
Abstract
Exercise is a pivotal tool in the prevention and management of chronic disease, a cornerstone of primary care. Yet, there is little formal exercise education in medical school and many medical students feel unprepared to effectively counsel patients about exercise. Since 2019, medical students in the Primary Care Program (PCP), a primary care-focused educational track, at the Keck School of Medicine (KSOM) of the University of Southern California (USC) have taught exercise classes to the local community as part of a service-learning experience. Students receive lectures on exercise from faculty and then deliver curated bilingual English/Spanish presentations and lead exercise classes for the community. Post participation in this program, students reported (1) increased knowledge of exercise principles, (2) increased predicted likelihood of counseling patients about exercise, (3) increased confidence in providing exercise counseling, and (4) intent to make positive changes in their own exercise habits. This curriculum provides a replicable lifestyle medicine model for other medical schools seeking to enhance exercise education and train the next generation of primary care physicians.
“Students reported that their experience would make them more likely to counsel their future patients about exercise goals, types of exercise, and community-based exercise resources.”
Introduction
Regular physical activity is a cornerstone of preventive medicine and chronic disease management. 1 Yet, few Americans adhere to the recommended 150 minutes weekly of moderate exercise and 20 minutes twice weekly of strength training. 2 Few physicians discuss exercise prescriptions with patients or feel confident making exercise recommendations.3,4
There is little exercise education throughout medical school. 5 Fewer than 6% of medical schools have exercise education courses/requirements. 6 In one study, only 2% of medical students correctly identified national exercise guidelines. 7 Without exercise education, the physician workforce lacks the exercise knowledge and expertise necessary to effectively counsel patients.
An overwhelming majority of medical students are receptive to additional exercise education. 8 Few studies describe medical education exercise curriculum and best practices; however, given that active learning improves retention, 9 incorporating skill-based exercise training may be effective.
To provide service-learning, skill-based exercise training for medical students, the Primary Care Program (PCP) at the Keck School of Medicine (KSOM) of University of Southern California (USC) trains first year medical students (MS1s) to teach nutrition, cooking, and exercise classes. The PCP is an educational track for students interested in pursuing primary care careers.10,11 PCP students have led these classes for the Los Angeles General Wellness Center (LAGWC) community since 2016. 12 In 2019, exercise was added and delivered in-person until March 2020, when classes pivoted to a virtual format due to the COVID-19 pandemic. 13 Starting in Fall 2022, classes were delivered in a hybrid in-person/virtual format. The goal of the classes was to engage in service-learning, simultaneously providing a service to the community and practical skills for medical students.
The purpose of this pilot study is to evaluate medical students’ experiences teaching and leading exercise classes to community members both virtually (Fall 2021) and as a hybrid virtual/in-person (Spring 2023) format. We hypothesized that, post course participation, medical students would report: (1) increased exercise knowledge; (2) increased confidence counseling patients about exercise; (3) positive changes in their own exercise habits; (4) high satisfaction for the virtual and in-person format; and (5) enhanced awareness of virtual health education best practices.
Methods
Participants
Participants include 2 KSOM cohorts who taught LAGWC exercise classes for the first time (except three second year medical students [MS2] who taught twice the year before): • Cohort 1: 32 PCP MS1s and 3 PCP MS2s taught virtually September-December 2021 • Cohort 2: 32 PCP MS1s taught hybrid virtually/in-person January-April 2023
Los Angeles General Wellness Center teaching is a PCP MS1 requirement and is unique to the PCP educational track. Students are informed of the extra time and effort required prior to acceptance to the program. MS2s volunteered, but few participated, perhaps due to competing academic demands.
Student Training/Preparation
Before teaching the exercise classes, students received 1 hour of training conducted by Family Medicine (FM) physician faculty. The training covered: (1) the health benefits of exercise, (2) evidence-based recommendations for types, duration and intensity of exercise, and (3) specific exercises for strength and balance. Course content was drawn from faculty clinical experience and recommendations from the World Health Organization (WHO), the Centers for Disease Control, the American Heart Association, and other evidence-driven public health organizations.
