
Abstract
Objective: The systematic review with meta-analysis aimed to verify the occurrence of a protective effect on hearing loss due to a higher intake of carotenoids, vitamins A, C, E, and folate present in diets. Methods: The search for scientific articles was carried out by 2 independent researchers in electronic databases. Meta-analysis was performed by constructing summary risk measures for each vitamin or antioxidant, combining the risk ratios or adjusted odds ratios (OR) for the various variables observed in the highest categories of vitamin or antioxidant consumption. Results: Five studies involving an estimated 100 549 participants were included in the quantitative synthesis. The summary measures calculated for the highest quartiles/quintiles of the studies were Hazard ratios (HR) .990 for vitamin C; HR 1.07 and OR .925 for vitamin E; HR .921 for folate and OR .906 for vitamin A. Conclusion: Dietary intake of vitamins and antioxidants was inversely associated with the risk of developing hearing loss. Individuals with a higher intake of antioxidants may have better hearing thresholds, especially with the intake of β-carotene.
“Dietary patterns characterized by a higher intake of nutrients such as vitamins and antioxidants may represent protective factors for the central auditory system.”
Introduction
Hearing loss (HL) represents a growing problem for public health worldwide. Approximately 466 million individuals worldwide suffer from HL, and the prospect of new cases is expected to increase to more than 900 million by 2050. Individuals with HL are more likely to have impaired activities of daily living, an impact on quality of life, and consequently a higher risk of cognitive decline and depression or other mental illnesses. HL is usually irreversible, so identifying potentially modifiable risk factors that can inform prevention strategies is extremely important. 1
Environmental factors, such as noise and ototoxic drugs, are among the known stressors that can induce early and effective HL. Decreased levels of essential nutrients, such as vitamins, appear to be associated with HL. 2 Despite the complexities associated with the identification of the relationships between nutrients, diet, and hearing function (including the development and progression of HL), there are reports of evidence suggesting a protective effect of nutrients presenting antioxidant, anti-inflammatory, and anti-ischemic properties and thus promote the reduction or prevention of HL. 3
Hearing loss is conceptually defined by age-related sensorineural HL as a bilateral and irreversible condition, affecting the sensory and/or a neural portion, manifested by an impairment in the ability to detect high-frequency sounds, affecting speech discrimination, recognition, and understanding. Hearing loss results from the gradual degeneration of sensory cells, ciliated cells of the Corti Organ, stria vascularis, and neurons of the spiral ganglion, accelerated by advancing age, mitochondrial DNA mutations, oxidative damage, exposure to noise, ototoxic drug use, and poor diet. The inner ear, composed of peripheral auditory and vestibular organs, resembles the brain in some aspects, making it comparatively susceptible to influences from gut microbiota. 3
Certain foods, especially fruits and vegetables, have antioxidants in their composition, such as vitamins C, E, and A, chlorophyll, flavonoids, carotenoids, curcumin, and others, besides presenting characteristics to reduce the spread of chain reactions and free radical-induced lesions. 4 The intake of carotenoids, vitamins A, C, E, and folate may play an important role in preventing/protecting hearing disorders. The otoprotective effects of free radical scavengers and the antioxidant properties of vitamins C and E and β-carotene are cited. These compounds have demonstrated protective action against damage to the inner ear caused by aminoglycosides, cisplatin, acoustic trauma, noise exposure, and HL.5,6
The implementation of hearing health promotion strategies, as well as the early diagnosis and rehabilitation of these conditions, can reduce or minimize the impact of HL on individuals. 7 Thus, knowing prevention forms, especially those involving individuals’ nutrition, can favor implementing these strategies. Therefore, interventions aimed at health promotion and that consider the singularities of the subjects point out actions capable of promoting the social participation of these individuals in the community in which they are inserted and can help the population have greater social participation. 8
The free radical aging theory postulates that aging results from increased or accumulated oxidative damage caused by free radicals. The prevention of age-related HL is a relatively new area of research. However, it is reported that the association of vitamin intake in the diet is significantly associated with a decrease in the prevalence of HL associated with age. 9
Thus, this systematic review with meta-analysis (SR-Met) aimed to verify the occurrence of a protective effect on HL due to higher intake of carotenoids, vitamins A, C, E, and folate present in the diets. The objective was to answer the guiding question: What is the protective effect of dietary vitamins A, C, E, carotenoids, and folate on hearing loss when comparing the group with the highest amount ingested in the diet (group of individuals in the last quartile/quintile of ingested concentration) with the group of individuals with the lowest intake (first quintile or quartile)? The assessment measure (protective effect) consisted of the Odds ratios (ORs)—(studies using logistic regression in this assessment) or the Hazard ratios (HRs)—(studies using Cox regression in the assessment).
Method
Study Design
The search for scientific articles was conducted by 2 independent researchers in the electronic databases MEDLINE (Pubmed), LILACS, SciELO, SCOPUS, WEB OF SCIENCE, and BIREME, without period, and location restriction. Select articles in Portuguese, English, and Spanish. The research was structured and organized in the PICOS form, representing an acronym for target
Research Strategy
The descriptors were selected from the controlled vocabularies Health Sciences Descriptors (DeCS) and Medical Subject Heading Terms (MeSH), given their wide use by the scientific community for indexing articles in the PubMed database. The search strategy used was combining the descriptor and Boolean operator: (Dietary supplements) and (hearing loss). The search occurred in a concentrated manner in December 2021.
