
Abstract
In this narrative review, we summarized evidence from peer-reviewed articles, published before February 2024, that investigated lifestyle behaviors among children (≤12 years) and adolescents (13-18 years) representing different geographic descents. These behaviors included dietary patterns, screen time, physical activity, smoking, alcohol consumption, oral hygiene, unsafe sex, and sleep duration and quality. We documented the significant impacts of parental, school, and sociodemographic factors on the adoption of numerous lifestyle behaviors in this age category. Several health consequences could be attributed to unhealthy lifestyle behaviors during childhood and adolescence. For example, poor dietary habits can lead to a higher risk of obesity and cardiovascular disease. Physical inactivity contributes to the development of musculoskeletal and psychological disorders. Excessive screen time is associated with visual acuity problems, poor sleep, and psychological and behavioral problems. Tobacco use poses a significant risk for severe respiratory and cardiovascular diseases. Risky sexual behaviors are related to sexually transmitted infections and exposure to violence. Short sleep duration is associated with a lack of physical fitness and poor cognitive function. However, potential interventions, such as school-based health programs, community outreach initiatives, and national health policies and regulations, can improve lifestyle behaviors among children and adolescents.
“Inadequate sleep may have disruptive effects on the cognitive function and learning capacity of children and adolescents.”
Introduction
Childhood and adolescence represent critical developmental periods when habits and behaviors are established, laying the foundation for future health trajectories. The impact of lifestyle factors during these formative years can extend into adulthood, affecting long-term health outcomes.1,2
The modern era has witnessed a substantial increase in the prevalence of chronic diseases, especially those of non-communicable origin, among children and adolescents.3,4 Unhealthy lifestyle behaviors have emerged as a significant contributing factor to this alarming trend.5,6 Lifestyle factors, such as dietary patterns, screen time, physical activity, smoking, alcohol consumption, oral hygiene, unsafe sex, and sleep duration and quality, can play a crucial role in shaping the health outcomes of young individuals.5,6
Investigating the contributing factors, health consequences, and potential interventions related to lifestyle behaviors is of paramount importance for promoting healthy living and preventing chronic diseases in this vulnerable population.7-9 Thus, we conducted this review to provide an overview of the lifestyle factors prevalent among children and adolescents. We explored factors that influence lifestyle behaviors in this age group, including societal, environmental, and familial determinants. Additionally, we described potential health consequences associated with unhealthy lifestyle choices during childhood and adolescence, such as obesity, cardiovascular disease (CVD), and mental health disorders. We also highlighted potential interventions and strategies that can be applied to promote positive lifestyle modifications among children and adolescents. Elucidating the effectiveness and feasibility of different interventions may provide insights and guidance to policymakers, health care professionals, parents, and teachers regarding their efforts to improve the health and well-being of the younger generation.
Methods
In this narrative review, we briefly presented contributing factors, health consequences, and potential interventions for certain lifestyle behaviors during childhood and adolescence. We collected evidence from 164 epidemiological studies, published in the Scopus and Web of Science databases before February 2024. The obtained studies investigated dietary patterns, screen time, physical activity, smoking behaviors, alcohol consumption, oral hygiene, unsafe sex, and sleep habits during childhood and adolescence. The age limits for childhood and adolescence were set based on the age limits of the reviewed studies (≤12 years for childhood and 10-12 to 18-20 years for adolescence). The publication time of the included studies ranged between 1986 and 2024 and was distributed as follows: before 2010: 11.6%, 2010-2015: 20.1%, 2016-2020: 32.3%, and after 2020: 36.0%. To reach generalizable conclusions, we included study populations representing different geographic descendants as follows: reviews, systematic reviews, meta-analyses, and cross-continental studies: 35.5%, North America: 15.9%, South America: 5.5%, Europe: 14.6%, Africa: 7.3%, West and Central Asia: 7.3%, East Asia: 11.6%, and Oceania: 4.3%.
Of note, we did not systematically obtain all related studies. Unpublished and non-peer-reviewed reports and studies published in languages other than English were not included.
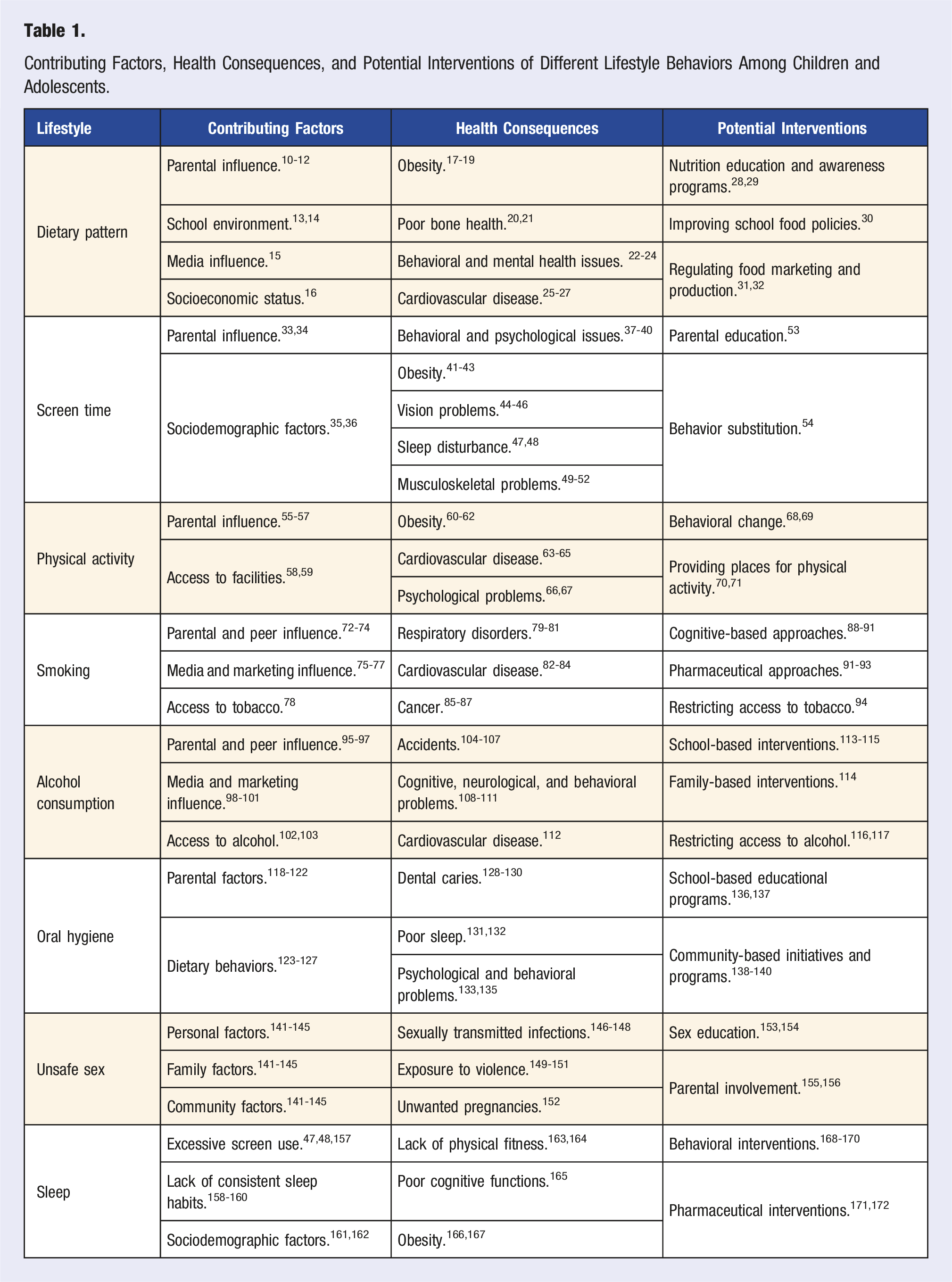
Contributing Factors, Health Consequences, and Potential Interventions of Different Lifestyle Behaviors Among Children and Adolescents.
