baseline.
Secondary and Tertiary Outcome Measures
We assessed the utility of the MHBC approach by examining health behavior coaction; behavior success criteria were used and counted in each group. Acceptability and satisfaction were evaluated in the momHealth group with items adapted from Mauriello et al.’s 43 MHBC study of adult pregnant women. Items focused on most and least useful program components, ease of understanding content, technology ease of use, time burden, components’ impact on learning, perceived support, program aesthetics and enjoyment, learning impact, potential to change health and behavior, and if they “would recommend” the program. The item responses for 15 items were on a 5-point rating scale of agreement-disagreement; Cronbach’s alpha reliability was .779 (n=19).
Data Collection
Study data were collected and managed using HIPAA-compliant REDCapTM.34,35 All data were de-identified and downloaded to IBM SPSS Statistics, version 26 and SAS, version 9.4 for analysis. Prior to data analysis, initial equivalence across groups was evaluated on pre-intervention variables. For analyses of intervention group data, dose and fidelity (ie, completion of intervention components over the past 7 days) were used as covariates, if appropriate.
Sample Size
Our target sample size was 25 per group. Power analyses were conducted using G*Power and Optimal Design. For differences in means at Postpartum and Follow-Up timepoints when no baseline data were available, that is, breastfeeding, a total sample size of 50 would ensure .80 power to detect between-group differences equivalent to a standardized effect size of d =.71. For outcomes with multiple timepoints, we estimated .80 power to detect medium standardized effect sizes equivalent to d= .48. To assess the utility of the MHBC approach and behavior coaction, we had .80 power to detect an effect size of w =.77 with 25 participants.
Data Analysis
