
Abstract
Effective dietary interventions are vital for combating morbidity and mortality, necessitating reliable assessment tools. This article explores diverse dietary assessment methods, emphasizing their complexities and applications. Food Frequency Questionnaires (FFQs) offer insights into dietary habits over specified periods but require validation for target populations. Traditional Food Records provide detailed insights but are labor-intensive and prone to underreporting. Technology-based and technology-assisted records offer efficient alternatives, leveraging mobile apps and wearable sensors, albeit with access and privacy concerns. 24 hour Dietary Recall (24HR) methods capture detailed intake within a day, with traditional and technology-assisted approaches strengthening population studies. The Automated Multi-Pass Method (AMPM) and technology-assisted ASA24 represent traditional and contemporary 24HR methodologies, respectively, both yielding comprehensive dietary data. In conclusion, dietary assessments are crucial for understanding dietary patterns and health implications. Integration of novel technologies streamlines data collection and analysis, enhancing researchers’ ability to accurately gauge short- and long-term dietary impacts. Proper utilization of these tools empowers researchers to make informed decisions regarding dietary interventions and public health initiatives.
“Dietary assessments can assist researchers and others in linking diet and nutrition factors with key health outcomes.”
Introduction
Dietary risk factors are well recognized as important contributors to morbidity and mortality and as a result the development of interventions that address diet are of continued and growing interest. Often lifestyle interventions include a nutrition or dietary component, aimed at addressing a health outcome. For example, an intervention aiming to reduce obesity might include education on portion control. While the outcome of interest may be weight or obesity, diet typically represents an immediate and measurable change that can be utilized to assess intervention impact. However, dietary intake is highly complex as is assessing diet. There are many facets to measure in diet such as the timing of eating occasions, the quantities and types of foods and beverages consumed, nutrients consumed, and even the source of food (home, restaurants, etc). Further, when assessing diet further examination of usual or habitual eating patterns can be of interest, as can how intake of foods and nutrients might change over the lifespan or even across seasons of the year. As such, a variety of dietary assessment tools and methods have been developed and are currently being developed based on the goal of the assessment. Understanding the properties of each method is key to selecting a method that is appropriate to the task at hand. These will be discussed in detail in this article.
Food Frequency Questionnaire
The purpose of a food frequency questionnaire (FFQ) is to obtain information about how often and in some cases, the portion size, of the foods and beverages consumed by a person over a stated time period (usually past month or year). 1 FFQs contain a finite list of foods and beverages with response categories indicating the typical frequency of consumption. In some cases, additional questions are included with regards to typical portion sizes consumed for each food. FFQs can allow for estimation of total diet, usually requiring 80 to 100 foods, but can also be utilized to assess specific foods or nutrients. For example, FFQs designed to measure calcium intake, may include a list of only calcium containing foods. Whereas tools aiming to measure total diet quality would likely contain a longer and more exhaustive list of foods. FFQs are usually self-administered but can be interview-administered in cases where literacy is may be low. FFQs are linked with nutrient composition databases that allow the researcher to quantify nutrient intake for respondents.
Key to this method is that the FFQ must be developed and validated to the target population, age, geographic location, language, and culture, as these may impact the foods included on the list and thus the ability for the assessment tool to accurately estimate nutrient intake. A strength of these tools is their application in assessing diet and nutritional status of populations, as well as in estimating the impacts of an intervention on diet. However, FFQs can be cognitively challenging, requiring individuals to rely on memory to complete, which introduces some bias.
Food Records
Food records capture dietary intake usually over 1 to 3 days, and in real-time, to help evaluate dietary patterns and behaviors.2,3 Traditionally foods records were completed manually; however, with advances in technology, new methods have emerged including food records captured with mobile applications and sensors on wearable devices.4–7 Traditional, technology-based, or technology-assisted food records each have their strengths and weaknesses and are valuable tools in clinical medicine.
Traditional Written Food Records
Traditional foods records are recorded manually, for example, using pen and paper, in a journal or food diary and take at least 15 minutes to complete over the day.2,3 Individuals record all foods, beverages, and dietary supplements consumed, including details on the time of consumption, amount consumed, ingredients for recipes, and cooking methods, for example, boiled, or fried. Visual aids and scales can be used to help estimate portion size.2,3
The strengths of traditional food records include that they allow for self-monitoring of dietary intake, which can help enhance individuals’ awareness of their food intake and can assist with informing healthy behavior change.2,3 Weaknesses of these traditional methods are they are a time burden for individuals to complete, individuals need to be literate and motivated to complete them, food records are prone to underreporting of energy (kcal) intake, and they are a time burden to analyze.2,3
Technology-Based and Technology-Assisted Food Records
Technology-based food records include but are not limited to mobile systems (apps),4,5,8,9 and sensor device-based tools, where technology is the primary method for recording intake. 7 For example, through mobile applications like MyFitnessPal, 10 users can scan a barcode or their food using a smart phone camera which is used to automatically identify food and quantify food volume through artificial intelligence.8,10 Wearable sensor devices, such as eyeglasses (non-corrective or corrective lens) containing a mounted camera (e.g., the automatic ingestion monitor, AIM), are also under development for automatically identifying and quantifying food intake. 7 These are all non-self-report-based measurements which limit error introduced by the individual completing the record.
