
Abstract
The American Heart Association recently included sleep health as one of eight factors that define cardiovascular health. Restorative sleep is a pillar of lifestyle medicine influenced by sleep duration, quality, and disorders. Short and long sleep duration are associated with greater risk of cardiovascular disease. Short sleep appears causally related to cardiovascular risk. Long sleep is more strongly predictive of cardiovascular risk, which may be due to comorbidities and other risk factors. Good-quality sleep appears to protect against the increased risk and is independently associated with risk of cardiovascular disease (CVD). Insomnia, particularly difficulty falling asleep and non-restorative sleep, is associated with an increase in cardiac events. Obstructive sleep apnea (OSA) is associated with cardiac risk and outcomes, which is typically observed in the context of contributing comorbidities. However, treating OSA with continuous positive airway pressure (CPAP) may not improve prognosis. Further research is needed to understand the causal mechanisms connecting sleep health with CVD and whether modifying sleep can improve outcomes. Sleep health should be considered as part of a holistic approach to improving cardiovascular health, as reflected in the scoring of LE8 and as one of the interrelated components of lifestyle medicine.
“Sleep appears to be obligate, non-negotiable. Sleep essentialism.” (Matthew Walker)
1
Domain, Metric, Measurement Tool, and Scoring Values for Sleep Health for Adults 20 and Older According to AHA’s LE8 Criteria.
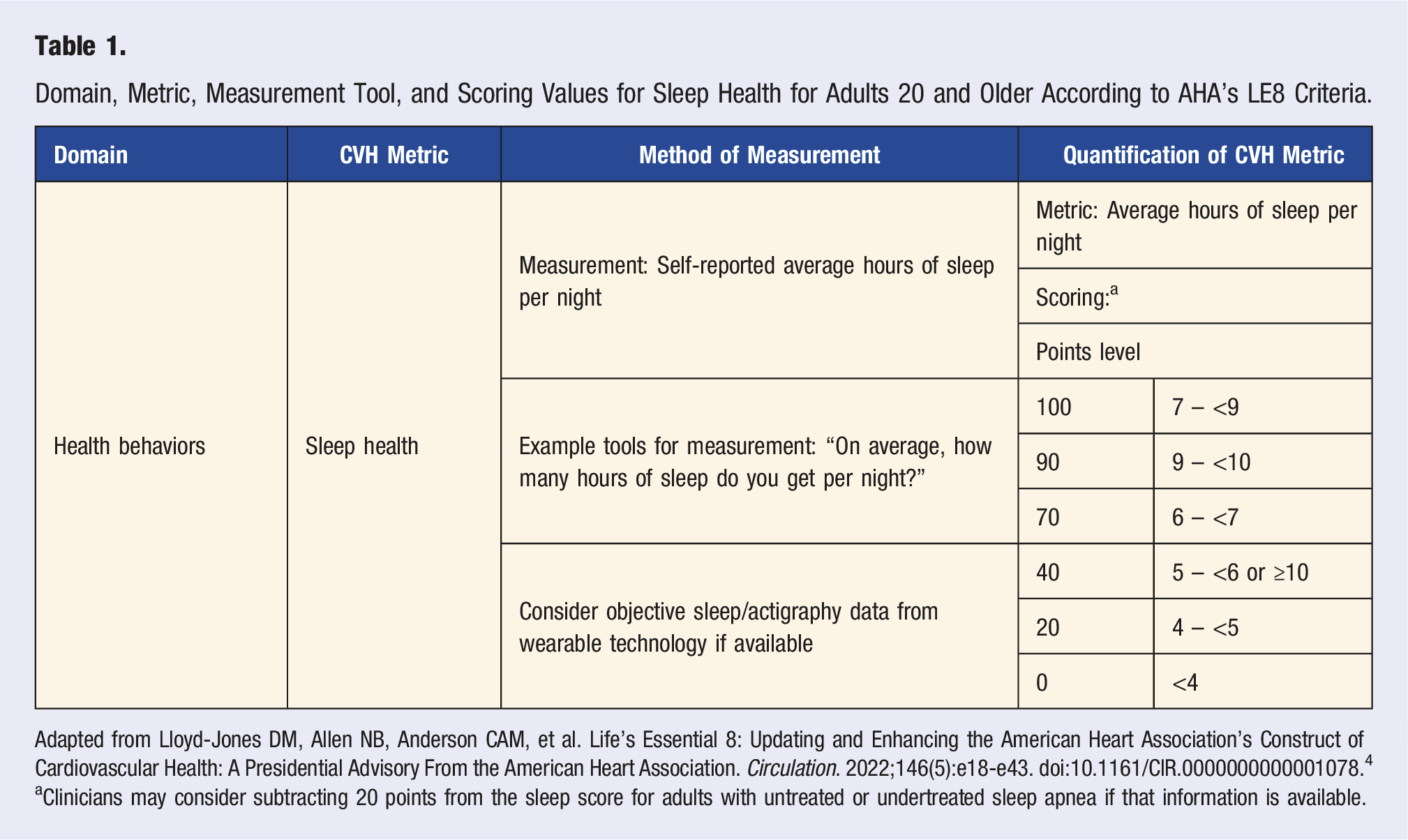
Adapted from Lloyd-Jones DM, Allen NB, Anderson CAM, et al. Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation. 2022;146(5):e18-e43. doi:10.1161/CIR.0000000000001078. 4
aClinicians may consider subtracting 20 points from the sleep score for adults with untreated or undertreated sleep apnea if that information is available.