Eligibility Criteria
Studies without language, period, and location restrictions were included. The average of the studies included for evaluation obtained a score of 12 in the modified protocol of Pithon et al (2015) 10 to evaluate their quality.
Risk of Bias
The quality of the methods used in this research was independently evaluated by the reviewer, according to the PRISMA recommendation (Preferred Reporting Items for Systematic reviews and Meta-Analyses). 11 The evaluation prioritized a clear description of the information.
Exclusion Criteria
Studies published in the formats of Letters to the editor, guidelines, literature reviews, narrative reviews, systematic reviews, meta-analyses, and abstracts were excluded. Studies unavailable in full or that the authors did not have access through contact with the authors, releases in libraries and research bases, were also excluded.
Data Collected
After screening, the text of the selected article was reviewed in detail and extracted in a standardized manner by one of the authors under the supervision of the third judge, identifying the year of publication, place of research, the language of publication, type of study, sample size (population studied), monitoring of HL population studied through tests performed, age of the population, sex of the population studied, total individuals with HL, risk estimates according to the regression model used in the study [HR or OR comparing the highest category of dietary intake vs the lowest category (represented by the value of 1.0) with their corresponding 95% confidence intervals], method, result, and conclusion of the study.
Clinical Outcome
The clinical outcome of interest was to verify the effect of dietary intake of carotenoids, vitamins A, C, E, and folate associated with HL. Studies that did not use the defined approach (evaluation of amounts of these nutrients in diets through questionnaires or “24-hour recall” in patients with or without HL) were not part of the meta-analysis sample.
Statistical Analysis
The meta-analysis was performed by constructing summary risk measures for each vitamin or antioxidant by combining the HRs or ORs adjusted for the various variables (multivariable-adjusted HR or OR) observed in the highest categories of vitamin or antioxidant consumption. The inverse variance method was used to evaluate the weighting of each study. For this, the standard error of the natural logarithm of each risk measure was calculated from its lowest values presented in the 95% CI and considered as the estimated variance of the logarithm HR or OR. Heterogeneity was evaluated by calculating the Q statistic (P < .05 indicating the presence of heterogeneity in the studies) and the I2 statistic (a value greater than 50% indicating substantial heterogeneity through the articles). The fixed-effects model was adopted for constructing the summary measures in the forest graphs considering that the observed heterogeneity was not very prominent. All analyses were performed using MedCalc® Statistical Software version 20.110.
Results
Selection of Studies
