
Abstract
African Americans (AAs) tend to have unhealthy eating behaviors, less physical activity (PA) participation, and higher stress levels compared to people who are White. These variables also have bidirectional relationships. Ecological Momentary Assessment (EMA) methodology can be used to examine these relationships through repeated data collection. This narrative review aims to assess EMA studies that examine the bidirectional relationships between healthy eating, PA, and stress in AA adults. Four databases were searched for studies that met inclusion criteria. Two separate searches were completed: one for healthy eating and stress, and one for PA and stress. Two reviewers independently assessed articles to minimize bias, while resolving discrepancies through discussion. Of the 97 articles identified, four studies met inclusion criteria (one on diet, two on PA, and one on both). These studies used five daily prompts sent for seven days and found that stress was associated with daily unhealthy eating and less daily PA, and increased PA participation was associated with less daily stress among AA women. No studies examined how healthy eating impacts stress or how both healthy eating and PA can influence stress, and three of the studies only included AA women. EMA methodology is useful for exploring how stress influences healthy eating and PA, and how PA impacts stress. Given the disproportionate stress burden among AA adults, future research should utilize EMA to explore how healthy eating impacts stress and the combined impact of healthy eating and PA on stress among this population.
“Findings revealed that associations have been found for the impact of healthy eating, PA, and stress on one another within some of those bidirectional relationships.”
Introduction
Research shows African American (AA) adults face various contextual factors that contribute to health disparities, such as food deserts, poor neighborhoods, and exposure to toxic substances. 1 These contextual factors, shaped by broader social determinants of health, such as racism, poverty, education, housing, access to healthy foods, environmental exposures, violence, and criminal justice, influence opportunities to engage in healthy lifestyle behaviors. 1 As a result of this, AA adults experience a heightened risk of chronic diseases and health issues, such as heart disease, diabetes, cancer, and stress, compared to other American races and ethnicities. 2 Evidence shows that participation in healthy lifestyle behaviors such as healthy eating and physical activity (PA) can lead to reduced stress. 3 Yet, it has been documented that AA adults have diets that are less healthy, 4 they are less physically active, 5 and have higher rates of stress when compared to the White population. 6
Unhealthy diets are defined as intake of red and processed meat, sugar-sweetened beverages, refined grains, and high-fat foods in high amounts. 7 Research shows diet patterns of AAs are typically higher in fried foods, processed meats, added fats, sugar-sweetened beverages, and bread. 4 In the year 2015, data from the National Health Interview Survey showed that 39% of non-Hispanic AA adults and 38.8% of Hispanics were more likely to be inactive compared to 27% of White persons. 8 More recent data show that these rates have been persistent. From 2017 to 2020, Black persons had the second highest physical inactivity prevalence at 30.0% among other racial groups (Asian, White, American Indian/Alaska Native, and Hispanic or Latino/a persons). 9
Stress, characterized by a state of worry or mental tension caused by a difficult situation, is also a concern among AA adults.6,10 Research over several decades has shown that AA adults are more stressed than non-Hispanic Whites. 6 Although these racial disparities are prevalent across the United States, they are especially of concern in the Southeast United States, where rates of chronic diseases linked to diet, 11 physical inactivity, 5 and stress are high.2 This is relevant to this review, as understanding the bidirectional relationships among these variables can help inform future research to reduce disparities in this highly impacted population within a highly impacted region.
More specifically, while unhealthy eating and lower PA participation have been associated with higher rates of stress, the relationship between these variables can also go in the inverse direction, with higher stress leading to the consumption of unhealthy foods and less PA participation. 3 However, few studies have examined the bidirectional relationships that exist between these lifestyle behaviors and their association with stress among AA adults, and many existing studies include samples from limited geographic regions or specific subgroups of individuals. It is critical to examine the role of stress in these lifestyle behaviors, specifically among AA adults, because structural racism contributes to disproportionate exposure to stressors, including discrimination and socioeconomic inequalities, which in turn may influence dietary behaviors, PA participation, and responses to stress.12
Ecological Momentary Assessment
Examining the bidirectional relationships between healthy eating, PA, and stress can be challenging, because these factors all change and vary from person to person within and across days. One method used to examine real-time associations between health behaviors that are shaped by social and environmental conditions in normal day-to-day environments is ecological momentary assessment (EMA). 13 EMA involves repeatedly collecting data on individuals’ behavior over a defined period to establish associations among variables. 13 There are also several key features common to EMA methods including data being collected in real world environments in the daily lives of subjects, focusing on the current state of individuals by way of self-reports that are considered momentary, strategically selecting moments for assessment based on interest (e.g., occasions when subjects feel stressed) or random sampling, and including multiple assessments from the same individuals over time to capture how experiences and behaviors change. 13 Different sampling strategies utilized in EMA data collection include event-contingent sampling, signal/random-contingent sampling, and time/interval-contingent sampling. 14 Event-contingent sampling involves reporting a predefined event, signal/random-contingent sampling involves collecting data at random times to obtain a representative sample of variables of interest throughout the study duration, and time-contingent sampling involves collecting data at fixed times. 14 By using EMA, it limits recall bias and maximizes ecological validity, which allows for a better depiction of reality and results than alternative methods such as surveys that require longer recall periods. 13
EMA has been used to examine both within- and between-person associations between these variables, with some studies addressing existing bidirectional links.15,16 Studies have used EMA to examine PA levels and psychosocial stress, 15 associations between processed food consumption and perceived stress among young adults, 16 emotions and food choices among college students, 17 and PA participation and healthy food consumption among college students. 18 While studies have used EMA methods to examine associations between these variables, research among AAs, a population disproportionately impacted by these variables, is limited. This narrative review examines the bidirectional relationships among healthy eating, PA, and stress, specifically in AA adults, highlighting the unique impacts within this population.
While bidirectional relationships exist between healthy eating, PA, and stress, the use of EMA facilitates examining these relationships with real-time associations. EMA also allows individuals to report on these variables in real time, improving the accuracy of data related to healthy eating, physical activity, and stress as they occur or shortly after. Additionally, using electronic devices to complete these EMA prompts can be convenient for participants as they go through their day-to-day lives. Lastly, EMA enables the examination of within-person and between-person associations between health behaviors and psychological variables over time, whereas cross-sectional analyses are limited to between-person associations at a single point in time. 19 Longitudinal data collection methods, such as EMA, also allow researchers to apply analytic approaches such as multilevel modeling and time-lagged analyses to better understand the potential bidirectional relationships between healthy eating. PA, and stress.