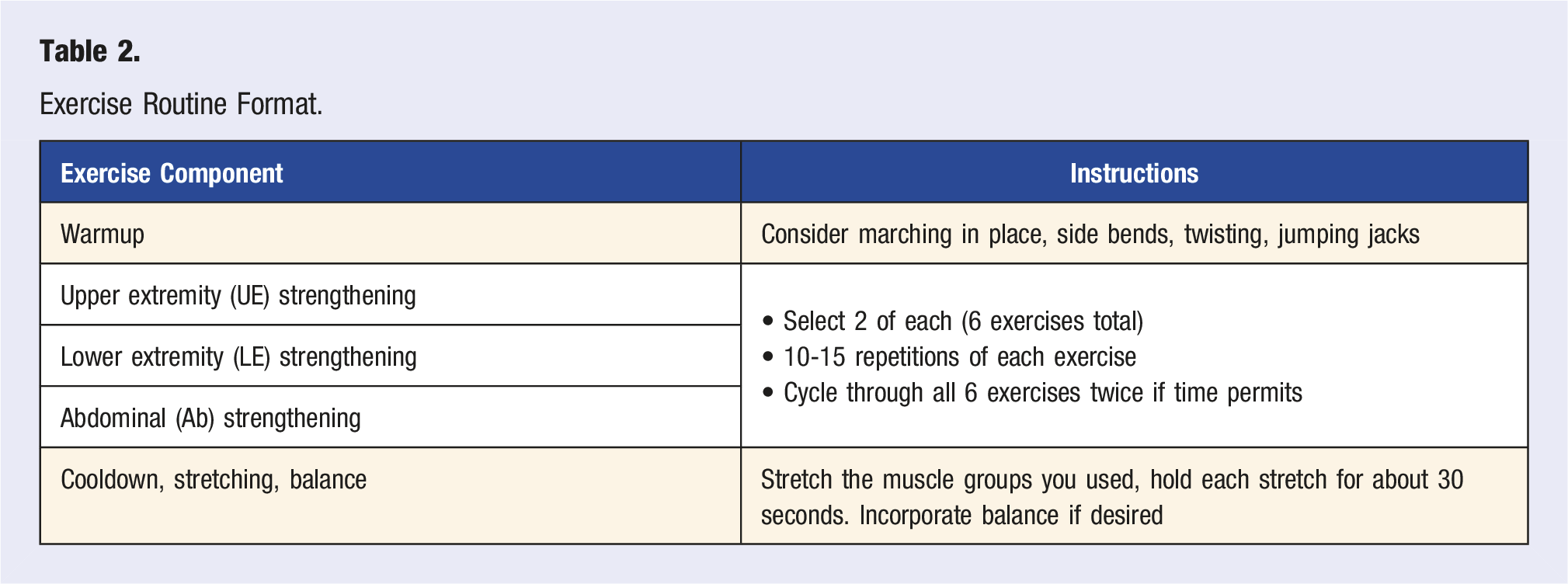
Students were given access to an exercise “bank,” created by a KSOM physical therapist and FM physician faculty, with exercise photos and descriptions prior to teaching. Students reviewed their specific lecture material 1 week ahead of their class, creating an exercise routine using the “bank” (Table 2). Students also had access to a video recording of a physical therapist demonstrating proper exercise form and modification alternatives. Immediately prior to teaching, FM faculty were available to answer student questions, suggest exercise modifications, and remind students of teaching best practices.
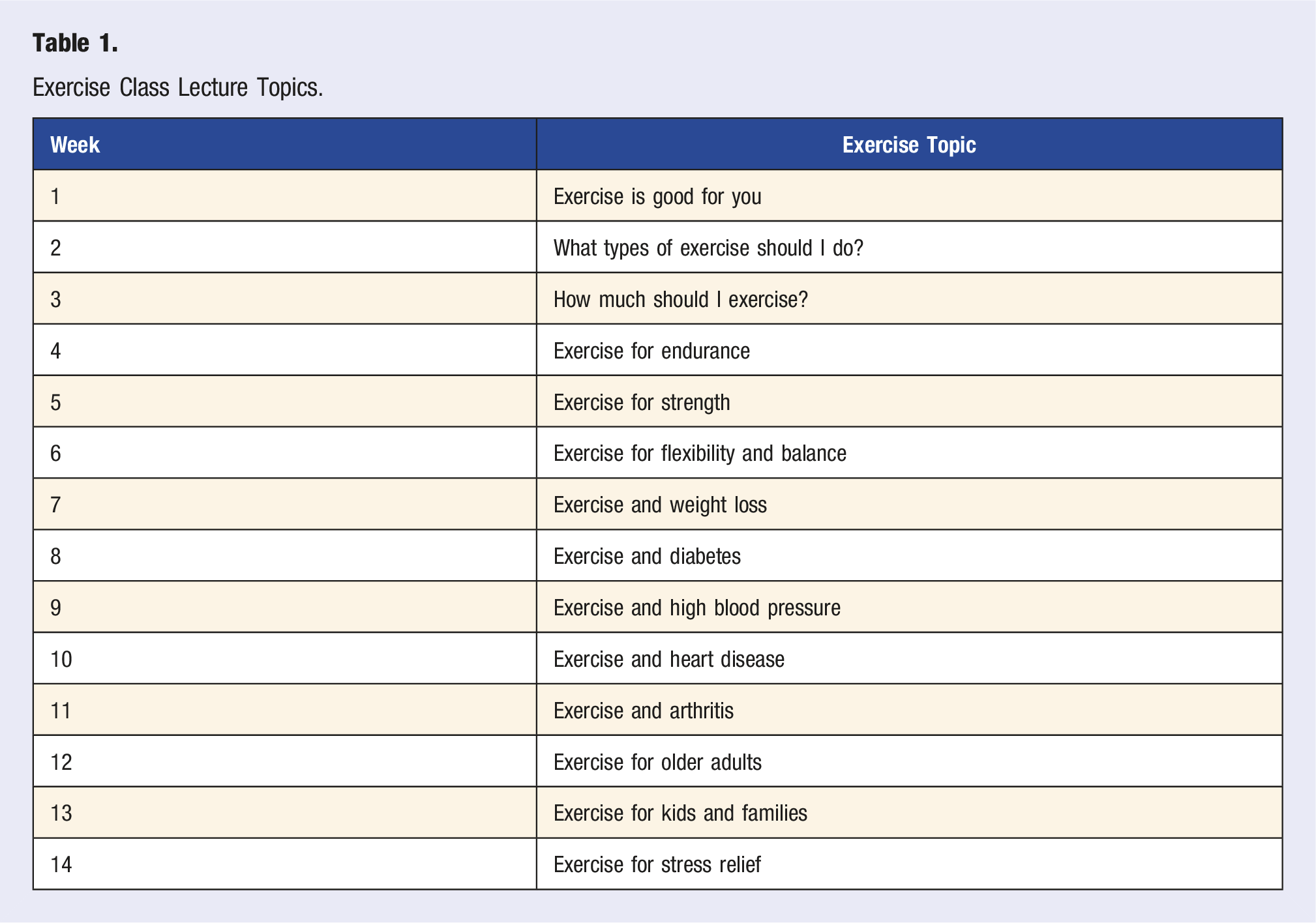
Exercise Classes
Exercise Class Lecture Topics.
Exercise Routine Format.
FM and PT faculty were available during the class to provide feedback to students and participants, ensure content accuracy, correct form, and help answer participant questions. All classes were taught bilingually in English and Spanish.
Data Collection and Analysis
Immediately after teaching, students were emailed an optional nutrition and exercise Qualtrics survey link. The survey included 12 closed- and open-ended nutrition and exercise questions (Appendix A and B). Questions were devised by the research team. For this acceptability study, 15 surveys examined the extent to which this service-learning opportunity addressed the established gap in medical student education regarding exercise principles and practices.
Closed-ended data were analyzed within Qualtrics. The team conducted open-ended analysis by coding responses for themes using an inductive approach. 16 The primary outcome examined was students’ reported gain in exercise knowledge. Secondary outcomes included confidence gained in providing exercise counseling, changes in personal behaviors, satisfaction with the virtual format, and experience gained in virtual teaching. Student satisfaction with teaching and class effectiveness were compared between cohorts through a chi-square test and significance was determined at P < .05. The study was deemed exempt by USC’s IRB (UP-20-01400).
