
Abstract
The purpose of this study was to examine the associations among physical activity, dietary behaviors, and other salient health behaviors such as smoking, alcohol consumption, and sleeping with self-reported adolescent mental health on the 2017 National Youth Risk Behavior Survey (YBRS). A multistage cluster sampling procedure was employed to yield a representative sample of US adolescents. The number of sampled adolescents with usable data was 14 765. Weighted logistic regression models were employed to examine the predictive utility of independent health behaviors associating with reported mental health problems (difficulty concentrating, remembering, or making decisions), and meeting multiple health behavior criteria with reported mental health problems adjusting for age, sex, body mass index percentile, and race/ethnicity. Meeting physical activity guidelines, consuming breakfast every day, not smoking and/or consuming alcohol in the past 30 days, and sleeping at least 8 hours per night independently associated with lower odds of mental health problems (P < .01). For every one additional positive health behavior met, there were significantly lower odds of reported mental health problems (OR = 0.73, 95%CI 0.68-0.78, P < .001). Meeting salient positive health behavior criteria and meeting multiple positive health behavior criteria associated with lower odds of self-reported difficulty concentrating, remembering, or making decisions on the 2017 National YRBS.
‘Difficulty concentrating, remembering, and making decisions is a possible indicator of mental health problems.’
Maintaining positive mental health is a struggle in today’s society for adolescents, as there has been a substantial rise in psychosocial disorders affecting young people over the past 50 years. 1 Many adolescents have difficulty concentrating, remembering, and making decisions that greatly affects quality of life, especially those who are diagnosed with attention deficit hyperactivity disorders. 2 Difficulty concentrating, remembering, and making decisions is a possible indicator of mental health problems. 3 Throughout the past couple of decades, health behaviors such as physical activity and diet,4,5 in addition to other health behaviors such as smoking, 6 alcohol consumption, 7 and sleeping have all been shown to correlate with health outcomes in adolescents. 8 Observed benefits of meeting various health behavior guidelines include lowered cardiometabolic disease risk and improved cognitive benefits leading to improved academic achievement.9,10 Lately, there has been a number of studies examining how meeting guidelines of multiple salient health behaviors may contribute to better health outcomes.11,12 However, many of these studies use small nonprobability samples of adolescents and/or focus on defined outcomes that may not contribute to the multiple domains of an adolescent’s life. Fortunately, the National Youth Risk Behavior Survey (YRBS) provides data from a representative sample of US adolescents that can be used to relate health behaviors with outcomes that may span the psychomotor, cognitive, and affective domains. 13
Previous studies have found associations between health behaviors and academic achievement (eg, grades, grade point average),5,14 and it has also been shown that meeting multiple health behavior guidelines associates with even better academic achievement.15,16 However, the link between salient health behaviors and mental health pertaining to concentrating, remembering, and decision making has yet to be explored. Difficulty concentrating, remembering, and making decisions may lead to disruptive behaviors in the academic classroom, 17 relate to poorer cognitive functioning, and may also lead to emotional problems such as anxiety, depression, and impulsivity that may contribute to risk behaviors that decrease health and lower overall quality of life. 18 Thus, difficulty concentrating, remembering, or making decisions may not only contribute to constructs within the cognitive domain, including executive function (ie, working memory, mental flexibility, and inhibition), but also to variables within the affective domain, which supports the importance of identifying contributing behavioral factors. To the author’s knowledge, no study to date has examined the relationship among multiple health behaviors and mental health, specifically difficulty concentrating, remembering, and/or making decisions, in a large representative sample of US adolescents. Therefore, the purpose of this study was to examine the associations among physical activity, select dietary behaviors, and other salient health behaviors such as smoking, alcohol consumption, and sleeping behaviors with self-reported adolescent mental health on the 2017 National YRBS. A secondary aim was to examine the association between meeting multiple health behavior criteria on self-reported adolescent mental health and the modifying effects of age and sex. Adolescent age and sex are related to health behaviors, 19 such as physical activity,20,21 and mental health. 22 Habitual physical activity tends to decrease with age and girls tend to participate in less physical activity compared with boys.23,24 Furthermore, girls tend to have greater mental health problems (eg, anxiety, depression) in adolescence compared with boys.25,26 Therefore, it is possible that either age or sex has a modifying effect on the relationship between health behaviors and mental health. It was hypothesized that meeting most positive health behavior criteria and meeting multiple positive health behavior criteria would associate with lower odds of an adolescent reporting having difficulty concentrating, remembering, and making decisions. It was also hypothesized that age and sex would both modify the relationship between health behaviors and difficulty concentrating, remembering, and making decisions.