Findings from previous EMA research help illustrate how healthy eating, PA, and stress are interrelated in real-time. For example, higher stress has been found to be associated with lower PA participation, and higher PA levels with less stress among a population of university students. 3 Additionally, more stress influenced food cravings among another sample of university students. 20 Furthermore, more stress can cause cravings and unhealthy eating behaviors. 21 Building on these findings, the following sections of this narrative review explore the directionality of these relationships in more detail, focusing specifically on how healthy eating and PA impact stress and how stress, in turn, influences these health behaviors.
Healthy Eating Influence on Stress
Healthy eating is considered foundational for health and well-being, characterized by diets rich in whole grains, vegetables, fruit, legumes, and nuts, and low in salt, free sugars, and fats. 22 While most research linking healthy eating to reduced stress comes from studies that include young adults, 23 college students, 24 and German adults, 25 there is less research specifically examining the association among AA adults, who are known to eat less healthy, 4 participate in less PA, 5 and be more stressed compared to other racial groups. 6 While healthy eating behaviors such as higher consumption of fruits and vegetables among AA college freshmen have been found to be associated with lower psychological stress in a previously completed EMA study, 18 few EMA studies have specifically examined the impact of healthy eating on stress levels of AA adults, highlighting the need for further research in this area.
Physical Activity Influence on Stress
PA, defined as any bodily movement that results in skeletal muscles utilizing energy, can also directly affect stress by lowering it and thus improving mental health. 3 In general populations, higher PA levels are associated with less stress, 18 more positive affect, 3 and improved coping. 26 Among AA adults specifically, higher levels of stress and depressive symptoms are associated with lower PA participation, 27 and engaging in regular PA is linked to reductions in depressive symptoms. 28
The Influence of Stress on Healthy Eating
Research has shown that higher stress is associated with lower consumption of healthy foods and higher consumption of unhealthy food options such as fast food; ready-prepared meals; and snacks, especially those high in sugar. 24 Specifically, among AA populations, stress is positively associated with less healthful eating and increased obesogenic behaviors. 29 Stress factors that can cause unhealthy eating within this population include perceived stress, occurrence of stressors, and discrimination-related stress. 29 Therefore, research assessing the relationship among these variables is warranted to improve eating behaviors, stress levels, and response among AA adults and inform the design of targeted, effective interventions and strategies to combat these challenges.
The Influence of Stress on Physical Activity
Regarding the impact stress has on participation in PA, a majority of research studies examining associations between stress and PA have found that higher psychological stress predicts and is associated with reduced participation in PA and exercise across diverse populations.30–32 Specifically for AA populations, AA adults partake in less PA when they are stressed. 33 These lower levels of PA participation within this population can lead to the negative health habits of overeating and sedentary behaviors, which are associated with negative health outcomes. 33 This leads to a negative recursive cycle, resulting in diminished quality of life and health outcomes.
To our knowledge, limited studies examine the associations between healthy eating, PA, and stress simultaneously. Understanding the associations between healthy eating, PA, and stress through EMA methodology can be useful to inform future nutrition and PA behavioral interventions, especially for populations in which these variables are limited. Also, to our knowledge, there has not been a narrative review of the directionalities and relationships of these variables through the use of EMA studies with AA adult populations.
Furthermore, using EMA to examine the proposed conceptual model (Figure 1) among AA adults can reduce recall bias; capture fluctuations in stress, healthy eating, and PA; and find within-person associations that may exist. Regarding AA adults, the use of EMA can identify how various stressors they experience can impact their healthy eating and PA behaviors. Lastly, researchers have the opportunity to better understand the real-time dynamics of these variables, which can impact designing culturally relevant, timely, and effective interventions. Conceptual model detailing bidirectional relationships between healthy eating, physical activity, and stress.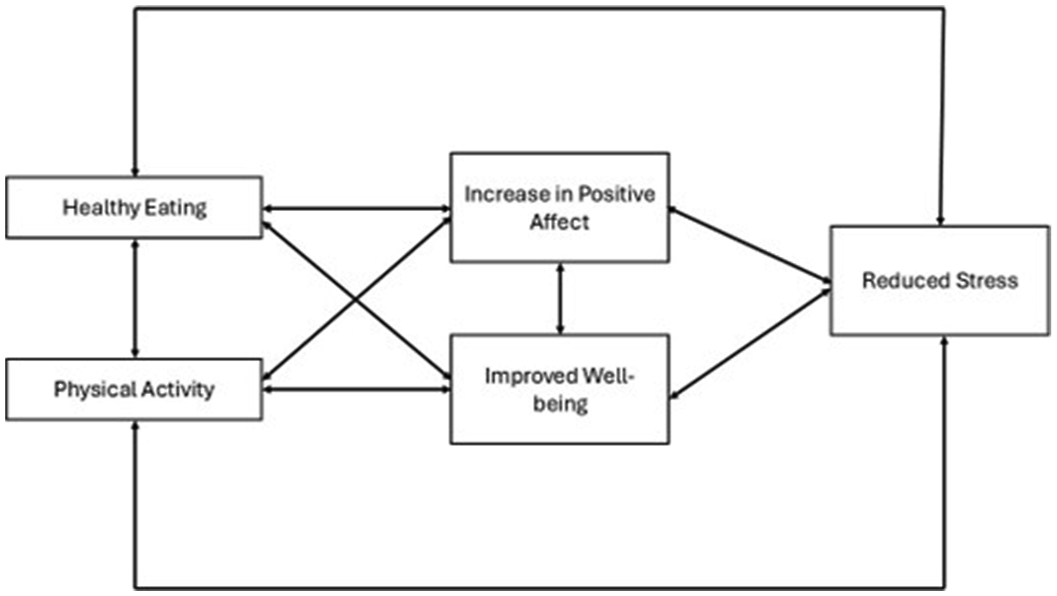
Additionally, previous research suggests that improvements in positive affect and subjective well-being may function as mediators linking healthy eating and PA to reduced stress. For example, consuming fruits and vegetables has been shown to predict greater positive affect, life satisfaction, and well-being. 34 Similarly, participation in PA has been associated with increased positive affect and well-being. 35 Although these mediators and bidirectional associations have not been extensively studied among AA adults, examining their role is important for understanding how healthy eating and PA influence stress in this population. This review includes only studies that use EMA to examine the impact that healthy eating and participation in PA have on stress levels of AA adults and the impact that stress has on the consumption of healthy foods and participation in PA.