Sleep Health
The addition of sleep health to the construct of cardiovascular health is a welcome development for the field of lifestyle medicine. Restorative sleep has long been a pillar of lifestyle medicine. 5 The recommendation is that individuals obtain 7 or more hours of sleep per night.6,7 Sleep health is a core competency for lifestyle medicine practitioners,8,9 and is one of seven intervention modalities in lifestyle medicine (nutrition, physical activity, sleep health, coaching behavior change, tobacco cessation, managing risky alcohol use, and emotional well-being).10,11 Sleep has a bidirectional relationship with disease and is implicated in many of the other pillars of lifestyle medicine. 12
Restorative sleep has been previously defined for lifestyle medicine, in consultation with the recommended sleep ranges provided by the National Sleep Foundation Scientific Advisory Council, 13 as the amount of sleep permitting a person to be “wide awake, alert, and energetic throughout the day without the aid of stimulants.” 12 This is broadly consistent with the scoring of the sleep metric in LE8. However, restorative sleep is influenced by several related parameters, including sleep duration, sleep quality, and the influence of sleep disorders. In turn, sleep duration and quality are affected by an array of cultural, social, psychological, behavioral, pathological, and environmental factors. 14 For example, short sleep duration could reflect the lack of a sufficient opportunity for 7-8 hours of sleep (e.g., work schedules, caretaking responsibilities, lifestyle choices) or some factor interfering with sleep duration that results in short sleep (e.g., insomnia, chronic pain, restless leg syndrome).
Methods
This analytical review was conducted by searching the MEDLINE Complete (National Library of Medicine, Bethesda MD) and PsycInfo (American Psychological Association, Washington DC) databases. We performed a search of the literature in the English language without limitations on the range of publication year but focused on more recent and contemporary reviews. We also reviewed all literature cited in the advisory statement by the American Heart Association which introduced sleep as the eighth metric in ideal cardiovascular health, 4 as well as recently published work that cited the AHA statement.
