
Abstract
Objective:
To determine the prevalence of occult hearing loss in elderly inpatients, to evaluate feasibility of opportunistic hearing screening and to determine subsequent provision of hearing aids.
Materials and methods:
Subjects (>65 years) were recruited from five elderly care wards. Hearing loss was detected by a ward-based hearing screen comprising patient-reported assessment of hearing disability and a whisper test. Subjects failing the whisper test or reporting hearing difficulties were offered formal audiological assessment.
Results:
Screening was performed on 51 patients aged between 70 and 95 years. Of the patients, 21 (41%) reported hearing loss and 16 (31%) failed the whisper test. A total of 37 patients (73%) were referred for audiological assessment with 17 (33%) found to have aidable hearing loss and 11 were fitted with hearing aids (22%).
Discussion:
This study highlights the high prevalence of occult hearing loss in elderly inpatients. Easy two-step screening can accurately identify patients with undiagnosed deafness resulting in significant proportions receiving hearing aids.
Key sentences
Approximately 14% of the elderly population use hearing aids despite a reported prevalence of deafness in up to 55%.
The use of hearing aids is associated with an improvement in physical, emotional, mental and social well-being.
An easy screening test for hearing loss consists of patient-reported hearing loss and a whisper test.
Opportunistic screening of elderly inpatients resulted in referral of 73% of screened patients for formal audiology.
Of the screened patients, 22% were provided with hearing aids.
Introduction
The prevalence of hearing loss among elderly people has been reported to be up to 55%. Despite this fact, only 14% use hearing aids. 1 Hearing loss among elderly people has been shown to exacerbate symptoms of dementia and depression, increase the risk of delirium and has a significant impact on quality of life. 2 In addition, individuals who fail to report their hearing loss and do not have hearing aids report sadness, depression, social isolation and insecurity compared with individuals of similar age using hearing aids.3–6 Consequently, the use of hearing aids is associated with an improvement in physical, emotional, mental and social well-being. 2
Elderly patients may have complex medical, social and care needs, and as a result, the presence of occult hearing loss may be overlooked. The problem is compounded by patients who may not report hearing loss due to cognitive impairment, poor recognition or by associating deafness with the natural consequences of ageing. The significant impact of hearing loss and the relative ease of providing hearing aids for affected patients raises the question of whether opportunistic hearing screening would be beneficial.
The gold standard in detecting hearing loss is pure tone audiometry. However, performing pure tone audiometry can be time-consuming and reliant on an appropriate environment and is therefore not appropriate as a screening tool. Several other forms of hearing assessment provide a quick and easy means of testing hearing, although they are not as sensitive as audiometry. An effective screening tool must be easy, quick to perform and reproducible.
Bagai et al. 7 proposed a model for elderly patients using a combination of a screening question and a whisper test to detect hearing loss. It has been shown to be an effective means of hearing assessment.
The aims of this study are threefold: to determine the incidence of occult hearing loss in a convenience sample of hospitalised elderly patients with and without cognitive impairment identified by an opportunistic screening test, to evaluate the correlation between the screening and subsequent formal audiological testing and to determine the dissemination of hearing aids.
Materials and methods
Ethical approval for this study was obtained from the National Research Ethics Service Committee, South Central, Berkshire, England.
Participants
Subjects over the age of 65 years were recruited from five general elderly care wards at the Royal Berkshire NHS Foundation Trust, Reading, England, between July and September 2011. Individuals were selected on the day of screening and gave verbal consent to participate in the study. All subjects had a Mini-Mental State Examination (MMSE) score 8 of greater than 20. Subjects with acute medical problems, active ear disease, MMSE < 20 and those who already had hearing aids were excluded from the study.
Screening
Screening for hearing loss was conducted by K.R. in all cases using a modified version of the method proposed by Bagai et al. 7 Subjects who met the inclusion criteria were asked whether they suffered from hearing loss. Otoscopy was performed initially, and the ears removed of any wax as required. A whisper test was then performed on all subjects at the bedside at a perceived quiet time of day, for example, not during ward rounds or visiting times. The method for the whisper test is outlined as follows.
One examiner (K.R.) stood arm’s length (0.6 m) behind the seated patient and whispered a combination of numbers and letters (e.g. 5-T-3). The patient was asked to repeat the sequence. In all cases, the examiner quietly exhaled before whispering to ensure as quiet a voice as possible. The screening test was considered to be passed if the patient responded correctly. When a patient responded incorrectly, the test was repeated using different number/letter combinations. Patients were deemed to have passed the screening test if they repeated at least three out of a possible six numbers or letters correctly. In all cases, the examiner stood behind the patient to prevent lip reading. Each ear was tested individually, starting with the ear with better hearing. During the testing, the non-test ear was masked by gently occluding the auditory canal with a finger and rubbing the tragus in a circular motion (see Figure 1).

