
Abstract
Background. Cardiovascular disease is a major cause of deaths. Elevated cholesterol levels to above the normal reference range is a major risk factor for developing cardiovascular disease. Current guidelines recommend the use of cholesterol-lowering drugs to lower cholesterol levels to within the normal reference range. However, the American Heart Association further recommends a change in lifestyle in managing cholesterol levels. Thus, cholesterol-lowering drugs may not be needed if a lifestyle-change alone is sufficient in lowering cholesterol levels to within normal ranges. Unfortunately, limited examples exist in academic literature to illustrate the effectiveness of lifestyle change alone in lowering of cholesterol levels. Case report. We report a case of a 33-year-old man, with moderately elevated cholesterol levels and a family history of cardiovascular disease. Method. The man followed an altered healthy fat diet accompanied with moderate exercise for 6 weeks, without the addition of cholesterol-lowering agents. Results. At the 6-week follow-up, he was able to decrease his total cholesterol by 40.25% and low-density lipid cholesterol by 52.8%, to within normal ranges. The cholesterol levels remained within normal ranges after 6 months. Conclusion. This case illustrates that in some individuals, lifestyle change alone is sufficient to lower moderately elevated cholesterol levels.
‘Statins may also result in a range of adverse effects, including muscle pain, diabetes mellitus, and central nervous system complaints, which might lead to noncompliant use by patients.’
Introduction
Diseases of the circulatory system are some of the leading causes of morbidity and mortality in South Africa, accounting for 17.8% of all deaths in South Africa in 2015. This is the second most common underlying cause of death, surpassed only by certain infectious and parasitic diseases. It is a worrying statistic because a slight increase of 1.1% has been seen in these deaths between 2013 and 2015. Diseases of the circulatory system include thrombosis-related disorders, such as stroke and heart attack. Cardiovascular diseases collectively accounted for 7.5% of deaths in South Africa in 2015. Thus, cardiovascular diseases remain a major cause of concern in South Africa. 1 The World Heart Federation lists high cholesterol (hyperlipidemia), and especially elevated low-density lipid (LDL) cholesterol levels, as a major risk factor for developing cardiovascular disease. LDL cholesterol (“bad” cholesterol) accumulates in arteries, increasing the risk of heart attack and stroke. However, high-density lipid (HDL) cholesterol (“good” cholesterol) serves as a carrier, that helps remove cholesterol from the blood stream. 2 HMG-CoA (3-hydroxy-3-methylglutaryl-CoA) reductase inhibitors, called statins, are the most commonly used cholesterol-lowering drugs. The Blood Cholesterol Expert Panel from the American College of Cardiology and the American Heart Association (AHA) recommends that patients older than 21 years of age, with a LDL cholesterol level of more than 4.92 mmol/L be placed on high-intensity statin therapy (atorvastatin 40-80 mg or rosuvastatin 20 mg) to lower the LDL cholesterol levels by at least 50%. 3 However, some controversy and debate has arisen subsequently to the publication of these recommendations, casting some doubt over the correct use of statins in treatment of elevated cholesterol. 4 Nonetheless, it was found that these guidelines had little to no effect on the use of statins or LDL cholesterol levels in the clinical setting, with only a small increase (4%) in the statin intensity observed in patients treated for hypercholesterolemia. 5 Statins may also result in a range of adverse effects, including muscle pain, diabetes mellitus, and central nervous system complaints, which might lead to noncompliant use by patients. 6 Conversely, the AHA also recommends 4 lifestyle changes to help improve hyperlipidemia: (1) eating a heart-healthy diet, (2) regular exercise, (3) avoiding tobacco smoke, and (4) losing weight (if you are overweight or obese). 7 Therefore, theoretically, a lifestyle change alone may be sufficient to lower elevated LDL cholesterol levels, without the use of cholesterol-lowering drugs, such as statins.