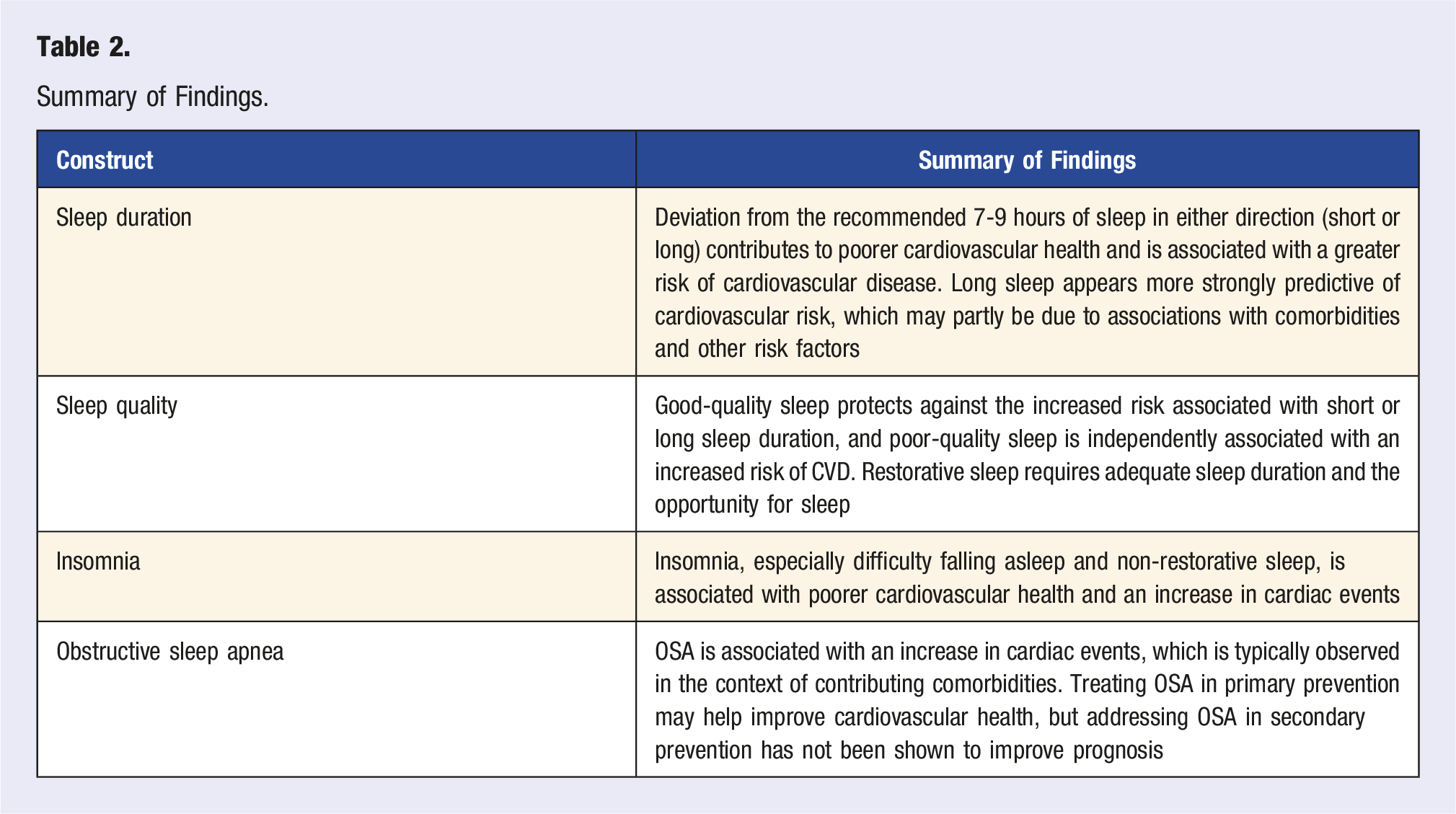
Summary of Findings.
Sleep Duration
Epidemiological research on the health risks associated with short and long sleep duration has measured the duration of sleep using self-reported hours of sleep per night. Short sleep is defined as less than 7 hours of sleep and long sleep is typically defined as greater than 9 hours per night. Sleep duration is linked with cardiovascular events and all-cause mortality, and individuals who report short sleep or long sleep are both at risk of cardiovascular disease (CVD).14-20 A meta-analysis of 19 studies with over 800,000 participants reported that both short and long sleep duration were associated with increased risk of cardiovascular mortality; this is the typical finding. 15
Because observational studies cannot confirm causality, prospective studies have also been summarized. A systematic review and meta-analysis of prospective studies that included 15 studies and 474,684 participants reported that short sleep duration was associated with increased risk of coronary heart disease (CHD) and stroke, whereas long sleep duration was associated with increased risk of both CHD and stroke and total CVD. 14 Another meta-analysis of prospective studies that included over 3.5 million participants reported a dose-response relationship confirming that deviating from the recommended 7-8 hours of sleep in either direction (short or long) was associated with a greater risk of CHD, CVD, and all-cause mortality. 20 However, the risk ratios for CVD and all-cause mortality appeared stronger for long sleep (1.36, 1.35) than for short sleep (1.14, 1.13), suggesting a greater risk of CVD for long sleepers. Greater risk among long vs short sleepers may reflect different mechanisms, such as the presence of comorbid health conditions among long sleepers.