Four different types of outcomes were analyzed. The first was single timepoint differences between groups on continuous outcomes (eg, duration of breastfeeding), which were analyzed using t-tests. For between-group differences in binary outcomes (eg, exclusive breastfeeding at 3 months), we used Fisher’s exact test. Predictors, such as breastfeeding intention, were examined at baseline, to identify any group differences. For continuous variables with data from multiple timepoints, we used multilevel modeling in SAS Proc Mixed. For questions where binary outcomes were examined with the use of multiple timepoints, SAS Proc Glimmix was used. For all models, we examined variables to account for group differences. Full Information Maximum Likelihood Estimation (FIML) was used for the repeated measures models to allow all available data to be used. FIML is equivalent or superior to multiple imputation for multilevel models like those proposed. Fisher’s exact tests were used to assess the MHBC approach and behavior coaction. We assessed if individuals who were successful on one behavior were more likely to be successful on one or both other behaviors. “Success” was defined as exclusive breastfeeding at 3 months, 5 or more fruit/vegetable servings per day, getting 45 or more minutes of MVPA per day, and EPDS (depressive symptoms) scores lower than 10.
Results
Participants
Of the 159 pregnant teens assessed for eligibility, 97 were excluded; 17 did not meet inclusion criteria, 64 declined to participate, and 16 consented to take part but eventually were not randomized due to decision not to participate or inability to schedule or complete baseline data collection (Figure 1). Sixty-two adolescents were randomized and allocated to the momHealth Intervention (n=31) and Control (n = 31) groups. Attrition during the follow-up period amounted to 9 (29%) in Intervention and 7 (22.5%) in Control, or total of 16 across groups (25.8%). CONSORT Flow Diagram.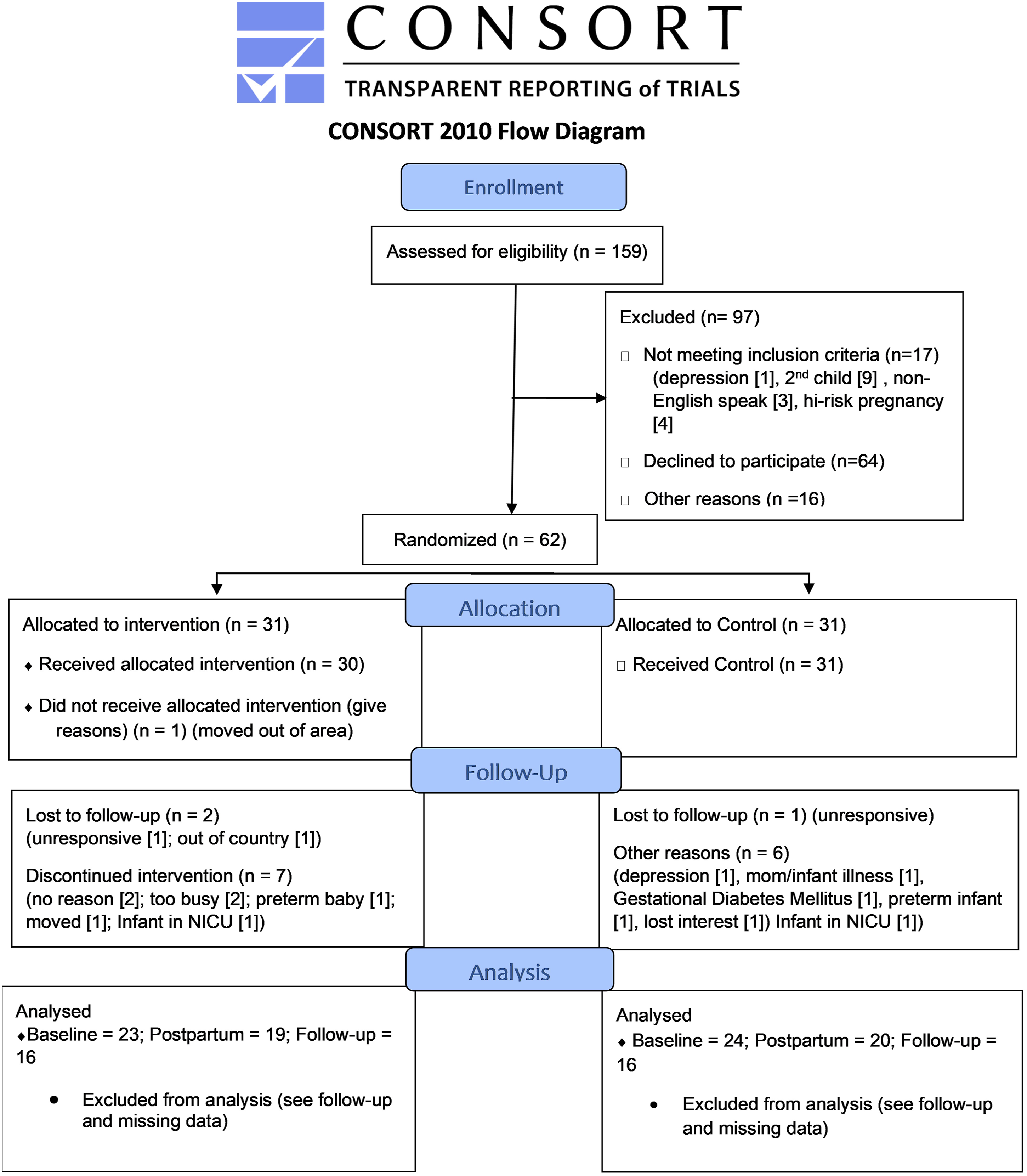
Participant Characteristics (N = 62).