Materials and Methods
Participants
Data were collected in 2017 and analyzed in 2019. A multistage cluster sampling procedure was used to yield a representative sample of US adolescents recruited from the 9th through 12th grade. The target population consisted of all public, Catholic, and other private school US adolescents from grades 9 through 12. A weighting factor was applied to each adolescent to adjust for nonresponse and the oversampling of Black and Hispanic students. The final weights were scaled so the weighted count of students was equal to the total sample size, and the weighted proportions of students in each grade matched population projections. 27 The National YRBS has been approved by the Centers for Disease Control and Prevention’s Institutional Review Board.
All regular public, Catholic, and other private school students in the 50 states and the District of Columbia were included in the sampling frame. Schools were selected systematically with probability proportional to enrollment in grades 9 through 12 using a random start. One hundred and ninety-two schools were sampled and 144 of the 192 sampled schools participated (75% response rate). All classes in a required subject or all classes meeting during a particular period of the day were included in the sampling frame. Systematic equal probability sampling with a random start was used to select classes from each school. The number of sampled adolescents was 18 324 with 14 765 of the 18 324 sampled students submitting questionnaires with usable data (81% response rate). The overall response rate (school response rate × student response rate) was 60%. 19
Youth Risk Behavior Survey Procedures
YRBS questionnaires were self-administered and adolescents recorded responses on a computer-scannable questionnaire booklet or answer sheet. Local procedures for obtaining parental permission were followed before administering YRBS at any school. Trained data collectors traveled to each participating school to administer the questionnaires. The data collectors read a standardized script to participating students explaining the YRBS. All procedures for the YRBS were designed to protect student privacy by allowing anonymous and voluntary participation. Students completed the self-administered questionnaire during one class period and recorded their responses directly on the computer-scannable booklet or answer sheet. When possible, the students’ desks were spread throughout the classroom to minimize chances of seeing another student’s responses. To increase student response rates, students who were absent during the YRBS had the option to complete the questionnaire if privacy was maintained. 26 Most questions on the YRBS have shown to have a high degree of test-retest reliability with kappa (κ) = 61% to 100%. 28
Data Processing
The outcome variable was the binary response item Q98 on the National YRBS that asked “Because of a physical, mental, or emotional problem, do you have serious difficulty concentrating, remembering or making decisions?” The response for item Q98 was numerically coded 1 = Yes and 0 = No. Three sets of predictor variables were analyzed consisting of physical activity behaviors, selected dietary behaviors, and other salient lifestyle behaviors consisting of smoking, alcohol consumption, and sleeping habits. To facilitate ease of interpretation, and to facilitate analyses of meeting multiple health behavior criteria, all predictor variables’ responses were dichotomized. Physical activity was assessed using item Q79 on the National YRBS that asked “During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day? (Add up all the time you spent in any kind of physical activity that increased your heart rate and made you breathe hard some of the time.).” Categorical responses included 0 to 7 days. Because of the national recommendations for children and adolescents to participate in at least 60 minutes of physical activity per day, 29 the responses were dichotomized into 1 = meeting 60 minutes per day and 0 = not meeting 60 minutes per day.