Case Report
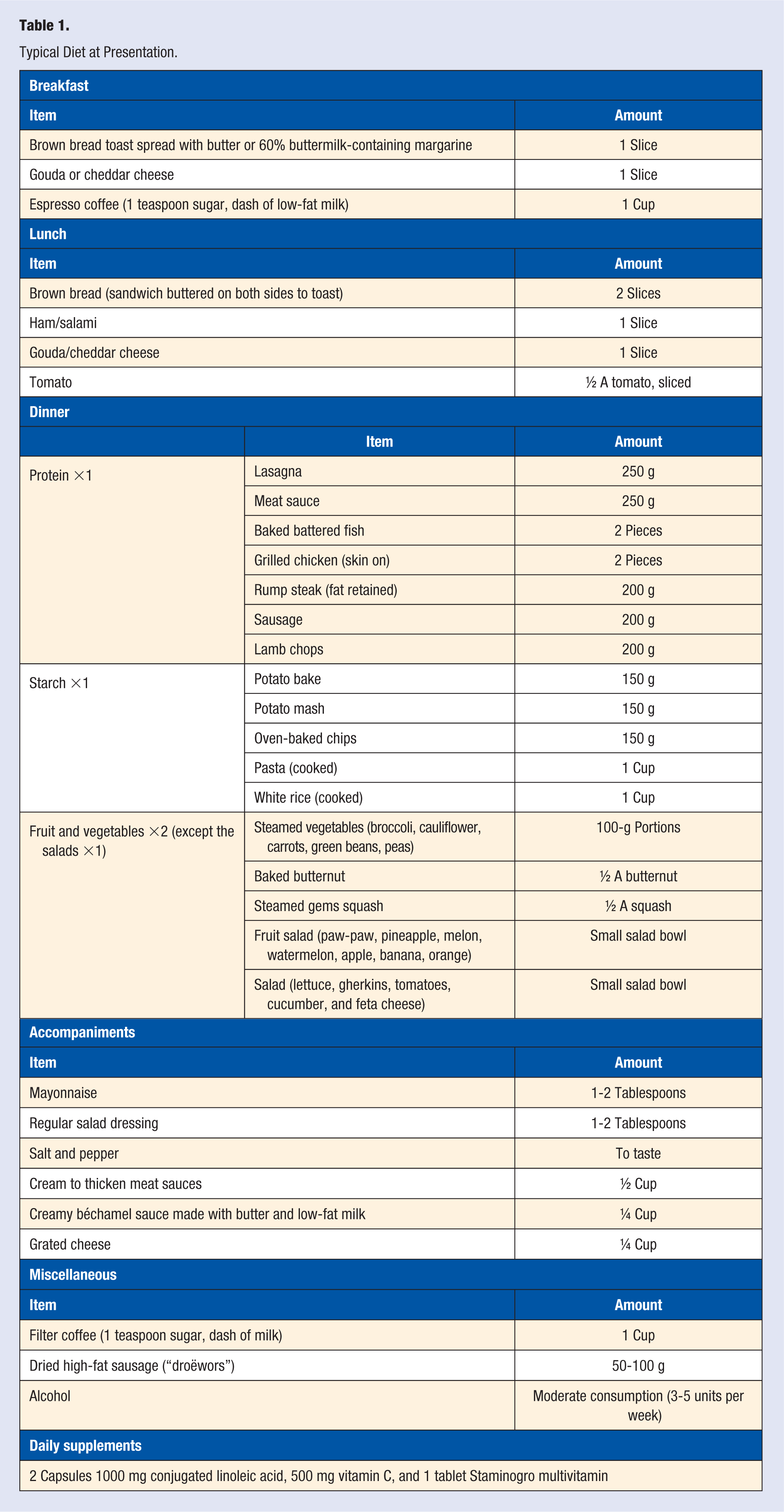
A 33-year-old nonsmoking Caucasian man presented at his employer’s yearly wellness screening with a point-of-care nonfasting total cholesterol level of 8.5 mmol/L and was subsequently referred to his general practitioner (GP) for follow-up. The man has a family history of hypercholesterolemia and heart disease, with both his living parents on long-term cholesterol-lowering medications and a paternal grandfather who died of a myocardial infarction at 54 years. He has an office job, with a large amount of time spent sitting, with moderate physical activity after hours. The typical diet at presentation is given in Table 1. The case report was approved by the Health Sciences Research Ethics Committee of the University of the Free State (HSREC 133/2017, UFS-HSD2017/1265). The patient gave informed consent for the results to be published.
