
Abstract
Background: Age-related hearing loss, also known as hearing loss, is an important and increasingly prevalent public health problem worldwide, as it induces disability and social isolation. Objective: To verify the association between eating habits and hearing loss in the older population. Methods: A cross-sectional study with data analysis of older patients treated in an Outpatient Hearing Health Service accredited to the Unified Health System. Older people aged 60 years and over who attended the Health Service to begin adaptation in the study. The audiological evaluation was performed through Tonal and Vocal Audiometry exams, the auditory rehabilitation process was done using the Individual Sound Amplification Device, and eating habits based on the Dietary Guide for the Brazilian Population. Results: The sample included (n = 654) participants, aged between 60 and 97 years. The type of hearing loss revealed a higher prevalence of sensorineural of moderate degree. Individuals with higher consumption of tea, non-fatty meats, rice, fish, and fruits presented better hearing compared to participants with lower consumption of these types of foods. Conclusion: A higher consumption of foods high in anti-inflammatories and antioxidants may decrease the risk of age-related hearing loss. A higher consumption of foods high in anti-inflammatories and antioxidants may decrease 50% of the risk of age-related hearing loss. The findings also indicate the hypothesis that a pro-inflammatory diet could increase the risk of hearing loss. Antioxidants are believed to counteract the deleterious effects of reactive oxygen species and may be effective in treating diseases related to oxidative stress, including hearing loss.
“Oxidative stress and free radical damage can lead to impaired auditory signal transduction, cell death and hearing loss.”
Introduction
Hearing is essential for quality of life (QOL), cognitive and socio-emotional development, and overall health at all stages of life. In adults, hearing loss (HL) is associated with cognitive decline1,2 and represents a significant risk factor for the development of dementia 3 Population aging is a global reality. 4 Thus, aging-related changes arise, such as the increase in the prevalence of hearing loss.
Hearing loss is conceptually defined by age-related sensorineural hearing as a bilateral and irreversible condition, affecting the sensory and/or a neural portion, manifested by an impairment in the ability to detect high-frequency sounds, affecting speech discrimination, recognition, and understanding. 5 Sensory hearing loss results from the gradual degeneration of sensory cells, ciliated cells of the Corti Organ, stria vascularis, and neurons of the spiral ganglion, accelerated by advancing age, mitochondrial DNA mutations, oxidative damage, exposure to noise, ototoxic drug use, and poor diet. 6
The inner ear, composed of peripheral auditory and vestibular organs, resembles the brain in some aspects, making it comparatively susceptible to influences from gut microbiota. 7 The cochlea contains a vascular system that maintains cellular metabolism and the endochlear potential as a driving force for sensory transduction if unrestricted antigens, toxins, metabolites, and circulating immune cells from the periphery can infiltrate the cochlear blood supply.7,8
Aging and age-related chronic diseases have been associated with the upregulation of pro-inflammatory mediators. 9 One study 10 with 734 older individuals investigated the relationship between hearing loss and foods/beverages classified as anti-inflammatory (fruits, vegetables, nuts, wine) or pro-inflammatory (processed meats, high-sugar juices, desserts, distilled beverages), observing that hearing loss was transversely associated with increased consumption of fruit juices and retrospectively associated with increased consumption of sugary foods, high-calorie drinks, beer, and distilled beverages. Thus, identifying risk factors, especially modifiable ones, can assist in planning and developing preventive strategies to reduce the progression and severity of age-related hearing loss. 11
Diet can influence hearing health. Certain micronutrients, including specific vitamins, carotenoids and long-chain polyunsaturated fatty acids, have been linked to the risk of hearing loss. A healthier overall diet could protect against hearing loss by several mechanisms, including preventing microvascular and macrovascular impairment of cochlear blood flow, reducing oxidative damage, and reducing inflammation. Decline in auditory function can result from cumulative contributions from genetics and environmental exposures, including noise and toxins. 12
In this context, this study aimed to verify the association between hearing loss in the older population related to eating habits.
Material and Methods
Database
A cross-sectional study with data analysis of older patients treated in an Outpatient Hearing Health Service (SASA, in Portuguese) accredited to the Unified Health System from May 2021 to July 2022. The vulnerability indicators of older people and the classification of the type and degree of hearing loss proposed by the World Health Organization 13 were analyzed to assess the quality of the protocols. This study was approved by the Research Ethics Committee (CEP in Portuguese): CAAE: 39562720.8.0000.012. A survey of sociodemographic information (gender, age, education, income) was conducted, and auditory symptoms were considered for data collection. The dietary habits of these individuals were evaluated through the Qualitative Assessment Protocol of the Diet of Older Individuals based on the Dietary Guide for the Brazilian Population.