Results
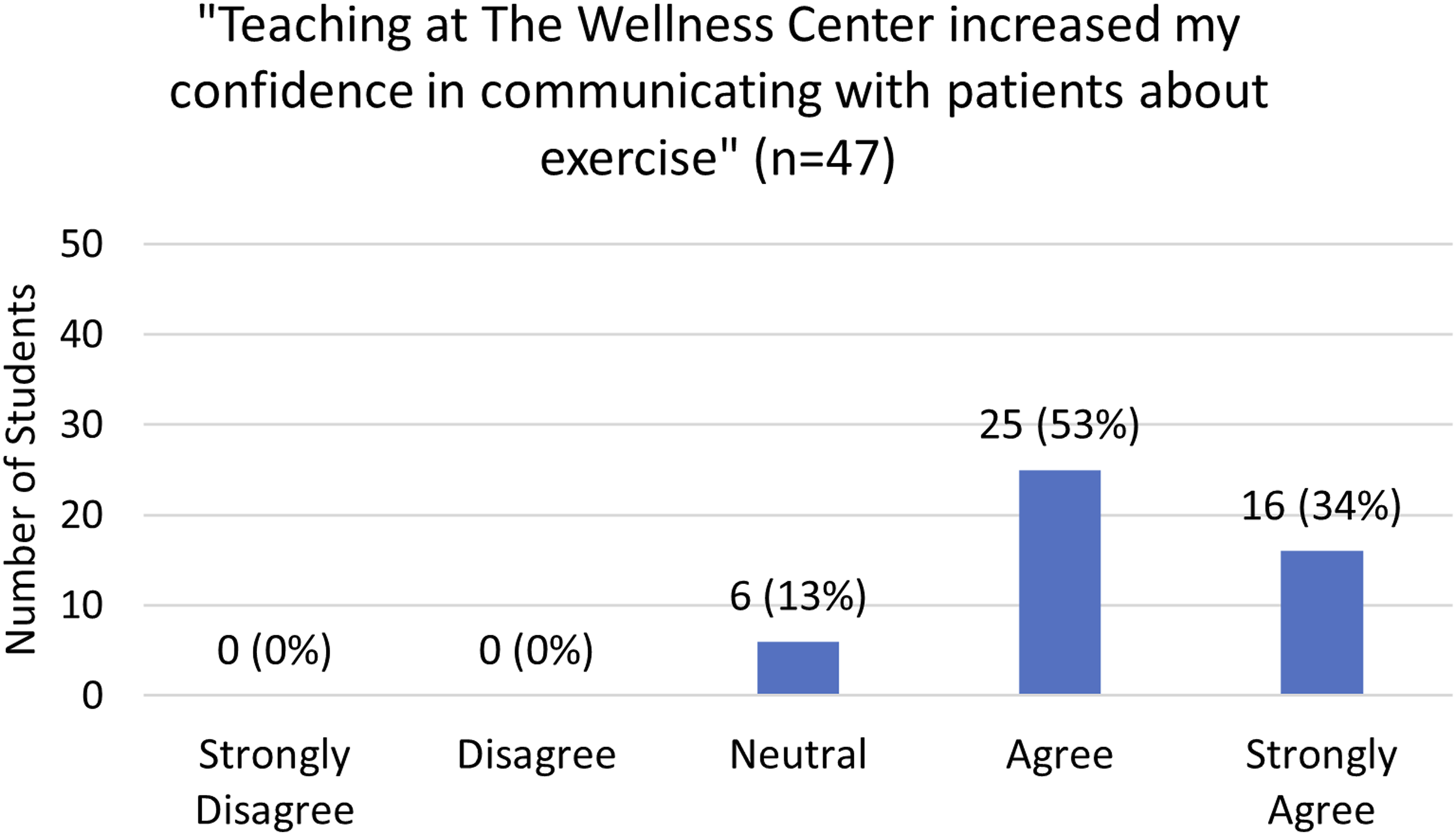
There were a total of 47 survey responses from MS1s (n = 45) and MS2s (n = 2). The overall response rate was 70% (n = 47/67), with 69% (n = 24/35) for Cohort 1 and 72% (n = 23/32) for Cohort 2. Students reported that teaching the classes increased their knowledge of exercise principles (ie, muscle groups, exercise types, exercise recommendations), with 19% (n = 9) strongly agreeing, 51% (n = 24) agreeing, 26% (n = 12) neutral, and 4% (n = 2) disagreeing (Figure 1). Additionally, most students reported that teaching increased their confidence counseling patients about exercise with 34% (n = 16) strongly agreeing, 53% (n = 25) agreeing, and 13% (n = 6) neutral (Figure 2). Exercise knowledge. Confidence in exercise counseling.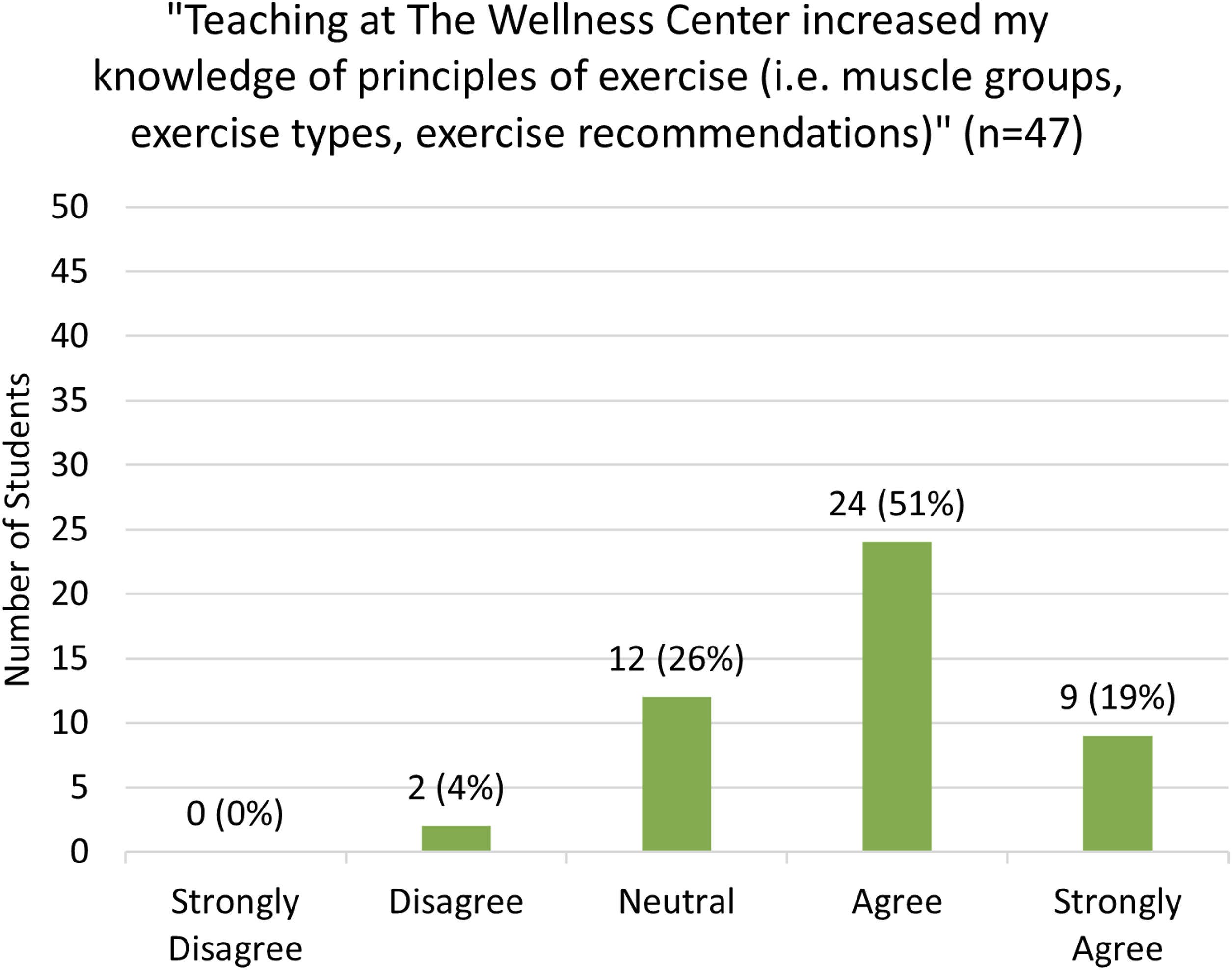
In a follow up question, Cohort 1 students (n = 24) discussed how exercise teaching may affect future patient counseling. Students reported increased likelihood to counsel their patients on attending community-based