
Abstract
The prevention and treatment of atrial fibrillation includes risk factor modification beyond ablation, with lifestyle modifications including treatment of obesity through diet and moderate exercise being at the top of the list. Losing 10% of body weight if obese, a plant-based diet, exercise, maintaining systolic blood pressure below 130 mm Hg, treatment of sleep disorders and obstructive sleep apnea, stress management, and treatment of depression and anxiety should all be included in treatment. Maximizing evidence-based treatment of chronic obstructive pulmonary disease and diabetes is also paramount.
‘Atrial fibrillation (AF) is commonly encountered in practice, and its diagnosis results in increased cardiac morbidity such as stroke and heart failure.’
Atrial fibrillation (AF) is commonly encountered in practice, and its diagnosis results in increased cardiac morbidity such as stroke and heart failure. A simple way to think about AF management is the ABC pathway: “A”—avoid stroke with anticoagulation; “B”—better symptom management, with patient-centered decisions on rate or rhythm control; and “C”—cardiovascular risk and comorbidity management, including attention to lifestyle factors. 1 This article will focus on the “C “pathway with the following 10 lifestyle changes that can help your patients with AF have a better quality of life.
Step 1: Treat Obesity and Aim for 10% Weight Loss
Many experts believe the increased rate in AF is due to the increase in obesity, and it has been shown that weight reduction and risk factor management result in lessening the effects of AF. 2 Rates of AF are rising. Overall, AF hospitalizations increased by 23%, from 2000 to 2010. The most frequent coexisting conditions are hypertension (60.0%), diabetes mellitus (21.5%), and chronic pulmonary disease (20.0%). 3 All these 3 diagnoses are linked to obesity. With this is in mind, when a patient is diagnosed with AF, the following lifestyle goals should also be part of the overall plan.
Weight loss is paramount. This is because every unit increase in body mass index (BMI) is associated with an increased risk of AF by 4%. 3 In a study of 3 million US adults, the authors noted that there was a doubling of risk (50%) in men and women across all ages when there was a 10 unit rise in BMI. 4 Surprisingly, in this study, factors one might associate with AF were not present. Blood pressure was less strongly associated with AF, and only in those younger than 70 years, suggesting some other mechanism behind the BMI and AF association. In addition, current smoking was not associated with AF. As a result of these findings, the authors concluded that rising rates of obesity might be driving the observed increase in AF in the developed world. 4 In addition, all classes of obesity are associated with increased levels of high-sensitivity C-reactive protein, 5 and it has been suggested that inflammation has a role in electrophysiological remodeling which could lead to AF. The role of C-reactive protein in AF has not been elucidated, however in a large study looking at the general population, high C-reactive protein levels were associated with risk of AF, which supports the inflammation hypothesis in AF pathogenesis. 6
With this in mind, we need to work on decreasing obesity rates earlier to prevent AF; patients should be warned of the dangers of AF and other possible diseases when they are diagnosed as being overweight (BMI 25-29.9 kg/m2) or obese. This could be a serious aid in prevention of obesity.
In patients who have AF, The 2019 American Heart Association Guidelines has added weight loss to its current new guidelines for treatment. 7 The main reason for promoting these guidelines was a trial by Abed et al 8 who evaluated the effect of weight loss on obese patients with AF for 15 months. 8 They found that those who lost the most weight (10% or more) had significantly greater reduction in AF symptom burden, severity, and number of episodes per week. It also showed that those with weight fluctuations did more poorly, pointing to the importance of weight loss and maintenance. Patients were place on a lowered calorie diet (1200-1500 calories per day). Patients who lost the most weight, that is over 10%, and improved 2 metabolic equivalents of activity, had less recurrence and AF symptoms. These were significant findings. 8
Step 2: Push for (Mostly) Plant-Based Diet
A plant-based diet should be encouraged. There is not much evidence on diets and AF; consequently, we will discuss heart healthy diets.
Patients can become confused as to what they are supposed to do, as not all plants are healthy (eg, French fries). 9 A recent study showed that plant-based diets containing higher amounts of healthy foods, such as whole grains, fruits, vegetables, nuts, legumes, oils, tea, and coffee are associated with lower cardiovascular disease (CVD) risk. Plant-based diets with less healthy plant foods, such as refined grains, potatoes/fries, and foods, juices and beverages that are high in added sugar, are linked to increased risk. The southern diet (fried foods, processed meats, added fats and sugars), which is associated with hypertension, should be discouraged. 10 What you eat makes a big difference in all aspects of health.