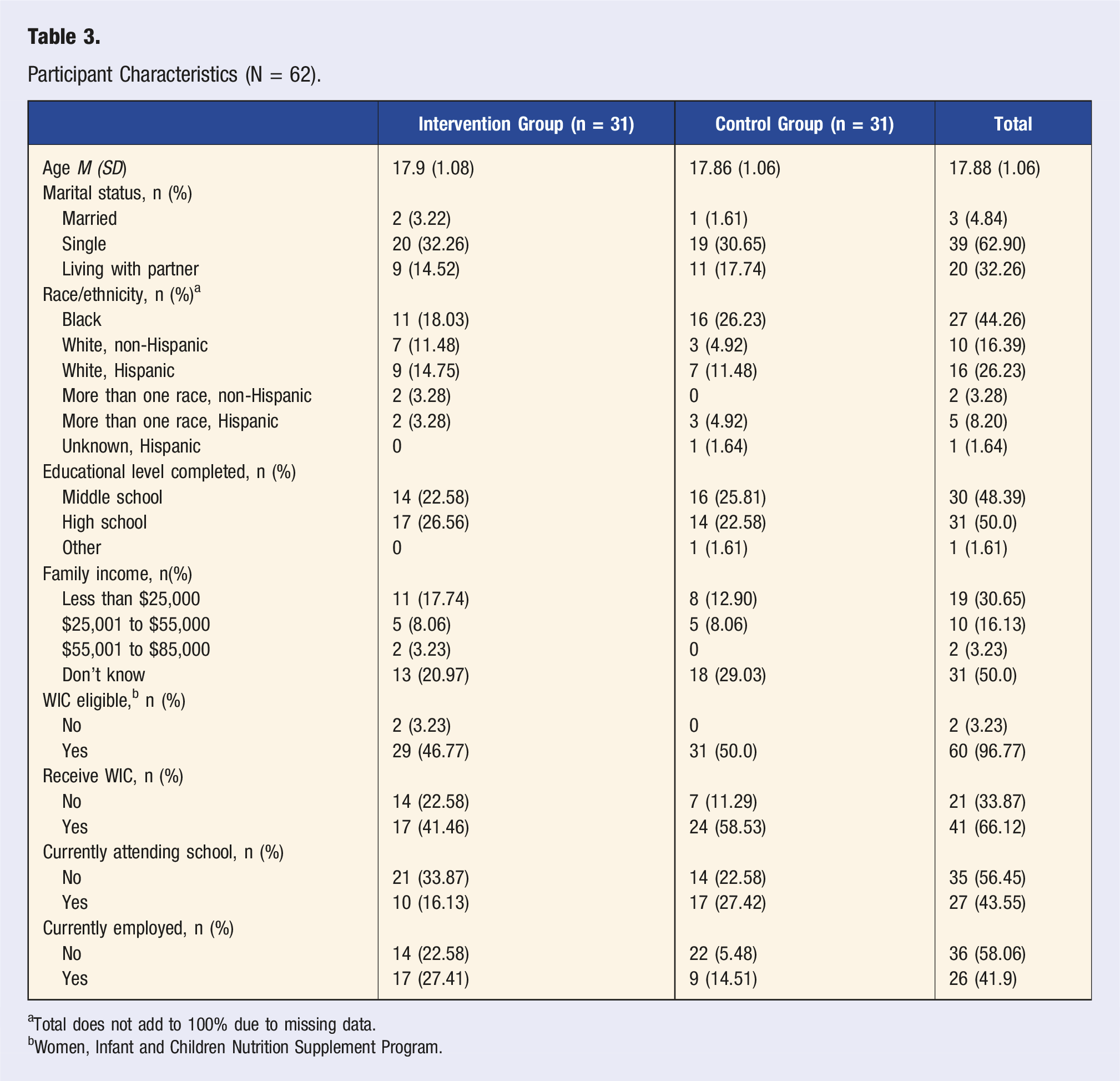
aTotal does not add to 100% due to missing data.
bWomen, Infant and Children Nutrition Supplement Program.
Breastfeeding Outcomes
Outcome Descriptive Data.
