
Abstract
“The amount of nutrition education a physical therapist received was shown to be beneficial in providing care.”
Introduction
A physical therapist (PT) is often thought of as a “movement expert,” but optimizing human movement and function requires a broad understanding of factors, including nutrition, that impact the ability to move, restore function, and prevent disability. 1 Nutrition is the science of how people obtain and use substances from food to maintain their body’s structural and functional integrity. 2 Knowledge of nutrition and its potential impact on a patient is important in maximizing rehabilitation outcomes, including strength, healing, functional mobility, and quality of life.2-8 Nutrition patient education may, however, be an underutilized skill set.
The American Physical Therapy Association (APTA) recognizes the direct impact of nutrition on patients’ recovery and ability to function physically, and recommends physical therapists screen for and address nutritional intake and eating patterns with their patients. 9 Unfortunately, potential barriers exist for physical therapists who desire to address and educate patients on the topic of nutrition.10,11 It is within the professional scope of physical therapist practice to screen for and provide nutrition education, as long as it follows any documented state practice laws on the matter. 12 Individual state physical therapy practice acts vary, however, and it is common for state laws to be silent on this topic, leaving therapist unsure of their role. Another potential barrier is the extent of knowledge and comfort in discussing nutrition with patients, which vary between physical therapists. The APTA advises that a physical therapist consider their own understanding of nutrition, as well as appropriateness of consultation and co‐management with or referral to a registered dietitian before providing education to their patients. 12
The Commission on Accreditation in Physical Therapy Education (CAPTE) requires that Doctor of Physical Therapy students have knowledge and learning experiences in nutrition content, however, specifics are not identified, and programs have freedom to determine how they will deliver content to achieve their program outcomes. 13 Concurrently, CAPTE requires that physical therapists are able to determine when patients/clients need further consultation or referral to another health care professional, such as a registered dietitian. 13 CAPTE additionally states that students in accredited physical therapy programs should be prepared to “provide physical therapy services that address primary, secondary, and tertiary prevention, health promotion, and wellness to individuals, groups, and communities.” 13 These criteria give guidance, but also leave room for interpretation. There is no published data on the quantity or specific curricular content related to nutrition in physical therapy programs across the United States.
The purpose of this study was to examine physical therapist’s education and comfort on nutrition related topics, as well as frequency of nutrition education given to patients in the northeast region of the United States. The aim was to assess the reported education background and comfort level of practicing physical therapists on the topic of nutrition and provide information that could lead to curriculum changes in academic doctor of physical therapy programs. It is hypothesized that based on recent changes in the educational demands of physical therapists, there would be a reported lack of comfort in nutrition, and nutrition education would be an underutilized intervention in clinical practice.
Review of Literature
Despite potential variability in education, there is a growing need for physical therapists to alter goals, strategies, and interactions with patient populations to include more lifestyle counseling beyond exercise.9-16 This includes providing nutrition education to patients/clients. The APTA advises that physical therapists take proactive roles with their patients to promote wellness early in an individual’s lifespan to prevent chronic disease and disability and reduce patient inequities. 17 This aligns with Healthy People 2030, which is focused on helping people reach and maintain a healthy weight by healthy eating and getting enough physical activity. 18
