
Abstract
Of nearly 800 000 strokes that occur annually, 23% are recurrent events. Risk for disability and mortality is higher following a recurrent stroke than following a first-time stroke, which makes secondary stroke prevention a priority. Many risk factors for stroke are modifiable and amenable to improvement through lifestyle modification. Lifestyle modification can be difficult for people with stroke, however, in part because of stroke-related physical and cognitive deficits. Despite these challenges, risk factor management through lifestyle modification is important. This article reviews the multiple cardiovascular and metabolic benefits associated with the modification of several lifestyle behaviors: diet, physical activity, smoking cessation, and alcohol consumption. Health behavior theories and existing lifestyle intervention programs are also reviewed to identify important behavioral and cognitive skills that can be used to facilitate modification of health behaviors, and practical skills and suggestions for health care providers are provided.
‘Although risk factor management through pharmacological intervention is often necessary, polypharmacy can result in a high treatment burden for people with stroke and carries added risk for morbidity and mortality.’
Introduction
A history of having a prior stroke increases the risk for experiencing a future stroke and concomitant mortality and disability. Of the 795 000 strokes that occur annually, 185 000 (23%) are recurrent events. 1 Following a first-time stroke, the estimated risk for stroke recurrence is 13% to 16% within the first year and 4% every year thereafter. This results in an elevated risk of 30% by 5 years 2 and 43% by 10 years. 3 In addition to these population-level risks, the impact of stroke recurrence on individuals can be severe. The risk of death in the 30 days following a recurrent stroke ranges from 23% to 41%, and the risk of new disability ranges from 39% to 53%.2-5 Such increased risk for mortality and disability should make secondary stroke prevention a priority, which can be addressed in part through risk factor management.
Risk Factors in People With Stroke
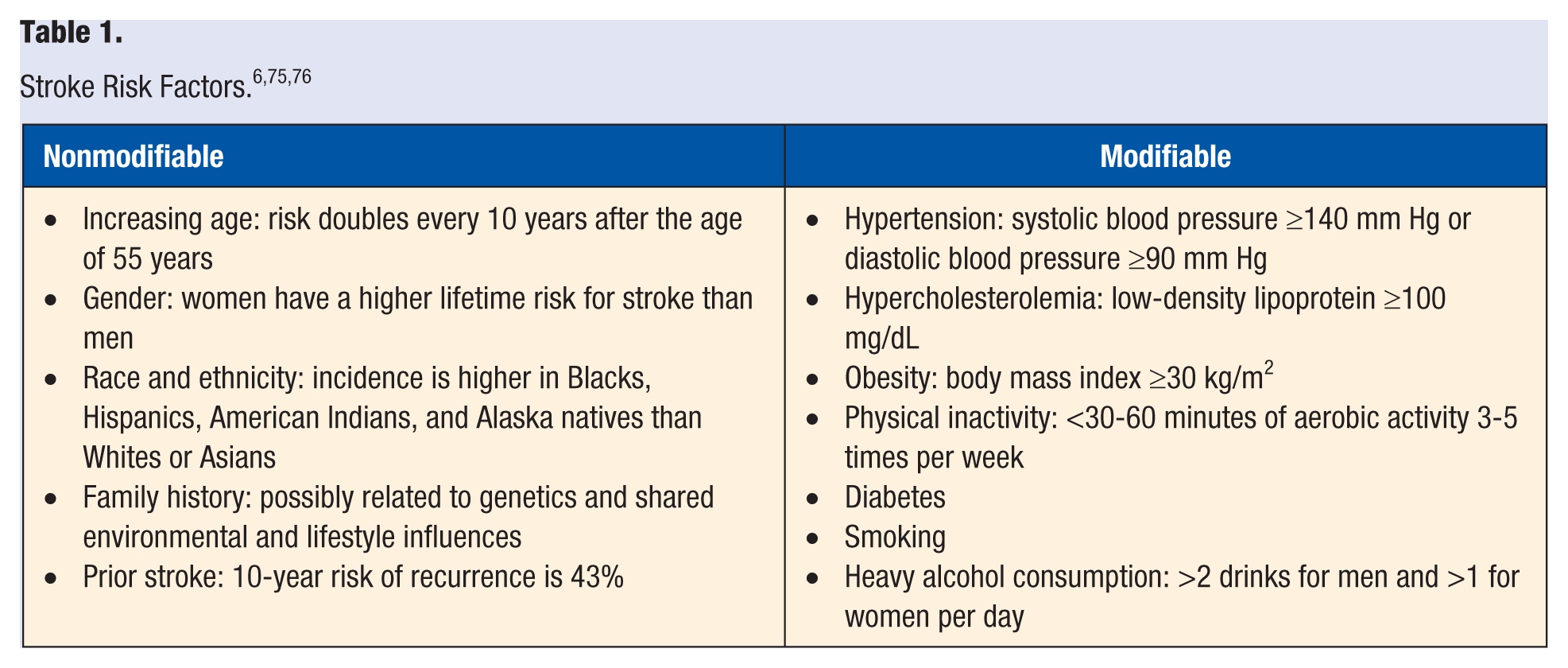
Although secondary stroke prevention through risk factor management has not been extensively studied, the evidence for primary stroke prevention is strong. It is generally accepted that risk factors for first-ever and recurrent ischemic stroke are the same (Table 1). 6 Many modifiable risk factors occur in people with stroke and often go unmanaged. 7 In one sample of community-dwelling adults with stroke, 99% had 1 unmanaged risk factor, and 91% had 2 or more unmanaged risk factors. 8 This is concerning because risk for cardiovascular mortality is 1.6 and 3.1 times higher in people with 1 and 2 unmanaged risk factors, respectively, compared with people with managed risk factors. 9 Risk factor management is, therefore, important for people with stroke.