In comparison, with technology-assisted food records, technology is used to support more traditional methods of dietary assessment. Therefore, technology-assisted methods still rely on the user or a trained reviewer to complete the food record. For example, using a mobile app, like the PortionSize app, 11 an individual can capture images of their food and then the individual can identify the food and estimate the food volume, or the images can be sent to a trained reviewer for further analysis using a validated method like the Remote Food Photography Method (RFPM).11,12 The Automated Self-Administered 24-Hour (ASA24®) Dietary Assessment Tool is another technology-assisted food record which is freely available online and is a web-based tool. 13
Strengths of technology-based and technology-assisted food records are they may help to reduce the costs of collecting food records, reduce the user and researcher burden for completing and analyzing foods records, and may improve the efficiency and accuracy of dietary assessment.2,4–6 Because technology-based food records can be analyzed in real-time and provide immediate feedback on dietary intake, they can also be used to facilitate behavior change. 5 The ASA24 Dietary Assessment Tool provides a detailed nutrient report once the entire record is completed. 14 Weaknesses of these methods include access to technology (e.g., access to a smart phone), technical challenges (e.g., reliance on Internet connectivity), and privacy concerns with collecting sensitive dietary information.2,5,6
24-hour Dietary Recall (24HR)
24 hour dietary recall (24HR) is a methodology used to collect dietary information in the previous 24 hours or the previous day.15,16 A 24HR captures detailed information on all foods, beverages and supplements consumed including the time and amount consumed, and preparation methods. Visual aids can also be used to assist with portion size estimation.3,16,17 A 24HR can be used for assessing dietary intake of individuals and larger populations. Traditional 24HR include the Automated Multi-Pass Method (AMPM) which is used in the United States as part of the National Health and Nutrition Examination Survey (NHANES) to collect population based dietary information.18,19 Traditional 24HR require an interviewer to conduct a structured interview either in person or over the phone. 16 However, technology-assisted 24HR like ASA24 do not require an interviewer.14,16 Traditional and technology-assisted 24HR have their strengths and weaknesses, and both are valuable in clinical medicine.
Traditional 24HR
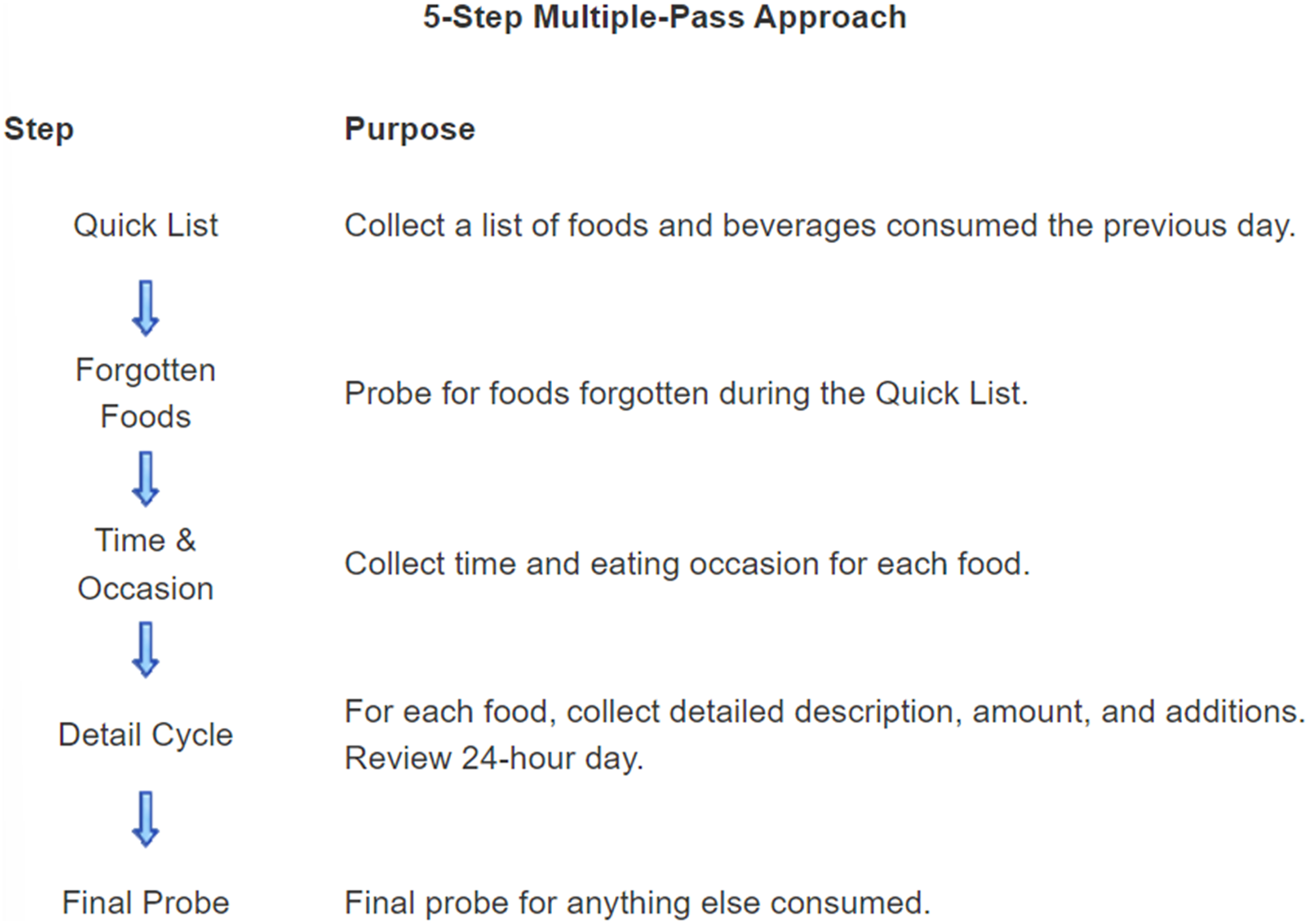
The most well-known traditional 24HR is the AMPM method.18,19 AMPM involves a 5 steps approach which is detailed in Figure 1.
18
The approach includes collecting a quick list of foods consumed in the previous 24 hours, followed by a probe for forgotten food, collection of contextual information (time and name of eating occasion e.g., breakfast, lunch), collection of further details including portion size, and a final probe.