Inclusion and Exclusion Criteria
The inclusion criteria were older individuals aged 60 years or older who attended the Outpatient Hearing Health Service for evaluation and performance of the Tonal and Vocal Audiometry exam and began the hearing rehabilitation process using the Individual Sound Amplification Device (ISAD). The participants were informed about the research and invited to participate. Those who agree must sign the ICF. Service users under the age of 60 who arrived at the institute using hearing aids or who did not have physical and/or cognitive conditions to participate in the study were excluded.
Data Analysis
The data were organized in Microsoft® Excel® to Microsoft 365 spreadsheets and subsequently exported and analyzed in the MedCalc® Statistical Software version 22.013 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org.2023). The data were presented in absolute and relative frequencies, with their respective 95% confidence intervals, to describe the categorical variables of the study population. Analysis was conducted between auditory alterations and eating habits in the older population, adopting the significance level of .05 (P < .05). The chi-square test was used to analyze the frequencies observed in the different categories of sociodemographic characteristics and audiological assessment (degree, type, or elderly person’s perception of hearing loss). Bivariate association analyzes were conducted by calculating crude odds ratios (OR) from 2X2 contingency tables and by obtaining adjusted odds ratios (aOR) through logistic regression. The outcome assessed was hearing loss perceived by the elderly person as excellent/very good/good/regular or bad/very bad, both in the calculations of crude ORs and in the logistic regression model for adjusted ORs. The independent variables tested were eating habits (consumption yes or no) listed in Table 3. In the logistic regression the variables sex (male or female) and age (in years of life) were also included in the analysis.
Results
Participant Sociodemographic Data.
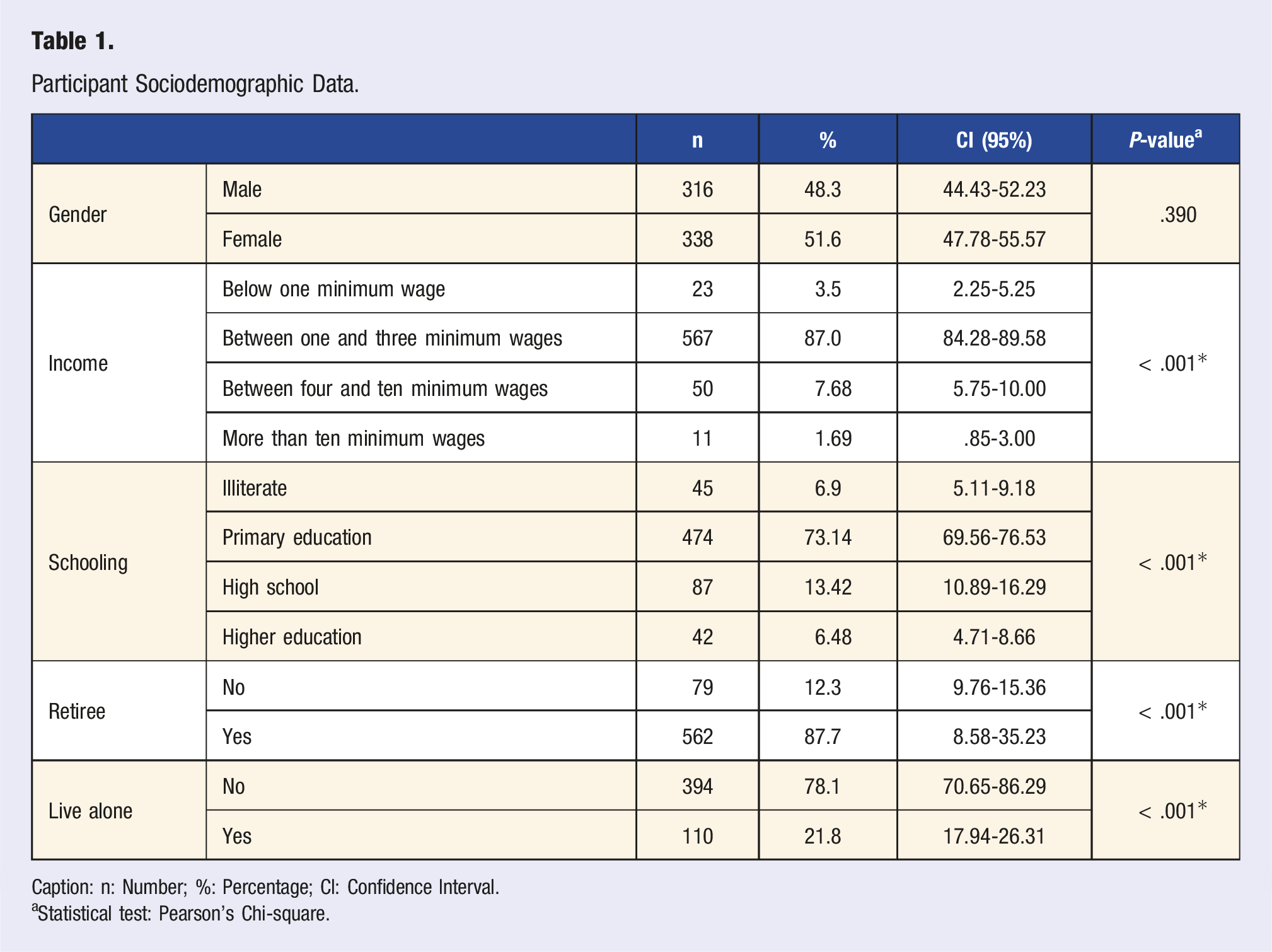
Caption: n: Number; %: Percentage; CI: Confidence Interval.