Initially, n = 392 articles were selected, resized to n = 385 after exclusion by repetition in the consulted databases; then, the titles and abstracts were analyzed, and n = 380 were excluded because they were not within the scope of the research proposal. Then, 5 articles were admitted to the final analysis, and all were included in the present research (Figure 1). Flowchart of identification, eligibility, and inclusion of articles.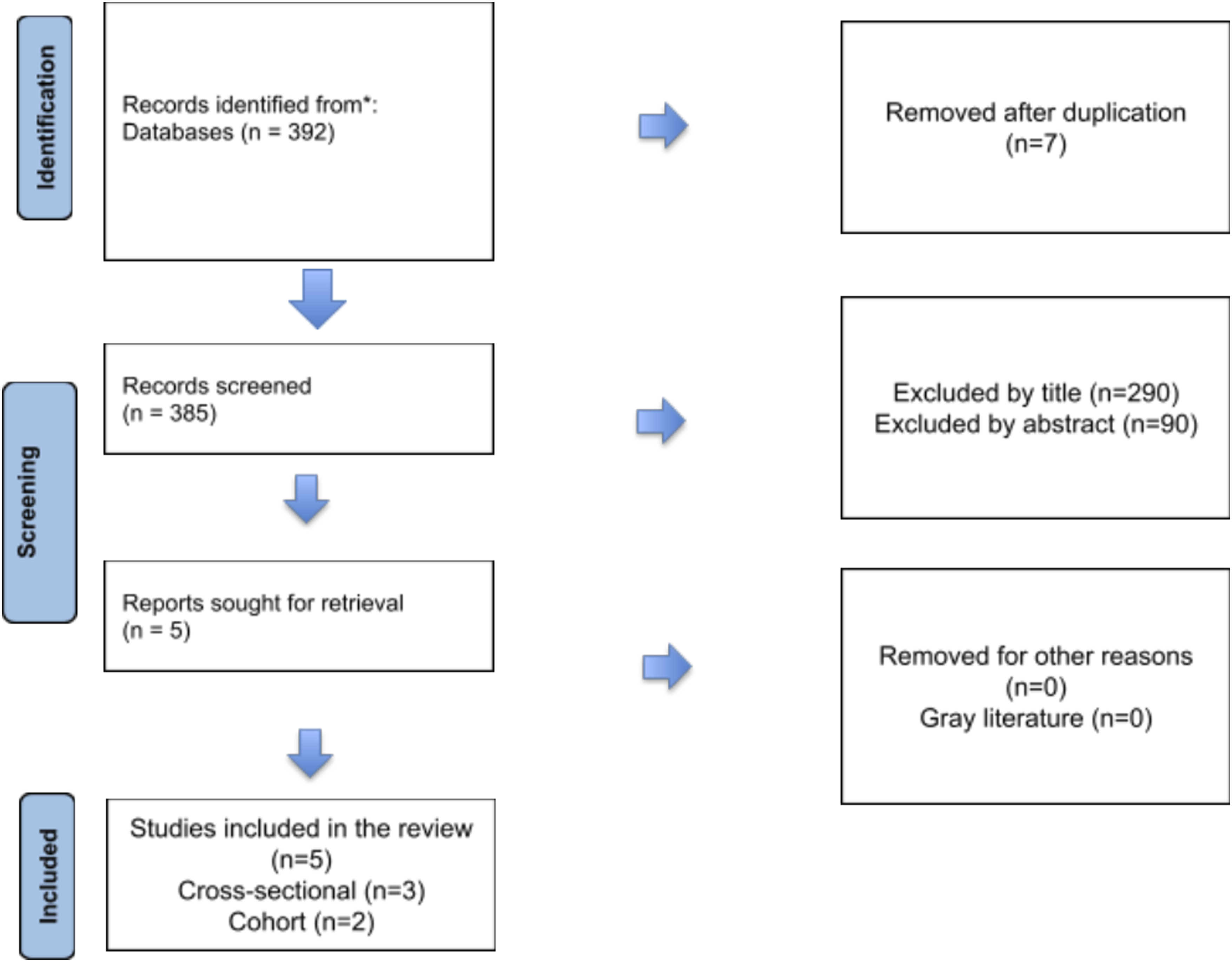
Design of Studies
The study by Shargorodsky et al (2010) 4 was performed with n = 26 273 men aged 40-75 years. Participants completed a detailed questionnaire on diet, medical history, and drug use [Semiquantitative food frequency questionnaire (SFFQ)]. Furthermore, the interviewees were asked every 2 years about the use of vitamin supplements, including the type, dose, duration, and specific brand. The total intake of each nutrient was calculated by multiplying the frequency of consumption of each food by the nutrient content of the specified portion size.
In another research, 12 n = 2956 subjects over 50 years old participated. Participants were invited to participate and be followed up for 5 years. Dietary data were obtained through the questionnaire “Self-administered food frequency questionnaire (FFQ) modified for Australian diet.” Besides, the Australian Tables of Food was used to calculate the nutrient intake. The audiological examination was obtained by pure-tone audiometry at frequencies of .25, .5, 1, 2, 4, 6, and 8 kHz.
In the study by Choi et al (2013), 13 the authors aimed to examine associations between the intake of antioxidant vitamins and magnesium with hearing thresholds in North American adults. Participants were n = 2592 subjects aged 20-69 years, from 2001 to 2004. Pure-tone air-conduction hearing thresholds were obtained for each ear at frequencies of .10-8 kHz in an intensity range of −10 to 120 dB NPS. The dietary intake of antioxidants and magnesium was estimated through an interview with a 24-hour recall. The interviews requested a list of all foods and beverages consumed by the interviewee, except drinking water, 24 h before the interview, quantities of food reported, and detailed descriptions of food.
The daily intake of nutrients from selected food items was determined by multiplying the content of each nutrient in each food item by its daily intake. Data on participants’ daily food intake were estimated as the sum of all food sources. Information on the use of the supplement during the 30 days before the interview was collected. The individual nutrient intake of the supplements was calculated using the supplement product ingredient information, the daily intake of the participants was calculated as the sum of all sources of intake of supplements, and the estimated total nutrient intake was the sum of food and supplement intake. 13
Curhan et al (2015) 5 aimed to examine the relationship between the intake of carotenoids, vitamins A, C, E, and folate and the risk of self-reported HL in women. The study included n = 1991 women aged between 25 and 42 years. The pure-tone audiometry test and a subjective questionnaire on hearing complaints were performed.