Dietary variables consisted of an item regarding consuming breakfast (Q78) that asked “During the past 7 days, on how may days did you eat breakfast?” and an item consisting of vegetable consumption (Q75) that asked “During the past 7 days, how many times did you eat other vegetables? (Do not count green salad, potatoes, or carrots.).” The breakfast predictor was dichotomized into 1 = consuming breakfast every day and 0 = not consuming breakfast every day to indicate if an adolescent consumed breakfast every day, and the vegetable predictor variable was dichotomized into 1= consuming vegetables at least 3 times per day and 0 = not consuming vegetables at least 3 times per day to indicate whether an adolescent consumed vegetables multiple times per day. 30
The final set of predictors consisted of an item regarding smoking behaviors (Q38) that asked “During the past 30 days, on how many days did you smoke cigars, cigarillos, or little cigars?”, an item regarding alcohol consumption (Q42) that asked “During the past 30 days, on how many days did you have at least one drink of alcohol?”, and an item regarding sleeping behaviors (Q88) that asked “On an average school night, how many hours of sleep do you get?”. Responses were dichotomized into 1 = smoking within the past 30 days and 0 = not smoking within the past 30 days to indicate any recent smoking behaviors, 1= consuming alcohol within the past 30 days and 0 = not consuming alcohol within the past 30 days to indicate any recent consumption of alcohol, and 1= sleeping at least 8 hours per day and 0 = not sleeping at least 8 hours per day to indicate if the adolescent met the minimum recommended hours of sleep. 31
Statistical Analysis
A probability weight based on an adolescent’s sex, race/ethnicity, and grade level was applied to each adolescent to adjust for school and student nonresponse and the oversampling of Black and Hispanic students. The complex survey design, including assigned stratum and primary sampling unit, was accounted for using STATA’s “svyset” prefix command. Missing data were not imputed. Weighted analyses used the Taylor Series Linearization variance estimation. For all categorical descriptive variables, unweighted and weighted prevalence statistics were reported. To examine the associations among physical activity, selected dietary behaviors, and other salient health behaviors consisting of smoking, alcohol consumption, and sleeping behaviors, weighted logistic regression models were employed. Predictors were entered into the models using block-wise entry. Model 1 consisted of the physical activity predictor, model 2 consisted of the model 1 predictor and dietary behavior predictors, model 3 consisted of the model 2 predictors and the predictors of smoking, alcohol consumption, and sleeping habits, and model 4 consisted of the predictors from Model 3 with the addition of age, sex, body mass index (BMI) percentile, and race/ethnicity. The added variables in model 4 were controlled for because they could potentially confound the relationship between health behaviors and difficulty concentrating, remembering, and making decisions. Socioeconomic status was not controlled for because it was not collected by the National YRBS. Communication of the results consisted of reporting the unadjusted and adjusted odds ratios (ORs) with corresponding 95% confidence intervals (CIs).