aStatistical test: Pearson's Chi-square.
Classification as to the Type and Degree of Hearing Loss.
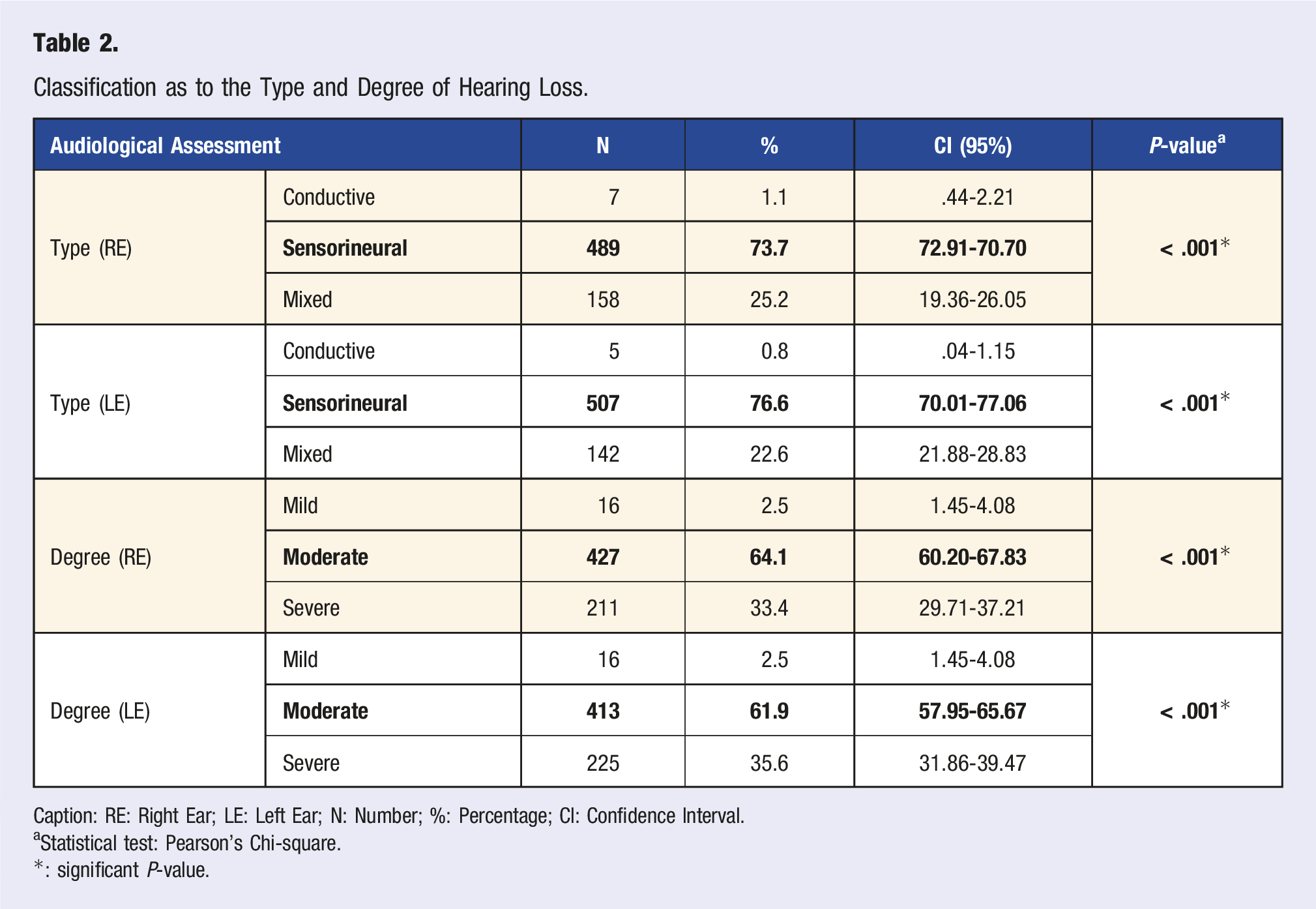
Caption: RE: Right Ear; LE: Left Ear; N: Number; %: Percentage; CI: Confidence Interval.