For physical therapist to take a proactive role and address nutrition with patients, they must understand how nutrition directly relates to disease risk and patient outcomes. Suboptimal eating patterns, including high calorie and high fat diets, lack of fruits, vegetables, and essential nutrients, and high intake of low-quality carbohydrates serve as risk factors for hyperinsulinemia, insulin resistance, dyslipidemia, low-grade systemic inflammation, and increased oxidative stress.19-25 This intern increases the risk of noncommunicable diseases such as heart disease, stroke, type 2 diabetes, irritable bowel syndrome, and some cancers.3,26-32 Additionally, increased fat intake can significantly increase blood pressure, total peripheral vascular resistance, and oxidative damage to the endothelial cells lining the blood vessels. 33 These changes cause decreased blood flow and impair the ability to transport nutrients to and take waste products away from working muscles.7,33-35 Increased caloric intake, poor food choices, and hyperinsulinemia also contribute to the rising obesity epidemic in the United States.2,20,21,23 Among adults aged 20 and over, the prevalence of obesity is 41.9%, and the prevalence of severe obesity is 9.2%, according to pre-pandemic health outcome estimates from the National Health Statistics Reports. 36 Persons who classify as obese are at higher risk of developing osteoarthritis and other musculoskeletal ailments as well as hypertension, stroke, cardiac and renal disease.37-40 Patients with these conditions are frequently seen by physical therapists. Promoting change in nutritional habits can reduce the risk of developing these comorbidities or slow down the progression of disease, and subsequently improve physical function and quality of life.32,33 The need for health care professionals to improve the delivery of nutrition related education in all practice settings continues to rise as chronic diseases and comorbidities continue to impact public health. 41
Educating patients on the benefits of eating foods rich in vitamins and minerals, and avoiding saturated fats and low-quality carbohydrates, may positively impact disease risk and comorbidities. For example, decreasing sodium intake and increasing potassium intake can lower a patient’s blood pressure and decrease their risk of heart disease.42-47 Increasing the consumption of fruit and vegetables, nuts, can decrease the risk of stroke by lowering blood pressure.48-52
Many vitamins and minerals play an influential role in bone and tissue healing, which is important knowledge for physical therapists who treat patients healing from wounds, trauma or surgery. Vitamins D, C, K, and Calcium all play a role in bone metabolism and decreasing the risk of fractures,36,53-56 increased bone healing,55,57 and decreasing the risk of osteoporosis.36,58,59 Conversely, a diet lacking in these vitamins and minerals has been shown to delay wound healing and increase risk of hip fracture, surgical site infection, thrombosis, pressure ulcer development, and postoperative mortality. 13 Complications after surgical operations resulting from poor nutritional status can also prolong hospital stays, cost, and rehabilitation time.36,60 A greater scope of knowledge and comfort with this information may allow physical therapists to participate in more productive conversations with their patients and elicit better outcomes.
A study completed by Snodgrass, et al, surveyed Australian physical therapists to identify knowledge, practices, and beliefs of physiotherapists regarding weight management advice to overweight or obese clients. Of the physical therapists surveyed, education in weight management was received by only 20% during either their professional entry level education or 10.8% during subsequent professional development. When asked about best practice for dietary management of clients who were overweight or obese, more than half of the physiotherapists (61.5%) reported a low level of knowledge, and 15.4% reported having no knowledge. The majority (81.5%) of physiotherapists surveyed, however, believed that providing weight management advice was within their scope of practice. 10 Most physiotherapists (84.6%) provided physical activity advice for weight management, but a minority only 41.5% provided dietary advice. Having received training in weight management during their professional entry level education positively correlated with providing dietary advice. The physiotherapists in this study reported barriers to providing nutrition education including, feeling that it was not part of their scope of practice, time management limitations, and not having confidence in their understanding to provide accurate advice to clients. 10
Recently Moore et al surveyed current physical therapy students and new graduates in the United States on attitudes and beliefs of nutrition. Of the 151 respondents, 19.2% of total respondents agreed or strongly agreed with feeling comfortable counseling clients and only 2.6% agreed or strongly agreed that their nutrition courses adequately provided them with the proper tools to educate clients on nutrition. Over 60%, however, agreed or strongly agreed that an introductory nutrition course should be a requirement of any Doctor of Physical Therapy education. 6
Based on the impact of poor nutrition and the discoveries in previous studies, the importance of determining physical therapists’ level of comfort and utilization of nutrition education must be further explored.