The intake of carotenoids, vitamins A, C, E, and folate was evaluated with a food frequency questionnaire [Semiquantitative food frequency questionnaire (SFFQ)]. For each food, a commonly used unit or portion size was specified, and participants were asked how often, on average, they had consumed each type of food or beverage during the previous year. Nine possible response options ranging from “never or less than once a month” to “6 or more times a day” were provided. The use of vitamin supplements was evaluated by collecting information on the use of multiple vitamins and specific supplements, including vitamin A, β-carotene, vitamin E, vitamin C, and folic acid. 5
The study by Chang and Kim (2019) 14 used data from KNHANES. KNHANES is an ongoing national epidemiological study conducted by the Korea Centers for Disease Control and Prevention of the Ministry of Health and Welfare. All participants are randomly chosen in districts of South Korean cities and provinces (Chang and Kim, 2019). 14 In this research, the total number of participants was n = 36 067 individuals. Among these n = 36 067 participants, n = 4742 individuals aged ≥65 years were included. Among the n = 4742 participants aged ≥65 years, n = 1022 participants were excluded because they did not undergo audiometric examination, had an altered tympanic membrane, did not complete the nutritional survey, or had incomplete data. 14
Otorhinolaryngologists performed otological examinations to evaluate any abnormalities related to the tympanic membrane or middle ear, including retraction, otitis media with effusion, and cholesteatoma. The audiological evaluation was performed using a diagnostic audiometer of .5, 1, 2, 3, 4, and 6 kHz in a soundproof booth. Hearing impairment was defined as a hearing level higher than an average of 40 dB in pure-tone audiometry at .5, 1, 2, and 4 kHz. Hearing loss was divided into bilateral hearing loss, considered hearing loss, and unilateral hearing loss. 14
Nutritional intake was assessed using the 24-hour recall method. All participants were instructed to continue their normal diets before the 24-hour recall assessment. Responses were not excluded for specific days, such as holidays or weekends. Nutrient intake was calculated based on the nutrient concentrations of the foods described in the Korean Food Composition, prepared by the National Institute for Rural Resource Development of Korea. As shown in a previous report, the nutrient intake data analyzed included total energy, protein, fat, carbohydrate, crude fiber, ash, calcium, phosphorus, iron, sodium, potassium, β-carotene, retinol, thiamin, riboflavin, niacin, and vitamin C. Vitamin A intake was calculated by adding retinol and β-carotene. 14
Main Findings of the Studies
Overall, the intake of vitamins C, E, or β-carotene was not associated with the risk of HL. The association between HL and intake of vitamins C, E, and β-carotene did not vary significantly with age. For folate, there was no association in men under 60 years of age. However, in men aged 60 years or older, the high folate intake index had a 21% lower risk of developing HL. 4