Statistical test: Pearson's Chi-square.
*: significant P-value.
Association of Food Consumption Habits Associated With Hearing Loss. In This Table, Commas (Portuguese) Were Replaced by Points (English) to Indicate the Decimal Part of the Numerals.
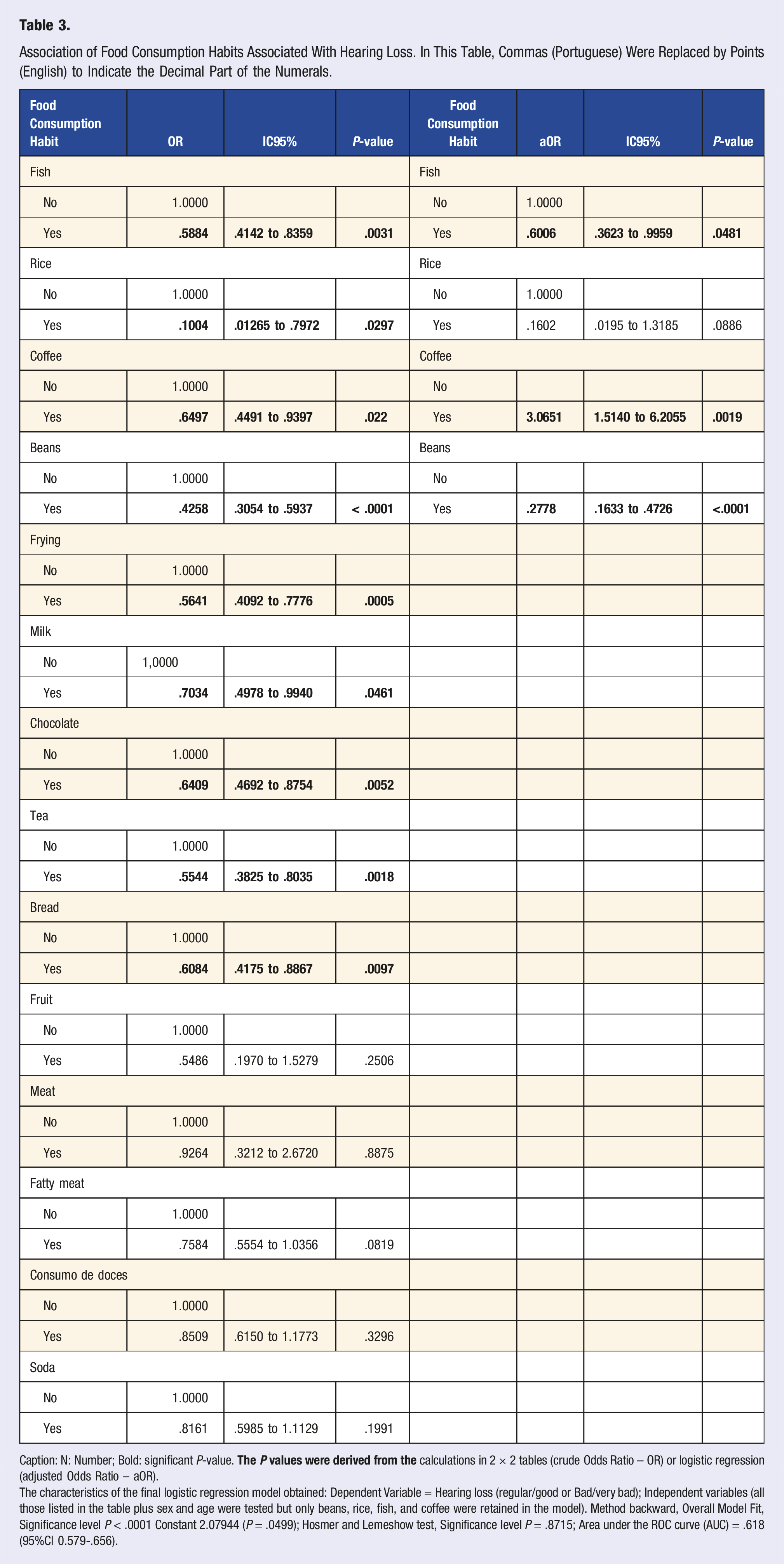
Caption: N: Number; Bold: significant P-value.