Lifestyle Modification
Although risk factor management through pharmacological intervention is often necessary, polypharmacy can result in a high treatment burden for people with stroke 10 and carries added risk for morbidity and mortality. 11 In recent years, the American Heart Association has published numerous guidelines directed at health care professionals for the management of cardiovascular risk factors, 12 primary stroke prevention, 13 acute management of stroke, 14 and secondary stroke prevention. 6 Each of these guidelines has identified lifestyle modification as a core component of risk factor management that should be implemented as part of comprehensive poststroke care.
Lifestyle modification can lead to improvements in hypertension, hypercholesterolemia, obesity, and glucose metabolism in diabetics, which are in turn associated with decreased risk for cardiovascular disease and death. 15 In fact, the rate of cardiovascular mortality in people with stroke over a 10-year period can be reduced by 85% to 92% by engaging in lifestyle behaviors such as eating sufficient fruits and vegetables, exercising, maintaining a body mass index between 18.5 and 29.9 kg/m2, moderate alcohol consumption, and not smoking. 16 Clearly, modification of lifestyle behaviors is important for secondary stroke prevention. The sections below will explore how modification of individual lifestyle behaviors can affect multiple risk factors.
Diet
Consuming a healthy diet is important for cardiovascular health and stroke prevention. In 2013, the American College of Cardiology and American Heart Association published lifestyle management guidelines to reduce cardiovascular risk. 12 The dietary recommendations are consistent with DASH- 17 and Mediterranean-style 18 dietary patterns, which are effective in reducing the risk of stroke.19-21 The recommendations encourage the intake of fruits, vegetables, whole grains, low-fat dairy products, poultry, fish, legumes, vegetable oils, and nuts; limited consumption of sweets, sweetened-beverages, and red meats; and reduced sodium intake.
Multiple benefits from adhering to these dietary patterns have been observed. Blood pressure and low-density lipoprotein (LDL) cholesterol can be reduced.6,12 Improved glycemic control and insulin sensitivity occurred in diabetics.22,23 Weight loss resulted in decreased rates of obesity, 24 which is important because of the strong relationship between obesity and stroke.1,25 Another important dietary consideration is calorie intake. Reduction of daily caloric intake by 20% to 25% for 3 months or longer in obese and nonobese individuals resulted in improved blood pressure, LDL cholesterol and triglycerides, insulin resistance, and glycemic control.26-29 Selecting healthy foods and consuming appropriate amounts can positively affect risk factors for recurrent stroke.