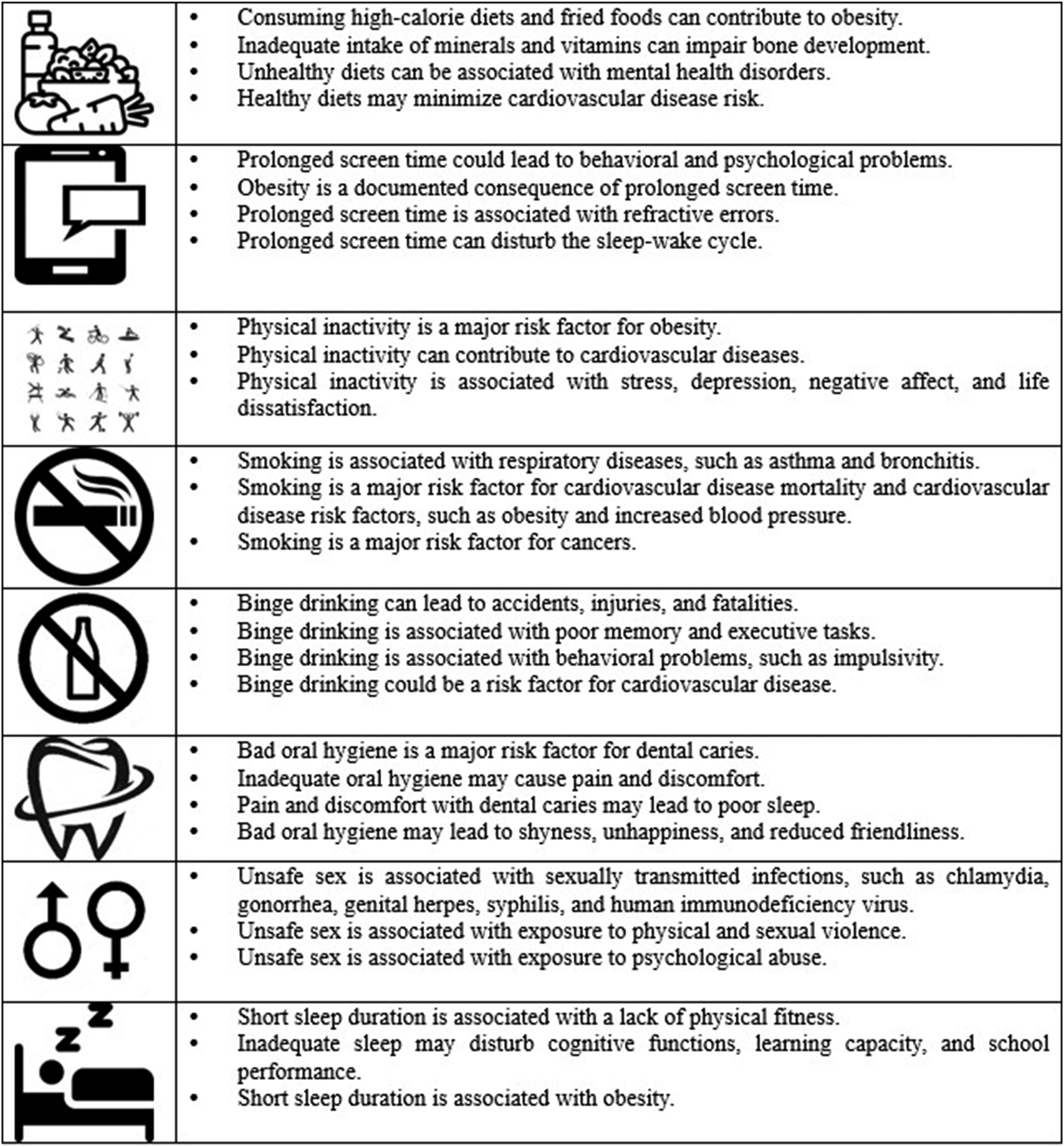
Main lifestyle behaviors and their associated health consequences in children and adolescents.