No significant associations were observed between any of the antioxidants in the diet and any degree of HL. Nonetheless, when the association with moderate or greater HL was examined, older subjects with high vitamin A intake in the diet had a 47% reduction in chances of HL compared to those with lower intake levels. However, moderate HL was not significantly associated with dietary intake of other antioxidants. Significant associations were not observed between the total intake of antioxidants (diet and supplements) and the prevalence of HL. 12
Participants with a high intake of β-carotene and magnesium had significantly lower hearing thresholds, consequently better. For the intake of vitamins C and magnesium, participants with high intake significantly reduced hearing thresholds at high frequencies. Moreover, participants with a high intake of antioxidants and magnesium had better hearing thresholds than subjects with a high intake of only β-carotene, magnesium, or vitamin C. The estimated joint effects were significantly greater than the sums of the individual effects of intake. 13
Higher carotenoid intakes, specifically β-carotene and β-cryptoxanthin, were significantly associated with a lower risk of HL. No significant associations were observed between retinol or total vitamin A ingestion and the risk of HL. In addition, a higher intake of folate was associated with a lower risk of HL. 5
In the study by Kim & Chung 14 (2019), 14 the occurrence of bilateral hearing loss above 40 dB NPS was 17.88% (n = 665), on average, in the age group above 65 years. The mean age of individuals with bilateral hearing loss was 75.4 ± 5.99 years. Individuals with bilateral hearing loss were older, weighed less, and were more likely to smoke and consume alcohol than those without bilateral hearing loss. Multivariate analyses adjusted for age, sex, smoking, alcohol consumption, hypertension, and diabetes mellitus showed a significantly lower risk of bilateral hearing loss in the higher quartiles of riboflavin, niacin, and retinol intake.
The higher intake of riboflavin, niacin, and retinol was inversely correlated with the prevalence of bilateral hearing loss in the age group ≥65 years. Age-related HL was lower in the groups taking niacin and riboflavin above the recommended intake. Although Koreans have continued to adopt more Western diets, older adults still maintain traditional grain- and vegetable-oriented eating habits. Therefore, encouraging the consumption of dairy products and meat to ensure sufficient supplies of riboflavin, niacin, and retinol in older populations can help reduce the incidence of age-related HL. 14
From the data of the selected articles, the studies were analyzed in meta-analysis according to the results provided in Figure 2. Analysis of Vitamin A, E, C, β-Carotene, and Folate (A = Hazard ratios studies; B = Odds ratio studies).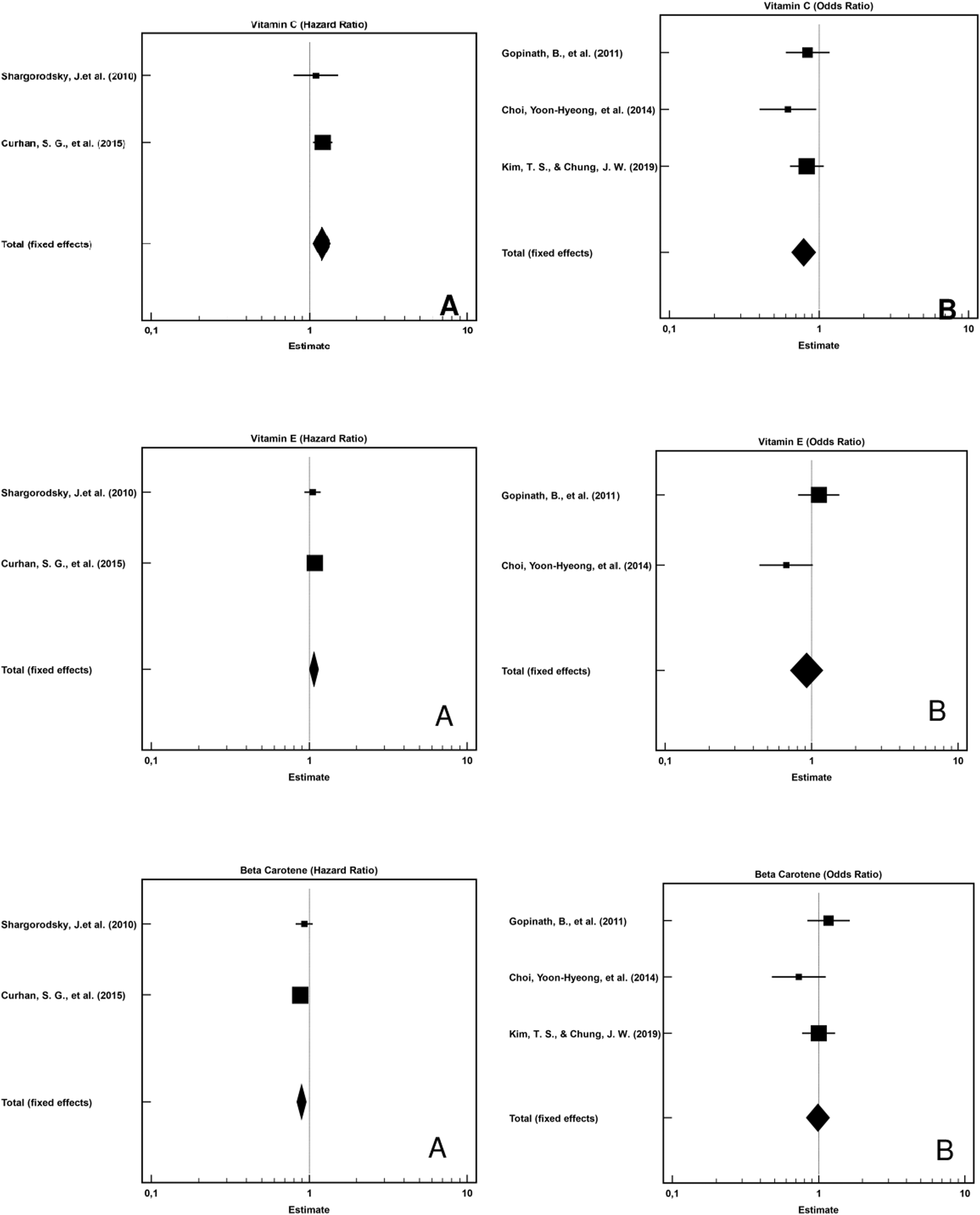
Meta-Analysis
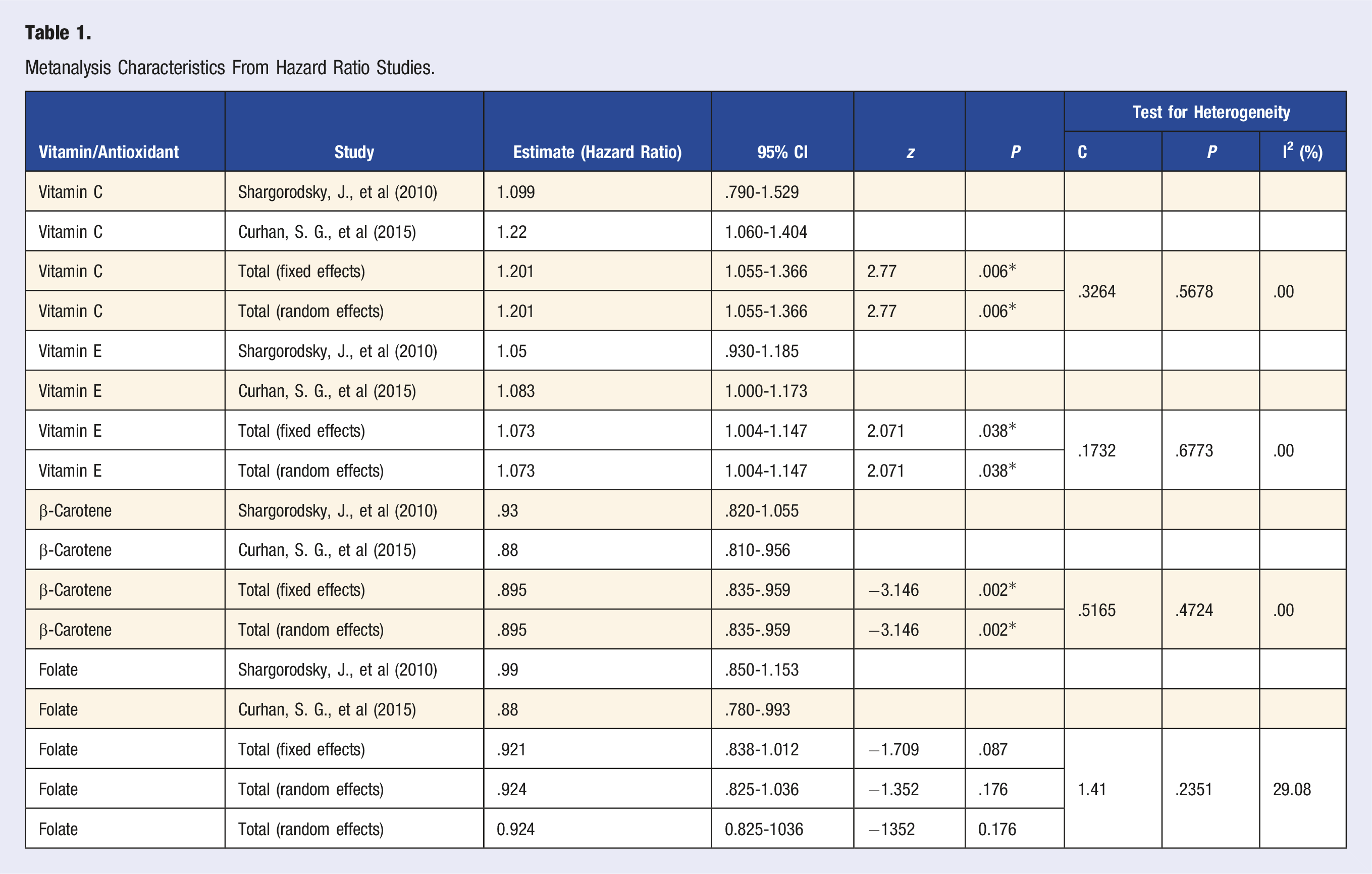
Metanalysis Characteristics From Hazard Ratio Studies.