exercise classes (83%, n = 20), specific exercises (67%, n = 16), the components of an exercise program (67%, n = 16), and recommended exercise goals (63%, n = 15) (Figure 3). Additionally, Cohort 1 students (n = 24) were asked about their own exercise habits. Students reported that they planned to increase their exercise frequency (50%, n = 12), increase their exercise time (46%, n = 11), vary their types of exercises (38%, n = 9), and add specific exercises to their routines (29%, n = 7) based on the exercise class they taught (Figure 4). Likelihood to counsel about exercise. Likelihood to make changes in exercise habits.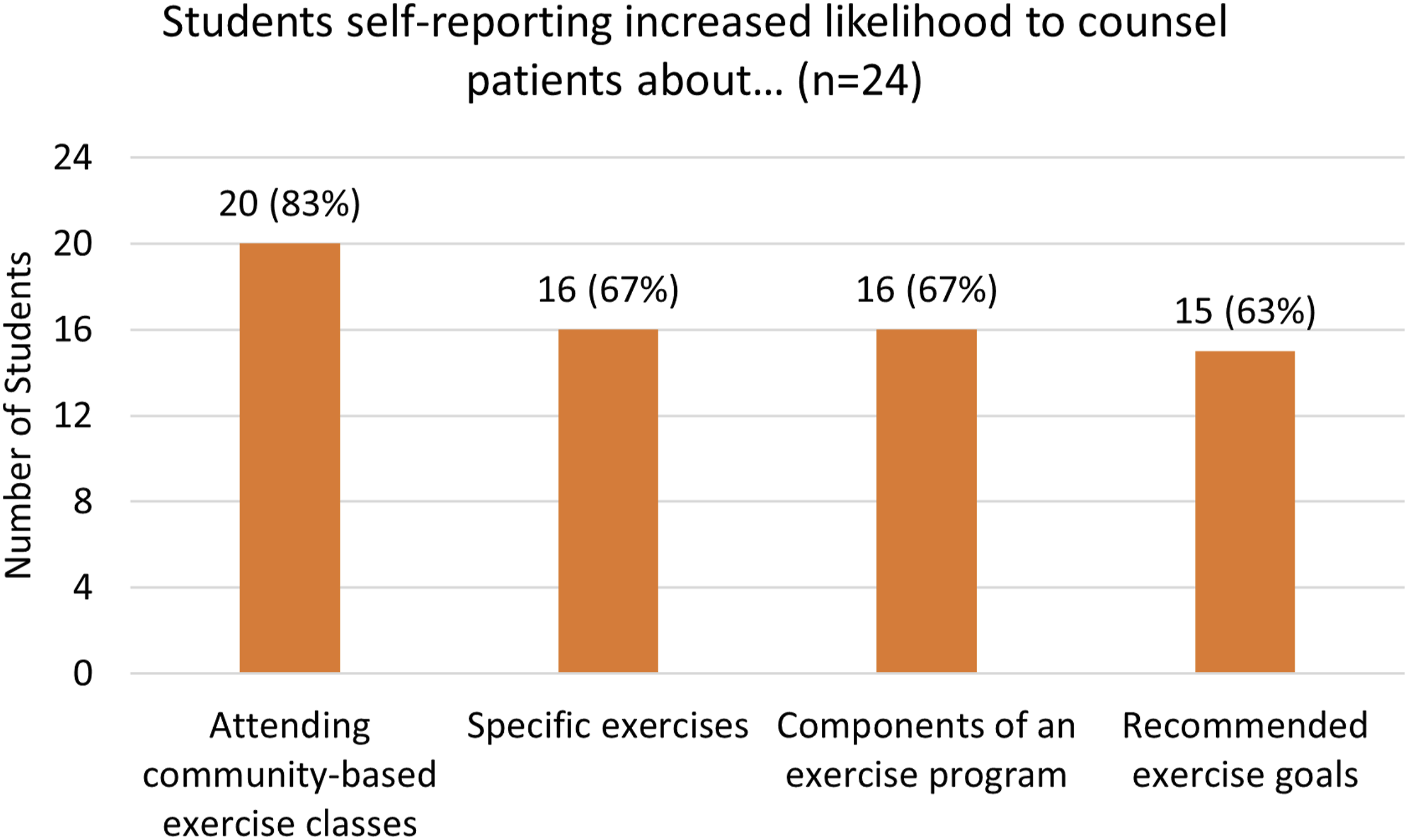

Participants in both cohorts (n = 44) reported learning new professional skills including: confidence with public speaking (n = 41, 93%), communicating information in an accessible way (n = 41, 93%), encouraging patients to actively participate in their health (n = 40, 91%), collaborating with others (n = 40, 91%), clarifying and answering patient questions (n = 38, 82%), giving an engaging presentation (n = 35, 80%), and teaching group classes (n = 35, 80%). Students reported that the virtual Cohort 1 and hybrid virtual/in-person Cohort 2 formats were very effective (57%, n = 27) or somewhat effective (43%, n = 20) to teach participants. There was no statistically significant difference in perceived effectiveness of class format between Cohort 1 (very effective: n = 11, somewhat effective: n = 13) and Cohort 2 (very effective: n = 16, somewhat effective: n = 7) (P = .10). Students were also overall satisfied with teaching in both formats, with 62% (n = 29) reporting they were very satisfied, 36% (n = 17) reporting they were mostly or somewhat satisfied, and 2% (n = 1) reporting they were somewhat unsatisfied. However, Cohort 2 was significantly more satisfied with the teaching format (very satisfied: n = 20, mostly satisfied/somewhat satisfied/somewhat unsatisfied: n = 3) compared to Cohort 1 (very satisfied: n = 9, mostly/somewhat satisfied: n = 15) (P = .00049).