Although prospective observational studies establish temporal precedence, in which measures of sleep duration precede cardiovascular outcomes, they cannot fully control extraneous and potentially confounding variables, such as the relationship between long sleep and certain phenotypes of depression. Toward that end, a recent meta-review and meta-analysis not cited in the AHA statement included both observational and Mendelian randomization studies. 18 Mendelian randomization studies allow for stronger causal inferences than observational studies, which are limited to statistically controlling for group differences. 21 The Mendelian randomization studies reported that genetically predicted short sleep duration was associated with an increased risk of coronary artery disease (CAD), myocardial infarction (MI), and heart failure, but not stroke, 18 supporting a causal relationship. In contrast, genetically predicted long sleep duration was not causally associated with the risk of CAD, despite the literature consistently supporting an association of long sleep and CVD risk. Long sleep may be a marker for risk as a reflection of the presence of other risk factors such as sleep apnea, 22 depression, or adverse social determinants of health such as low socioeconomic status and unemployment. 23
Thus, sleep duration is directly linked to CVD and cardiovascular mortality. Short sleep duration appears causally related to CVD, while long sleep duration may be a marker of risk. Short sleep duration is also related to cardiovascular health as measured using Life’s Simple 7. 24 The average American’s sleep duration has decreased compared to previous decades, which itself is an independent risk factor linked to health problems such as obesity, hypertension, diabetes, and immune status.12,25
Sleep Quality
Restorative sleep requires adequate sleep duration, which can reflect a sufficient opportunity to sleep and which can be impeded by poor sleep quality. Whereas most epidemiological research on sleep has assessed duration, there are fewer systematic reviews and meta-analyses reporting on the association of sleep quality and CVD.16,26 Subjective sleep quality is typically assessed using self-report questionnaires such as the Pittsburgh Sleep Quality Index.27,28 An earlier analysis of prospective studies reported that subjective poor sleep quality was associated with an increased risk of CAD. 16 The most recent used a Bayesian network meta-analysis, which stratified sleep quality into good and poor subgroups, to evaluate the relative independent contributions of sleep duration and quality to risk of CHD. 26 Good-quality sleep appeared protective against the increased risk associated with short or long sleep duration and suggested that poor-quality sleep was independently associated with increased risk. Specifically, among people reporting 7-8 hours of sleep per night, those with poor-quality sleep had an increased risk of CHD compared to those reporting high quality sleep (HF 1.3).
These findings are consistent with the observation that a small proportion (less than 25%) of the population are short sleepers who need less sleep and do not appear to experience adverse effects.20,29 For most people, short sleep is associated with poorer quality sleep due to disrupted sleep, sleep disorders, or other risk factors. For example, LE8 identifies poor sleep to be associated with worse psychological health and social determinants of health, which are “contextual drivers” of cardiovascular health. 4 Of course, when sleep quality is disturbed by sleep abnormalities, such as sleep apnea, patients have an increased risk of long-term mortality due to cardiovascular and cerebrovascular conditions. 30
With the addition of sleep, LE8 continues to capture the essential factors contributing to cardiovascular health in a more comprehensive and detailed manner. Specifically, sleep is subjectively captured through self-report of average hours slept per night, with overall scoring indicating the optimal sleep duration to be 7 to 9 hours. Clinicians are also encouraged to consider deducting points for those with untreated or undertreated sleep apnea, indicating a need to screen for sleep disorders and their subsequent impact on cardiovascular health. For example, when Life’s Simple 7 and LE8 scores were compared in relation to CVD risk, both were related to CVD prevalence, but only LE8 scores predicted CVD incidence in a cohort of older adults. 32 This may be a combined effect of LE8’s addition of sleep health and increased precision of metric scaling, however, the novelty of LE8 requires further research to compare its effectiveness to Life’s Simple 7 in measuring cardiovascular health and predicting CVD. For example, when objective measures of sleep duration, quality, and disorders assessed with actigraphy and polysomnography data were considered, LE8 scores were significantly associated with CVD prevalence and incidence. 32 AHA’s decision to include a measure of sleep duration is an important milestone in incorporating all aspects of sleep and their influence on cardiovascular health.