Subjects
Inclusion criteria included being a physical therapist at one of our universities’ clinical sites in the Northeast region of the United States and actively treating patients at this facility. A list of 169 clinical placement sites, in the Northeast region of the United States was obtained from the Director of Clinical Education (DCE) at the investigators’ university. This population was selected as a convenience sample and to inform the investigators on the type and amount of nutrition education that physical therapists practicing at our clinical placement cites were giving to their patients.
Methods
Instruments and Procedures
A 28-question survey was designed, using Google Forms, by the team of investigators including a registered dietitian, a physical therapist with cardiovascular and pulmonary board certification and three physical therapy doctorate students. Upon completion, the survey was reviewed by an external expert and modifications were made based on feedback. This survey consisted of two portions and was designed to take participants 5-10 min to complete. The first portion contained questions about demographic information and education of the survey responder including practice setting, years of experience, hours per week of direct patient contact, number of nutrition courses taken in their physical therapy curriculum as well as continued education and if they felt nutrition was covered sufficiently during their education to properly educate patients in practice. The second portion contained Likert-style questions about level of comfort and how often they used topics of nutrition in practice. The content of the survey was created based on expert knowledge, APTA statements related to nutrition as well as published literature on the role of physical therapists in nutrition education and CAPTE guidelines.1,3,13,17,29,61 Given the overwhelming nature of content related to nutrition, the authors chose to focus on overall comfort with nutrition education, referrals to an appropriate provider and topics related to obesity and weight loss, cardiovascular and renal health. These areas were chosen secondary to the obesity epidemic in this country as well as the overwhelming impact of diabetes and cardiovascular disease on patients and medical system.2,3,26-29,33-40 Topics of the survey included weight loss, healthy food choices, caloric intake, hydration, diet modifications for heart and kidney disease, referring to a registered dietitian, and measuring BMI and body composition. Respondents were also asked how prepared they felt discussing nutrition related topics overall, if they believed nutrition education should be a part of a patient’s overarching wellness plan, how comfortable they were if a patient asks for advice on nutrition and how often this occurs. Application for exemption from federal regulation was submitted and approved (#05221) prior to initiation of the study.
This survey was distributed by emails sent to the clinical site coordinator at 169 locations. The clinical site coordinator was asked to share this survey with all licensed physical therapists actively treating patients at their facility. Two weeks after the initial e-mail, another email was sent as a reminder. Four weeks after the initial email, a final reminder was sent out via email. The data gathered from the survey remained anonymous.
As compensation for taking their time to complete the survey, a pre-recorded webinar was created by a registered dietitian regarding pertinent information on nutrition discussed in the survey questions. Facilities gave their name in the final question of the survey if they wanted to receive this compensation. One examiner collected all the initial survey results, maintained a list of those respondents who opted in to receive the in-service and immediately removed this information from the survey results prior to any analysis. The in-service was available via pre-recorded lecture link.
Data Analysis
Descriptive statistics were performed including frequencies and percentages for qualitative variables and means and standard deviation for quantitative variables for all survey questions. For Likert-style questions, summary scores for level of comfort and frequency of providing nutrition education were calculated for each participant. These scores were derived by summing the 10 respective items for each. Both scores demonstrated good reliability (Cronbach’s alpha of .79 for frequency and .83 for comfortable). An ANOVA with post-hoc paired comparisons was used to compare qualitative demographic variables and the two summary scores, and the nonparametric Spearman correlation was used to test for a relationship between the quantitative demographic variables and the two summary scores. Power analysis was calculated based on obtaining a sample size of 100. For ANOVA assuming a four-level grouping variable and an alpha level of .05 there was sufficient power (80%) to detect a medium/large effect size (Cohen’s f = .33) and for correlation power was 80% to detect a medium size effect (r = .28). Analyses were conducted using SPSS v27 and statistical significance was set at an alpha level of .05.
Results
Demographic Characteristics of Respondents (N = 125).