Physical Activity
Physical inactivity is a significant risk factor for stroke. 1 Unfortunately, people with stroke spend up to 86% to 88% of their time in sedentary activity compared with 57% to 72% in adults without stroke. 30 One reason for decreased physical activity after stroke is diminished exercise capacity, as measured by maximal oxygen uptake (ie, VO2max). The amount of oxygen consumed during routine walking in people with stroke is twice that of adults without stroke; and performance of self-care activities such as bathing, grooming, and dressing after stroke can require individuals to exert 66% to 75% or more of their total exercise capacity. 31 This illustrates how once-simple tasks become challenging after stroke. Additional barriers to physical activity after stroke include deconditioning, depression, inaccessible environments (eg, wheelchair-friendly transportation and gym equipment), low motivation, poor social support, and physical impairment. 32
Despite these challenges, physical activity is critical. Moderate to vigorous physical activity for primary stroke prevention leads to decreased blood pressure, LDL cholesterol, and weight gain and increased weight loss.1,6,12 It also results in increased glucose uptake and insulin sensitivity in people with and without diabetes.33,34 For people with stroke, exercise training can improve hypertension, lipid profiles, glucose metabolism, and insulin sensitivity.35,36 These latter improvements are important because up to 80% of people with stroke experience abnormal glucose metabolism. 36 Additional benefits of exercise training after stroke include improved balance, gait speed, and endurance and decreased disability. 37
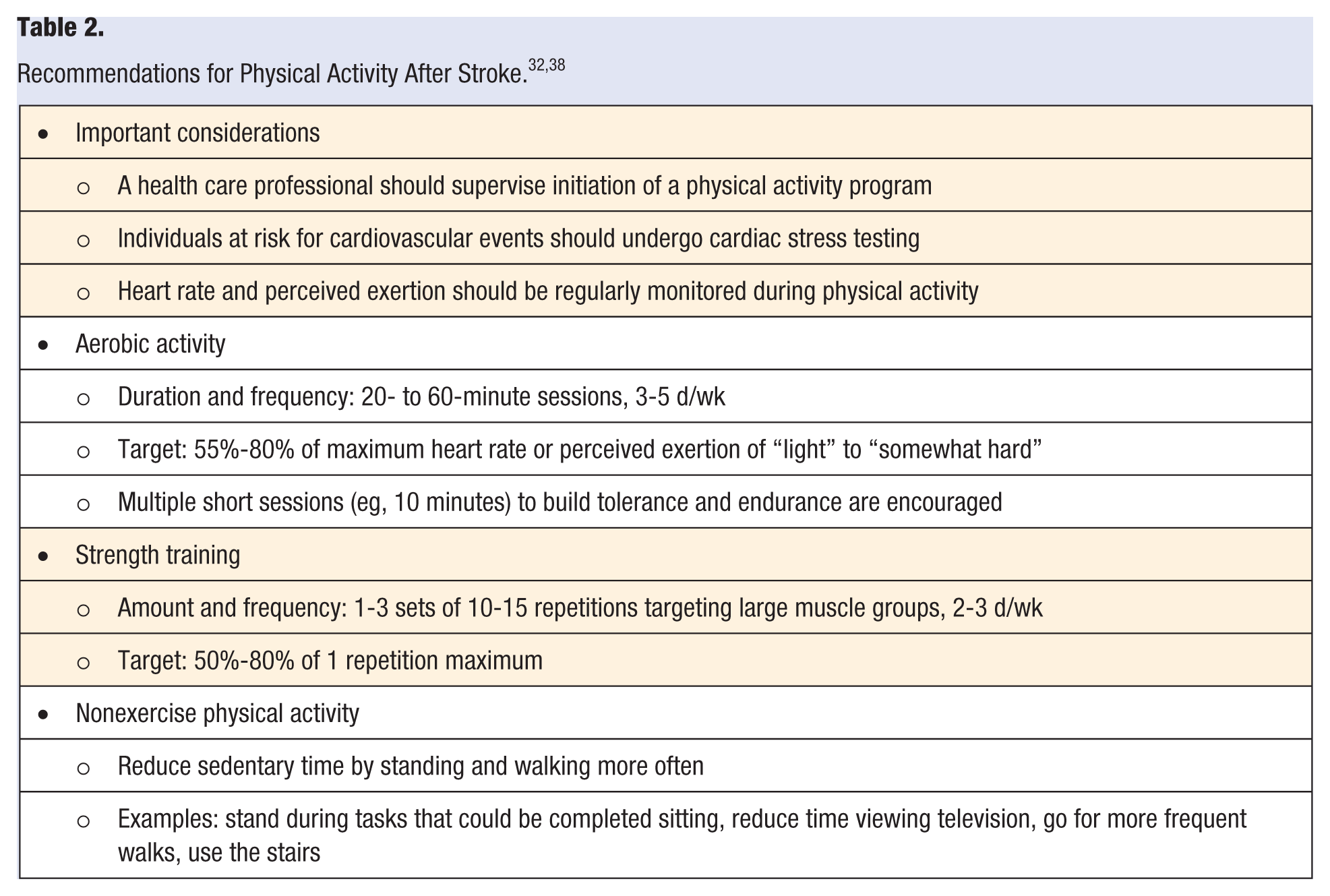
Because of the challenges associated with deconditioning and physical impairment after stroke, the American Heart and American Stroke Associations have established guidelines for health care professionals that outline physical activity and exercise recommendations after stroke (summarized in Table 2). 32 In addition to increasing physical activity, sitting and other sedentary behaviors should be reduced by performing more light-intensity, nonexercise physical activity, such as standing and walking. 38 Important considerations for increasing physical activity after stroke include cardiac and stress testing for high-risk individuals and supervision by a trained professional when initiating a new exercise program. Physical and occupational therapists should be involved in designing physical activity programs after stroke because these professionals have the necessary training and experience to teach people with stroke how to safely increase physical activity levels.