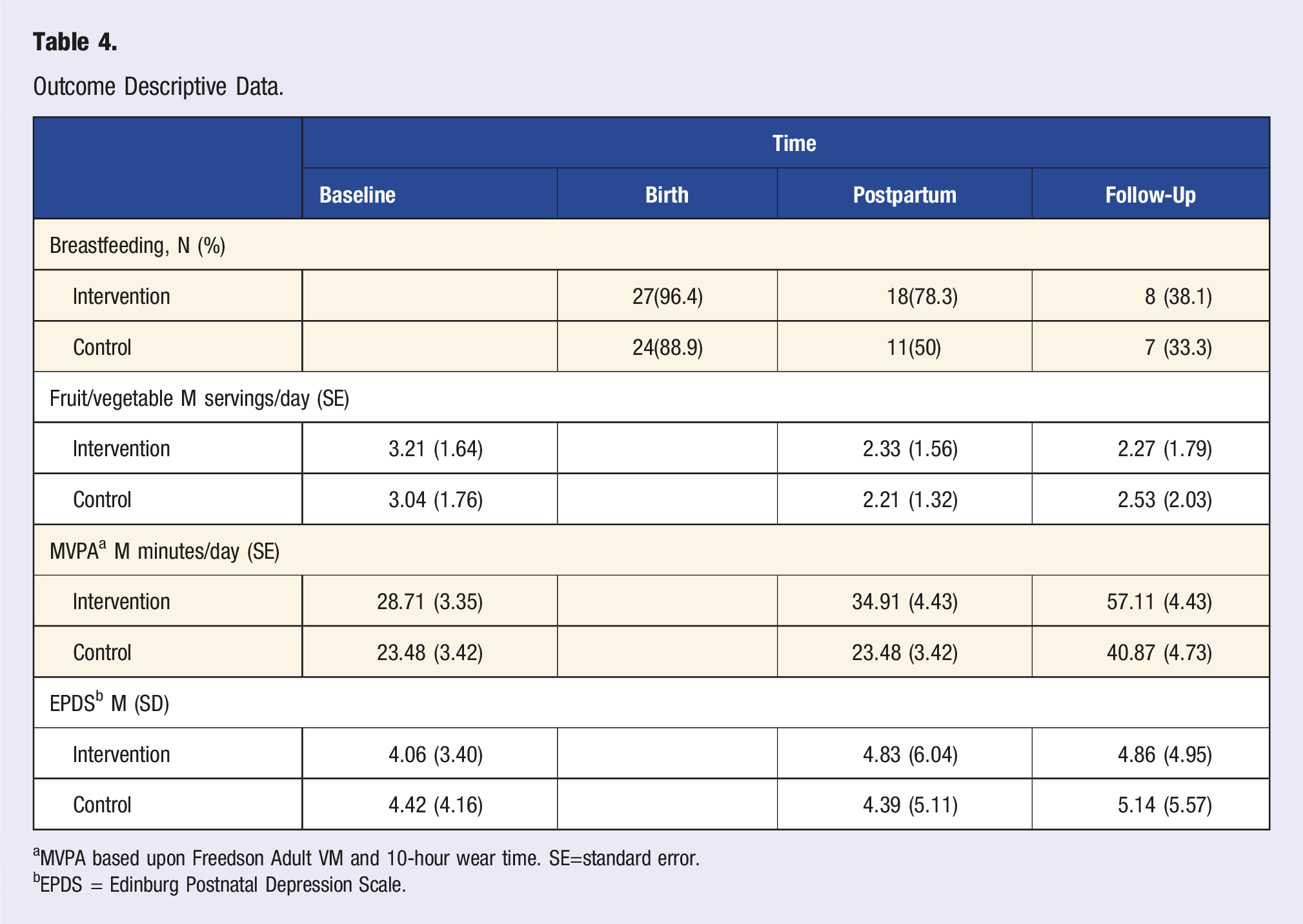
aMVPA based upon Freedson Adult VM and 10-hour wear time. SE=standard error.
bEPDS = Edinburg Postnatal Depression Scale.
Multilevel Models by Outcome of Interest.
