
Abstract
Introduction
Nutrition education and counseling are critical to patient health. Primary care physicians are positioned to provide this counseling; however, due to a lack of nutrition education, many physicians-in-training lack these skills. This study evaluates the knowledge and self-efficacy of Keck School of Medicine (KSOM) of University of Southern California (USC) Primary Care Program (PCP) medical students after leading community-based nutrition classes.
Methods
First-year PCP KSOM students completed a survey immediately after teaching nutrition classes (Phase I: Spring 2017-Spring 2020) and 1-4 years after teaching (Phase II: August 2021). Open-ended responses were coded thematically, and descriptive data were analyzed in Qualtrics.
Results
There were 93 phase I respondents; however, not everyone answered every question. Among 45 question respondents, students reported learning about macronutrients (29%), portion sizes (16%), glycemic index (15%), and metabolic syndrome (12%). Among 57 question respondents, 49% reported having knowledge to now counsel patients about nutrition. There were 60 phase II respondents. Students reported sustained, increased nutrition knowledge (88%) and confidence (85%) from baseline, and making healthy personal dietary changes.
Discussion
It is important for physicians-in-training to gain nutrition education early in their career. This training can benefit student knowledge, behavior change, confidence, and their future patients through counseling.
PCP students were taught nutrition concepts and then led required service-learning nutrition education classes for local community members.
Introduction
Chronic diseases like diabetes, hypertension, and high cholesterol are common worldwide and have been linked to increased weight.1,2 In the United States, one third of adults have a BMI over 25, classified as overweight, and another third over 30, classified as obese. 3 It is estimated that one third of children born after the year 2000 will have diabetes in their lifetime. 4 Nutrition-related illnesses are preventable but many adults lack the knowledge to make dietary changes.5,6 Additionally, there are racial and ethnic disparities in diseases and deaths related to nutritional deficiencies, type 2 diabetes, and obesity prevalence.7-9 Preparing the physician workforce through nutrition training, as well as understanding food insecurity and dietary cultural nuances, 10 are critical to advocating for change.
There is a significant void in nutritional training in undergraduate and graduate medical education globally. 11 A recent British study indicated that less than 70% of medical students had more than 2 hours of nutrition training. 12 In 2015, 71% of US medical schools did not meet the minimum 25-hour National Research Council recommendation for nutrition education, averaging 20 hours. 13 50% of graduating medical students do not believe they have sufficient nutrition knowledge to counsel patients. 14 A survey of US residents, fellows, and practicing physicians found that on average, they answered only 50-66% of the nutrition knowledge questions correctly. 14 Once in practice, fewer than 14% of US, and 26% of British, physicians believe they were adequately trained in nutritional counseling.15,16 Training physicians in lifestyle management skills is critical to improving their abilities to guide patients and improve their own health.
In response to the deficiency in undergraduate and graduate medical education nutrition curriculum, there has been improved USA efforts.17-19 These reforms are consistent with recommendations made by the 2016-2025 United Nation Decade of Action on Nutrition to improve nutrition education. 20 While these reforms are exemplary, globally there remains a paucity of consistent, evidence-based nutrition curriculum across medical education.
At Keck School of Medicine (KSOM) of University of Southern California (USC), approximately 80% of medical students were not satisfied with the quality and quantity of their nutrition education and 65% did not feel confident discussing diet with patients. 21 In response, the KSOM Primary Care Program (PCP) developed a nutrition service-learning course for its primary care track pipeline students. This study describes and evaluates the knowledge and self-efficacy of these KSOM PCP students after leading community nutrition courses immediately after teaching and 1-4 years later, looking at levels of self-reported nutrition counseling confidence, nutrition knowledge, and personal lifestyle behavior changes.