Smoking
The risk for first ischemic stroke in smokers is nearly 4 times the risk in nonsmokers. 39 Although information on the risk for recurrent stroke is limited, one study demonstrated that the risk of recurrent stroke in elderly smokers was double that of nonsmokers. 40 Smoking results in acute increases in heart rate, blood pressure, and arterial stiffness,41,42 which are especially dangerous for individuals with hypertension. Furthermore, smoking is associated with insulin resistance and dyslipidemia. 43
Smoking cessation, however, can lessen the risk for stroke. Smokers who quit reduce their risk for ischemic stroke by half, and smokers with hypertension who quit experience a greater benefit compared with smokers without hypertension. 39 Chronic smokers who quit smoking experience decreased blood pressure, heart rate, and arterial stiffness44,45 and increased high-density lipoprotein (HDL) cholesterol. 46 Additionally, diabetic smokers who stop smoking experience improved glycemic control, blood pressure, LDL cholesterol, and insulin resistance. 47 Because of the multiple risk factors that can be improved through smoking cessation, people with stroke who smoke, and especially those with hypertension, should be given encouragement and resources to stop.
Alcohol Consumption
Heavy alcohol consumption increases the risk for first-ever and recurrent stroke.48,49 Although the exact mechanisms are unknown, heavy alcohol consumption is associated with increased risk for hypertension and diabetes,50-53 which are major risk factors for stroke and cardiovascular disease.
Low to moderate alcohol consumption, defined as ≤2 drinks for men and ≤1 drink for women daily, 6 is associated with reduced risk for first-ever stroke. 48 Although further research is needed, it is possible that low alcohol consumption may reduce cardiovascular risk by decreasing hypertension 51 or increasing HDL cholesterol. 54 Reducing current levels of alcohol consumption can lead to decreases in blood pressure, with greater reductions occurring in individuals with higher pressures, which has important implications for reducing stroke risk in hypertensive individuals. 55 Additionally, the incidence of diabetes is lower in individuals with low alcohol consumption than in those with heavy consumption. 53 Notwithstanding these potential benefits, the American Heart and Stroke Associations do not currently recommend drinking alcohol to gain cardiovascular benefits. 6
As observed with other health behaviors, modifying the amount of alcohol consumed can influence multiple risk factors for cardiovascular disease. This makes alcohol consumption a potential target for secondary stroke prevention. Because of the risk for alcohol dependence, however, individuals who do not drink should not be encouraged to drink. 6
Lifestyle Behavior Intervention
Behavior change is challenging and often difficult to sustain because of complex personal, environmental, and social factors. Health behavior theories have been developed to explain how these factors influence the adoption and modification of specific health behaviors, and intervention programs have been developed that utilize these theories to help patients modify lifestyle behaviors across patient populations and settings.
Barriers
A common barrier to behavior change for patients is limited insight, knowledge, and awareness of how lifestyle factors contribute to risk for subsequent stroke. 56 If patients do not perceive a need to modify lifestyle behaviors, then behavior modification is unlikely. Even when patients understand the need to modify their behavior, knowledge rarely translates into behavior change because additional barriers exist. Limited self-efficacy (ie, one’s self-confidence in one’s ability to carry out a specific action), social support, outcome expectations, and motivation, among other factors, must also be considered. 57 Additionally, physical, cognitive, and emotional conditions, including depression, are common after stroke and affect a patient’s ability to enact lifestyle modifications.32,58
Health Behavior Theories
Several theories have been proposed to explain how health behaviors are acquired and how barriers to lifestyle modification can be overcome. Well-known theories include the Social Cognitive Theory and the Transtheoretical Model. 59 Social Cognitive Theory posits that health behaviors are influenced by interactions among environmental, social, and personal (eg, cognition, affect, biology) factors. Self-efficacy is the main component of the theory and often targeted for intervention by helping patients set small, achievable goals and helping patients observe and learn from their peers. Self-regulation strategies can also be utilized to enhance self-efficacy and promote lifestyle modification. Examples of self-regulatory strategies include systematic observation of one’s behaviors (ie, self-monitoring using a food or exercise log), self-reward, enlistment of social support, and modification of social and physical environments to facilitate specific behaviors.