Typical Diet at Presentation.
Anthropometric Values at Presentation
At presentation, the patient weighed 84.4 kg and, taken together with his height of 178 cm, had an overweight body mass index (BMI) of 26.64 kg/m2.
Fasting Lipogram at Presentation
The laboratory fasting lipogram results were as follows (normal reference ranges in brackets):
Total cholesterol 7.7 mmol/L (2.8-4.9 mmol/l)
Triglycerides 2.29 mmol/L (0.5-1.6 mmol/L)
HDL cholesterol 1.7 mmol/L (1.0-1.6 mmol/L)
LDL cholesterol 5.3 mmol/L (1.6-2.9 mmol/L)
Non-HDL cholesterol 6.0 mmol/L (0.8-3.7 mmol/L).
Medical Intervention
In consultation with the GP, it was decided to allow the patient to alter his lifestyle via diet and exercise and to perform a follow-up lipogram after 6 weeks, without prescribing any cholesterol lower drugs.
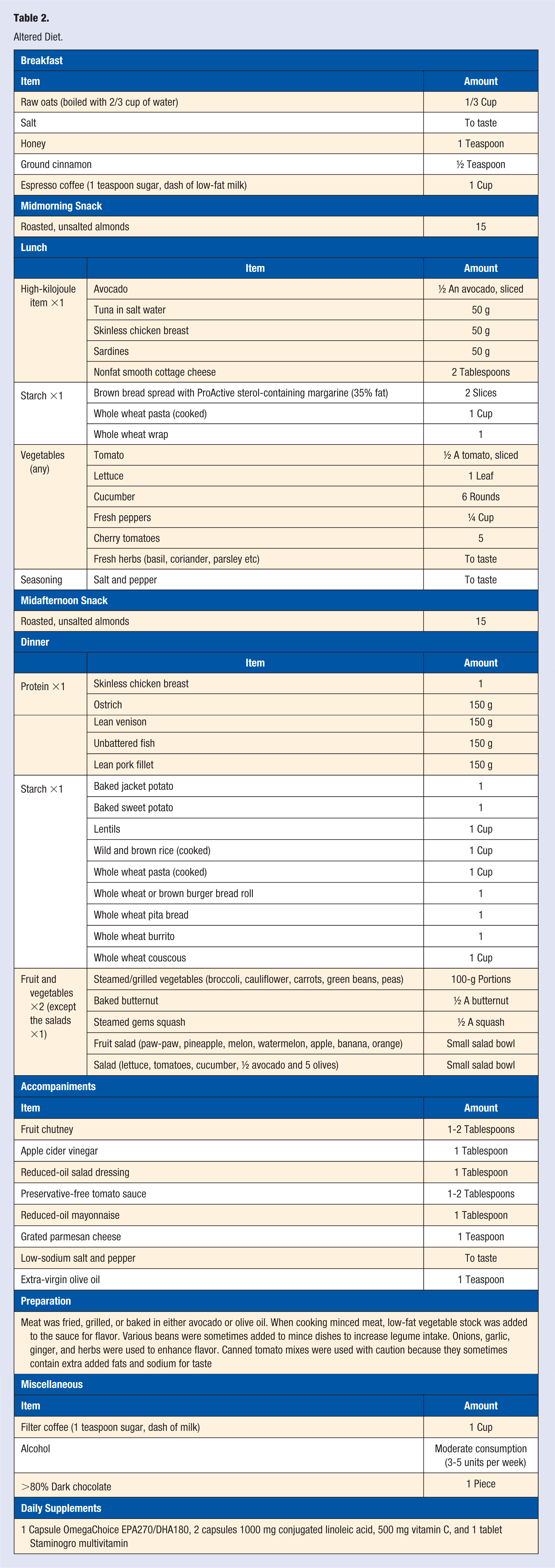
Altered Diet (Table 2)
The patient added clinically proven cholesterol-lowering foods to his daily diet, such as 1/3 cups raw oats, which is equivalent to roughly 1.3 g of oat β-glucan,8,9 30 g of almonds, 10 at least half an avocado, 11 and extra virgin olive oil. 12 An omega 3 supplement was also added to the daily diet. 13 The patient used conjugated linoleic acid (CLA), vitamin C, and a multivitamin as daily supplements prior to the altered diet. The effect of CLA on the blood lipid profile remains highly debated and largely inconclusive. 14 However, because the patient already used a daily CLA supplement, it was decided to continue with 2000 mg CLA in order to limit the amount of variables taken away during the altered diet. Because 500 mg vitamin C per day has a proven positive impact on fat oxidation during moderate exercise, 15 it remained as part of the altered lifestyle. The multivitamin (Staminogro) was previously recommended to the patient by his GP and is a combination of amino acids, antioxidants, B-complex vitamins, calcium, and other vitamins and minerals. An addition of a good multivitamin assists in maintaining a person’s nutrient status at optimal levels, and it was therefore continued.