Methods
Didactics
The Nutrition for Prevention and Chronic Illness Management course taught PCP first year medical students (MS1s) (between 19-25 MS1s each year) the fundamentals of nutrition as chronic disease prevention and then allowed students to apply this knowledge through service-learning community-based nutrition teaching. The course was funded through the PCP, with PCP physician support provided “in-kind.” PCP physician faculty taught the MS1s a 2 hour, community-focused nutrition curriculum in August of their first semester. This curriculum was developed by the physician faculty in consultation with a dietician. The curriculum was the same content that students would later teach during the service-learning component and was supplemental to the 4-hour core nutrition curriculum taught to all KSOM MS1’s by the same PCP physician team.
Service-Learning
Beginning in September, students taught the English/Spanish nutrition/cooking course weekly free of charge in the Los Angeles County Wellness Center (LACWC) kitchen, a community-based center.
22
12 unique classes were taught in the fall (September-December) and then repeated in spring (January-April) (Figure 1). From August 2016 until March 2020, this course was delivered in-person to 20-50 participants weekly. Due to Covid-19, the classes were taught virtually from September 2020-March 2022 and both in-person/virtually since March 2022.
23
This paper focuses on the in-person student teaching experience. Of note, the curriculum has been published on the Family Medicine Digital Resource Library (FMDRL) and 2 classes have since been added that are included as supplemental material.
24
Nutrition and cooking class topics and schedule taught by medical students.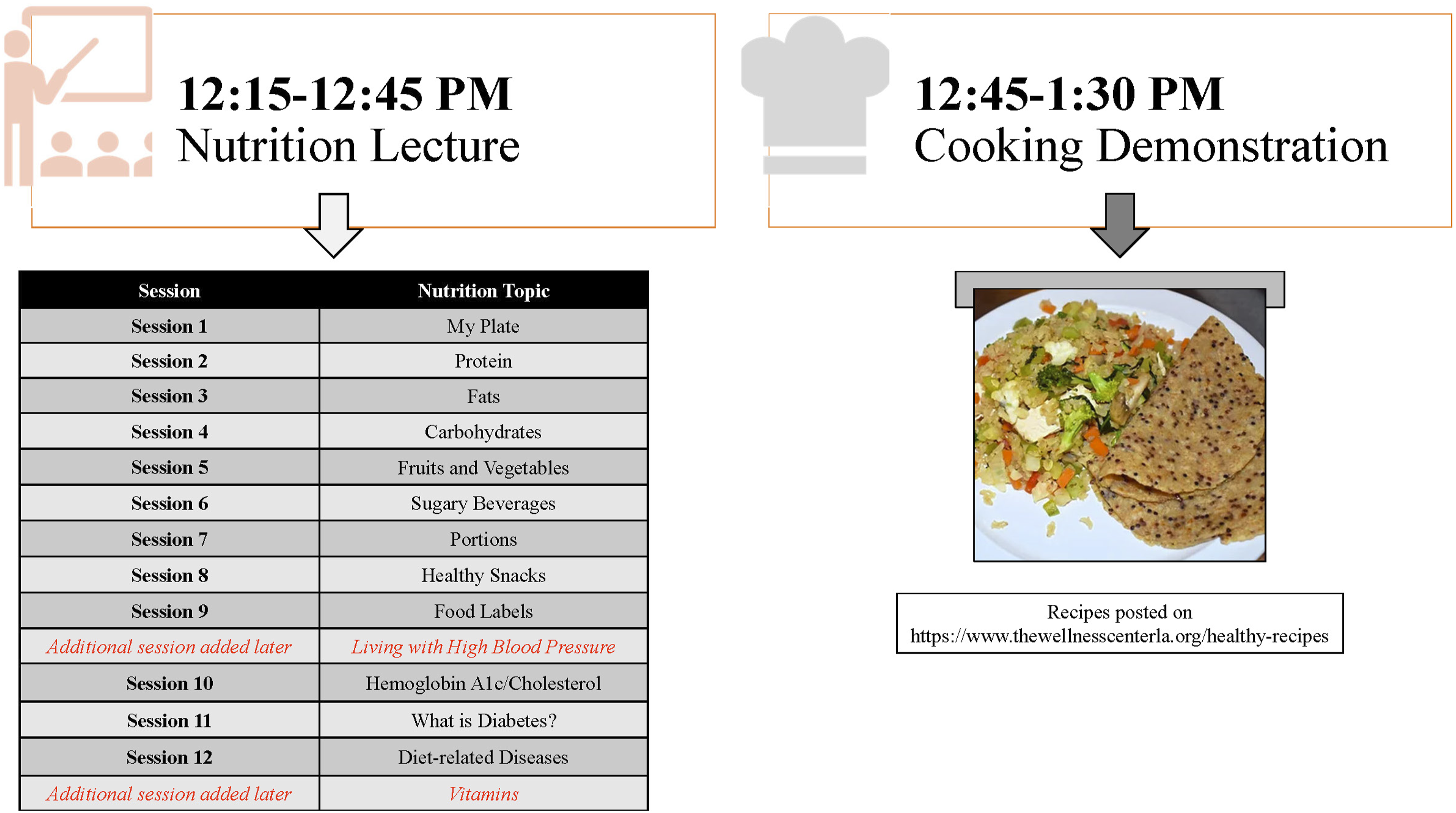