Lifestyle Behaviors: Contributing Factors, Health Consequences, and Potential Interventions
Dietary Patterns
Contributing Factors
Parental Influence
Parents play a vital role in providing healthy meals, setting an example through their eating behaviors, and creating a positive food environment at home. In the ToyBox Study, among 5185 European parents of preschool children (3-5 years), being permissive about unhealthy snacking and acceding to child demands for unhealthy snacks were associated with a greater intake of unhealthy snacks by children. 10 Parents with better nutritional knowledge of snack food recommendations were more likely to have children consuming healthy snacks. 10 Additionally, the family food environment can play an essential role in shaping food consumption at a young age. In a study including 9686 Chinese students (grades 3-12) and their parents, family food availability, parents’ nutritional literacy, meal practices, and food rules were associated with healthier food consumption. 11 Shared family meals are pointedly related to nutritional health in children and adolescents. A meta-analysis of 17 studies showed that children and adolescents who shared family meals ≥3 times/week were more likely to have healthier dietary patterns and were less likely to engage in disordered eating. 12
School Environment
Schools can influence children’s dietary intake by offering healthy meal options, implementing nutrition education programs, and promoting a supportive food environment. In a study including 1010 US students (12-13 years) from the Military Teenagers Environments, Exercise, and Nutrition Study (M-TEENS), unhealthy item availability at school was associated with purchasing sweets, snacks, and sugar-sweetened beverages. 13 A study of 812 Canadian students (10-11 years) showed that children exposed to unhealthy food outlets around the school had lower diet quality and consumed fewer fruits and vegetables. 14
Media Influence
The marketing of unhealthy foods and beverages to children and adolescents can influence their dietary preferences, purchases, and consumption. Various marketing strategies, especially those aimed at a younger audience, can shape their perceptions and choices related to food and drinks. Appealing packaging and design, advertising on children’s media and video games, promotions and contests, and celebrity endorsements are among these strategies. 15 A systematic review of 26 studies showed that unhealthy food and beverage marketing, especially through social media (6 studies) and advergaming (20 studies), can negatively impact children’s food choices and intake. 15
Socioeconomic Status
Socioeconomic status can play an essential role in determining the quality of the food consumed. A systematic review of 40 studies showed that parental education and family income were inversely associated with unhealthy dietary patterns, especially in developing countries. 16
Health Consequences
Obesity
The association between dietary patterns and obesity in children and adolescents is profound, with studies consistently demonstrating that diets high in processed foods and sugary beverages significantly contribute to the rising prevalence of childhood obesity. Conversely, adopting a balanced and nutrient-dense diet, rich in fruits, vegetables, and whole grains, plays a crucial role in mitigating the risk of obesity and promoting overall health in children. 17 The IDEFICS (Identification and prevention of Dietary- and lifestyle-induced health EFfects In Children and infantS) study analyzed data from 8341 children (2-9 years) representing 8 European countries and concluded that processed dietary pattern or changing to a sweet pattern were associated with increased body mass index, waist circumference, and fat mass 2 years later. 18 A study investigating 487 urban-dwelling children and adolescents (9-15 years) from 24 schools in Ghana showed that energy-dense dietary patterns, characterized by processed meat, fried foods, and sugary foods, were associated with overweight/obesity, while dietary patterns including starchy root staples and vegetables were associated with decreased overweight/obesity. 19 A systematic review and meta-analysis of 60 studies reported that a higher intake of sugar-sweetened beverages, fast food, meat, and refined grains was associated with a higher risk of overweight/obesity, while a higher intake of whole grains was associated with a decreased risk of overweight/obesity. 17
Poor Bone Health
The relationship between diet patterns and poor bone health in children is evident, as inadequate intake of essential nutrients such as calcium and vitamin D can compromise bone development later in life. 20 A prospective cohort study of 2850 Dutch children showed that infant dietary patterns at the age of 13 months, characterized by high intakes of dairy, whole grains, and eggs, were associated with increased bone mineral content at the age of 6 years. 20 A recent systematic review involving 7130 children and adolescents (3-17.9 years) showed a significant association between healthy dietary patterns and bone health markers in 7 studies. 21
Behavioral and Mental Health Issues
Unhealthy dietary patterns can be associated with an increased risk of mental health disorders. A study including Australian children (n = 1367; 5-10 years) and adolescents (n = 1277; 11-15 years) showed that those who met vegetable, fruit, and discretionary food intake guidelines were less likely to develop emotional, behavioral, and social problems. 22 Among 7114 adolescents (10-14 years) from the Australian Healthy Neighbourhoods Study, healthy diets, defined as having a daily breakfast and consuming low-fat dairy, 2 servings of fruit, and 4 servings of vegetables every day, were associated with a lower risk of depression. 23 In a study involving 71 553 Brazilian adolescents (12-17 years), healthy dietary patterns, having breakfast, and sharing meals with family were associated with better mental health. 24
Cardiovascular Disease
Healthy diets may minimize CVD risk by preventing its risk factors. A prospective cohort study of 116 430 female US nurses from the Nurses’ Health Study II (NHSII) showed that frequent consumption of fruits, vegetables, and whole grains during high school was associated with a lower risk of hypercholesterolemia and hypertension during adulthood. 25 In a study of 435 German children and adolescents (4-18 years), the intake of fruits and vegetables was associated with reduced blood pressure in the pre-puberty group, while salt intake was associated with elevated blood pressure in the puberty group. 26 Among 232 Brazilian children and adolescents with congenital heart disease (median age = 10 years), the excessive intake of ultra-processed foods was associated with high CVD risk defined as central adiposity, elevated high-sensitivity C-reactive protein, and subclinical atherosclerosis. 27
Potential Interventions
Nutrition Education and Awareness Programs
Providing nutrition education in schools and community settings can empower children and adolescents to make informed food choices and develop lifelong healthy eating habits. Besides, educating parents and caregivers about the importance of healthy diets and providing them with resources and guidance on meal planning and preparation can positively influence children’s eating habits.28,29 A study of 1535 Japanese adults revealed that those who received nutrition education at elementary and middle schools had better attitudes towards nutrition education during adulthood. 28 Additionally, family conversations on diet during elementary school years had a positive impact on consuming nutritionally balanced diets during adulthood. 28 A statewide program serving low-income US children (≤5 years) showed that enacting policies promoting healthy foods and educating parents about healthy diets were associated with increased consumption of fruits and lean proteins. 29