A wide spectrum of plant-based diets can be nutritionally adequate, confer cardiovascular benefits, and also be more environmentally sound. 11 Rather than debating with patients about which is the healthiest diet, the focus should be on improving overall diet and increasing eating healthy plants with this in mind. A brochure with a list and pictures of the best foods would help. A registered dietician can help immensely with this transition, as well.
If there is a request for a specific diet, one can recommend the Mediterranean diet. The traditional Mediterranean diet is primarily plant-based with fish and no significant amount of added sugars or processed foods. In addition, olive oil, nuts, high fruit and vegetable consumption may decrease AF due to the presence of natural antioxidants. Extra virgin olive oil may help prevent AF. 7
The American Heart Association recommends 2 servings of fish per week. 7 Unfortunately, research on fish oil supplements has shown no clear evidence as yet of any benefit for reducing the effects of AF. Omega-3 foods are heart healthy because they reduce blood clot formation and decrease inflammation. Included are fatty fish and plant foods such as walnuts, flaxseeds, and canola and soybean oils. In terms of fish, fatty fish such as salmon, tuna, sardines, mackerel, and trout are full of omega-3 fatty acids. Interestingly, in a Swedish study, fatty fish was not associated with a lower risk of AF. However, 3 servings of consumption of lean fish per week (cod, saithe) was associated with a lower risk of AF, 12 and more studies are needed to discern if there is a solid relationship. It appears the eating of leaner fish may have more positive effects.
Alcohol use should be very limited. There has been a consistent linear dose-response relationship between alcohol consumption and AF risk, with an overall average 8% increase in AF risk per 1 drink/day increment in alcohol consumption. 13 Patients with more than 21 drinks per week were most vulnerable. In another large study, patients who drank once a week had the lowest risk and those who drank everyday had the highest risk of new-onset AF over binge drinkers. 14
Coffee intake is not associated with AF. 15
Step 3: Encourage Moderate Exercise and Yoga
Exercise at 30 minutes 3 to 4 times a week, working up to 200 minutes per week at moderate intensity.
Low physical activity is a risk factor for AF. 16 Moderate exercise is associated with decreased AF occurrence. Moderate exercise is defined as 150 minutes of moderate-intensity exercise, such as walking several times per week. A Swedish study noted that daily walking or cycling decreased AF risk. 17
Again, to emphasize that in a study of those who lost 10% of their body weight and increased their exercise endurance by 2 metabolic equivalents, freedom from arrhythmia without drug therapy was evidenced in 75% of them. 2 This was not a randomized control trial.
Although there is a relationship between endurance exercise and AF, this represents a small group of people already at low risk of developing AF. However, one observational study is worth noting. 18 In this study, every-day jogging was associated with an increased risk of AF over cycling, racquetball, and swimming, and only in men younger than 50 years. They participated in endurance exercise 5 to 7 days per week. This is thought to be due to a higher parasympathetic tone in these younger men. With most patients, exercising vigorously is not an issue, but if they are younger than 50 years, it seems prudent to advise patients with AF against daily running.
With regard to a review of exercise-based cardiac rehabilitation with various types of AF, a Cochrane review showed no clinically relevant effect on health-related quality of life. Pooled data showed a positive effect on the surrogate outcome of physical exercise capacity, but due to the low number of patients and the moderate to very low quality of the evidence, the researchers concluded that high-quality randomized trials are needed to assess the benefits and harms of exercise-based cardiac rehabilitation for adults with AF on patient-relevant outcomes. 19 More research needs to be done in order to properly advise patients with exercise regimens.
In addition, yoga has been associated with reductions in the mean number of symptomatic AF episodes. In one study, almost one-quarter of patients with AF during the control period experienced no AF episodes during the yoga training, which occurred twice a week. 20 A larger, randomized, and multicentered trial would certainly help validate these findings.