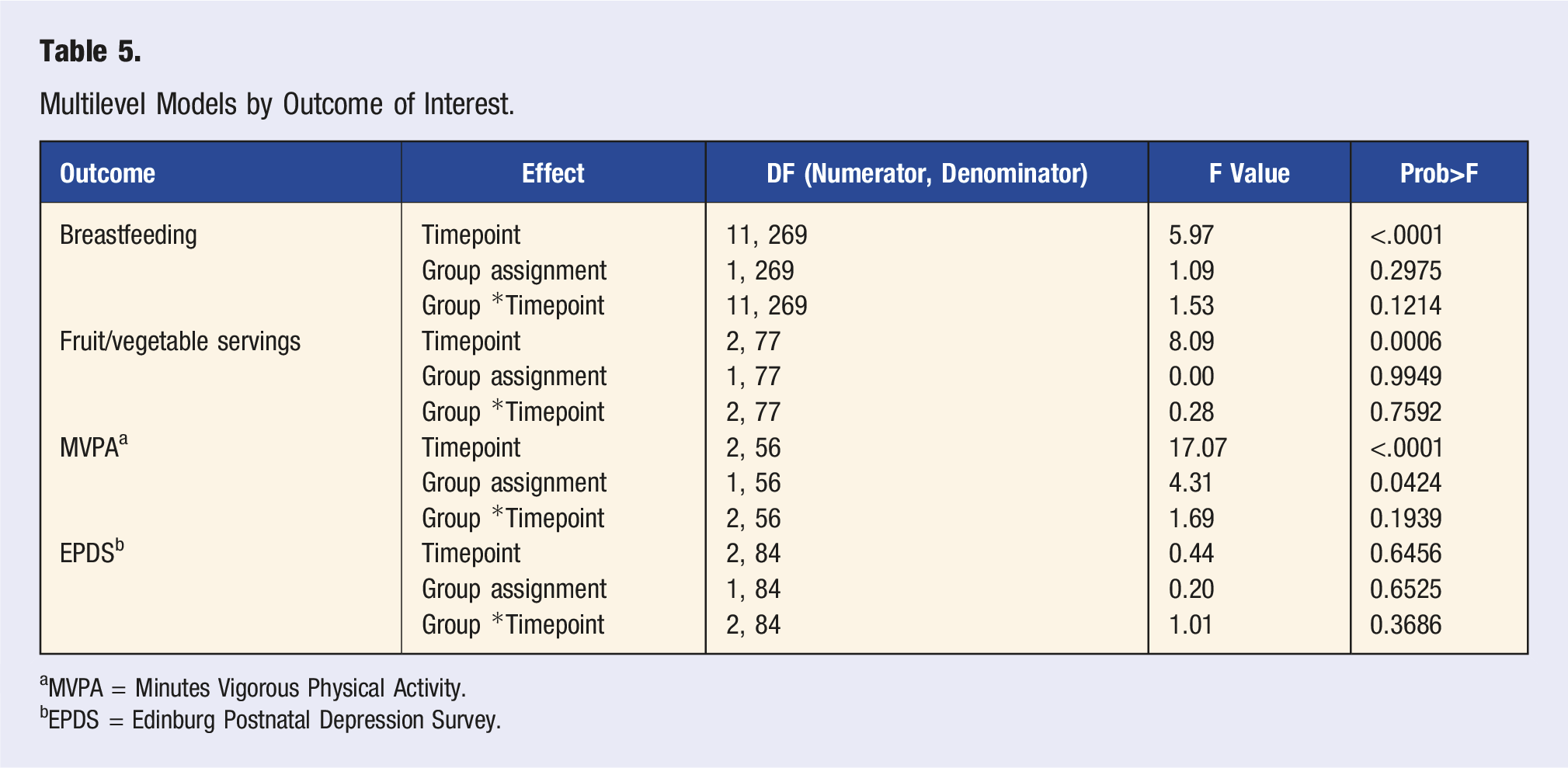
aMVPA = Minutes Vigorous Physical Activity.
bEPDS = Edinburg Postnatal Depression Survey.
Diet and Physical Activity Outcomes
Servings/day of fruits/vegetables were highest at the baseline visit and decreased across time (P < .001), with no significant differences between the groups (P > .05), nor significant interactions between group and time (P > .05; Table 5). Minutes of MVPA per day were higher in the intervention group (P = .04) and increased across time (P < .001), but there was no interaction between time and group (P > .05). A larger proportion of those in the Intervention group met the guideline of 45 minutes per day of MVPA (M = 26.67%) compared to those in the Control group (M = 16.13%), but this difference was not statistically significant.
Depressive Symptoms Outcome
EPDS scores were low across the two groups and there were no significant differences between groups, or across time (P > .05), and no interaction between group and time (P > .05; Tables 4 and 5). There was no difference in number of participants who were successful in maintaining low depressive symptoms across the two groups.