Improving School Food Policies
Implementing policies that promote nutritious school meals and ensure food safety standards can have a significant impact on children’s dietary behaviors. A meta-analysis of 91 interventions, aiming to modify school food environment policies, showed that direct provision policies, which mainly targeted fruits and vegetables, and competitive food/beverage standards, which mainly targeted sugar-sweetened beverages, were effective in improving the nutritional knowledge and behaviors of students. 30
Regulating Food Marketing and Production
Regulating food marketing and using economic incentives to promote healthier food choices, such as introducing taxes on sugary beverages and unhealthy snacks, while offering subsidies for fruits and vegetables, should be attempted. Still, more evidence is needed to explore the effectiveness of these interventions.31,32
Screen Time
Contributing Factors
Parental Influence
Parental behavior and attitudes towards screen use can impact screen time among children. A study of 489 Malaysian children (<5 years) showed that prolonged parental screen time and the positive perception of parents towards the influence of screen time on a child’s cognitive health were positively associated with screen time among their children. 33 Using screen devices as discipline tools was also associated with increased screen time in a study of 3141 Lebanese children (7-11 years). 34
Sociodemographic Factors
Sociodemographic factors may affect children’s screen time. Two studies including children and adolescents from Colombia (n = 16 459; 3-17 years) and Iran (n = 14 880; 6-18 years) showed that children and adolescents who came from wealthier families or were living in urban areas had more screen time.35,36
Health Consequences
Behavioral and Psychological Issues
Prolonged screen time could lead to serious behavioral and psychological problems among children and adolescents, emphasizing the importance of mindful screen use in maintaining optimal mental well-being. In the Adolescent Brain Cognitive Development study, 11 875 US children (9-10 years) and their parents showed increased rates of rule-breaking and aggressive behaviors and social and thought problems among children who reported greater screen time. 37 Among 101 350 US children and adolescents (≤17 years) from the 2018-2020 National Survey of Children’s Health (NSCH), prolonged screen time was associated with developmental delay, speech disorder, learning disability, behavioral and conduct problems, autism spectrum disorders (ASD), and attention deficit hyperactivity disorder. 38 A study investigating 1140 Palestinian adolescents (16-17 years) showed that using electronic devices (smartphones, laptops, tablets, and video game players) for a long time was associated with depression and anxiety. 39 Additionally, a study from Egypt, including 560 preschool children from 10 nurseries and their mothers, showed a positive correlation between the duration of media exposure and experiencing learning problems, hyperactivity, impulsivity, conduct problems, anxiety, and psychosomatic problems. 40
Obesity
Obesity is a documented consequence of prolonged screen time. 41 Displacing time that could be spent practicing physical activity, food advertising, and eating while viewing can explain this association. 41 Previous meta-analyses indicated positive associations between screen time and overweight/obesity among children and adolescents.42,43
Vision Problems
Screen time is a near-work activity associated with several visual problems. A study of 1508 students (8-14 years) from Hong Kong detected a dose-response association between smartphone use and digital eye strain. 44 Among 469 Egyptian students (12-14 years), screen time was positively associated with refractive errors (myopia, hyperopia, and astigmatism). 45 In a study involving 7497 Spanish children (5-7 years), children who reported more screen hours were more likely to develop myopia. 46
Sleep Disturbance
Prolonged screen time has a potentially disturbing impact on children’s sleep-wake cycles. In a study including 314 caregivers of Korean children (4-7 years), the frequency of smartphone screen use was associated with bedtime resistance, nighttime awakening, and daytime sleepiness. 47 A systematic review of 109 studies investigating children and adolescents in Western countries showed that prolonged screen time was associated with difficulty falling asleep, short sleep duration, poor sleep quality, and daytime tiredness. 48
Musculoskeletal Problems
Prolonged screen time, particularly when accompanied by poor ergonomics and improper posture, can contribute to musculoskeletal problems. A study including 200 adolescents (10-14 years) from Hong Kong showed that increased computer use was associated with trunk asymmetry, undermining the health-related quality of life. 49 Another study including 1022 adolescents (11-15 years) from the Nordic countries showed a positive association between screen time and physical complaints. 50 A systematic review of 9 Brazilian studies showed a positive association between screen time and non-specific low back pain in adolescents (6-19 years) exposed to screen time for ≥ 3 hours/day. 51 In a dose-response meta-analysis of 9 studies investigating adolescents (11-19 years), there was a positive correlation between daily computer time, daily mobile phone time, daily TV watching, and the risk of low back pain, separately. 52
Potential Interventions
Parental Education
Promoting digital literacy among parents could be effective in minimizing screen time among children and adolescents. A meta-analysis of 204 studies showed that educating parents about the potential dangers of screen time helped them monitor their children’s screen use and minimize their screen time. 53 Intervention strategies with clear goals, feedback, and planning behavioral techniques were noticeably effective. Yet, the effectiveness of most interventions was short-term. 53
Behavior Substitution
Replacing screen use with healthier habits, such as practicing physical activity, is a promising approach. A meta-analysis of 7 randomized controlled trials showed that behavior substitution could effectively reduce screen time. 54
Physical Activity
Contributing Factors
Parental Influence
Parental support and involvement play a crucial role in promoting physical activity among children. A study of 102 Canadian children (3-5 years) showed that children who received greater parental support for physical activity were almost 6 times more likely to be physically active. 55 In a study investigating 717 Japanese children (8-9 years), direct parental assistance for physical activity encouraged children to engage in moderate-to-vigorous physical activity. 56 Another study including 651 adolescents (grade 10) from Bosnia showed that maternal and paternal education was associated with higher physical activity levels among their children. 57
Access to Facilities
The physical environment in which children live, play, and attend school can influence their physical activity levels. A study of 136 US children (2-5 years) showed that the provision of sufficient outdoor active play, using portable play equipment, the presence of a variety of fixed play equipment, and having a suitable indoor play space were associated with higher levels of physical activity. 58 In a systematic review of 14 studies investigating Pacific Island Countries and Territories with Non-European, Non-Asian ancestry children and adolescents, community barriers to physical activity included minimal indoor facilities for physical activity, inadequate footpaths/cycle paths, distance for active transport, and safety issues. 59
Health Consequences
Obesity