Insomnia
Insomnia is the most common sleep disorder in the general adult population, affecting nearly 10%–30% of adults worldwide and 15%–24% in the United States. It is broadly characterized by inability or difficulty falling or staying asleep and subjective dissatisfaction with sleep quality or duration.33,34 Thus, insomnia overlaps with sleep quality. Importantly, there are several methods to characterize insomnia presentation and its impact on daytime functioning: sleep dissatisfaction, presence of insomnia symptoms as listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), insomnia symptoms with daytime consequences, and insomnia diagnosis. 34 Insomnia presents as a situational, recurrent, or chronic problem, with most individuals endorsing long-term insomnia that persists even after the initial cause has faded. 35 Longitudinal studies found that 69% of individuals with insomnia reported it one year after baseline, 50% reported it three years after baseline, and 27% of those in remission eventually experienced a relapse in insomnia symptoms.36,37
Insomnia is also highly comorbid with psychiatric illnesses, predominantly depression, anxiety, and post-traumatic stress disorder. Around 50% of individuals with depression also experience insomnia, and those with insomnia are twice as likely to experience depression compared to those without sleep difficulties.38,39 Depression is a risk factor for the development of CVD40-42 and is associated with a worse prognosis.43-45 The overlap between insomnia and depression could implicate the contribution of depression in observed associations of insomnia with poorer cardiovascular health and risk of CVD.
Insomnia has been linked with CVD, predominantly CHD, hypertension, and all-cause morbidity and mortality. 46 A meta-analysis of 13 prospective studies found that insomnia was associated with a 45% increased risk of developing or dying from CVD. 47 The studies in this meta-analysis evaluated only individuals without CVD at baseline and who reported varying levels of insomnia or sleep complaints, an important sample given that some studies observed the impact of sleep following CVD occurrence. One major limitation, however, was the lack of sufficient evidence to support an association between insomnia and individual types of CVD, as the review could only confirm that insomnia was associated with an increased risk of fatal CVD.47,48 A subsequent meta-analysis with 4 additional studies reported that insomnia significantly increased the risk of cardiovascular outcomes and mortality, particularly after controlling for existing risk factors. Insomnia was associated with an increased relative risk (RR) of MI (RR = 1.41), CHD (1.28), stroke (1.55), and CVD mortality (1.33). 48
More recently, a review of 29 cohort studies with over 1.5 million participants sought to identify mechanisms underlying the association between insomnia and mortality. Whereas difficulty falling asleep and non-restorative sleep were significantly associated with increased risk of all-cause and CVD mortality, difficulty maintaining sleep and early morning awakening did not increase risk for all-cause mortality. 49 Of note, the increase in risk was most prominent in middle-aged and older adults. In contrast, another analysis including over 36 million participants found no difference in the mortality rate between those with and without insomnia. 50 However, when the results of a single study which accounted for 96% of the total sample size were removed, the odds ratio of mortality increased from 1.06 to 1.16. 50 The study in question examined the outcomes of sleep disturbances in older inpatients. 51 Insomnia was assessed using ICD9 discharge codes at diagnosis, and the prevalence was .75%, which appears much lower than typically reported. This discrepancy in findings may be partly a result of a selection effect and the operationalization of insomnia. Specifically, ICD9 discharge codes may not capture many cases of insomnia and include only patients who are hospitalized. With respect to defining insomnia, some studies focus on sleep duration and call it insomnia, when they, in fact, are different constructs. Others focus on diagnostic symptoms of insomnia or a clinical diagnosis of insomnia. To address this, some studies have examined the relationship between specific symptoms of insomnia and CVD. Difficulty falling asleep and non-restorative sleep were both associated with an increase in the hazard ratio (HR) of all-cause mortality (HR = 1.13; HR = 1.23, respectively) and CVD mortality (HR = 1.20; HR = 1.48, respectively) in older adults. 49 Difficulty maintaining sleep and early morning awakening were not associated with increased risk for either all-cause or CVD mortality. A diagnosis of insomnia was not associated with either, perhaps because the aspects of insomnia that overlap with sleep duration (e.g., difficulty falling asleep) and quality (e.g., non-restorative sleep) were driving the association. 49
The specific underlying mechanisms behind insomnia and CVD risk remain a focus of ongoing study. Potential mechanisms include shared genetic liability, increased activity in the sympathetic nervous system, increased stress-related hormones, or other more serious risk factors associated with insomnia.52,53 Nevertheless, the implications of insomnia for CVD and ideal cardiovascular health are incompletely understood. Not all symptoms of insomnia contribute to increased risk, as those related to non-restorative sleep ultimately affect sleep duration and quality and consequently appear more predictive of CVD.
Obstructive Sleep Apnea
Obstructive sleep apnea (OSA) is another of the most common sleep disorders, affecting 936 million adults worldwide.