Together, these studies suggest that the relationships between healthy eating and stress, in addition to PA and stress, are bidirectional. While many studies have examined the directionality of these associations among either one or the other health behaviors of healthy eating and PA, studies that have simultaneously examined both behaviors and directions are limited, especially among AA populations. As a result, current available literature only provides partial insight into these relationships and does not fully capture the relationships between healthy eating, PA, and stress in real time. This research gap highlights the importance of research needed in future EMA research that simultaneously examines healthy eating, PA, and stress to better understand their reciprocal relationships.
The present study aims to conduct a narrative literature review of EMA studies that have examined the bidirectional associations between healthy eating and PA with stress, specifically among AA populations, a group disproportionately affected by health disparities related to diet, PA, and stress.4-6 More importantly, these behaviors occur within broader contextual conditions that may shape health behaviors and daily experiences. Contextual factors, including neighborhood food environments, opportunities for PA, socioeconomic conditions, and exposures to discrimination-related stress, may influence dietary behaviors, PA participation, and general stress experiences among AA adults. 1 By examining studies that assess the bidirectional relationships between healthy eating, PA, and stress, this review highlights current evidence and identifies current research gaps to inform future culturally relevant and contextually responsive interventions. Based on prior literature, we anticipate that studies will include bidirectional relationships between healthy eating, PA, and stress, with potential mediators including increased positive affect and improved well-being, as seen in Figure 1.
Methods
A narrative review approach to this topic was chosen due to the small number of eligible studies, the differences between study designs, measures, and EMA methodologies, and the emerging stage of this research area. Because the current study was conducted as a narrative review, a formal preregistered protocol was not developed. Narrative reviews are appropriate for identifying trends and gaps in the literature, so directions for future research can be established. In the context of this study, a narrative review allowed us to describe how EMA has been used among AA adults and highlight unique considerations for EMA-based studies in this population.
The present review was completed by searching PubMed, Web of Science, PsycInfo, and Scopus Databases. These databases were selected for this review because they include a wide range of public health and behavioral health journals relevant to diet, PA, stress, and EMA research, and reviewers had access to them. These databases also ensure coverage of medical and health sciences research and literature. A combination of terms was used to search for related articles that included terms connected to diet (i.e., food, nutrition, and meal), PA (i.e., physical activities and exercise), and stress (i.e., stress and psychological). The search terms stress and psychological were used to broadly capture studies related to stress (i.e., perceived stress, emotional stress, cognitive stress, etc.). We did not include the search terms stressor or chronic stress in our searches, as we anticipated the broad term of stress to include these subjects. The terms “African Americans” or “Blacks” and “Ecological Momentary Assessment” or “EMA” were mandatory inclusion criteria. For studies to be included in this review, they had to be (1) focused on AA adult participants (ages 18+ years), defined as samples completely composed of AA adults or studies reporting subgroup analyses by AA adults, (2) peer-reviewed, (3) written in English, (4) published in the last 10 years (as of April 1, 2024), (5) utilized ecological momentary assessment (EMA) as a method to collect data on healthy eating, PA, or stress, (6) used original empirical and experimental data to examine the associations and results, and (7) included any timeframe for EMA data collection. Since studies were required to focus on AA adult participants ages 18 years and older, we did not include the search term “adults” in searches. Furthermore, the review was limited to studies published within the last 10 years to reflect rapid growth in EMA research, particularly in the last 10 years. 36
Two searches were completed in each database. The first search included Black* or African American*, Ecological Momentary Assessment* or EMA, Diet or food or nutrition or meal*, and Stress or psychological. The second search included Black* or African American*, Ecological Momentary Assessment* or EMA, Exercis* or physical activit*, and Stress or psychological. Asterisks were used as a truncation symbol to capture multiple word endings (e.g., “exercis*” captures exercise, exercising, and “activit*” captures activity and activities).
The first search in PubMed led to one article included and 12 excluded (n = 4 focused on children or adolescents, n = 7 included multiple races and ethnicities without stratifying by race, n = 1 being a development and usability study), and the second search led to two included articles and seven excluded articles (n = 5 were study protocols, n = 1 included multiple races and ethnicities without stratifying by race, and n = 1 being a duplicate from the previous search). The first search in Web of Science led to one article included and 13 excluded (n = 2 focused on populations other than AAs alone, and n = 11 were duplicates from a previous search). The second search in Web of Science led to zero articles included and 17 excluded (n = 1 being a feasibility and acceptability study without presenting analyses of associations, n = 1 focused on adolescents, n = 1 including multiple races and ethnicities without stratifying by race, n = 1 being a design and rationale study, and n = 13 articles being duplicates of a previous search).
The first search in PsycInfo led to zero articles included and eight excluded (n = 2 not including healthy eating or PA measures, n = 1 included children, n = 1 included multiple races and ethnicities without stratifying by race, and n = 4 were duplicates from a previous search). The second search in PsycInfo also led to zero articles included and eight excluded (n = 1 not including a stress measure, n = 3 did not stratify results by race, n = 2 focused on adolescents, n = 2 were duplicates from a previous search). The first search in Scopus led to 0 articles included and 15 excluded (n = 2 focusing on adolescents and n = 13 being duplicates from a previous search). Lastly, the second search in Scopus led to 0 articles included and 13 excluded (n = 4 being a study protocol without presenting analyses of associations, n = 2 not including healthy eating or PA measures, and n = 7 being duplicates from a previous search).
A second reviewer minimized bias by performing the same search using the same databases and search terms. Studies were selected based on inclusion criteria, and compared with the chosen studies to ensure all eligible studies were covered. If discrepancies existed between the inclusion decisions of reviewers, the studies in question were simultaneously examined by both reviewers. The studies in question were only added in the review if both reviewers agreed that the criteria for the review were met. If a discrepancy existed and could not be resolved between the reviewers, we had planned to consult a mentor faculty member for additional insight. However, a consultation as such was not necessary for this review.