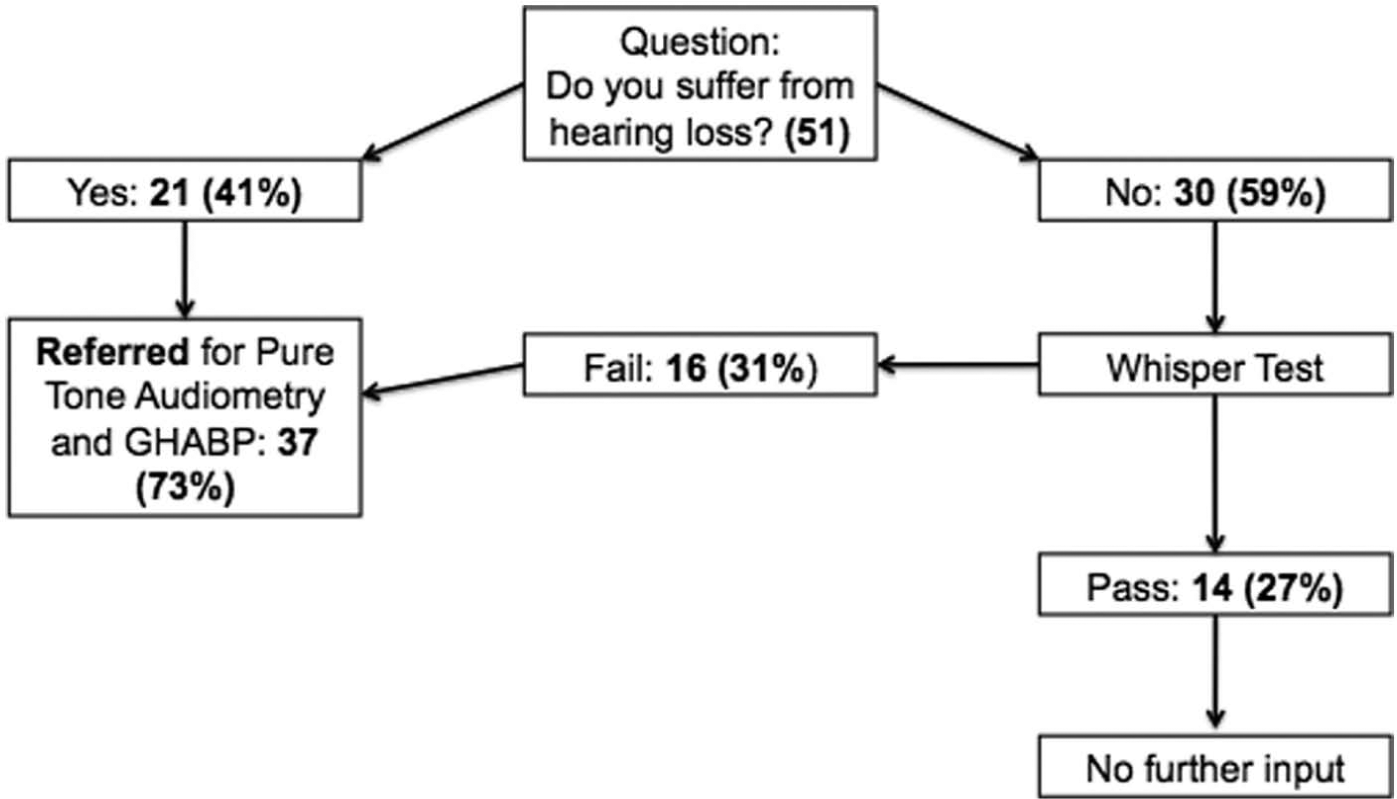
Data collection pathway.
The other ear was assessed similarly with a different combination of numbers and letters. Patients who reported hearing loss or failed the whisper test were offered pure tone audiometry. 9
Instrumentation
An Adastra DSM-425 digital sound-level meter was used to monitor the intensity of the whisper. In a quiet environment, the whisper was measured at 30 dB. This was reproducible to within 5 dB on repeat testing. On the wards, the sound metre was used to measure background noise. Consistent whispers (30 dB above background noise) were maintained by using the same assessor (K.R.) in all cases. A dual-range sound-level metre was used which had a decibel range of 30–135 dB. The device prior to use was calibrated to ensure minimal error and its accuracy was stated at ±1.5 dB.
Pure tone audiometry was completed under standard conditions in the Audiology Department at the Royal Berkshire NHS Foundation Trust. Hearing aids were offered as appropriate, in line with local protocol. No sources of funding were required as all aids were provided by patients’ local primary care trust as per patients outside this study.