18
The AMPM is designed to be used by trained interviewers and clinicians can use this methodology to record dietary information for their patients or for research purposes. The 24HR takes approximately 20 to 60 minutes to complete.3,15,18 5-Step multiple-pass approach.
18
The strengths of traditional 24HR include collecting detailed dietary information for a small or large population, and conducting 2 24HR on non-consecutive days allows you to estimate usual dietary intake. 16 Also, because traditional 24HR are interviewer administered, the interviewee doesn’t need to be literate, and this method is ideal for people with physical disabilities (e.g., blindness, arthritis). 16 Limitations include some groups may find it difficult to recall what was eaten in the previous day which may introduce error in estimating intake, and interviewers should undergo training so the 24HR is administered correctly. 16 Error for estimating intake with 24HR is generally higher than for food records. 16
Technology-Assisted 24HR
For technology-assisted 2HR like ASA24, users are emailed a weblink and username and password to complete the ASA24 in a location convenient to them and without an interviewer .14,20 Like traditional 24HR, individuals report everything consumed in the last 24 hours or the previous day. Technology-assisted 24HR have similar strengths and weaknesses to traditional 24HR. However, technology-assisted 24HR may help to reduce the burden for the user completing the assessment and the person analyzing the diet, and the cost of assessment.14,20 In addition, research has shown that in the United States 70% assessed preferred ASA24 over the more traditional interviewer administrated AMPM. 20 ASA24 can usually be completed in 17 to 34 minutes. 14 A limitation of technology-based 24HR like ASA24 is the literacy needed to complete an online 24HR without an interviewer, and access to the Internet. 14
Conclusion
Dietary assessments are highly complex, but useful tools for quantifying short- and long-term dietary intake patterns. These can assist researchers and others in linking diet and nutrition factors with key health outcomes. There are a number of tools available to measure diet, which are increasingly reliant on novel technologies that can streamline collection and analysis for researchers. Because dietary intake can change quickly as a result of an intervention, diet can be a useful tool for quantifying short term impacts of interventions. Dietary intake of individuals can also be habitual and be studied over a lifecourse to understand how particular patterns of food intake can influence disease risk. Knowledge and familiarity of these tools allows researchers to accurately access diet by selecting the tool appropriate to the question at hand.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.