The first reviewer found 97 results using the search terms in the databases. For the second reviewer, 109 results were found between the databases. Of the 109 results from the second reviewer, the same 97 results from the first reviewer were included in the second reviewer’s findings. Differences in the number of results identified by each reviewer were due to variations in database access (institutional access vs public access), which may have affected availability of certain studies. However, the records were screened collaboratively for inclusion, so this did not affect the overall sample. While the initial number of results found differed, the final number of inclusion articles differed by one, with four for the first reviewer and five for the second reviewer. Both reviewers addressed the one study discrepancy, and a unanimous decision was made to exclude the study due to no measure of healthy eating or physical activity.
Results
Overall, four studies met the eligibility criteria for inclusion, and the detailed study selection process is shown in Figure 2. Studies included in the final review had a timeframe of seven days, with five prompts sent daily; however, they ranged in study population, genders, ages, measures, and outcomes, as shown in Table 1. The prompts were delivered at predetermined times via smartphones and handheld devices. Collected data included food intake, PA participation, and self-reported stress (i.e., hassles and racial discrimination), with three studies including accelerometry data. While the sampling strategies were similar for the included studies, there were variations in measures assessed and prompt timing. As a result, the studies have been further narratively described while detailing their study measures and findings. The search found no studies that included healthy eating, PA, and stress measures concurrently among an AA adult population. The four quantitative studies that met inclusion criteria focused on environmental and personal factors associated with snack food intake,
37
sedentary time and PA,38,39 associations between racial discrimination (i.e., denied a bank loan, unfairly fired, and stopped by police and treated unfairly in any part of that interaction including being stopped itself) and PA,
39
and associations between daily work hassles (i.e., hassles arising from fellow workers, a problem on the job due to being a woman, being given more work or the most undesirable tasks or jobs at work than someone who is White/non-Black or equal or less seniority and qualifications) and energy balance.
40
In summary, the studies included in this review found that stress was associated with daily unhealthy eating and less daily PA,37,38,40 and increased PA participation was associated with less daily stress.
39
These studies are described in more detail in Table 1, including study design, length of study duration, outcomes, and major study findings. Prisma flow diagram.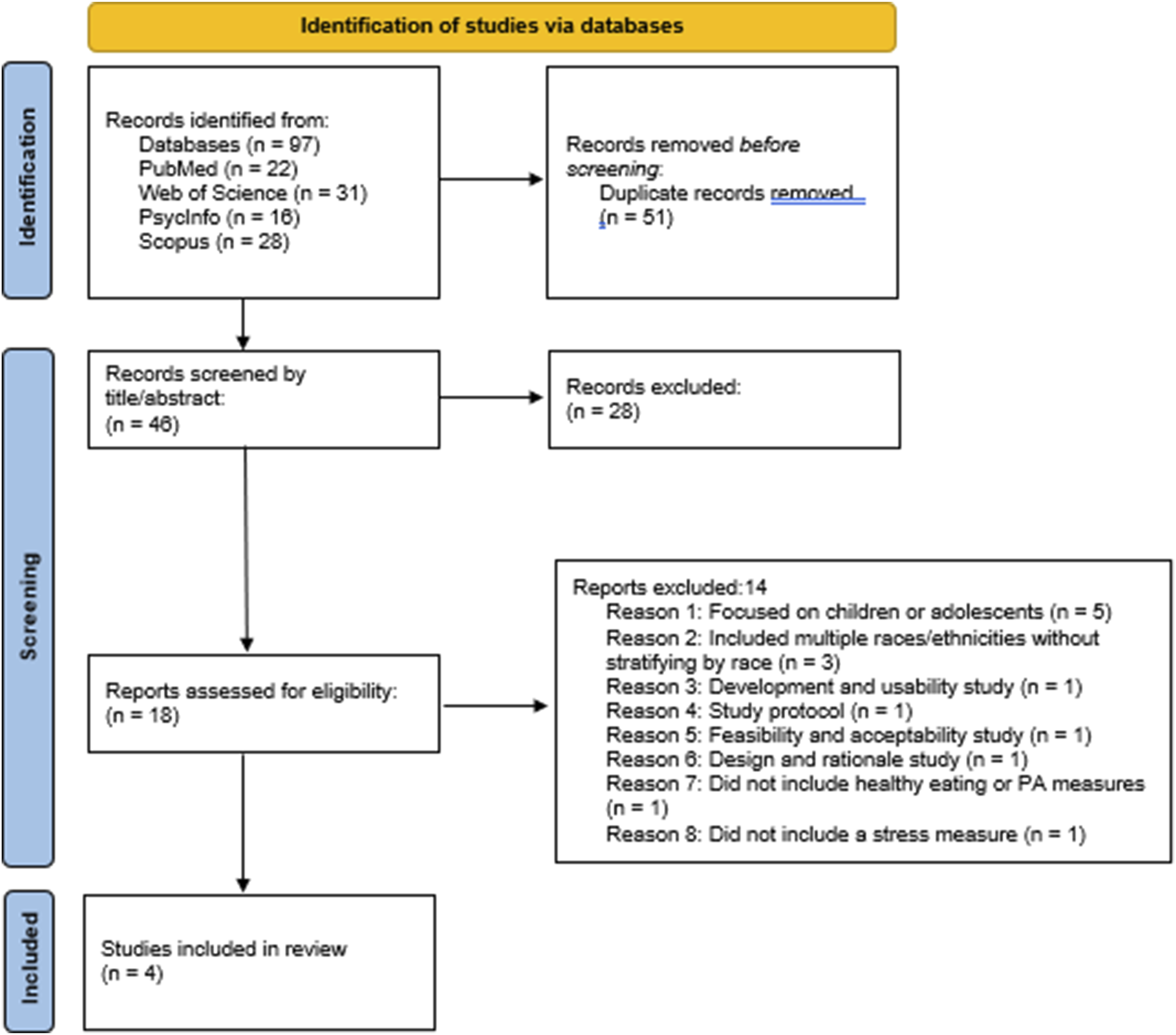
In studies included in the present review, it was found that higher snack intake was associated with lower self-efficacy at the between-person level 37 ; and increased moderate to vigorous PA (MVPA) was associated with decreased stressors related to subjective social status (i.e., participants reporting their perceived standing in society with the top representing the most money, most education, and the best jobs and the bottom representing the people who are worst off, have the least money, have the least education, and who have the worst jobs or no job). 38 Furthermore, the studies included in this review found that higher experiences of stressors related to racial discrimination contributed to higher time spent participating in sedentary behaviors 39 ; and higher stress led to higher unhealthy food intake. 40 While “healthy eating” was used throughout this review for consistency, it is important to note that not all included studies explicitly defined this term. Instead, studies used EMA measures related to specific dietary behaviors (i.e., empty calorie and snack food intake). Below are details of the four studies identified through this narrative review.