Childhood lower physical activity levels are strongly associated with obesity. A study of 1266 Indian children and adolescents (6-17 years) showed that the lack of physical activity, in the form of passive transport to school, not playing during lunch breaks, and not participating in household work, was associated with obesity. 60 Besides, among 1090 South African primary schoolchildren (mean age = 8.3 years), lower moderate-to-vigorous physical activity was associated with overweight/obesity and higher relative body fat. 61 In a study investigating 688 children and adolescents (6-16 years) from Saudi Arabia, lack of physical activity was associated with overweight and obesity. 62
Cardiovascular Disease
The lack of physical activity is a risk factor for CVD. A 30-year cohort study of 5115 US young adults, registered in the Coronary Artery Risk Development in Young Adults (CARDIA) study, showed that lower physical activity levels during younger age were associated with future risk of coronary heart disease, heart failure, and stroke. 63 A study from Poland including 568 children and adolescents with intellectual disabilities (7-18 years) showed that the risk of hypertension was greater among those who reported lower levels of physical activity. 64 A study of 1961 Finnish children and adolescents (3-18 years) showed that physical activity was associated with a lower risk of major CVD risk factors, including obesity, high triglyceride, low high-density lipoprotein cholesterol, and insulin and glucose concentrations, during adulthood. 65
Psychological Problems
Physical activity can support the current and future mental health of children and adolescents. A meta-analysis of 114 studies investigating children and adolescents showed that physical activity was positively associated with psychological well-being, life satisfaction, happiness, and self-image, but negatively associated with stress, depression, negative affect, and psychological distress. 66 A meta-analysis of 31 studies showed that the administration of physical activity, compared to a control group, led to moderate improvements in ASD and depression among children and adolescents. 67
Potential Interventions
Behavioral Change
Promoting physical activity for schoolchildren and adolescents via interventional programs that educate parents, teachers, and schoolchildren about the health impacts of physical activity is important. Freely chosen and unstructured physical activity at schools was shown in a systematic review to have the potential to promote physical activity. 68 A meta-analysis of 57 controlled trials showed that interventions with both school and family or community involvement promoted physical activity among children and adolescents. 69 Multicomponent interventions that aimed to promote physical activity among other healthy lifestyle behaviors were particularly effective. 69
Providing Places for Physical Activity
Providing indoor and outdoor spaces may help children and adolescents engage in physical activity. A study including 179 Chinese children and adolescents (6-14 years) showed that the availability of playgrounds and open green spaces was associated with higher levels of physical activity. 70 Providing enough indoor spaces for 496 preschool US children resulted in greater involvement in physical activity. 71 These findings highlight the need for considering several environmental factors, such as the availability of safe play spaces, walkability, and access to sports and recreational facilities and programs.
Smoking
Contributing Factors
Parental and Peer Influence
Adolescents with parents or peers who smoke are more likely to start smoking due to exposure to and normalization of smoking behaviors. In a prospective cohort study including 8944 UK adolescents (13-15 years) who had never smoked tobacco, having parents or peers with smoking behaviors more than doubled the risk of smoking among those adolescents 2 or 3 years later. 72 Besides, Ethiopian students in rural and urban secondary schools (10-19 years; n = 341) who reported smoking were more likely to have parents, friends, or classmates who were current smokers. 73 In a study including 5705 US parents and their children (9-16 years), parent-youth connectedness and parental monitoring and punishment for smoking significantly decreased the odds of smoking initiation. 74
Media and Marketing Influence
Media and marketing campaigns that encourage or normalize smoking among adolescents have negative impacts. Additionally, the visibility of tobacco products in marketing and advertising can contribute to the perception that they are easy to obtain. The more prevalent and accessible these products appear in media and promotional materials, the more likely adolescents may perceive them as readily available.75-77 A one-year follow-up study of 11 279 US adolescents (12-18 years), registered in the PATH (Population Assessment of Tobacco and Health) study, showed that exposure to and interactions with social media presenting tobacco content were associated with their tobacco use. 75 Among 4332 Nigerian students in rural and urban secondary schools (10-19 years), exposure to tobacco smoking-related media was associated with current smoking. 76 Using data from adolescents (mean age = 14.3 years) from the Global Youth Tobacco Surveys (GYTS) (2014-2017) for Cameroon, Gabon, Comoros, Seychelles, Mauritius, Tanzania, Gambia, Ghana, and Sierra Leone, tobacco marketing was closely associated with smoking initiation. 77
Access to Tobacco
Easy access to tobacco is also a risk factor for smoking. The perception among adolescents that tobacco products are easy to obtain is considered a risk factor for smoking initiation and progression. This perception can contribute to a more permissive attitude toward tobacco use, making it seem more accessible and socially acceptable. 78 A meta-analysis of 11 studies showed a significant association between tobacco outlet density around homes and adolescents’ past-month smoking behavior. 78
Health Consequences
Respiratory Disorders
Smoking during adolescence has negative health impacts on the respiratory system. A study including 2295 Swedish adolescents (16 years) showed that smoking was associated with reduced forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) ratio and increased peripheral airway resistance. 79 Smoking was also associated with a higher risk of chronic bronchitis among 3108 high school students (15-19 years) from Poland. 80 A prospective cohort study including 2609 US students (4-7 grades) showed that smoking ≥ 7 cigarettes/day was associated with an increased risk of asthma. 81
Cardiovascular Disease
Smoking is a major risk factor for CVD, even in young individuals. A Greek study of 238 adolescents (12-15 years) showed that those who reported smoking had a higher prevalence of CVD risk factors, such as obesity and increased blood pressure. 82 In the Harvard Alumni Health Study, cigarette smoking from adolescence to middle age was positively associated with CVD mortality among 5785 US men. 83 In a study including 236 Aboriginal Canadian youths (10-19 years), smoking ≥ 6 cigarettes/day increased CVD risk profile consisting of a higher mean systolic blood pressure and homocysteine level and a lower mean serum folate level. 84
Cancer
Smoking during adolescence significantly increases the risk of developing various types of cancers later in life. A study of 102 098 Kenyan and Nigerian women showed that women who started smoking during their teenage and continued to smoke for 20 years or more had a higher risk of breast cancer compared to those who did not smoke or those who initiated smoking later in age. 85 Similarly, starting smoking at a young age was associated with an increased risk of breast cancer among 102 927 UK women from the Generations Study. 86 A prospective cohort study including 40 897 Japanese middle-aged and older adults showed that those who started smoking before the age of 17 years had significantly a higher risk of lung cancer than those who started smoking after the age of 20 years. 87