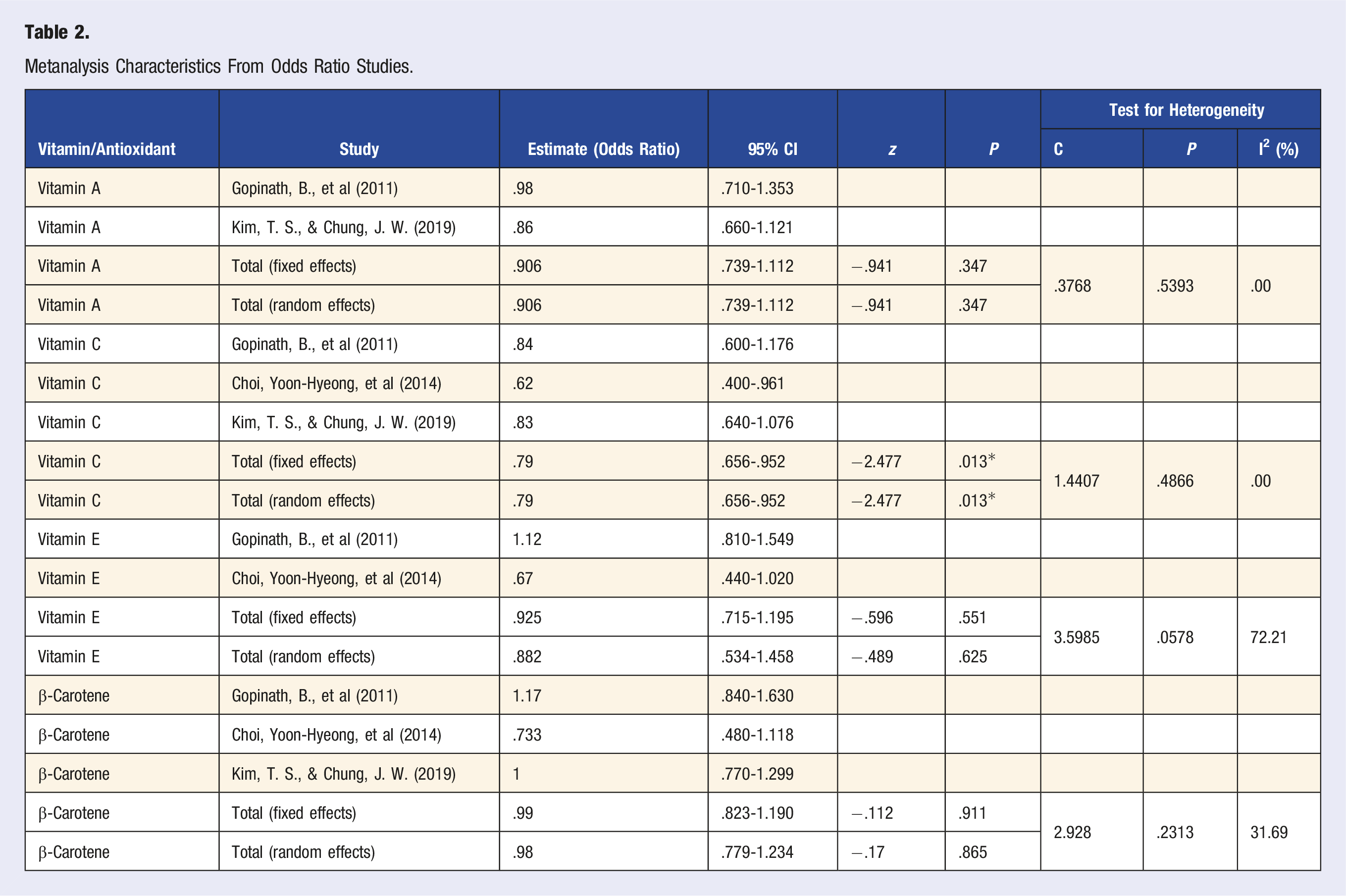
Metanalysis Characteristics From Odds Ratio Studies.