Study 1: Impacts of Stress on Healthy Eating (“What Impact Does Stress Have on Healthy Eating?”)
One study examined the relationship between environmental and personal factors (i.e., perceived food availability and expense, daily hassles, self-efficacy, and positive and negative affect) and snack food intake among AA women (n = 100; ages 25-65 years). 37 Stress was assessed through the reporting of daily hassles using three measures (i.e., two single item measures: “Have you experienced a stressful event since your last entry?” and “Have you experienced a stressful or problematic social interaction since your last entry?” and an 89-item daily hassles checklist). 37 The study specifically looked at between-person and within-person associations and found that women who reported on average more stressful events—as subjectively reported without a predefined list—were more likely to consume snack foods, and being close to a restaurant or store heightened the likelihood of snack consumption, respectively. 37 The study also found that for every one-unit increase in the frequency of daily hassles reported on the 89-item daily hassles checklist (e.g., meeting a deadline, argued with someone, cooking, traffic, unfair treatment), participants were 14% more likely to have snack food consumption. 37 This shows that daily hassles that are experienced and contribute to more stressors among this population can cause them to consume foods that are lower in nutrients and considered unhealthy. Related to the relationships found between the frequency of daily hassles experienced and negative affect with snack food intake, researchers found that these relationships differed depending on the availability and expense of food. 37 For example, when food was more easily available, the frequency of daily hassles was positively associated with snack food intake and when food was not easily available, the frequency of daily hassles was not associated with the probability of snack food intake. Lastly, the study also found that women with higher diet-related self-efficacy levels reported less snack food consumption. 37 This suggests that greater self-efficacy for dietary behaviors is associated with lower consumption of snack foods and foods that are not considered healthy, independent of other factors.
Studies 2 and 3: Bidirectional Relationships Between Physical Activity and Stress (“What Impact Does Physical Activity Have on Stress?” and “What Impact Does Stress Have on Physical Activity?”)
The second study focused on within-person associations in AA women (n = 97, ages 25-65), focusing on how personal factors—including daily stressors—were associated with their MVPA participation and sedentary behaviors. 38 Although environmental factor variables were assessed, findings related to stress and PA align with the aims of this review. Participants answered prompts via a web-based survey. Interval-contingent prompts were delivered to study-provided smartphones once during five different time blocks from 7 a.m. to 7 p.m. 38 The only environmental factor that affected PA was weather, such that their MVPA was reduced by 27.3% on days when women reported poor weather. 38 The study also found that the participants were more likely to participate in MVPA and less likely to participate in sedentary behaviors when they reported negative affects at the beginning of their day. 38 This finding suggests that experiencing negative affects at the beginning of the day may require the women to multitask and move around more. This finding may also suggest that this increased time spent completing tasks leaves the women with less time to relax, explaining the reduction in sedentary behaviors. Lastly, the study found that more participation in MVPA during the day was associated with more positive emotions at the end of the day. 38 Similar results were found for sedentary behavior, whereby more time spent in sedentary behavior resulted in reduced positive affects for the study sample. 38 For the future, the researchers suggested that interventions should focus on increasing PA levels, addressing emotions in terms of positive and negative effects, and reducing sedentary behaviors to improve health outcomes. 38
The third study focused on racial discrimination-related stressors and their association with sedentary time and PA among an AA population (n = 12, ages 30-55). 39 More specifically, the study sought to examine the effects of racial discrimination on PA outcomes. 39 This study was distinctive in examining a root cause of chronic stress that disproportionately affects AAs and contributes to health disparities—systemic, structural, and interpersonal racial discrimination. This study looked at both group and individual associations and found that a higher energy expenditure was associated with lower lifetime discrimination. 39 This study also found more experiences of perceived racial discrimination were associated with more sedentary time at the within-person level. 39 Translating these findings to other AA women suggests that lower PA levels may co-occur with greater exposure to racial discrimination-related stressors. However, the directionality and causality of this association remain unclear and should be interpreted with caution due to the limited sample size. Contrary to these findings, the study also found opposing results between PA and social status and racial discrimination. The first contrasting result found that more MVPA was associated with lower self-reported subjective social status levels. 39 The second contrasting result found that more perceived racial discrimination was associated with slightly higher MVPA completion. 39 These results explain that more participation in the health behavior of MVPA could be used as a coping mechanism for racial discrimination stressors. While these findings can contradict what one hypothesizes, they may be due to the smaller sample size and the need for a longer study duration. 39 Furthermore, the smaller sample size limits generalizability and may account for some of the contrasting findings. However, the findings of this study could be deemed helpful for looking at the examination of the frequency of racial discrimination stressors experienced by individuals in the population and what can be done to minimize and eliminate the negative health impacts these stressors impose.
Study 4: Impact of Stress on Healthy Eating and Physical Activity (“What Impact Does Stress Have on Healthy Eating and Physical Activity?”)