Secondary analyses consisted of examining the relationship between meeting multiple health behavior criteria and the odds of reporting mental health problems. A multiple health behavior composite variable was derived by adding counts of health behavior met across all observed binary predictor variables. For this analysis, the smoking and alcohol consumption binary variables were reverse coded so that 1 = positive met heath behavior (eg, not smoking). A weighted logistic regression model was then run using this derived health behavior composite as the primary predictor, adjusting for BMI percentile and race/ethnicity. Age and sex were tested as effect modifiers by deriving 2-way interaction terms with the health behavior composite variable. Predicted marginal probability plots were derived to visually communicate significant trends across the number of positive met health behaviors. All analyses had an alpha level of P < .05 and were carried out using STATA v15.0 statistical software package (College Station, TX, USA).
Results
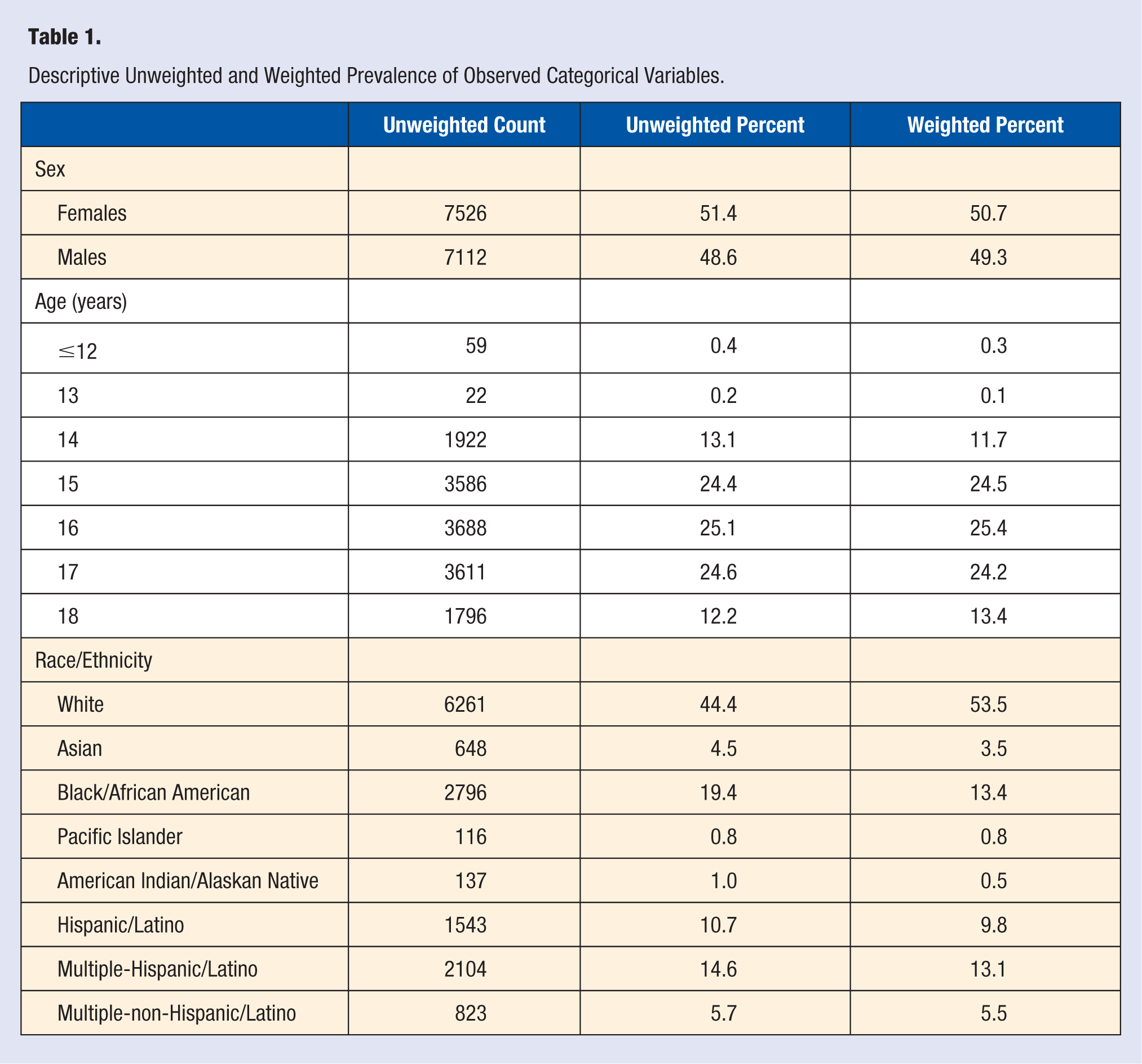
Table 1 displays the unweighted and weighted prevalence of sex, age, and race/ethnicity. The unweighted prevalence of adolescents reporting mental health problems was approximately 32.3% of the sample (10 668 adolescents; 4097 nonresponse) and the weighted prevalence was 32.0%. Of adolescents who reported mental health data (Q98), <1% missing data was present for each predictor except for alcohol consumption where missing data = 12.6%. Table 2 reports the parameter estimates for the weighted logistic regression models. Adolescents reporting being physically activity all 7 days during the week for 60 minutes per day significantly associated with lower odds of reporting mental health problems (P < .001). This relationship held controlling for other health behaviors and potential confounding variables (P = .013). Other health behaviors significantly relating to lower odds of reported mental health problems included consuming breakfast everyday (P < .001) and sleeping at least 8 hours per day (P < .001). Health behaviors significantly relating to higher odds of reported mental health problems included smoking at least once in the past 30 days (P < .001) and consuming alcohol at least once in the past 30 days (P < .001). Neither age nor BMI percentile related to self-reported mental health problems. Being male was significantly related to lower odds of reporting mental health problems compared to females (p < 0.001). Concerning the race/ethnicity strata, adolescents reporting being multiple races for both Hispanic (P = .003) and non-Hispanic (P = .006) ethnicities significantly related to higher odds of reported mental health problems compared with Whites.
Descriptive Unweighted and Weighted Prevalence of Observed Categorical Variables.