Altered Diet.
Exercise
The patient exercised a minimum of 30 minutes, twice per week. The exercise included 10-minute cardio exercise (10 minutes treadmill at level 9/10-minute exercise stationary bicycle at resistance level 5/2-kilometre jog), and 20-minute high-intensity free weight routine (with minimal rest between sets).
Anthropometric Values at the 6-Week Follow-up
At follow-up, the patient weighed 77.3 kg, which gives a normal BMI of 24.40 kg/m2.
Fasting Lipogram at 6-Week Follow-up
The follow-up laboratory fasting lipogram results were as follows (baseline results in brackets):
Total cholesterol 4.6 mmol/L (7.7 mmol/l)
Triglycerides 0.9 mmol/L (2.29 mmol/L)
HDL cholesterol 1.9 mmol/L (1.7 mmol/L)
LDL cholesterol 2.5 mmol/L (5.3 mmol/L)
Non-HDL cholesterol 2.7 mmol/L (6.0 mmol/L)
Anthropometric Values at the 6-Month Follow-up
At follow-up, the patient weighed 68.2 kg, which gives a normal BMI of 21.50 kg/m2.
Fasting Lipogram at 6-Month Follow-up
The follow-up laboratory fasting lipogram results were as follows (baseline results in brackets):
Total cholesterol 4.6 mmol/L (7.7 mmol/l)
Triglycerides 0.9 mmol/L (2.29 mmol/L)
HDL cholesterol 1.7 mmol/L (1.7 mmol/L)
LDL cholesterol 2.8 mmol/L (5.3 mmol/L)
Non-HDL cholesterol 2.9 mmol/L (6.0 mmol/L)
Conclusion
The patient in this report was able to reduce his total cholesterol by 40.25% and his LDL cholesterol by 52.8% over the course of 6 weeks, without the use of cholesterol-lowering drugs. The altered diet reduced the amount of dairy and high animal fat foods, contained more lean meat, and increased the intake of food clinically proven to decrease LDL cholesterol (such as oats, almonds, avocados, and olive oil). After 6 months, the cholesterol levels remained constant within the normal range, and the patient stabilized his weight at a BMI of 21.50 kg/m2. It has been reported that weight loss in combination with a cholesterol-lowering diet is more effective in lowering LDL cholesterol levels than weight loss alone; therefore, the substantial decrease in LDL cholesterol in this case cannot be exclusively attributed to either the weight loss or diet but rather the combination of factors. 16 Thus, it can be concluded that in some individuals with moderately high cholesterol levels, lifestyle changes (such as an altered, healthy fat diet and moderate exercise, together with weight loss) have the potential to lower cholesterol to within normal ranges without the addition of cholesterol-lowering drugs, such as statins.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was granted by the Health Sciences Research Ethics Committee of the University of the Free State, HSREC 133/2017, UFS-HSD2017/1265.
Informed Consent
The patient gave consent for the results to be published.
Trial Registration
Not applicable, because this article does not contain any clinical trials.