54
In the United States, OSA prevalence is at a high, with mild OSA (apnea-hypopnea index (AHI) > 5 per hour) affecting 33.9% of men and 17.4% of women and moderate OSA (AHI
Excessive sleepiness, one of the most common symptoms of OSA, places these individuals at a greater risk of falling above the reference category of 7 to 9 hours for sleep duration resulting in low-quality sleep for longer hours during the night. 56 Individuals with OSA are also two to three times more likely to develop cardiovascular and metabolic diseases, therefore placing them at higher risk for comorbid disorders that further contribute to cardiovascular risk. 57
OSA is highly associated with known risk factors such as obesity, hypertension, and diabetes. 52 It is strongly associated with systemic hypertension, pulmonary hypertension, and cardiac arrythmias. 58 Conversely, OSA is an independent risk factor for CVD, particularly in those with severe OSA. However, it becomes difficult to disentangle the relationship between sleep apnea and comorbid diagnoses and differentiate the primary condition from the secondary. 59
A 2013 meta-analysis of prospective observational studies found OSA to be a strong independent factor for all-cause and cardiovascular mortality, with a 1.6 and 2.6 fold increase in risk respectively, with the more severe the apnea the higher the risk.60,61 A second 2013 meta-analysis found that moderate-to-severe OSA increased the risk of experiencing a cardiovascular event by 2.5-fold and doubled the risk of stroke. 62 The more severe the OSA, the higher risk a person was for developing CVD.
Whereas the underlying mechanisms connecting OSA and the increased risk of cardiovascular events have not been fully elucidated, OSA worsens the mediating risk of diabetes and hypertension. 62 Specifically, OSA may lead to intermittent hypoxia, intrathoracic pressure swings, recurrent arousals, and increased sympathetic nervous system activity, all of which have been found to increase the development of atherosclerosis, leading to an increase in cardiovascular events. 62 Despite a steady increase in evidence, a consensus on an established causal pathway between OSA and CVD has not been reached. This may be due in part to the inherent limitations of observational studies such as confounding bias and selection bias given that many OSA studies are conducted in clinics where the patient population differs from the general population (e.g., patients referred for evaluation and treatment may have higher cardiovascular risk). 62
Modifying Sleep
The AHA statement highlighted the relative lack of evidence that interventions modifying sleep can improve cardiovascular health. 4 However, it is feasible to extend sleep for individuals who experience short sleep, and an increase in sleep duration may lower the risk for cardiometabolic problems. 63 Treatments for sleep health generally fall into the categories of lifestyle changes to increase adequate sleep opportunities (e.g., reduce voluntary sleep restriction), address insomnia, and treat sleep apnea.
Treating Insomnia
The leading treatment for insomnia is cognitive behavioral therapy for insomnia (CBTi: SeeSupplemental Digital Content for a description of CBTi). In patients free from CVD, CBT-I did not improve early markers of CVD. 64 However, CBT-I also impacts cardiometabolic health biomarkers, consistently improving glycemic regulation and c-reactive protein. 65 Whether interventions for insomnia decrease cardiovascular risk in primary care has not been adequately tested. For patients with CVD, CBT-I has been shown to improve sleep, lower levels of anxiety and depression, reduce consequences of insomnia, including symptoms and adverse health effects, and overall improve quality of life.66,67 Many of these results are limited but promising, including improvements in sleep efficiency and sleep quality. 68 CBT-I improved sleep in patients with comorbid heart failure and insomnia69,70 but not biomarkers of the hypothalamic pituitary axis or autonomic function. 69 Whether the treatment of insomnia improves cardiovascular prognosis in secondary prevention has not been demonstrated. 67
Treating Obstructive Sleep Apnea
As a result of the high comorbidity between OSA and obesity, the first-line treatments for individuals with OSA are physical activity, diet control, and weight loss.71,72 While they are meant to primarily target obesity and OSA, these interventions have the added benefit of decreasing blood pressure, depressive symptoms, anxiety, and fatigue, all of which also result from non-restorative sleep. Of course, sustained behavior changes and maintained weight loss are challenging goals for many patients, and a substantial subset of patients who present with OSA are not obese. Thus, sleep apnea is also treated using continuous positive airway pressure (CPAP). Observational studies suggested that CPAP was moderately effective for OSA, 73 however, CPAP adherence is low. To see improvement in OSA symptoms, patients need to be using the CPAP 4-6 hours per night at least 70% of the week, a practice that only 50% of patients maintain after 6 months and 17% after 5 years.74,75 Compliance with CPAP is a well-recognized problem that has yet to be sufficiently addressed.