The last study, which focused on the associations between daily work hassles and energy balance behaviors in AA females (n = 70, ages 25-60), examined how hassles such as annoyance or frustrations at work affect food intake, MVPA and sedentary behavior participation, and sleep duration and disturbances. 40 This study utilized EMA methods to measure daily accelerometer data, empty calorie food intake, and daily work hassles. For the latter two measures, prompts were sent to study-provided smartphones for participants to respond to five times daily. 40 This study found that experiencing at least one daily work hassle was associated with higher same day consumption of empty calorie foods and a daily additional 35.8 min of sedentary behavior. 40 However, no significant associations were found between daily work hassles and MVPA participation, sleep duration, or sleep disturbances. 40 The study also found that the association between daily work hassles and empty calorie intake was no longer significant when conducting a sensitivity analysis and controlling for the participants’ work schedules, with two possible explanations being workers consuming more empty calorie foods on the weekends and days they are not at work and a small sample size that may have reduced the statistical power of the study. 40
Discussion
This review aimed to assess the associations between healthy eating, PA, and stress through completed EMA studies. While there was a total of 109 articles reviewed for inclusion between the reviewers, only four met inclusion criteria. The studies included in the current review found various associations between the variables, and all used EMA to examine the associations. All of the studies also included an EMA timeframe of five prompts sent daily for seven days. The studies were all published within the last 10 years, with one published in 2014, one in 2017, and two in 2021. One study examined the impact of stress on healthy eating, one examined the impact of PA on stress, one examined the impact of stress on PA, and one examined the impact of stress on both healthy eating and PA. Of the four studies included in this review, three focused exclusively on AA women, and one included both AA men and women. Participants across studies ranged from 25 to 65 years of age from Chicago, Illinois, and New Haven, Connecticut communities. While none of the studies explicitly reported gender-based differences in their findings, the focus on AA women in most of the included studies in this review may limit generalizability to AA men. Therefore, future research should examine potential gender differences in the relationships between healthy eating, PA, and stress.
This narrative review examined how EMA has been used to examine the associations among healthy eating, PA, and stress among AA adults. Results of this review indicate potential bidirectional relationships, particularly in the Zenk et al. (2016) study, where multivariable linear regression models were used and found that negative affect predicted reductions in MVPA and increased sedentary behavior. 38 The Zenk et al. (2016) study also found that increased MVPA was associated with higher positive affect. 38 Other studies in this review assessed stressors as predictors of behaviors without testing the bidirectionality of the behaviors (i.e., testing if healthy eating or PA predicted stress). Furthermore, findings revealed that associations have been found for the impact of healthy eating, PA, and stress on one another within some of those bidirectional relationships. These findings suggest that stress is positively associated with higher consumption of unhealthy foods, stress is negatively associated with PA participation, and PA participation is negatively associated with stress.
Furthermore, these relationships may also be influenced by broader contextual factors that affect AA communities. Structural and environmental conditions such as food availability within neighborhoods, access to safe environments for PA participation, and racial discrimination experiences can influence exposures to stress and the opportunity to engage in healthy behaviors. Considering these contextual factors is essential when interpreting the associations examined within EMA studies. Taking into account these contextual factors is also important when designing interventions aimed at improving health behaviors in AA populations.
Results of the current review are aligned with research that has examined associations between stress, healthy eating, and PA within other populations. Mouchacca, Abbott, and Ball (2013) reviewed associations between stress, PA, and healthy eating among women aged 18-46 years old who lived in socioeconomically disadvantaged neighborhoods, and reported that cross-sectional associations were found between stress and physical activity and increased odds of more fast-food consumption. 41 Higher stress scores were associated with an increased likelihood of consuming a high fast-food intake. 41 Stress also led to reduced engagement in PA. 41 Another study by Gillan et al. (2013) reviewed correlations among stress, PA, and healthy eating among a sample of school-based employees in a southeastern Louisiana school district, and found that those who engaged in vigorous PA regularly had less perceived stress. 42 Individuals who consumed green salad and fruit were more likely to use task-oriented coping as a healthy way to control stress. 42 There had also been an EMA study completed by Schultchen et al. (2019) that examined the bidirectional relationships of stress and affect with physical activity and healthy eating among a sample of university students, and found that higher stress, negative affect, and lower positive affect were related to reduced PA. 3 Likewise, higher PA was related to less stress, less negative affect, and more positive affect.
The outcome of high stress levels leading to lower healthy eating found in this review is comparable to a systematic review completed by Kazmierski et al. The review by Kazmierski et al. (2021) found that among studies with AA adults examining the association of stress on eating, stressful events, perceived stress, discrete stressors, and discrimination-related stress experienced by this population were associated with decreased healthy eating and more obesogenic eating patterns. 29 Previous research has also shown that AA adults who consumed healthy food components, including vegetables, greens, fruits, whole grains, and legumes, reported better mood, energy, and sleep. 43 This finding is also comparable to our review, as we found that AA women with lower snack consumption had higher self-efficacy levels. 37 A study by Hill et al. (2021) reviewed stress and eating behaviors in healthy adults and found that stress was associated with increased consumption of unhealthy foods. 44 Hsu and Raposa (2020) examined the impact of stress on healthy eating behaviors of adolescents through ecologically valid daily diary assessments and found that the adolescents who had more perceived stress reported higher rates of craving tasty foods and trouble stopping the consumption of these foods, which are associated with unhealthy foods. 21
Although recent research on PA lowering stress levels of AA women is limited, previous research has shown that even a medium amount of daily PA can improve stress levels. 3 This finding is consistent with the finding in our review that more participation in MVPA during the day is associated with more positive emotion from using EMA. 40 Previous research has also found that increased levels of interpersonal stressors, such as racial discrimination, were associated with lower PA and increased sedentary behavior through a mediator of depressive symptoms. 27 This finding is supported by the current study, as research in this review showed that more experiences of perceived racial discrimination were associated with more sedentary time. 39
A previous EMA scoping review study completed by Wright, Williams, and Veldhuijzen (2023) reviewed associations between PA, sedentary behavior, and stress and found that stress is associated with lower PA at the within-person level. 45 The review also found that PA was associated with lower stress. 45 A previous study by Schultchen et al. (2019) found that higher stress was related to a reduction in PA, and higher PA levels were associated with less stress. 3 Another study by Dunton et al. (2017) found that children’s healthy eating at the day level was not associated with their own perceived stress or the perceived stress reported by their mothers. 46 The same study also found that mothers participated in more healthy eating on the days when their perceived stress was higher than usual, but their daily healthy eating was not associated with their children’s perceived stress levels. 46 Although there are studies that have examined the associations between healthy eating, PA, and stress, there have been very few studies that have examined these associations among populations of AA adults who are documented to be negatively impacted by unhealthy eating, 4 physical inactivity, 5 and stress. 6 Therefore, this review highlights current findings and gaps in literature that can help inform future research.