The Transtheoretical Model, also called the Stages of Change Model, describes behavior modification in terms of 5 stages of motivational readiness to change behavior. 59 In the first 2 stages—precontemplation and contemplation—behavior change may be absent or considered, respectively. In the 3 remaining stages—preparation, action, and maintenance—behavior change has been attempted, implemented, or maintained, respectively. Several cognitive and behavioral strategies have been developed to help individuals modify health behaviors by progressing between stages. 60 Examples of these strategies include increasing awareness about a person’s behavior with respect to a given health condition, assessing how one feels the benefits and costs of behavior change, learning to substitute healthy behaviors for unhealthy behaviors, enlisting social support, and removing stimuli of unhealthy behaviors while adding stimuli of healthy behaviors.
Lifestyle Modification Programs
Several lifestyle modification programs for managing cardiovascular risk factors have been developed and successfully implemented that utilize elements from Social Cognitive Theory and the Transtheoretical Model. The EUROACTION program for patients with coronary heart disease and their families consisted of 8 weekly instructional workshops taught by nurses. 61 Lifestyle behaviors and risk factors were addressed, including diet, physical activity, and smoking, using strategies from the Transtheoretical Model to help patients increase self-awareness and self-regulation of lifestyle behaviors. Following the intervention, improvements in waist circumference, blood pressure, blood cholesterol, dietary targets, and physical activity targets were observed. In the GOSPEL study for secondary prevention of myocardial infarction, participants received one-on-one counseling by a cardiac nurse, physiotherapist, and cardiologist. 62 The intervention consisted of lifestyle and risk counseling, preventive interventions, supervised exercise, and pharmacological treatment. Visits lasted 2 hours and were held once a month for the first 6 months, then every 6 months for 3 years, and family support was encouraged. At the end of the 3-year study, cardiovascular mortality and prescription of cardioprotective medications were reduced, and lifestyle behaviors (eg, exercise, diet, stress management, body weight) were improved.
A comprehensive lifestyle health coaching program (ie, INTERVENT) administered in clinical and community-based settings has also been effective in cardiovascular disease risk reduction.63,64 This program is delivered mainly over the telephone and internet and lasts for a minimum of 1 year. Trained health coaches follow a standardized program to help participants set behavior change goals, develop action plans, and implement action plans. Health coaching consists of one-on-one counseling sessions that last for 15 to 20 minutes, where participants are taught cognitive and behavioral strategies (eg, increasing knowledge, risk awareness, and self-efficacy and developing skills in self-monitoring, enlisting social support, and controlling stimuli). This program has been successfully delivered in hospitals, physician practices, work sites, and health centers and has led to improvements in blood pressure, cholesterol, weight, and cardiorespiratory function. The program has also been utilized in randomized controlled trials for primary (ie, CREST-2 65 ) and secondary (ie, SAMMPRIS66,67) stroke prevention.
Clinical Applications
The programs described above demonstrate the importance of intensive, long-term interventions that involve family and social support and that provide participants with the necessary knowledge, skills, and strategies for successful health behavior modification. For busy clinical practices, the time required to implement intensive health behavior interventions may be a barrier. 64 Additional barriers include limited reimbursement for preventive services, low outcome expectations that patients will comply with behavior prescriptions, and lack of provider self-efficacy in providing lifestyle intervention counseling. 68 Even though these factors are real barriers for providers, clinical guidelines are explicit about lifestyle modification for the prevention of cardiovascular disease and stroke.6,12-14 Suggestions for implementing clinical guidelines in the face of provider-related barriers are given below.
Meet the Patient “Where They’re At”
Although physicians and other health care providers are recognized as health experts, patients often resist being told what to do. 69 Therefore, it is important to meet patients “where they’re at” and provide them with information that is consistent with their current level of motivation. One strategy for doing so is to utilize motivational interviewing. Motivational interviewing is a patient-centered, collaborative approach to help patients become aware of their values and priorities, understand how current health behaviors act as barriers to or facilitators of values and priorities, and generate action plans for changing health behaviors. 70 Motivational interviewing has been extensively studied in the context of diet and physical activity. 71 In meeting patients at their current level of readiness to change behavior, patients may be less resistant and more open to discussing strategies for modifying lifestyle behaviors.