Secondary Outcomes
To assess the utility of the MHBC approach, behavior success was measured in each group and compared. Participants were successful in 0 to 4 areas, with the most common number of successes for those in momHealth being 2 behaviors, and in the Control, 1 behavior. The mean number of successes for those in the momHealth group was 1.26, while in the Control group, it was 1.00 and not significant (F(1,60) = 1, P = .321), although the Cohen’s d indicated a small effect (d = .25). To further assess behavior coaction, correlations were calculated between all major behaviors (any breastfeeding, fruit/vegetable consumption [5/day], physical activity [45 min/day], and lower depressive symptom scores) within momHealth group. The only significant correlation was between fruits/vegetable consumption and continued breastfeeding at Follow-Up (r = .34, P = .03). This was confirmed by X2 Fisher’s exact tests, which were nonsignificant for all combinations except breastfeeding at 3 months and total fruit and vegetables greater than 5 (X2=4.848, P=.047).
Tertiary Outcomes
Program Evaluation Items and Ratings (n = 23).
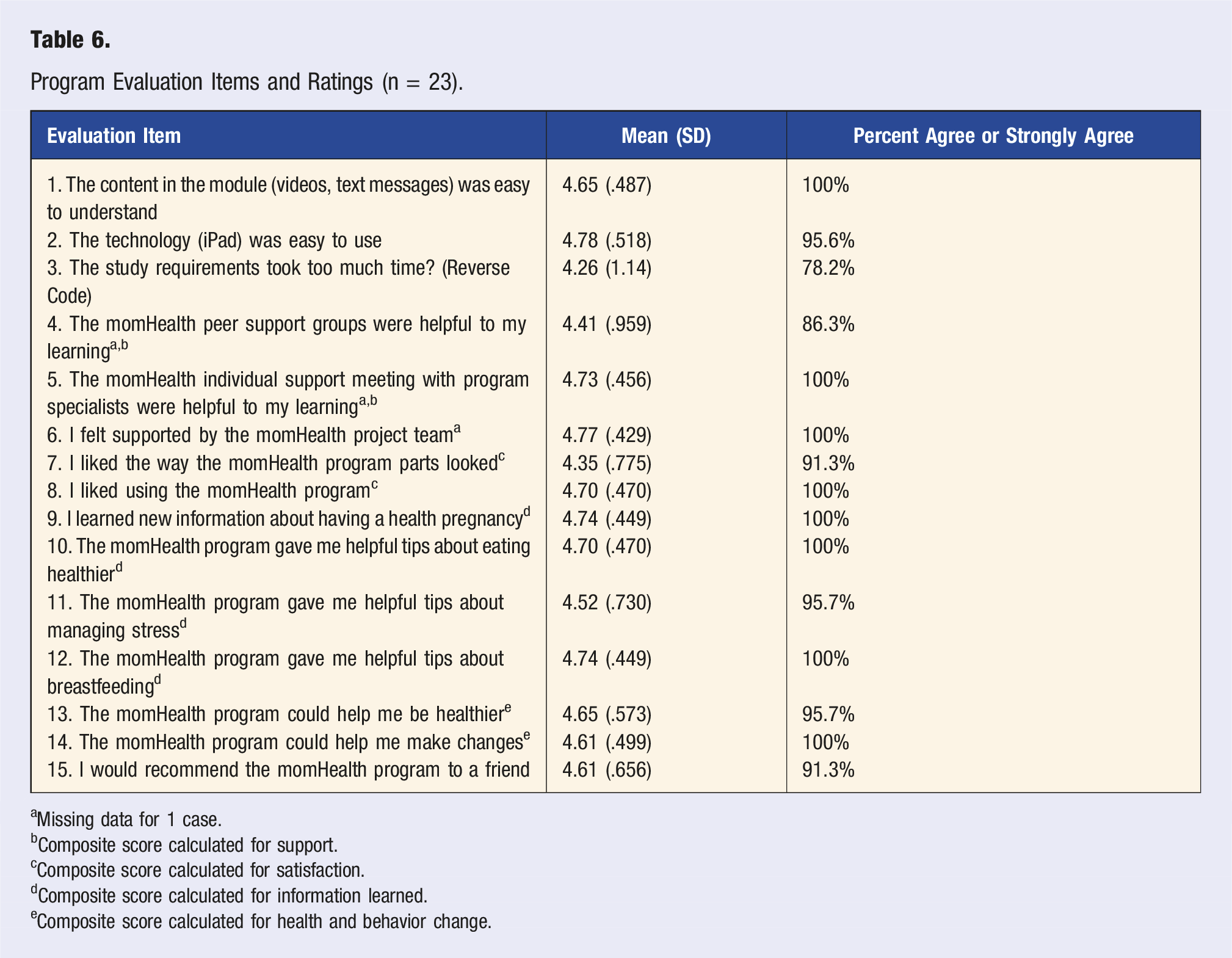
aMissing data for 1 case.