Parameter Estimates From the Weighted Multiple Logistic Regression Model. a
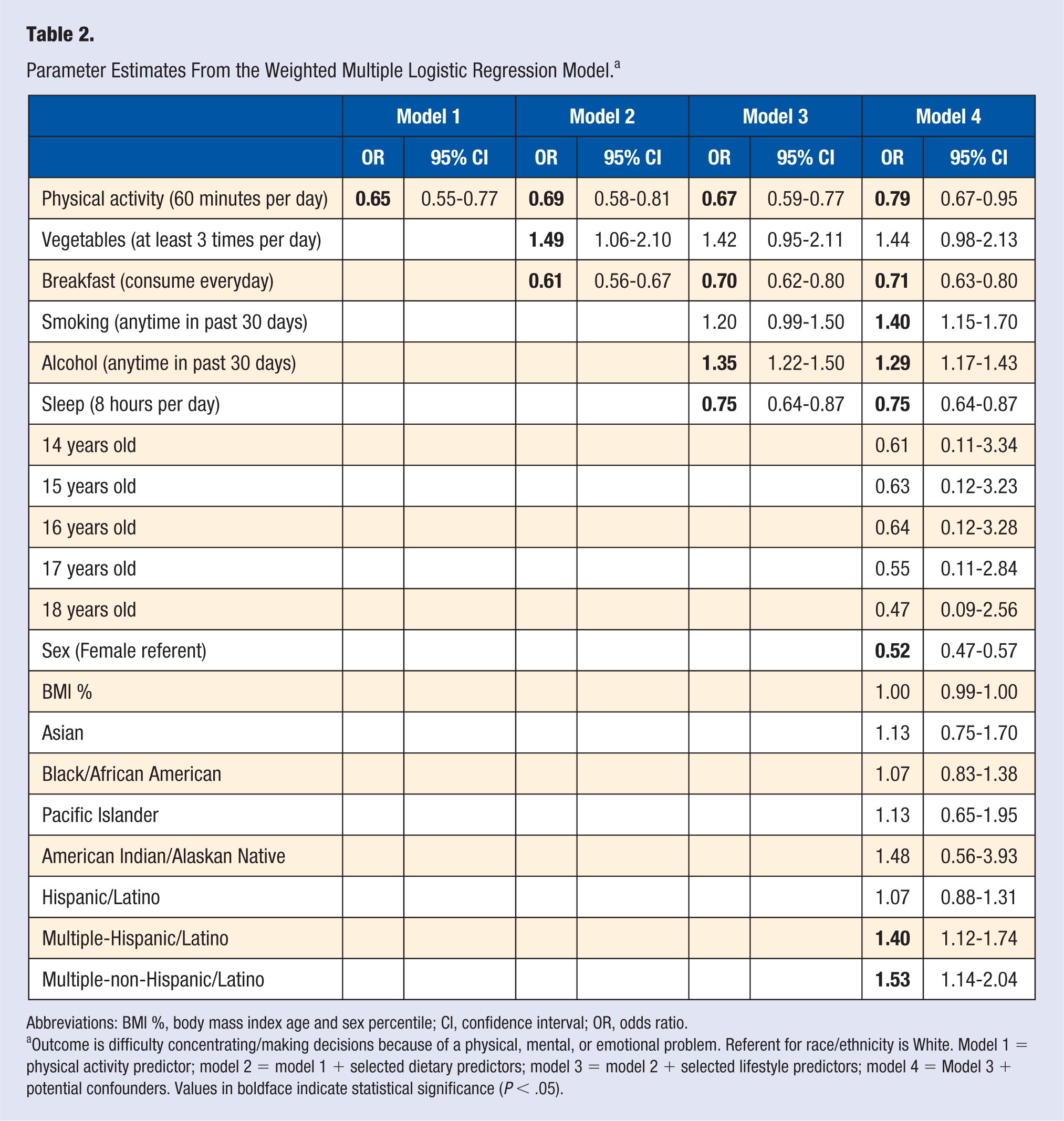
Abbreviations: BMI %, body mass index age and sex percentile; CI, confidence interval; OR, odds ratio.
Outcome is difficulty concentrating/making decisions because of a physical, mental, or emotional problem. Referent for race/ethnicity is White. Model 1 = physical activity predictor; model 2 = model 1 + selected dietary predictors; model 3 = model 2 + selected lifestyle predictors; model 4 = Model 3 + potential confounders. Values in boldface indicate statistical significance (P < .05).
The associations regarding meeting multiple health behavior criteria were also explored. For every one additional met health behavior, there were significantly lower odds of an adolescent reporting mental health problems (OR = 0.73, 95% CI 0.68-0.78, P < .001). This relationship was slightly modified by sex, as males displayed a stronger health behavior protective effect on mental health problems (OR = 0.67, 95% CI 0.62 – 0.73, p < 0.001) compared with females (OR = 0.81, 95%CI 0.75-0.87,P < .001). Figures 1 and 2 display the marginal predicted probabilities on the relationship between met health behavior and self-reported mental health problems.