This review does have some limitations. First, no study was included in the review that determined the associations between the impact of healthy eating and PA simultaneously on stress levels, warranting the need to complete an EMA study to examine these associations. Secondly, three studies in the review only studied AA women, increasing the need for studies that include men when using EMA methods to examine these associations across sex and for the population. Also, the studies included in this review only included AAs from limited locations, vs. surveying individuals across multiple states, which may limit the generalizability of findings to AAs. Furthermore, the majority of included studies lack attention to racial discrimination and other structural stressors as sources of general stress. With systematic, structural, and interpersonal racism being well-documented contributors to health disparities among AAs, future EMA studies should include racism-related stressors, discrimination-related stressors, and other contextual determinants of health to better understand their role in shaping health behaviors.
Next, the studies included in this review did not specify the time of year when data collection occurred. This limits the ability to examine whether seasons or holidays influence findings. Future research should consider reporting seasonality in the study designs and analyses. Analytic approaches using longitudinal EMA data could also be used to better capture the relationships between healthy eating, PA, and stress in EMA studies. These approaches will provide more insight into the directionalities of these relationships. Also, a formal appraisal of study quality or bias was not conducted, which limits the ability to assess the confidence that can be placed in these findings. Although study strength of evidence was part of our inclusion criteria, future reviews should include quality assessments to better inform the interpretations of the evidence. Lastly, there were only a limited number of EMA studies and study designs to deduce information, and all studies included in the review utilized interval-contingent prompts to report health behaviors. However, there is the potential to find more information if other EMA designs are used, such as daily diaries, event-contingent prompts, or signal-contingent prompts. The limited number of EMA studies identified in this review highlights that using EMA methodologies remains a novel approach for examining the bidirectional relationships between healthy eating, PA, and stress in AA adults. Given the disproportionate burden of stress and chronic disease among AA adult communities, the ability to capture experiences in the moment is significant for the potential to inform targeted interventions. Future research should be expanded by using EMA methods in larger AA populations and including other study designs to further understand the complexity of the relationships. Although limitations exist with this review, it does have several strengths. One of them includes examining studies that utilized EMA to find real-time associations. EMA methods were used similarly throughout all the studies, with prompts being sent five times a day for seven days to assess the different measures. Another strength includes using a second reviewer to ensure comprehensive inclusion and exclusion decisions.
Conclusion
While ample literature examines the associations between healthy eating, PA, and stress in different combinations and among general populations with and without the use of EMA methods, there is limited research among AA adults alone using EMA. There are also a limited number of studies that examine daily associations through EMA between healthy eating, PA, and stress, both independently (i.e., impact of stress on healthy eating; impact of stress on PA; impact of healthy eating on stress; and impact of PA on stress) and simultaneously (i.e., impact of stress on healthy eating and PA; impact of healthy eating and PA on stress), within AA adult populations. This review found that stress is associated with unhealthy food consumption, physical activity is associated with lower stress, and experiencing racial discrimination stressors is associated with less PA participation at the within-person level. More specifically, the review suggests that daily hassles and racial discrimination were commonly associated with greater unhealthy eating and sedentary behavior. Although associations with PA were mixed, they highlight the complexity of these relationships.
While EMA has been effectively used in the reviewed studies to examine how stress influences healthy eating and PA, and how PA impacts stress, to our knowledge, no studies have applied EMA methodology to explore how healthy eating impacts stress or the combined effects of healthy eating and PA on stress in AA adults. Future research should consider using EMA to assess the relationships between healthy eating, physical activity, and stress, as it allows for real-time, naturalistic data collection methods that can increase the ecological validity of the findings; capture the variables within daily lives; and ensure the accuracy of findings by limiting recall bias among participants. Future studies should also focus on different populations at risk for health issues based on the examined variables, and simultaneously study the variables of healthy eating, PA, and stress. Lastly, future research studies should also ask about perceived food availability and expense at each EMA prompt, regardless of food intake; have both event-contingent and signal-contingent signals at random and multiple times per day; and improve dietary assessment during prompts to extend beyond a checklist of items for foods consumed.
This review’s findings through utilizing measures in day-to-day environments are relevant for implementing interventions aimed at increasing healthy food consumption, increasing PA levels, and decreasing stressors, specifically among AA adult populations. The creation and implementation of interventions with the information received from day-to-day results can assist in alleviating adverse health outcomes and improving the overall health of AA adults, who may be at risk for chronic health conditions due to the day-to-day disparities they experience.
Footnotes
Ethical Considerations
This declaration is not applicable.
Consent to Participate
This declaration is not applicable.
Consent for Publication
This declaration is not applicable.
Author Contributions
All authors contributed to the conceptualization, drafting, and final approval. Data collection was performed by Alexis Bell, MPH and Enid Keseko, MS. The first draft of the manuscript was written by Alexis Bell, MPH, and all authors contributed comments to the previous manuscript versions to be addressed before the submission of the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This declaration is not applicable.
Code Availability
This declaration is not applicable.