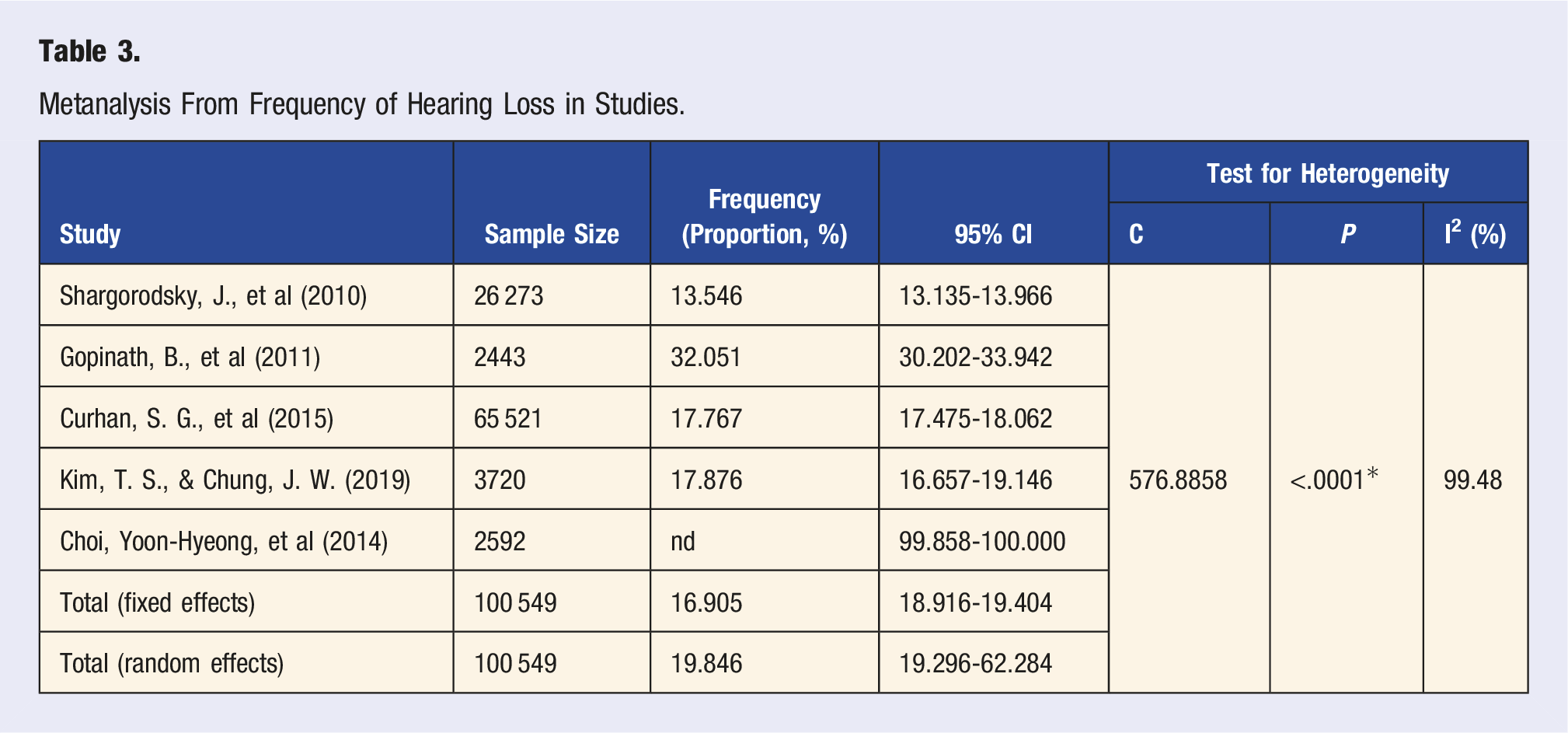
Metanalysis From Frequency of Hearing Loss in Studies.
Significance was found for the estimated summary measures of dietary intake of Vitamin C in both study groups. A summary OR of .790 reveals that the intake of Vitamin C in concentrations in the range of 200 mg/day (data from the articles) approximately reduced the chances of HL by 19%. However, for this same vitamin with the studies that followed the patients prospectively and the relative risk (HR) was evaluated through the Cox regression model, the calculated summary HR was 1,201, showing a worsening of HL. In these studies, these groups ingested concentrations higher than 1000 mg/day of vitamin C in their diets, and the groups with the lowest quartile/quintile ingested concentrations lower than 200 mg/day.
It was also observed that the HR summaries calculated for the group with the highest consumption of vitamin E had a relative risk of about 7% (HR 1.07) higher than the group with the lowest consumption (HR 1.000). In the case of studies evaluating Vitamin E using a logistic regression model for evaluation, although the summary OR had a value less than 1.000, the 95% CI observed for this measure showed great dispersion, including values greater than 1.000 (95% CI of OR = .534-1.458).
Vitamin A and folate had no apparent protective effect (both the summary measures calculated for the studies evaluated by Cox regression and those using logistic regression).