Results and analysis
Hearing screening was performed on 51 subjects, aged between 70 and 95 years (mean 84.5 years). Of the 51 subjects screened, 21 (41%) reported hearing loss and were referred for formal audiological assessment. The whisper test was performed on the 30 subjects (59%) who did not report hearing loss. Of the 30 patients, 16 (53%) failed the whisper test and were referred for formal audiological assessment. The total number of patients referred for audiological assessment following hearing screening was 37 of the 51 patients tested (73%) (see Figure 2).
Proportion of patients in each group.
Of the 37 subjects (see Figure 3) referred to audiology, 20 underwent audiological assessment. Of those who did not undergo further assessment, 9 declined testing and 7 were found to be unsuitable due to significant medical comorbidities. One subject died before testing was performed. Of the 20 subjects who underwent assessment, 17 were found to be suitable for hearing aids (85%). Out of the 51 patients originally screened, 11 (22%) subjects were provided with hearing aids, where screening identified a 73% incidence of hearing impairment, of which 85% were thought suitable for hearing aids on audiological testing, and 55% of those tested actually received hearing aids. Of the 6 patients offered hearing aids, 1 declined and 5 were lost to follow-up. There were no adverse events during data collection.

Results at audiology.
Discussion
Literature from Bagai et al. 7 have demonstrated that both the screening question and the whisper test offer a sensitive means of detecting hearing loss. A ‘yes’ response when subjects are asked whether they suffer hearing loss has a summary likelihood ratio (LR) of 2.5, compared to 0.13 for a ‘no’ response. Inability to perceive whispered voice at 60 cm has a LR of 6.1, compared to 0.03 for those able to perceive whispered voice at 30 cm. 7
In this study, the use of a combined screening question and whisper test demonstrated a high rate of occult hearing loss in elderly inpatients – 73% of patients screened, and the whisper test alone identified hearing loss in 53% of patients reporting normal hearing. These results are consistent with previous studies which have also demonstrated a high rate of hearing loss in elderly inpatients. 10 Macphee et al. 11 identified that 61% of patients (mean age 81 years) on elderly care wards in a single institution had hearing impairment.
Crucially to our study, 22% of screened patients were provided with a hearing aid after assessment by a formal audiology service, or a screen:aid ratio of 4.6:1 (screen:aid ratio for those failing the whisper test was 8:1 and for those reporting hearing impairment 2.3:1). Not only does opportunistic hearing screening identify a significant unmet need among elderly patients, the screening triggers a referral process, which results in a significant proportion of patients receiving treatment. When taking into account the number of patients actually assessed by audiology following screening, 85% were offered hearing aids and 55% received them.
The extensive benefits of correcting hearing loss in elderly patients are well established, and yet the identification of deafness is all too often overlooked. Elderly hospitalised patients with complex comorbidities and frailty syndromes represent a distinct at-risk population, while being a convenient screening population for a clinician. We have shown that the significant unmet need among elderly inpatients can be identified with a quick and easily performed screening question and a whisper test which requires minimal training. The screening triggers referral for standard audiological assessment resulting in a high proportion of patients receiving hearing aids.
A follow-up study could be undertaken to gather information on those who received hearing aids, if they now still use them and if so, has it been continual or for only a few hours per day? Furthermore, looking at those who declined hearing aids initially and to see whether they were now using aids. This may help to further justify the benefit of this opportunistic screening. Data on improvement of quality-of-life scores would also be valuable consideration in a future study.
We recognise some limitations to this study: the hearing screening was conducted at the bedside on elderly care wards, and as a result, there were occasionally significant levels of background noise. This was done deliberately in order to replicate real-life conditions when a screening tool might be used in clinical practice. A sound-level meter was used to ensure that the whisper was presented at 30 dB above background. In addition, although we endeavoured to minimise exclusion criteria and include an accurate sample of elderly patients that might be encountered in clinical practice, we excluded patients with moderate and severe cognitive impairment (MMSE < 20). Such patients are more likely to have occult deafness overlooked and are likely to gain significantly from identifying and correcting hearing loss. However, a dedicated approach may be necessary which is less reliant on patient comprehension and active participation, and this was out with the scope of our screening method and formal audiology service. We encourage further work to identify easy screening methods applicable to patients with significant cognitive impairment.
Conclusion
This study has demonstrated that an easy opportunistic screening question and whisper test is an effective and feasible means of detecting a significant burden of occult hearing loss in elderly inpatients with and without cognitive impairment. The screening tool is an effective means of triggering further audiological assessment resulting in the administration of hearing aids to 22% of patient screened.
Footnotes
Acknowledgements
Abstract of this study was presented at the 14th British Academic Conference in Otolaryngology and ENT Expo, July 2012 and British Geriatrics Society Meeting, April 2013.
Declaration of conflicting interests
This material has never been published and is not currently under evaluation in any other peer-reviewed publication.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.