Students taught the nutrition classes in groups of 2-3 and students each taught 1 class during the fall and spring semesters. The 1.5 hour class consisted of a nutrition presentation and Q&A (45 minutes) and cooking demonstration (45 minutes) with a bilingual English/Spanish chef (Figure 1). At least 1 student spoke Spanish in each group. One week prior to teaching, the students were given 5-10 pre-developed English/Spanish nutrition slides for that week’s topic. Students reviewed the material and then developed 3 questions to ask participants. During the presentation, students used plastic food models (healthedco.com) and educational handouts (livingwithdiabetes.org) to enhance their teaching. Students and bilingual PCP faculty co-moderated and co-facilitated participants’ questions.
The spring semester classes culminated in an annual 3 hour Diabetes Day (DD) event. DD attracted a broader audience with a larger promotional outreach. During DD, multiple nutrition presentations were delivered by all PCP MS1s. The nutrition lectures were delivered separately in English and Spanish, and the cooking was taught together in both languages.
Cooking Demonstration
At the beginning of each cooking session, the English/Spanish recipes were given to the students and participants. These recipes were developed weekly by a bilingual, bicultural chef and reinforced the healthy eating topics discussed during each class. Recipes have since been developed into a bilingual cookbook, provided to class attendees for free. 25 Under the chef’s supervision, the students prepared the food alongside the community participants under the chef’s supervision.
Evaluation
Phase I Response Data.
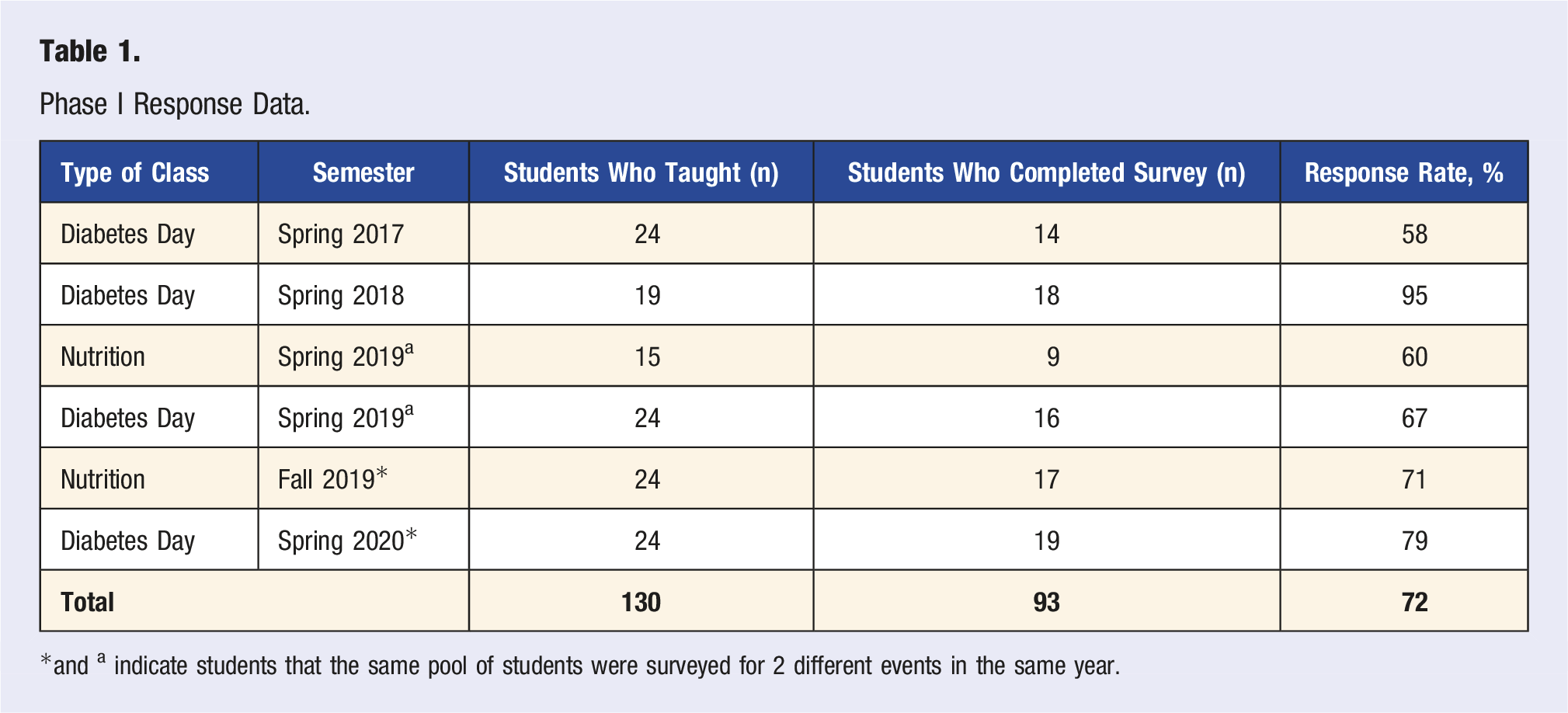