bComposite score calculated for support.
cComposite score calculated for satisfaction.
dComposite score calculated for information learned.
eComposite score calculated for health and behavior change.
Discussion
We pilot tested the momHealth MHBC program for adolescent pregnant/parenting mothers by comparing outcomes in breastfeeding, healthy lifestyle, and depressive symptoms to a control group; in addition, we evaluated our ability to recruit and retain this challenging underserved population. Breastfeeding initiation was high in both groups and continuation decreased over time to 3 months postpartum when 38% and 33% of the Intervention and Control group breastfed, respectively. Notably, Intervention group mothers were significantly more likely than the Control to continue breastfeeding to 5 weeks postpartum, but this difference was not sustained to 3 months postpartum. It appears that the Intervention contributed to the continuation of breastfeeding through 5 weeks, while the Control experienced more precipitous drops in breastfeeding maintenance in the same period. EBF rates at birth, 5 weeks, and 3 months and breastfeeding duration did not differ significantly between groups, suggesting lack of power to detect group differences.
The rate of breastfeeding in our total sample and by group is higher than overall 2017 US rates (84.1%), as well as that for mothers under age 20 years (74%) and mothers between 20 and 29 years (82.4%). 44 These higher rates of breastfeeding in our sample may be partially attributed to enhanced national public health emphasis on breastfeeding and enhanced breastfeeding supportive practices by hospitals and health care providers, for example, Healthy People 2020 and 2030 and the Baby Friendly Health Initiative. 45
A recent meta-analysis of breastfeeding support strategies for young mothers 46 determined that peer counseling, that is, a trained lay person, who is similar to the individual, provides breastfeeding support, was the most promising strategy associated with higher rates of exclusive breastfeeding. Our individual weekly counseling sessions were focused on all three behavioral areas but were provided by an International Board-Certified Lactation Consultant (IBCLC) which may have resulted in a heavier focus on breastfeeding. Participants rated these sessions highly for learning and support in all three areas. Larger studies of this momHealth intervention could capitalize on the professional counseling aspect and focus more on maintenance of “any” and “exclusive” breastfeeding.
Mothers in the intervention group ate fruits/vegetables at a comparable rate as their peers in the control group, demonstrating limited effect of the intervention on our primary benchmark for healthy eating. However, it is promising that there was synergy between breastfeeding at 3 months and fruit/vegetable consumption, potentially indicating that breastfeeding counseling may also benefit fruit/vegetable consumption. It may be that adolescents view healthy eating as critical to supporting the quality of their milk, in which case breastfeeding counseling with emphasis on the importance of long-term healthy eating may help promote health among these mothers. Of additional note, the average fruits/vegetables intake was lower than recommended in both groups, reflecting overall poorer nutrition seen in adolescents who are pregnant10-12 and may be associated with the barriers pregnant adolescents report to healthy eating such as socioeconomic status, 16 stress, motivation, and convenience. 17 Future iterations of momHealth may benefit from the identification of participant barriers to heathy eating and tailored intervention strategies to address these barriers. Mothers in the momHealth group met recommendations for MVPA at a higher rate than those in the Control—a promising finding. Overall, these results signal strong potential for MHBC interventions to promote healthy living behaviors among pregnant adolescents.