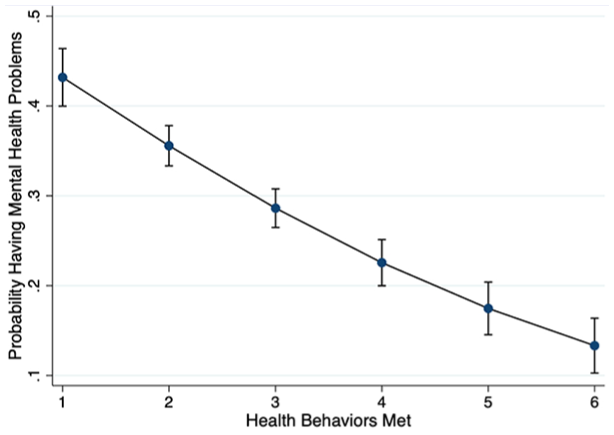
Marginal predicted probabilities of having mental health problems as a function of the number of met self-reported health behaviors.
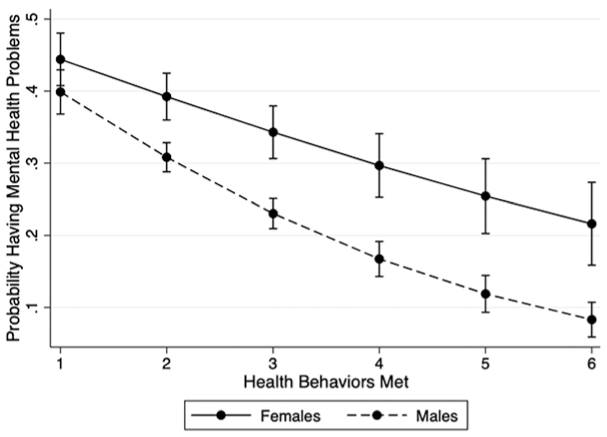
Marginal predicted probabilities of having mental health problems as a function of the number of met self-reported health behaviors, moderated by sex.
Discussion
The purpose of this study was to examine the associations among physical activity, dietary behaviors, and other salient health behaviors such as smoking, alcohol consumption, and sleeping with self-reported adolescent problems in concentrating, remembering, or making decisions on the 2017 National YRBS. Most salient health behaviors significantly related to adolescent mental health and meeting multiple health behavior criteria significantly relates to adolescents’ self-reported mental health. The latter relationship was slightly modified by sex. Interpretation of these findings and practical implications are discussed further.
Several health behaviors in the current study were shown to independently associate with mental health in adolescents. Physical activity, or any bodily movement to increase caloric expenditure above resting levels, is a salient behavior consistently linked to mental health. 32 School-based programming to improve physical activity has been shown to improve classroom behavior.33,34 Physical activity may provide a means to moderate psychological arousal, which may have a positive effect on classroom behavior and learning. 35 Physical activity may improve attention span and working memory by altering the neurochemicals serotonin, dopamine, norepinephrine, in addition to brain-derived neurotrophic factor, synaptic proteins, and insulin-like growth factor–1. 35 Hyperactivity in students and its associated disruptive behaviors in classroom settings may also be attenuated by physical activity’s ability to improve inhibitory control. 36 Given the results of the current study, independent of other health behaviors, physical activity has a robust association with adolescent mental health.