Step 4: Adequate Control of Hypertension Aim for ≤130/80 mm Hg
In patients who do not have AF, but do have hypertension and left ventricular hypertrophy, a systolic blood pressure ≤130 mm Hg was associated with a lower risk of new-onset AF. 21
Among patients with AF undergoing hypertension treatment, patients with a blood pressure of ≤130/80 mm Hg was the optimal blood pressure treatment target for patients with AF. In a large Chinese study, both angiotensin receptor blocker (ARB) and angiotensin-converting enzyme inhibitor (ACEI) reduced new-onset AF in patients with hypertension. An ARB prevented AF better than and ACEI in patients with a history of prior stroke or transient ischemic attack. 22
Step 5: Encouragement of Restful and Adequate Sleep: Aim for 7-8 Hours and Test and Treat for Sleep Apnea
Quality and duration of sleep is emerging as an important factor in diseases such as obesity, diabetes and cardiovascular disease. Adequate sleep (7-8 hours) is extremely necessary in combating obesity. Inadequate sleep quality and duration is emerging as an important risk factor for many diseases, including AF. Interestingly, in a large observational study, each 1-hour reduction in sleep duration was associated with 17% greater risk of prevalent AF and 9% greater risk of incident AF. 23 Working with patients to improve sleep duration is very important.
Obstructive sleep apnea (OSA) causes obstruction of airway during sleep. Treatment is generally with a continuous positive airway pressure (CPAP) mask, which has been shown to help with freedom from AF after ablation.
A meta-analysis of 4000 patients revealed that OSA confers at 25% higher AF recurrence risk following ablation. 24 Adequate sleep is also a factor for those patients who are undergoing catheter ablation; those with treated OSA experience lower recurrence rates of those patients without OSA. 25 Thus, those patents with new diagnosis of AF that have symptoms of OSA should have a sleep study as soon as possible and be treated with CPAP. 25 A recent study has shown that early treatment of OSA with a 16-week program of weight loss and CPAP has resulted in improvement of weight, in comparison with those without CPAP. 26
Step 6: Treatment of Stress and Working Less Hours
In the REGARDS study, increasing levels of perceived stress were associated with prevalent AF and they suggested targeted interventions aimed at reducing stress in those with AF. 27 Interestingly, when they looked at the association between perceived stress and AF by income as a continuous variable, the association was significantly stronger for those with low compared with high incomes.
In addition, working long hours is a noted factor. In a large European study, those who work long hours, especially more than 55 hours per week, are at risk for AF. 28 They showed that employees working long hours (over 55 hours) were 40% more likely to develop this cardiac arrhythmia than those working standard hours (less than 35-40 hours). As this association seemed to be independent of other known risk factors for AF, further research is needed to determine which mechanisms are responsible, such as whether shorter sleep durations are actually the cause.
Patients who work long hours should be counseled to work less if possible, and target interventions to decrease stress is helpful.
Stress reduction as a treatment has not been studied in detail.
Step 7: Quit Smoking
Although results have been inconsistent in the relationship of smoking and AF, in the REGARDS study there was an increased rate of smoking in patients diagnosed with AF, particularly in younger patients, those with existing heart disease, and nonwhites (American English is nonwhites). 29
However, since patients with AF are at risk for thromboembolism, cancer, and increased mortality, 30 quitting smoking is advantageous in all cases.
Steps 8 and 9: Treat Anxiety and Depression
AF is linked with depression, anxiety, and mood disorders as well as poor quality of life, which can be improved with treatment.