Table 3 shows the relative frequencies (proportions) of HL found in the different studies, as well as the total number of individuals evaluated in each study. The calculated summary measure of these relative frequencies (summary proportion) is also presented. It was impossible to calculate this frequency for the study by Cho et al (2014). 13
The risk or otherwise of HL is associated with the binary variable. The index indicates a lower value when protected, meaning less HL.
Discussion
Nutritional status or nutritional factors are known to cause aging-related problems, and the literature has suggested interaction effects between nutrition and HL (Kim & Chung, 2019). In the present study, subjects with a high intake of β-carotene and magnesium had better hearing thresholds, as well as better speech recognition. For the intake of vitamins C and magnesium, participants with high intake significantly reduced hearing thresholds at high frequencies. The estimated joint effects were significantly greater than the sums of the individual effects. 13
The literature indicates the relationship between retinol and hearing since retinol has a high concentration in the inner ear and retinoic acid, an active metabolite of retinol, contributes to the development of the organ of Corti. On the other hand, higher consumption of riboflavin was significantly associated with better hearing thresholds. Retinol and riboflavin are found mainly in animal foods such as milk, cheese, and eggs. 14 Regarding vitamin C, studies did not find an association between higher vitamin intake and lower risk of HL.4,12
The cochlea contains a vascular system that maintains cellular metabolism and the endochlear potential as a driving force for sensory transduction if unrestricted antigens, toxins, metabolites, and circulating immune cells from the periphery can infiltrate the cochlear blood supply. 4
Antioxidants are believed to counteract the deleterious effects of reactive oxygen species and may be effective in treating oxidative stress-related diseases, including HL. 15 The data obtained in the present study demonstrate a significant increase in the number of patients at risk of HL referred for evaluation compared to the baseline rates of the respective studies. Both studies reported that patients with HHI scores ≥10 had a higher referral rate than those who scored <10 points.
Servidoni and Conterno (2017) 16 corroborate that the questionnaire is suitable for hearing screening due to its high accuracy and ease of use. According to the study by these authors, in participants ≥60 years, the accuracy of the questionnaire was 86.2%, sensitivity 89.1%, and specificity 75.0%. According to the research by Rosis et al (2009), the sensitivity of the HHI questionnaire when applied in the Audiology Outpatient Clinic was 23.5%, while the sensitivity was 94.7% when applied in the Geriatrics Outpatient Clinic, demonstrating the effectiveness of the questionnaire only when applied in primary care.
The studies above corroborate the effective methodology of the postulated instrument for identifying sensory loss since, in the study by Servidoni and Conterno (2017), 16 76.1% reported the perception of some level of deficiency in the use of the questionnaire. When comparing with the results of the use of audiometry, whose number was 79.7%, numerical proximity is perceived, which indicates a good tool compared to strategies for identification and referrals.
Rosis et al (2009) 17 corroborate that the instrument evaluated for hearing screening in the other studies mentioned has high specificity and sensitivity in identifying HL when health services are often not specific for hearing changes. Nevertheless, comparing the use of the questionnaire for audiological clinics and their referrals, it does not prove to be an efficient instrument due to its low sensitivity. In this perspective, primary care is responsible for collective actions aimed at promoting hearing health, prevention, and early identification of HL, in addition to conducting informative and educational processes, 18 and the opportunity for most situations to be resolved before reaching the other levels of care; medium and high complexity. Health education is the process in which the population participates in the context of their daily life and not only at risk of becoming ill. It is characterized as a transformative social practice. 19
The quality of intake of the supplements investigated is strongly related to the quality of life of individuals, as already described in the literature. Still, this association is not yet fully explained. The studies included in this analysis showed a relationship between better hearing thresholds and intake of antioxidants and vitamins, especially in elderly individuals, also highlighting the importance of guidance and dissemination of information for them.
It should be considered that in this research the heterogeneity based on some studies was evaluated, and the Cochran test and the I2 statistic should be used with caution when the number of studies is less than 20, this factor should always be considered as an important limitation of the study, considering that in this research there were 5 studies admitted for analysis. 20
In epidemiological studies, participants’ pathology is often collected through self-reported results rather than formal medical examinations, most often due to budgetary constraints. However, authors mention that self-reported results are often subject to measurement errors and can lead to biased estimates if used in statistical analyses. In the study by Wu and Wang, 2023, 21 the authors carried out statistical methods to correct measurement errors resulting in analyzes with multiple types of failures through a reweighting strategy. In another study, 22 the authors report that in epidemiological hearing research, estimating the association between exposures and HL using audiometrically assessed hearing measures is challenging due to the complex correlation structure in the pooled data and by location of test and by the speech therapist who performs the exam. The study proposes a linear mixed-effects model to take into account the multilevel correlation structures of the data. From this, it is highlighted that new research is important to verify, in different types of studies and collection methods, the estimated correlation between responses and how the information was obtained.
Conclusion
Considering that the prevalence of HL is associated with the aging process, aspects related to nutrition may also play a significant role in the acceleration of HL. Dietary patterns characterized by a higher intake of nutrients such as vitamins and antioxidants may represent protective factors for the central auditory system. Therefore, in addition to the cardiometabolic benefits associated with healthy eating, HL can also be attenuated by consuming certain foods. Future research is necessary on the topic given the wide range of information and results that can be correlated based on the responses of the subjects included in the studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.