Potential Interventions
Cognitive-Based Approaches
Cognitive-based approaches for smoking cessation among adolescents focus on teaching skills to manage withdrawal symptoms and prevent relapse using self-monitoring, coping skills, and positive reinforcement for abstinence. 88 However, previous interventions from the US (n = 407; mean age = 16 years) 89 and France (n = 1814; mean age = 16.9 years) 90 showed that these approaches had minimal impacts. A meta-analysis of interventions showed a modest effect for group counseling, but no effect for individual counseling, mixed delivery methods, or computer or messaging interventions. 91
Pharmaceutical Approaches
Nicotine replacement therapy is a widely used pharmacotherapy for smoking cessation. Previous interventions performed on Dutch adolescents (n = 257; mean age = 16.7 years) showed that nicotine replacement therapy slightly promoted abstinence rates in the short run only.92,93 A meta-analysis of pharmaceutical interventions failed to detect significant impacts of nicotine replacement therapy or other medications on smoking cessation. 91
Restricting Access to Tobacco
Several policies could be attempted to limit youth access and exposure to tobacco, such as increasing the minimum age of sale, limiting the number or type of tobacco outlets, and banning the display of tobacco products. 94 However, limited evidence is available about the effectiveness of these interventions. 94
Alcohol Consumption
Contributing Factors
Parental and Peer Influence
Parents with permissive attitudes toward alcohol can increase the likelihood of adolescent drinking. Peers also have a significant influence because adolescents may feel pressured to drink to fit in, be accepted, or conform to social norms. A study of 3017 US students (6-12 grades) showed that parental and peer drinking behaviors were associated with moderate or heavy drinking among adolescents. 95 Using data from 1183 Taiwanese children (10-11 years) registered in the Child and Adolescent Behaviors in Long-term Evolution (CABLE) study, having parents who both used alcohol, less parental support, and more family conflict were significant predictors of first alcohol use in the following year. 96 Another study including 413 adolescents (16-19 years) in a rural community in Thailand showed that having close friends consuming alcohol increased the likelihood of current drinking. 97
Media and Marketing Influence
The portrayal of alcohol in the media, including movies and advertisements, can glamorize drinking and create a perception that it is a normative behavior for adolescents. Previous systematic reviews detected that the exposure of adolescents to alcohol-related content on the internet, media, and commercials was associated with their subsequent alcohol consumption.98-101
Access to Alcohol
Adolescents who live near alcohol outlets tend to consume more alcohol, despite laws prohibiting alcohol purchases. In a study including Australian adolescents (n = 44 897 from urban settings and 23 311 from regional settings; age = 12-17 years), higher densities of general, on- and off-premises outlets in the immediate neighborhood were associated with a higher likelihood of alcohol consumption. 102 Another study including 1388 sixth-grade US students and their parents showed that accessibility of alcohol at home was associated with significant increases in the trajectories of young adolescent alcohol use and intentions. 103
Health Consequences
Accidents
Underage drinkers are more likely to engage in risky behaviors such as driving under the influence of alcohol, which can lead to accidents, injuries, and fatalities. Alcohol impairs judgment, coordination, and reaction time, making it particularly dangerous for drivers.104,105 A study of 4021 US young adults who reported alcohol drinking showed that those who started drinking at an age <21 years were more likely to get involved in motor vehicle crashes and unintentional injuries compared with individuals who started drinking at the age of 21 years. 106 Starting drinking at an age <14 years increased the odds of motor vehicle crashes by 6 times and unintentional injuries by 4 and a half times. 106 In a study investigating 4729 injured adolescents visiting 6 emergency departments in South Korea, motorcycle-related injuries were strongly associated with alcohol use. 107
Cognitive, Neurological, and Behavioral Problems
Alcohol consumption during adolescence has several cognitive and neural consequences. A study of 89 university students (mean age = 18.8 years) from Brazil showed that participants with a persistent binge drinking trajectory over 2 years performed poorer in memory and executive tasks than those who gave up their pattern of consumption and non-binge drinkers. 108 A longitudinal analysis of 548 US adolescents (12-21 years) showed that those who initiated alcohol drinking were more likely to show MRI-documented disturbed cerebellar growth, suggesting they would experience coordination, imbalance, and gait disorders later in life. 109 Another study including 116 US adolescents (10-19 years) showed a positive association between binge drinking and impulsivity. 110 A study including 828 Norwegian tertiary school students (15-20 years) showed more depressive and psychosomatic complaints and problems with parents and peers among those who reported alcohol intoxication. 111
Cardiovascular Disease
Adolescent binge alcohol consumption is a risk factor for CVD. A study including 1266 UK adolescents (17 years), registered in the Avon Longitudinal Study of Parents and Children (ALSPAC), showed vascular damage attributed to high-intensity alcohol drinking; carotid to femoral pulse wave velocity (PWV) was higher among heavy drinkers, and this effect was augmented among smokers. 112
Potential Interventions
School-Based Interventions
School-based interventions to minimize alcohol misuse among adolescents include a constellation of programs, such as educational programs, life skills training, social norms campaigns, peer-led interventions, and parental involvement programs. Schools may offer screening and counseling services and enhance alternative activities. Previous systematic reviews showed varying effects for these programs.113-115 Interventions characterized by combining more than 1 program and involving parents were more likely to be effective.113-115
Family-Based Interventions
It is important to work with the entire family to address underlying issues that may contribute to alcohol misuse among adolescents. Parental involvement, modeling, dynamics, and communication patterns may influence the behavior of young individuals, including their relationship with alcohol. 114 Parenting skills training, family education programs, and promoting positive interactions and active communication between parents and adolescents were shown in previous systematic reviews to be effective. 114
Restricting Access to Alcohol
Policy strategies aiming at increasing the minimum legal drinking age, reducing the commercial and social access of adolescents to alcohol, enforcing retailer compliance, and controlling the density of alcohol outlets may be useful.116,117 However, effective underage drinking prevention typically involves a combination of these strategies, tailored to the specific cultural and legal context of a given region. Collaborations among government agencies, law enforcement, educators, parents, and community organizations are keys to implementing and enforcing these policies successfully.116,117
Oral Hygiene
Contributing Factors
Parental Factors