Appendix
Description of EMA Studies Focused on Healthy Eating, Physical Activity, and Stress Among African American (AA) Adult Populations; Study Design, Sample, and Methods (N = 4).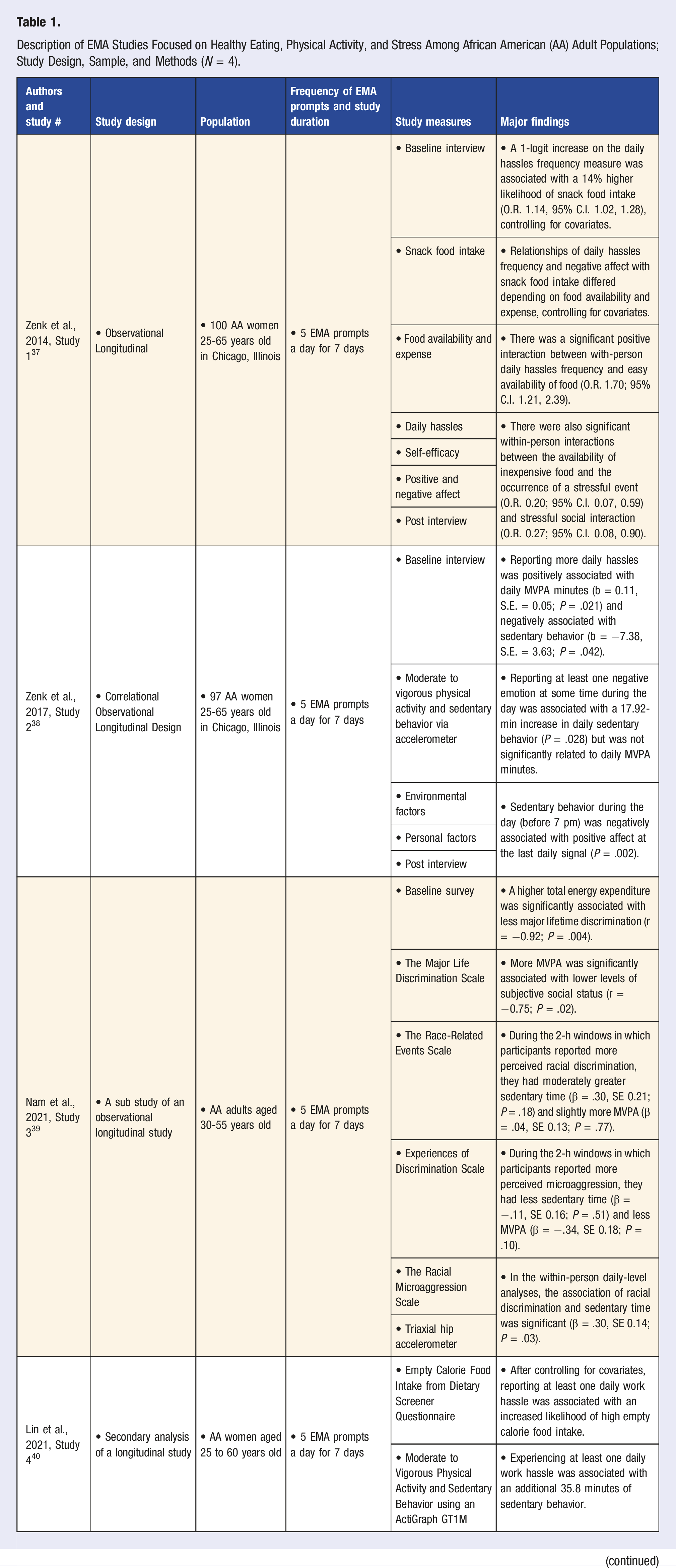
Authors and study #
Study design
Population
Frequency of EMA prompts and study duration
Study measures
Major findings
Zenk et al., 2014, Study 1
37
• Observational Longitudinal
• 100 AA women 25-65 years old in Chicago, Illinois
• 5 EMA prompts a day for 7 days
• Baseline interview
• A 1-logit increase on the daily hassles frequency measure was associated with a 14% higher likelihood of snack food intake (O.R. 1.14, 95% C.I. 1.02, 1.28), controlling for covariates.
• Snack food intake
• Relationships of daily hassles frequency and negative affect with snack food intake differed depending on food availability and expense, controlling for covariates.
• Food availability and expense
• There was a significant positive interaction between with-person daily hassles frequency and easy availability of food (O.R. 1.70; 95% C.I. 1.21, 2.39).
• Daily hassles
• There were also significant within-person interactions between the availability of inexpensive food and the occurrence of a stressful event (O.R. 0.20; 95% C.I. 0.07, 0.59) and stressful social interaction (O.R. 0.27; 95% C.I. 0.08, 0.90).
• Self-efficacy
• Positive and negative affect
• Post interview
Zenk et al., 2017, Study 2
38
• Correlational Observational Longitudinal Design
• 97 AA women 25-65 years old in Chicago, Illinois
• 5 EMA prompts a day for 7 days
• Baseline interview
• Reporting more daily hassles was positively associated with daily MVPA minutes (b = 0.11, S.E. = 0.05; P = .021) and negatively associated with sedentary behavior (b = −7.38, S.E. = 3.63; P = .042).
• Moderate to vigorous physical activity and sedentary behavior via accelerometer
• Reporting at least one negative emotion at some time during the day was associated with a 17.92-min increase in daily sedentary behavior (P = .028) but was not significantly related to daily MVPA minutes.
• Environmental factors
• Sedentary behavior during the day (before 7 pm) was negatively associated with positive affect at the last daily signal (P = .002).
• Personal factors
• Post interview
Nam et al., 2021, Study 3
39
• A sub study of an observational longitudinal study
• AA adults aged 30-55 years old
• 5 EMA prompts a day for 7 days
• Baseline survey
• A higher total energy expenditure was significantly associated with less major lifetime discrimination (r = −0.92; P = .004).
• The Major Life Discrimination Scale
• More MVPA was significantly associated with lower levels of subjective social status (r = −0.75; P = .02).
• The Race-Related Events Scale
• During the 2-h windows in which participants reported more perceived racial discrimination, they had moderately greater sedentary time (β = .30, SE 0.21; P = .18) and slightly more MVPA (β = .04, SE 0.13; P = .77).
• Experiences of Discrimination Scale
• During the 2-h windows in which participants reported more perceived microaggression, they had less sedentary time (β = −.11, SE 0.16; P = .51) and less MVPA (β = −.34, SE 0.18; P = .10).
• The Racial Microaggression Scale
• In the within-person daily-level analyses, the association of racial discrimination and sedentary time was significant (β = .30, SE 0.14; P = .03).
• Triaxial hip accelerometer
Lin et al., 2021, Study 4
40
• Secondary analysis of a longitudinal study
• AA women aged 25 to 60 years old
• 5 EMA prompts a day for 7 days
• Empty Calorie Food Intake from Dietary Screener Questionnaire
• After controlling for covariates, reporting at least one daily work hassle was associated with an increased likelihood of high empty calorie food intake.
• Moderate to Vigorous Physical Activity and Sedentary Behavior using an ActiGraph GT1M
• Experiencing at least one daily work hassle was associated with an additional 35.8 minutes of sedentary behavior.
• Pittsburgh sleep Quality Index
• Daily work hassles were not significantly associated with MVPA engagement (OR: 1.1, 95% CI: .3, 3.4), short sleep duration (OR: .8, 95% CI: .2, 3.0), or sleep disturbance (OR: .5, 95% CI: .2, 1.6).
• Hassles and Uplifts Scale