In their free responses, Cohort 1 respondents (n = 24) identified 3 main learning areas (Table 3): 1. Communication (54%, n = 13)—learned how to effectively use verbal cues and visual aids (i.e., handouts) to communicate with participants in a virtual platform 2. Engagement (46%, n = 11)—learned to promote participant engagement through check-ins and encouraging/motivating statements 3. Presentation (25%, n = 6)—learned the importance of being aware of the camera and making sure they were in view to maintain participants’ attention Telemedicine Lessons Learned With Student Quotes.
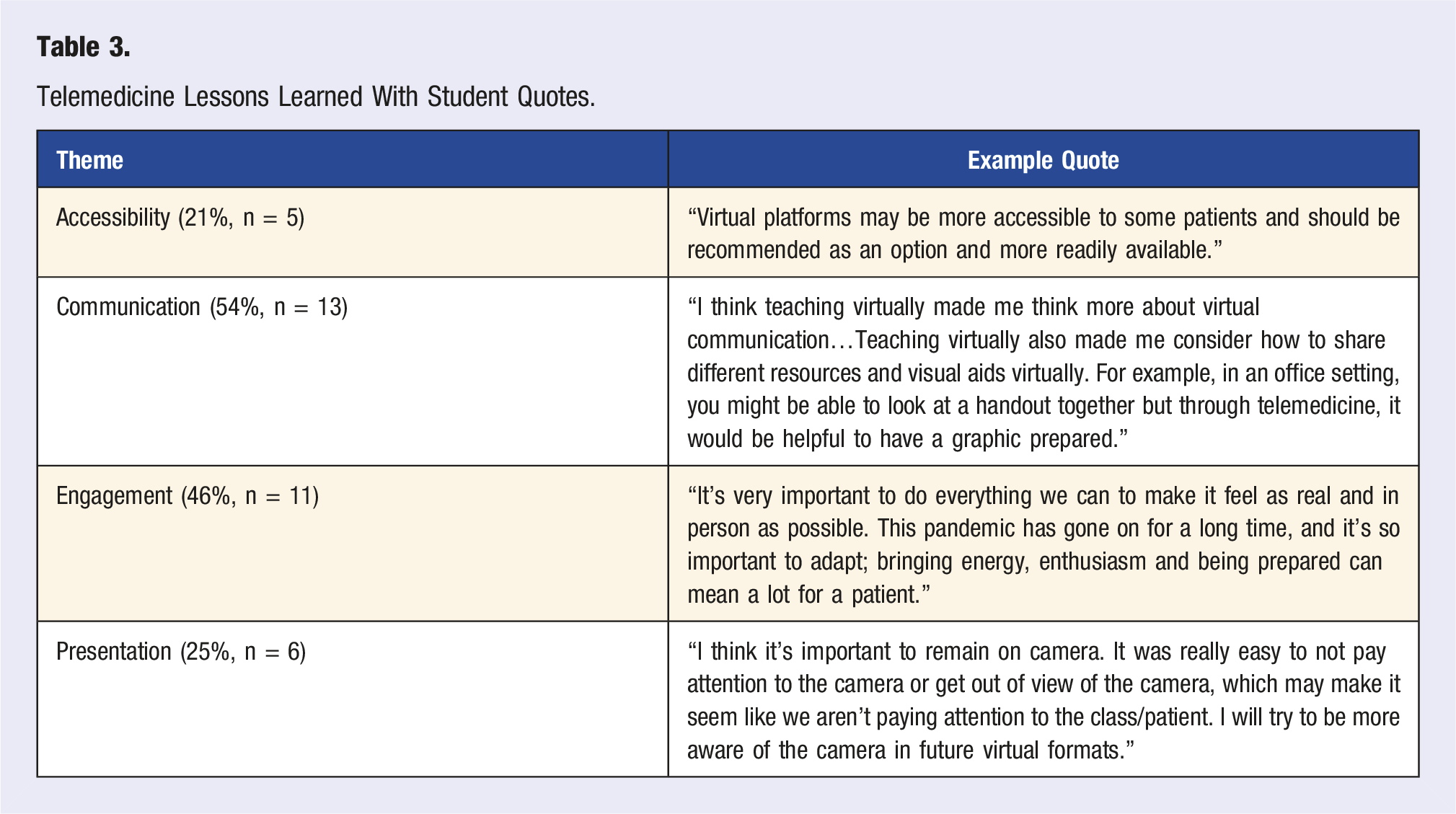
Further, students’ free responses noted how virtual teaching could increase health education accessibility (21%, n = 5).