Breakfast consumption was also linked to mental health in adolescents. There is evidence that habitual breakfast consumption has a positive effect on children’s academic performance, especially on mathematic and arithmetic grades. 37 An increased frequency of habitual breakfast was consistently positively associated with academic performance. 37 In adults, it has been shown that memory, attention, and executive function show a small but robust improvement after consuming breakfast. 38 Studies in the pediatric population echo these findings, but may be confounded by breakfast type. 39 Regarding the other observed health behaviors, both smoking and consuming alcohol independently associated with mental health. Both smoking and alcohol consumption have been shown to alter an adolescent’s brain development, which affects short and long-term memory and decision making. 40 Some of these physiological alterations may be irreversible. 41 Smoking may affect cognitive functioning by reducing gray matter volume. 42 Meanwhile, chronic alcohol use is related to neuronal damage and reduced neurogenesis. 43 It should be noted that smoking and consuming alcohol may have a bidirectional reciprocal relationship with mental health. Including the current study, most research exploring these relationships are cross-sectional, 44 which precludes directionality and causal influences. However, it can be postulated that poor mental health leads to adverse risk behaviors such as smoking and alcohol consumption in addition to smoking and alcohol consumption influencing mental health problems. Sleep was the final health behavior examined that showed a significant independent relationship with mental health. The relationship between sleep quantity and quality and cognitive performance has been well studied. 45 Given that rapid eye movement sleep’s important role in selective facilitation of affective memories and preserve previously learned implicit knowledge, the major implication for adolescents is that preserving normal overnight sleep architecture appears critically important for successful physical, cognitive, and psychological functioning. 46
This study shows a robust relationship between meeting multiple health behaviors and lower odds of reporting mental health problems, a relationship that is slightly affected by sex. The relationship between meeting multiple positive health behaviors and mental health was slightly stronger in boys compared with girls. Therefore, interventions targeting multiple health behaviors to improve mental health may be slightly more effective for boys than girls. However, given the small magnitude of these effect modification differences, the practical significance may be negligible. Nevertheless, interventions or programs that focus on multiple behaviors may be significantly more effective at improving an adolescent’s cognitive functioning than targeting a single health behavior. There is longitudinal evidence showing that individuals that have no healthy behaviors from early to late midlife have significantly higher probability of poor executive functioning than those that engage in 3 to 4 healthy behaviors across the same time span. 47 Unfortunately, studies focusing on multiple health behaviors and outcomes related to concentration, memory, or making decisions in adolescents are sparse. Because adolescence is characterized by physical and cognitive changes in addition to emotional variability that can negatively affect quality of life, 48 multibehavioral change interventions targeting this population have substantial merit. Multicomponent interventions targeting multiple levels of the social-ecological model may yield positive benefits on improving multiple health behaviors and subsequently mental health in adolescents. Programs like Comprehensive School Physical Activity Programs (CSPAPs) have been shown to correlate with improved physical activity behaviors and classroom behavior in youth49,50; however, use of the theoretical framework employed by programs like CSPAP to improve other health behaviors such as diet, sleeping, and refrainment from the consumption of substances such as alcohol and nicotine may have potential to have an additive effect on the mental health of adolescents.
It has been proposed that the relationship between health behavior and executive function in adolescents may be bidirectional. Allan et al 51 communicated that executive function supports the volition, planning, performance monitoring, and inhibition necessary to enact intentions and override urges to engage in health damaging behavior. Mounting evidence suggests that health behaviors can not only induce improvements in executive function but that executive function links to the consistent performance of health-promoting behaviors and the avoidance of health risk behaviors. 51 Because of these potential interdependent nonrecursive pathways, it is potentially even more imperative to stress the importance of meeting multiple health behaviors in adolescents because of this positive feedback mechanism. That is, cognitive function sustains health behaviors which themselves protect cognitive function and physical health as individuals advance into older age. 52 However, empirical evidence examining multivariate bidirectional relationships in adolescents have been largely unexplored and should be a priority in future research.
There are limitations to this study that must be considered before the results can be generalized. First, the study design was cross-sectional, therefore no causal inferences can be made. Second, all variables were collected using self-report, therefore there is potential for recall and social desirability bias. Third, all predictor variables were dichotomized; more specific information may have been obtained if the entire scales were used for analysis. This is especially pertinent for the risk behavior predictor variables (eg, smoking and alcohol consumption), as there may be significant variability in mental health risk between adolescents who engage in the behaviors only one time per month compared with adolescents who engage in these behaviors every day. Fourth, only 2 moderators of effect were examined; future research should examine the relationships with mental health with other variables which may contribute to effect modification. Finally, mental health is a construct that can be operationally defined in many ways. The use of only one item to assess mental health is not ideal and should be assessed using multiple items to improve the construct’s psychometric characteristics. Furthermore, anxiety and depressive symptoms were not examined and contribute to mental health. The results do not generalize past the self-reporting of difficulty concentrating, remembering, or making decisions.
In conclusion, salient health behaviors and meeting multiple health behavior criteria associates with an adolescent self-reporting difficulty concentrating, remembering, or making decisions on the 2017 National YRBS. Sex slightly modified the relationship between meeting multiple health behavior criteria and the self-reporting of mental health. This is the first study to examine these relationships using a representative US sample of adolescents, supporting strong external validity evidence to the US adolescent population. These observed relationships can be used to develop and justify programs aiming to change multiple health behaviors. School and community-based behavioral interventions targeting multiple health behaviors may impact how adolescents concentrate, remember, and make decisions, which may further influence cognitive and emotional outcomes that improve overall quality of life.
Footnotes
Acknowledgements
The authors would like to thank the data collection personnel and the adolescents who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.