Some studies have reported that treating central sleep apnea using CPAP decreased the frequency of cardiovascular events, lower the risk of cardiovascular mortality, and significantly lowered blood pressure.60,73,76 CPAP treatment can also lower daytime sleepiness and increase health-related quality of life, suggesting improvement in sleep health and non-restorative sleep.77,78
However, several major randomized controlled trials did not find a reduction in future cardiovascular events with CPAP use. 79 Specifically, the international Sleep Apnea and Cardiovascular Endpoints (SAVE) study examined mostly male patients with moderate-to-severe OSA split between a CPAP group and a usual-care group. While those who used the CPAP experienced a decrease in their apnea-hypopnea index, there was no significant difference between the two groups in terms of a decrease in primary cardiovascular endpoint events. 80 For patients with CAD, CPAP did not improve cardiovascular outcomes. 81 For patients with chronic heart failure (CHF), CPAP slightly improved daytime sleepiness but did not improve CHF severity. 82 While these findings may be disheartening, future trials should look at individuals with moderate-to-severe OSA with a focus on excessive sleepiness and stricter CPAP adherence, as these are two factors that may have limited the effectiveness of CPAP in previous trials. 79 Nevertheless, current literature suggests that treating OSA with CPAP has not improved prognosis. It is possible that high adherence and the addition of other lifestyle changes, particularly weight loss and dietary changes that concurrently improve cardiovascular health, would provide more promising results.83,84
Limitations
This analytical review focused on systematic reviews and meta-analyses to summarize the evidence prompting the addition of sleep health to the AHA’s construct of cardiovascular health in adults and whether modifying sleep can improve prognosis. In keeping with these aims, we did not address some topics, such as screening for or assessing sleep beyond providing the scoring metric for sleep health. For additional information on assessing sleep, see the Supplemental Digital Content. Furthermore, we did not cover how to treat insomnia or sleep apnea; the Supplemental Digital Content describes CBTi in more detail. We did not describe the effects of cardiac events on sleep health or the influence of confounding factors such as predisposition and lifestyle factors; nevertheless, these interactions play an important role in understanding the dynamic characterization of cardiovascular health. We did not address parasomnias (see Quan, 2009 5 ) or the relationship between sleep and health more broadly (e.g., in children). However, there are excellent resources available such as a recent book, 55 a recent review in The Journal of Family Practice, 12 and information on sleep as a core competency for lifestyle medicine practitioners.8,9
Conclusion
Understanding the multifactorial, bidirectional relationship between sleep and cardiovascular health is an important step in contextualizing its far-reaching impact on those at risk for CVD. Non-restorative sleep can lead to an increased risk of CVD and mortality. Given the impact of confounding factors within research studies, continuation rates, and insufficient interventions, the evidence that improving sleep improves prognosis is mixed. It is possible that the adverse effects from non-restorative sleep may have already emerged by the time sleep becomes a focus of treatment in patients who have or who are at high risk for CVD. For example, in patients diagnosed with OSA, treatment with CPAP has not been shown to reduce cardiovascular risk. These findings underscore the need for early screening for those with insufficient sleep, low-quality sleep, non-restorative sleep, and sleep disorders as part of a comprehensive approach to the primary prevention of CVD. Those who lack a sufficient opportunity to sleep require particular attention, as this may be a driving force behind subsequent sleep problems. The effect of obesity on sleep quality and OSA further highlights the need for integrative treatment focusing on weight loss, exercise, and dietary quality. Sleep health should be considered as part of a holistic approach to improving cardiovascular health, as reflected in the scoring of LE8 and as one of the interrelated pillars of lifestyle medicine. When it comes to cardiovascular health and disease, sleep is essential.
Supplemental Material
Supplemental Material - Sleep is Essential for Cardiovascular Health: An Analytic Review of the Relationship Between Sleep and Cardiovascular Mortality
Supplemental Material for Sleep is Essential for Cardiovascular Health: An Analytic Review of the Relationship Between Sleep and Cardiovascular Mortality by Yasmine M. Eshera, Lyubov Gavrilova and Joel W. Hughes in American Journal of Lifestyle Medicine.
Footnotes
Acknowledgments
We would like to thank Dr Noha Eshera, MD and Dr Cameron Bixby, DO for their comments on a draft of this review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.