In 1 study, approximately one-third of AF patients had elevated levels of depression and anxiety, which persisted at six months. Symptoms of depression were the strongest independent predictor of future quality of life in these patients. 31 In men, data from the Framingham Offspring Study have implicated tension, anger, and hostility as risk factors for AF in males. 32
In a new moderate-sized study looking at AF and depression, patients with less education and lower income were far more likely to experience depression than those with bachelor’s or graduate education and higher income. In this study patients treated with cardioversion or antiarrhythmic medication had less likelihood of minor or major depression. The authors recommended to screen for depression in patients with AF. 33 In another study, quality of life was better and patients reported that they had less psychological distress when taking novel anticoagulants over coumadin, presumably due to less side effects such as bleeding.34,35
In another study, diagnosis of depression in patients with AF was associated with an increased risk of ischemic stroke. 36
Anxiety and depression are related to the development and recurrence of AF, even after ablation, than those patients without these psychiatric diagnoses. 37 In general, patients have less anxiety and depression after left atrial ablation, but those who continue to be depressed are more likely to have recurrence. In a small study, AF reappeared after ablation in 85% of the depressed patients in comparison with 39% in the not depressed. 38
In light of the above findings, patients should be screened and treated for anxiety and depression. After diagnosis, patients need to be treated with cognitive behavioral therapy (CBT) or a selective serotonin reuptake inhibitor (SSRI) antidepressant. One meta-analysis showed that CBT was effective in reducing anxiety and depression and improving quality of life in patients with cardiovascular disease. However, considerable heterogeneity was present between studies and AF patients were poorly represented. Face-to-face CBT sessions seem to achieve the greatest patient benefit. More studies need to be done to look and see if CBT decreases AF occurrence or severity. 39 In a Swedish randomized study, patients with AF and their spouses were treated with a brief dyadic mindfulness CBT-based program, which consisted of three 2.5-hour meetings over nine weeks, teaching patients different mindfulness-based therapies such as deep breathing and positive emotions. Those in the treatment group had improved quality of life and decreased psychological distress as compared to usual care over a duration of 12 months. 40
Unfortunately, there are not randomized studies of pharmacologic treatment of depression in AF.
CBT, if feasible, should be tried first as all SSRIS are associated with weight gain, especially after a few years. 41
The studies seem to paradoxically suggest both management of mood as a means to reduce AF and also management of AF as a means of supporting mood: and this is accurate. On reflection, we do this often in medicine. For example, most studies show that for diabetic patients with depression, when treated for both at the same time, have improved glycemic control and adherence to medicine. 42 This is often accomplished in multidisciplinary groups. One study did look at collaborative care groups to manage complex patients with diabetes, cardiovascular disease, and depression, and showed improved outcomes overall. 43
Step 10: Treat Chronic Disease, Diabetes, and Work on COPD Management
Diabetes has been associated with higher risk of developing a fib, as was longer duration of diabetes and worse control. 44 In this study, a hemoglobin A1c more than 9% was associated with twice the risk of AF than when it was less than 7%. In diabetic patients with AF, a new study showed an increase stroke risk with inadequate control, although this was not present in those who had diabetes for more than 10 years. This suggests that maintaining control of diabetes is important in preventing AF and stroke. 45
Among patients with AF, chronic obstructive pulmonary disease (COPD) is associated with higher symptom burden, worsening quality of life, and worse cardiovascular and bleeding outcomes.
Every effort should be made to increase exercise performance and weight loss to improve outcome at diagnosis. All patients with COPD should be considered for referral to a pulmonary rehabilitation program, as this decreases 30-day readmission rates for COPD. 46
Patients with COPD and AF have not been studied specifically as to whether pulmonary rehabilitation results in improvement and recurrence of AF, and this is warranted.
In conclusion, the prevention and treatment of AF includes risk factor modification beyond ablation, with the goals of treatment being a 10% weight loss in those patients with obesity through a plant-based diet and moderate exercise being at the top of the list. Cardiology departments should consider use of a multidisciplinary team to help in risk factor management. 47 In addition, after reviewing the literature, the following questions come to mind: (1) studies looking at cardiac rehabilitation that takes into account all of the above recommendations as to how they affect outcomes needs to be undertaken; (2) a multidisciplinary team that includes weight loss, exercise, psychological care, and a registered dietician would all seem feasible; (3) it would seem that this could be a great opportunity for research to look at shared medical meetings (even group Zoom televisits in light of COVID) that focus on risk factor reduction; and (4) randomized studies on which treatment is superior of depression in patients with AF.