Parental socioeconomic status and behaviors can significantly influence the oral hygiene of their children. A study including 2338 parents of children from 167 kindergartens in Poland showed that parental education, income, health literacy, and oral hygiene practices were associated with better oral hygiene among their children. 118 Among 791 Libyan children (12 years), 213 Indonesian children (<12 years), and 400 Indian children (5 years), lower parental education was associated with dental caries.119-121 A systematic review of 14 studies detected that parental tooth brushing behavior, educational and occupational levels, dietary patterns, dental visits, snacking frequency, psychological status, and knowledge of oral health were associated with dental caries among their children. 122
Dietary Behaviors
There is abundant evidence that certain dietary behaviors are risk factors for dental caries. A study of 8647 Portuguese children (4 years) and their mothers showed that children who consumed energy-dense foods and multiple snacks were more likely to develop severe dental caries 3 years later. 123 Among 495 Australian children (5-10 years), chocolate consumption was associated with primary dentition caries. 124 A study investigating 247 preschool children (mean age = 4.1 years) from Saudi Arabia showed a higher risk of dental caries among children who consumed sweetened milk, soft drinks, and sweets. 125 In a study including 698 Iranian children (10-12 years), children who consumed fizzy soft beverages and sweet biscuits > once/day were more likely to have dental caries. 126 A systematic review of ten longitudinal studies showed that the intake of candy, 100% juice, and soft and sweet drinks at bedtime was associated with dental caries in children. 127
Health Consequences
Dental Caries
Bad oral hygiene is a major risk factor for dental caries. Previous studies from the UK (n = 1450; 1.5-4.5 years), Iraq (n = 342; 6 years), and Palestinian refugee camps in Jordan, Lebanon, Syria, Gaza Strip, and West Bank (n = 2781; 12 years) showed that infrequent tooth brushing was associated with dental caries.128-130
Poor Sleep
Bad oral hygiene and dental caries may cause pain and discomfort; factors that can result in poor sleep. A study investigating 332 Japanese preschoolers (3-6 years) showed that children with dental caries slept significantly shorter periods. 131 Having untreated dental caries was associated with trouble sleeping among 1589 students (8-10 years) from Brazil. 132
Psychological and Behavioral Problems
Dental health may also affect psychosocial well-being. Among 793 Brazilian children (8-10 years), cavitated carious lesions were associated with general anxiety. 133 A study of 40 752 US children and adolescents (6-17 years) showed that dental problems were associated with shyness, unhappiness, feelings of worthlessness, and reduced friendliness, especially among those between 15-17 years. 134 In a study including 713 713 Korean adolescents (12-18 years), experiencing oral symptoms was associated with increased suicide ideations and attempts and feelings of sadness and despair. 135
Potential Interventions
School-Based Educational Programs
Raising children’s awareness of oral health, including proper brushing techniques, flossing, and regular dental checkups, should begin in kindergartens and schools. Interventions given by various aids, such as lectures and presentations, flipcharts, drawings, leaflets, albums, models, E-programs, and games were shown in a meta-analysis of 7 trials to be effective in improving oral hygiene and reducing dental caries among school students (5-16 years). 136 Another meta-analysis of 12 trials showed that school-based educational interventions in developing countries could improve oral health knowledge, attitudes, and behaviors. 137
Community-Based Initiatives and Programs
Several community-based initiatives were launched to improve the dental health of children by applying free or low-cost dental diagnostic, preventive, restorative, prosthodontic, and endodontic services, such as dental examinations, cleaning, X-rays, fillings, extractions, and oral surgeries. Other initiatives included oral health educational activities, supervised toothbrushing programs, and motivational interviewing. Besides, community outreach and awareness campaigns targeting parents were shown to be essential for promoting the oral health of their children. These campaigns involved distributing educational materials, organizing workshops, and promoting healthy dental habits.138-140
Unsafe Sex
Contributing Factors
Starting sexual activity at a young age, having a high-risk partner or multiple sex partners, and engaging in unprotected sex are common risky sexual behaviors during adolescence. A systematic review of 16 studies showed that several personal, family, peer, and community factors can contribute to risky sexual behaviors. These factors interact in a way that they could not be described solely, and most studies investigated them together. 141 A study investigating 659 Ethiopian adolescents (15-19 years) showed that poor social support, living out of the family, experiencing parental neglect, and drinking alcohol were associated with risky sexual behaviors. 142 Among 397 adolescents from Thailand (10-19 years), risky sexual behaviors were positively associated with age, male sex, having a boyfriend/girlfriend, uninvolved parenting style, parental approval of sex, perceived peer norms, neighborhood disorganization, and community norms, but negatively associated with religious beliefs and practices, parental monitoring, and neighborhood social cohesion. 143 Another study including 6167 high school and vocational students (mean age = 15.6 years) from Thailand showed that smoking cigarettes, using cannabis, gambling, and experiencing childhood sex abuse were associated with risky sex behaviors. 144 Using data from 1200 Australian adolescents (13-17 years) registered in the Western Australian Pregnancy Cohort [Raine] Study, internalizing (e.g., anxious/depressed, withdrawn) and externalizing (e.g., delinquent, aggressive) behavior problems were associated with earlier first sexual intercourse. 145
Health Consequences
Sexually Transmitted Infections
Chlamydia, gonorrhea, genital herpes, human papillomavirus (HPV), syphilis, and human immunodeficiency virus (HIV) are among the most frequent sexually transmitted infections (STIs) affecting adolescents. In a study including 196 Brazilian adolescents (14-19 years) treated at a family planning outpatient clinic in the western Amazon, 32% had at least 1 STI, with the most prevalent being chlamydia (23%), trichomoniasis (5.6%), herpes simplex (4.6%), and gonorrhea (3.1%). 146 A study including 317 Spanish adolescents (10-19 years) who were referred to an STI clinic in Madrid put the prevalence of gonorrhea, chlamydia, syphilis, and HIV at 21.7%, 17.1%, 4.8%, and 2.4%, respectively. 147 The study also showed that having first sexual relations at a young age was associated with STI. 147 Among 4389 US adolescents (14-20 years) presenting to an Emergency Department, 10% reported a previous history of STIs, and risky sex behaviors were associated with increased odds of STIs history. 148
Exposure to Violence
Adolescents who engage in unsafe sex are more likely to be physically or psychologically victimized. Among 517 sexually active adolescent girls (<18 years) who presented for contraceptive care in the US, experiencing violence was associated with early initiation of sex, having sex with strangers, having multiple partners, or having a partner with multiple partners. 149 A study of 563 African US students (13-19 years) showed a significant association between risky sex behaviors and exposure to community violence. 150 Another study including 179 adolescent girls (mean age = 18.9 years) recruited from social service agencies in the US showed that risky sexual behaviors were associated with both physical assault and sexual victimization. 151