The characteristics of the final logistic regression model obtained: Dependent Variable = Hearing loss (regular/good or Bad/very bad); Independent variables (all those listed in the table plus sex and age were tested but only beans, rice, fish, and coffee were retained in the model). Method backward, Overall Model Fit, Significance level P < .0001 Constant 2.07944 (P = .0499); Hosmer and Lemeshow test, Significance level P = .8715; Area under the ROC curve (AUC) = .618 (95%CI 0.579-.656).
Discussion
The present study verified that older people who presented eating habits with higher consumption of foods considered healthy had lower hearing thresholds than those with lower consumption of this type of food.
The associations between inflammatory markers and hearing impairment appear to be age-related. Increased inflammation is associated with many age-related diseases, including cardiovascular disease, dementia, and Alzheimer’s disease, since higher levels of systemic inflammation are associated with older age, and hearing impairment often occurs with other health conditions, such as diabetes and hypertension.14-16 Few studies have focused on possible associations between systemic inflammation and age-related hearing impairment.
The increase in inflammation with age may be due to the higher prevalence of cardiovascular disease or other morbidities in older adults or to other age-associated processes, including oxidative stress. Inflammation is associated with pathophysiological processes of aging, including vascular damage and neurodegeneration. The cochlea and the central auditory pathway tissues depend on an adequate blood supply. Therefore, vascular damage can have deleterious effects on their function.17-19 The study by Trune et al 20 demonstrated that circulating inflammatory molecules can negatively affect the tissues of the cochlear vasculature, both proximally in the spiral artery and distally between the capillaries of the stria vasculature.
The present study also demonstrated this, in which the consumption of fish, beans and rice showed a significant association with reducing hearing loss by 50%. In addition to nutrients, minerals, and phytochemicals, non-nutritive bioactive compounds commonly found in plants also exhibit antioxidant activities. Thus, these compounds may have contributed to the observed inverse association between the risk of hearing loss and a diet rich in vegetables. 21 All dietary indices examined in current and previous studies emphasize the higher consumption of vegetables, fruits, whole grains, nuts, and legumes, which are great sources of antioxidant compounds.22-24 In addition, high-quality diets protect against vascular impairment and reduce cochlear blood flow by promoting beneficial blood lipid profiles, better endothelial function, lower blood pressure, and less inflammation. Healthy diets can also reduce neuroinflammation and neurodegeneration of auditory nerve fibers and central auditory pathways. 25
There are several mechanisms by which a healthier diet can protect against hearing loss. Evidence from animal models suggests that dietary factors may influence susceptibility to sensorineural hearing loss, whether due to hearing damage from inadequate cochlear blood supply, hypoxia and ischemic damage, inflammation, increased oxidative stress, mitochondrial dysfunction or auditory neurodegeneration. Healthier diets could protect against vascular compromise and reduced cochlear blood flow by promoting beneficial blood lipid profiles, improving endothelial function, lowering blood pressure and reducing inflammation. Oxidative stress and free radical damage can lead to impaired auditory signal transduction, cell death and hearing loss. Healthier eating patterns have been associated with a lower risk of neurodegenerative diseases and could protect against auditory neuroinflammation and neurodegeneration. 12
Diets high in fat and cholesterol have deleterious effects on hearing that could be avoided with less consumption. On the other hand, increased consumption of fruits and vegetables, polyunsaturated fatty acids (omega-3), and antioxidants in the form of vitamins can prevent the development of age-related hearing loss. The protective effect of overall diet quality on auditory functions among older adults observed in the present study, including those at high auditory frequencies, is consistent with most previous investigations. 26
Conclusion
The study’s results suggest that a higher consumption of foods high in anti-inflammatories and antioxidants may decrease the risk of age-related hearing loss and hypothesize that a pro-inflammatory diet could increase the risk of age-related hearing loss. The benefits of adherence to healthy eating patterns have been demonstrated for numerous positive health outcomes since a healthy dietary pattern has been significantly and inversely associated with hearing loss. Implementing appropriate strategies focusing on modifiable risk factors can reduce the overall burden of disease. Low-grade systemic inflammation associated with a high-fat diet is one of these modifiable risk factors for hearing loss.
Nutritional status or nutritional factors are known to cause aging-related problems, and the literature has suggested that there are interaction effects between nutrition and hearing loss. Antioxidants are believed to counteract the deleterious effects of reactive oxygen species and may be effective in treating diseases related to oxidative stress, including hearing loss.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.