Provide Opportunities for Skills Training
Once patients are aware of the need to modify lifestyle behaviors and are willing to discuss strategies for behavior change, they must be given the opportunity to develop skills to ensure success. In addition to learning the cognitive and behavioral skills outlined in Social Cognitive Theory and the Transtheoretical Model, patients may also need to learn skills for performing specific health behaviors (eg, reading a nutrition label, preparing a meal, using gym equipment). It is unreasonable to expect that any one health care provider will be an expert in all these skills. One option, therefore, is to refer patients to commercial lifestyle behavior programs, such as those described in this article. Programs that are phone- or internet-based may be especially important for people with stroke, where stroke-related impairments may impede transportation.
Another option is to implement a multidisciplinary, team-based approach to managing health behaviors. Following an initial consultation with a physician, more intensive skills training and lifestyle counseling may be delegated to a nurse or health coach who works in a physician practice. In cases where patients require more specialized intervention, referral to a health psychologist may be appropriate. Physicians may also refer patients to physical therapy for the design and implementation of a home exercise program, a dietitian for education and training in selecting appropriate foods, and occupational therapy for skills training in meal preparation, increasing nonexercise physical activity, using adaptive equipment, and implementing compensatory strategies to overcome physical and cognitive impairments.
Patients may also learn skills from their peers, as emphasized by Social Learning Theory. Thus, participation in social groups that bring stroke survivors together may be beneficial. Stroke groups can be found using the American Stroke Association’s Stroke Support Group Registry: http://www.strokeassociation.org/STROKEORG/strokegroup/public/zipFinder.jsp.
Review Progress
Reviewing progress at regular intervals with patients can be an important way to provide feedback on patients’ behavior change efforts. 72 In the same way that self-monitoring provides feedback to patients about their behavior, reviewing progress during regularly scheduled appointments allows providers to provide feedback. Follow-up appointments also give patients the opportunity to discuss challenges to behavior change with providers, which may lead to much needed interventions or referrals.
Just as when initiating a conversation about behavior change, it is important to provide feedback that is consistent with a patient’s current level of readiness for behavior change. When patients are not aware of or are just beginning to think about the need to modify health behaviors, general feedback on the benefits of behavior change is appropriate. When patients are ready to make a change or are actively changing their behaviors, targeted feedback with specific information can be shared. Regardless of the feedback provided, the manner in which it is provided should be positive, genuine, and empathetic. 72
Opportunities for Future Research
There are many opportunities for future research on secondary stroke prevention through lifestyle modification. Few large-scale randomized controlled trials have been conducted that examine secondary stroke prevention as the primary outcome; for practical reasons, cardiovascular risk reduction has been the main outcome of interest. Small, nonrandomized studies have demonstrated an improvement in health behaviors and cardiovascular risk factors, but sample sizes have been too small to detect a reduction in stroke recurrence.73,74 Large-scale, randomized trials of lifestyle interventions for secondary stroke prevention are needed.
Effectiveness trials that examine primary care–based intervention are also needed. Because physicians are often the first point of contact for patients seeking help for chronic conditions, effective physician-based or physician-initiated interventions need to be developed and tested. It is also important that clinical and effectiveness trials examine interventions that result in long-term adherence in the form of lasting behavior change. Permanent behavior change is paramount for secondary stroke prevention, and additional research is needed to determine how lifestyle interventions can achieve this outcome.
Conclusion
Modifiable risk factors for recurrent stroke and cardiovascular disease are common in people with stroke. These risk factors often go unmanaged, which leads to increased risk for mortality and disability. Clinical guidelines recognize that lifestyle modification for risk factor management should be a priority following stroke. Improving diet, increasing physical activity, smoking cessation, and reducing alcohol consumption are specific health behaviors that should be targeted because of their effects on multiple cardiovascular risk factors.
Health behavior theories and lifestyle modification programs demonstrate that modification of health behaviors is possible through intensive, long-term interventions that elicit social support and provide individuals and families with a variety of skills. Lifestyle modification can be initiated in clinical practice environments and enhanced through referral to allied health care professionals or lifestyle intervention programs. Although behavior change is difficult, provider use of health behavior theories, implementation of cognitive and behavioral strategies, and refinement of communication skills may facilitate patients’ efforts at secondary stroke prevention through lifestyle modification.