*and a indicate students that the same pool of students were surveyed for 2 different events in the same year.
Results
Phase 1: Post-Teaching
130 surveys were sent to the MS1s directly after they taught the nutrition/DD classes with a total of 93 responses (72%) (Table 1).
45 students responded to the question of what nutrition information they learned from teaching. Their answers included learning about macronutrients (proteins, carbs, fat, fiber, lipids) (29%, n = 13), portion sizes (16%, n = 7), glycemic index (15%, n = 6), and metabolic syndrome (12%, n = 5). 40 students responded to the question of what patient education resources they learned from teaching, including learning about My Plate (43%, n = 17), the LACWC as a resource (30%, n = 12), and the educational handouts as a resource (18%, n = 7). 57 students responded to the question of how teaching would impact their patient care, with 49% of students (n = 28) noting they would implement nutrition counseling discussions during patient interactions. Students also learned about delivering culturally responsive health care, specifically understanding specific cultural food staples when counseling patients (n = 15, 26%). One student reported: “People’s diets depend a lot on their culture. This is definitely something doctors should take into account...”
Phase 2: Follow-Up Survey
Of the eligible medical students who taught nutrition/DD as a MS1 (n = 92), 60 (65%) completed the follow-up survey in August 2021. The breakdown of respondents among all students contacted each year included: 20 3rd year medical students (n = 20/25, 80%), 19 4th year medical students (n = 19/24, 79%), 15 interns (n = 15/19, 79%), 5 residents (n = 5/24, 21%). One respondent did not indicate their training level.