There were no significant differences observed between the intervention and control groups in depressive symptoms on the EPDS. This may be influenced by the project’s focus on depressive symptom prevention and related to exclusion criteria for untreated depression. Similar nonsignificant results were observed in a recent randomized trial by Phipps et al 47 Larger scale trials are needed to inform if depression prevention interventions may result in small yet significant effect sizes with at-risk populations.
momHealth participants rated the stress management/depression prevention curriculum useful. Future studies may look toward the impact of depression prevention component with adolescent populations particularly at risk for prenatal and postpartum depression. Hyman and Girard’s systematic review 48 suggests several factors that may be implicated in the onset of adolescent postpartum depression (PPD), including prior depression, lack of familial social support, and socioeconomic hardship. In addition, longer-term studies are needed to inform whether the depression prevention curriculum may have positive impact over time.
momHealth participants were ethnically diverse and most participants were from a low socioeconomic environment, with the mhealth technology well received. Future studies may explore a broader public health prevention component with resources associated with social determinants of health, which in turn may positively impact multibehavior health outcomes of interest and technology-supported delivery. A systematic review and meta-analysis 49 concluded social determinants of health contribute to the risk of adverse pregnancy outcomes in adolescent mothers, that is, being a member of a marginalized racial group, rural residence, inadequate education, and low SES. They suggest interventions take into consideration the underlying causal pathways to inequalities in adolescent pregnancy experience and outcomes. Future MHBC interventions could explore individual, neighborhood, and community-related intervention components to support adolescent mothers around social determinants of health. 50 Furthermore, consideration of the influence of power and stigma in young women’s lives is needed with an understanding of peripartum mental health and wellbeing as situated in physical and structural factors, rather than individual capacities alone.
Limitations
This study was a pilot test, and the sample was relatively small and underpowered for the detection of small effects. Furthermore, we experienced a total 25.8% attrition across the study, with larger attrition in the control than experimental group. However, this rate of attrition is smaller than in one of our previous studies with adolescent mothers 31 and attrition in other clinical trial research with young mothers is described as high in systematic review. 46 Despite the reduced power in our study, effect sizes for the significant differences by group were moderate and provide evidence for calculating power in a future momHealth RCT. Although ethnically diverse, the sample was predominantly from one bi-state urban area in the Midwest US. Our future RCT will include a larger and geographically diverse sample of rural and urban adolescent mothers to improve generalizability of study results.
Conclusion
In addition to high satisfaction with the intervention components, the momHealth intervention positively affected early breastfeeding continuation and trended toward positive outcomes in healthy living and depressive symptoms. Pandemic social distancing has further underscored the importance of mhealth interventions such as momHealth to deliver multi-behavioral health supports to the convenient home-based setting. This is particularly true with increased maternal anxiety and depression compared with pre-pandemic peers and increased need for social support and mental health services. 51 The increased familiarity and widespread adoption of clinical telehealth has high potential to extend evidence-based mHealth behavioral interventions for adolescent and the broader population of pregnant and parenting mothers. 52
Supplemental Material
sj-pdf-1-ajl-10.1177_15598276221080367 – Supplemental Material for A Health Behavior and Lifestyle Intervention Pilot Trial for Childbearing Adolescents
Supplemental Material, sj-pdf-1-ajl-10.1177_15598276221080367 for A Health Behavior and Lifestyle Intervention Pilot Trial for Childbearing Adolescents by Karen Wambach, Ann M. Davis, Eve-Lynn Nelson, Rebecca Swinburne Romine, Karman Romero, Rachel Muzzy, Megan Murray and Dana Bakula in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health [R21HD088913]; the Office of the Director of the National Institutes of Health [UG1OD024943] and a National Institutes of Health Clinical and Translational Science Award grant [UL1 TR002366] awarded to the University of Kansas; and University of Kansas School of Nursing and the Center for Children’s Healthy Lifestyles & Nutrition.
Author’s Note
Affiliation for KR is now Department of Nursing, Park University, 8700 NW River Park Drive, Parkville, MO 64152,
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding sources were not involved in data collection, analysis, or translation; in the writing of the report; or in the decision to submit the article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.