Discussion
Exercise is a critical component of disease prevention and chronic disease management. Yet, medical students receive little formal training in exercise and do not feel prepared to provide optimal exercise counseling to their future patients.6,8 Training medical students to teach exercise classes may better prepare future physicians in lifestyle medicine skills, including counseling patients, supporting patient rehabilitation, and improving overall patient health.
This study demonstrated that medical students who received supplementary exercise education and taught exercise classes reported increased knowledge of exercise guidelines and increased confidence in their ability to counsel patients about exercise. Students reported that their experience would make them more likely to counsel their future patients about exercise goals, types of exercise, and community-based exercise resources. Additionally, results suggest that teaching exercise may motivate students to make positive changes to their own exercise habits, which may ultimately benefit their patients, as research shows that physicians who themselves exercise are more likely to counsel their patients about exercise. 17 While this study focused on the student experiences with teaching exercise, we previously conducted a study that analyzed the experiences of participants who attended these classes virtually and found positive effects on participant knowledge and experience as well. 14 Our study results are consistent with previous literature describing the benefits of service-learning for medical students community members, with students experiencing enhancement of intra- and inter-personal skills, academic and professional skills, civic engagement, and social responsibility.18,19
Additionally, this study supported the use of virtual teaching to deliver patient education. Students gained experience engaging participants virtually, a useful skill given the expanding role of virtual care in medicine. 20 In this way, student experience with virtual health education seems to parallel research showing participant’s positive experiences with virtual health delivery.14,21
Limitations of this study include a small sample size, variability in the course content taught weekly, and reliance on student self-report data. Additionally, a pre survey was not conducted to assess baseline knowledge and behavior, so change from baseline could not be measured. Lastly, because PCP students elect to participate in PCP due to their interest in primary care, they may have more knowledge of and interest in lifestyle medicine compared to other medical students, potentially limiting the generalizability of our findings.
To address some of these limitations, starting in Fall 2023, standardized slides were added to each week’s presentation so that all students teach WHO recommendations for frequency and duration of cardiovascular and strength training exercise and a standard list of exercise benefits. Additionally, the next Cohort of student teachers will be surveyed about their exercise knowledge, counseling comfort, and personal exercise habits both before and after they teach at the LAGWC.
In addition to capturing the effects of the above changes, future studies will examine a larger cohort of students longitudinally to assess their retention of exercise knowledge and counseling confidence. Future studies should also measure actual changes in students’ exercise habits and compare these changes with peers who did not participate in exercise teaching.
Conclusion
In summary, the virtual and hybrid virtual/in-person exercise classes were successful in teaching foundational exercise principles to future physicians early in their medical training. Medical students reported that teaching these classes encouraged them to make and recommend healthy lifestyle choices for themselves and their future patients, respectively. Additionally, the classes provided a service to the community, offering participants multiple modalities to engage in exercise based on preferences and abilities, all while highlighting community outreach in primary care. This paper offers a replicable model to teach medical students about exercise through service-learning. More widespread inclusion of exercise training early in medical education may improve exercise knowledge, counseling confidence, and lifestyle medicine habits among the next generation of primary care physicians.
Supplemental Material
Supplemental Material - Service-Learning Through Community-Based Exercise Teaching Enhances Medical Students’ Exercise Knowledge, Counseling Confidence, and Habits
Supplemental Material for Service-Learning Through Community-Based Exercise Teaching Enhances Medical Students’ Exercise Knowledge, Counseling Confidence, and Habits by Isabel Edge, MD, Jo Marie Reilly, MD, MPH, FAAFP, and Ilana Greenberg, MPH in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Service-Learning Through Community-Based Exercise Teaching Enhances Medical Students’ Exercise Knowledge, Counseling Confidence, and Habits
Supplemental Material for Service-Learning Through Community-Based Exercise Teaching Enhances Medical Students’ Exercise Knowledge, Counseling Confidence, and Habits by Isabel Edge, MD, Jo Marie Reilly, MD, MPH, FAAFP, and Ilana Greenberg, MPH in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors wish to acknowledge Bryan Ayala-Rivera; John Javier, PT, DPT, OCS; Lucy Hernandez; Nathalie Sami, MD; and Victoria Dunn, MBBS, MRCGP, DRCOG for their assistance in the development and administration of the LAGWC exercise classes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.