In the 1-4 years post teaching these classes, 88% (n = 53) of students felt their knowledge about macro and micronutrients, food labels, and nutrition for chronic diseases increased because of their earlier teaching. 85% (n = 51) felt their confidence in communicating with patients about nutrition increased because of this teaching. Specifically, students noted increased likelihood to counsel patients about the following: nutrition interventions for diabetes control/prevention (78%, n = 47), portion sizes (75%, n = 45), sugary beverages (75%, n = 45), My Plate (72%, n = 43), resources for attending community-based nutrition classes (62%, n = 37), and nutrition interventions for hypertension control/prevention (62%, n = 37). Lastly, students reported that teaching at the LACWC inspired personal health changes: 55% (n = 33) reduced their portion sizes, 52% (n = 31) drank more water, 50% (n = 30) ate more fruits and vegetables, 47% (n = 28) made healthy food substitutions, 43% (n = 26) reduced sugary beverages, and 40% (n = 24) read food labels.
Discussion
With chronic diseases globally at record highs and physicians poorly trained in nutrition counseling for lifestyle management, medical student dietary education reform is critical. PCP students were taught nutrition concepts and then led required service-learning nutrition education classes for local community members. These students self-reported improved and sustained nutrition knowledge, confidence, and personal health behavior change, both directly, and 1-4 years after this nutrition education and applied teaching. Due to the Covid-19 pandemic, the nutrition classes pivoted to a virtual format. Preliminary data has shown similar gains in student knowledge and patient education impact. 23 While isolating the service-learning nutrition training as the only contributing experience to our student’s increased nutrition confidence, knowledge, and healthy behavior change is difficult 1-4 years later, we believe that it contributed to their overall nutritional education confidence and performance. There is a tremendous paucity and variability of directed dietary education teaching and counseling in medical school and residency, including in our program. As such, we believe teaching dietary nutrition skills, followed by applied and supervised service-learning with community members, is a viable model to teach early medical learners. Further, there is currently no single, validated survey instrument in the literature assessing student’s nutrition knowledge and behavior change across their medical training and our study helps contribute to evaluating such training.
Limitations
Study limitations include a small sample size and the possibility of selection bias. Phase 1 respondents during the 2018-2019 and 2019-2020 academic years may have answered the survey twice, which perhaps favored more motivated and/or satisfied students. The Phase 2 survey had a response rate of 65% which may not represent all students who taught, especially residents who had the lowest response rate (21%). Further, there was a lack of a control group to assess medical students who did not participate in this nutrition training. Students also self-reported their knowledge and personal behavior changes. Finally, students who participated in the nutrition teaching are part of a primary care track and may have had a vested interest in primary care, chronic disease prevention, and health education that was not representative of non-primary care bound students.
Nutrition Curriculum Applications
The bilingual English/Spanish nutrition curriculum 24 addresses the core pillars of chronic disease management and nutrition. It is adapted for learners with a lower language and health literacy, multiple ages from youth to older adults, and is culturally appropriate. Further, it is adapted for multiple teaching and community settings, and can be delivered by a wide audience, including nontraditional educators (i.e., promotoras). The lecture topics can be given on their own, given in series, or a combination of both. The bilingual English/Spanish curriculum is most effectively delivered by an individual or group who feel comfortable speaking both languages.
Conclusion
It is crucial for physicians-in-training to gain nutrition skills early in their medical education to best serve their future patients and impact their own health habits. Students who participated in the KSOM’s Nutrition for Prevention and Chronic Illness Management course reported sustained increases in their nutrition knowledge, personal health behaviors, and patient counseling skills/confidence. Medical student dietary training, followed by direct application, may be an effective training model for nutrition competency. Medical schools should consider similar student nutrition service-learning educational opportunities as a tool for sustained dietary counseling and skill-based training.
Footnotes
Acknowledgments
We would like to acknowledge Lindsay Nagatani-Short for assistance with this data collection. This data has been presented at the Teaching Kitchen Research Conference at University of California, Los Angeles (UCLA) on Tuesday, October 18, 2022.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.