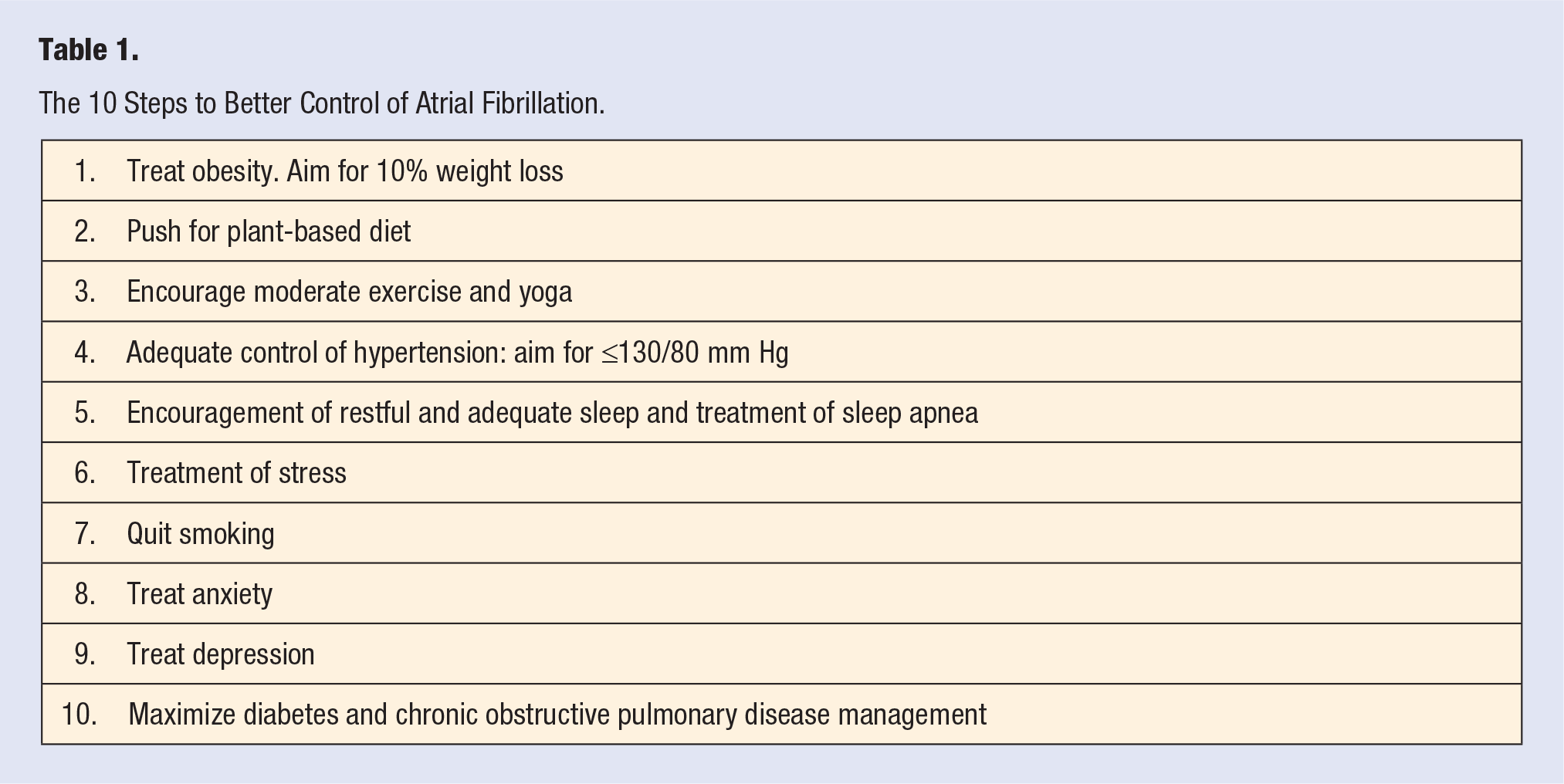
Again, lifestyle changes should include the following: (1) if obese, losing 10% of body weight; (2) adopting a mostly plant-based diet and encouraging the patient to see a registered dietician; (3) encouraging moderate exercise; (4) maintaining systolic blood pressure <130 mm Hg; (5) eliminating or decreasing frequency of alcohol; (6) treatment of sleep disorders and OSA; (7) stress management; (8) treatment of depression and anxiety; (9) if diabetic, HbA1c should be less than 7%; and (10) maximizing treatment of COPD and pulmonary rehabilitation should all be part of the treatment plan (Figure 1 and Table 1).

Lifestyle management of atrial fibrillation.
The 10 Steps to Better Control of Atrial Fibrillation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.