Unwanted Pregnancies
Unwanted pregnancies and abortions are common among female adolescents engaging in unsafe sex. Among sexually active female street-involved adolescents (10-19 years) in Nigeria, 63.7% reported having had sex and 23.7% had a history of pregnancy, of which 59.4% gave a history of induced abortion of the last pregnancy. 152
Potential Interventions
Sex Education
Implementing evidence-based, age-appropriate, and culturally sensitive sex education programs in schools is important. These programs should cover topics like reproductive health, contraception, STIs, consent, and healthy relationships. Providing accurate information empowers adolescents to make informed decisions.153,154
Parental Involvement
Encouraging parents and caregivers to engage in open and non-judgmental conversations about sexuality and relationships is important. Supportive parental involvement can positively influence the decisions of adolescents.155,156
Sleep
Contributing Factors
Excessive Screen Use
Screen time is closely associated with sleep duration and quality. In a study including 314 caregivers of Korean children (4-7 years), the frequency of smartphone screen use was associated with bedtime resistance, sleep duration, nighttime awakening, and daytime sleepiness. 47 Among 11 878 US children (9-10 years), greater screen time was associated with decreased sleep duration and increased sleep onset latency, excessive sleepiness, insomnia, and overall sleep disturbance symptom severity. 157 A systematic review of 49 studies investigating children and adolescents (≤15 years) showed that electronic media use was associated with delayed bedtime and poor sleep quality in children (6-12 years). 48
Lack of Consistent Sleep Habits
Good sleep habits include a consistent sleep routine, avoidance of active and stimulating activities before sleep, utilizing only the bed for sleeping, and adhering to consistent sleep and wake-up times. 158 Having a consistent bedtime routine is often recommended to parents of young children. A study of 405 US mothers and their infants (n = 206; .5-1.5 years) or toddlers (n = 199; 1.5-3 years) showed that having a bedtime routine resulted in significant reductions in problematic sleep behaviors for infants and toddlers. 159 Another study investigating mothers of 10 085 children (≤5 years) from 14 countries showed that having a consistent bedtime routine was associated with better sleep outcomes, including earlier bedtimes, shorter sleep onset latency, reduced night wakings, and increased sleep duration. 160
Sociodemographic and Environmental Factors
Several sociodemographic and environmental factors can affect sleep quality. A study including 855 children (4-9 years) and 1047 adolescents (10-17 years) from Germany showed that lower socioeconomic standard was associated with bedtime resistance, sleep onset delay, sleep-related anxiety, night waking, and parasomnia. 161 Another study of 6728 German adolescents (11-17 years) showed that living with a single parent, having siblings, and residing in provincial, urban, or metropolitan areas were associated with more sleep problems. 162
Health Consequences
Lack of Physical Fitness
Sleep duration and quality may also affect physical fitness. Among 21 857 Chinese children (3-6 years), abnormal sleep duration was associated with low physical fitness. 163 A systematic review of 6 studies investigating 5797 children and adolescents (6-19 years) from 11 countries showed that shorter periods of sleep and worse sleep quality were associated with lower levels of physical fitness. 164
Poor Cognitive Functions
Inadequate sleep may have disruptive effects on the cognitive function and learning capacity of children and adolescents. In a large meta-analysis of 86 studies investigating 35 936 children (5-12 years), sleep duration was positively associated with cognitive performance, especially executive functioning, performance on tasks that address multiple cognitive domains, and school performance, but negatively associated with both internalizing and externalizing behavioral problems. 165
Obesity
Sleep duration may also be associated with obesity. A meta-analysis of 33 articles, involving 57 848 children and adolescents, revealed statistically significant associations between short sleep duration and obesity. In dose-response meta-analyses, short sleep duration increased the risk of obesity in toddlers (1-2 years) by 20%, in preschool-aged children (3-5 years) by 58%, and in school-aged children (6-13 years) by 82%. 166 A meta-analysis of 25 prospective cohort studies including 56 584 children and adolescents showed that short sleep duration was associated with obesity and weight gain during follow-up. 167
Potential Interventions
Behavioral Interventions
Several behavioral changes could improve sleep in children and adolescents, such as establishing a regular sleep routine by setting a consistent bedtime and wake-up time, limiting screen time before bed, creating a sleep-friendly environment by keeping the room dark, quiet, and at a comfortable temperature, encouraging regular physical activity, and limiting caffeine and sugar intake, especially in the late afternoon and evening.168-170
Pharmaceutical Interventions
Melatonin, antihistamines, benzodiazepines, and alpha agonists are the most commonly prescribed medications for the management of sleep disorders in children and adolescents. However, evidence of their long-term safety and efficacy is not robust.171,172
Conclusion
This review highlighted various lifestyle behaviors that play a pivotal role in shaping the overall health of children and adolescents, including dietary patterns, screen time, physical activity, smoking, alcohol consumption, oral hygiene, unsafe sex, and sleep duration. Identifying the factors influencing these behaviors allows for a better understanding of the complex interplay between individual, familial, societal, and environmental determinants. Additionally, we described the health consequences of unhealthy lifestyle behaviors and potential interventions that may revert these behaviors or mitigate their effects. We believe that this review can serve as a resource for policymakers, health care professionals, parents, and teachers, emphasizing the need for collective efforts in enhancing healthy lifestyle behaviors among children and adolescents.
Supplemental Material
Supplemental Material - Lifestyle Behaviors of Childhood and Adolescence: Contributing Factors, Health Consequences, and Potential Interventions
Supplemental Material for Lifestyle Behaviors of Childhood and Adolescence: Contributing Factors, Health Consequences, and Potential Interventions by Ahmed Arafa, Yuka Yasui, Yoshihiro Kokubo, Yuka Kato, Chisa Matsumoto, Masayuki Teramoto, Saya Nosaka, and Miho Kogirima in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
We would like to thank Dr Rena Kashima.
Authors’ Contributions
A. A. (conceptualization, literature review, and manuscript drafting), Y. K. (conceptualization, funding acquisition, and supervision), and all authors (revision and editing).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Intramural Research Fund for the cardiovascular diseases of the National Cerebral and Cardiovascular Center (20-4-9, 23-B-9), the JH Young Researcher Grant, the Health and Labour Sciences Research Grants of the Ministry of Health, Labour, and Welfare of Japan, AMED (21dk0207053h0001), the Japan Science and Technology Agency (JPMJPF2018), and the Cross-ministerial Strategic Innovation Promotion Program (SIP) “Building a Resilient and Nourishing Food Chain for a Sustainable Future.” From the Bio-oriented Technology Research Advancement Institution (JP J012287).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.