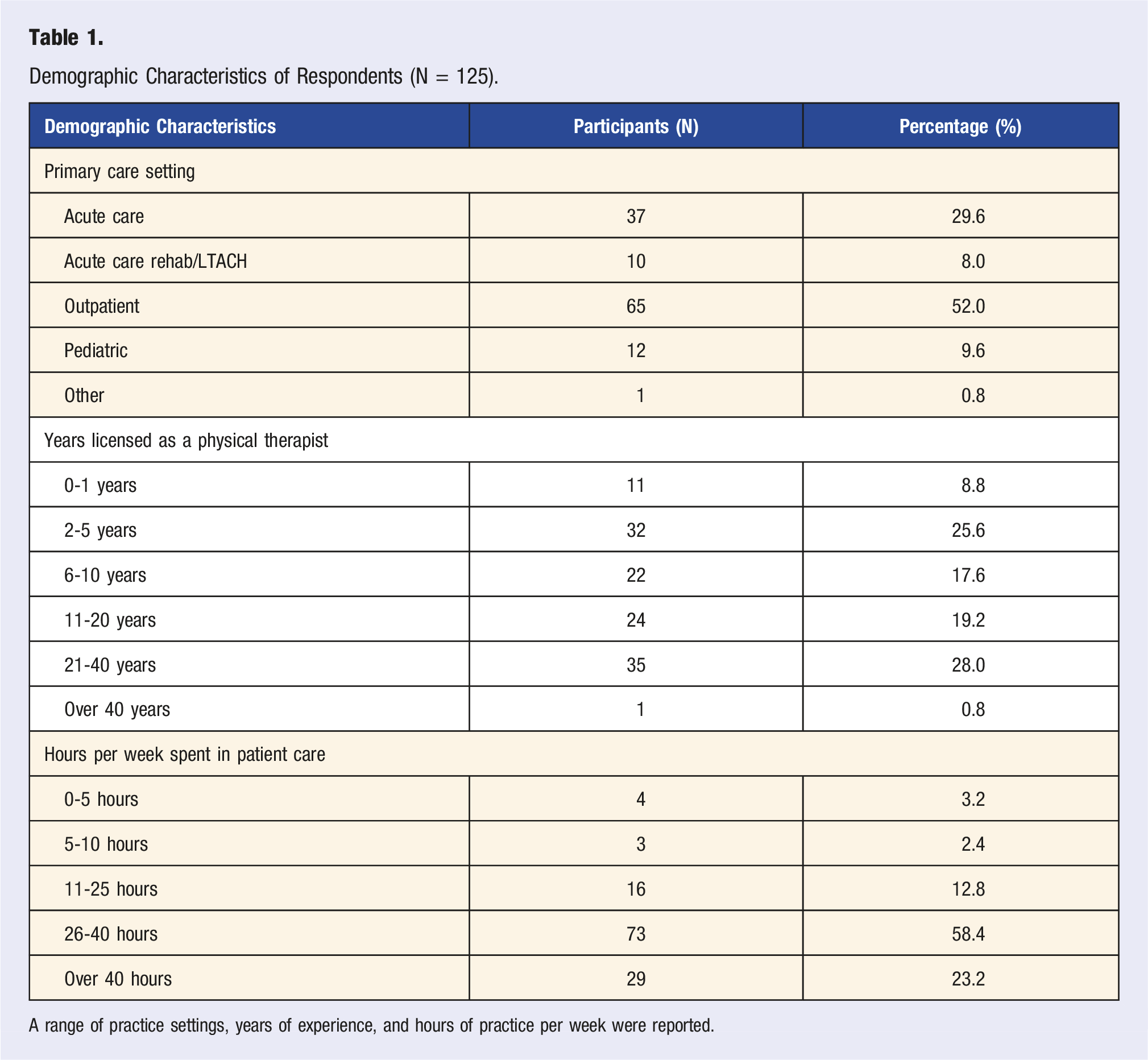
A range of practice settings, years of experience, and hours of practice per week were reported.
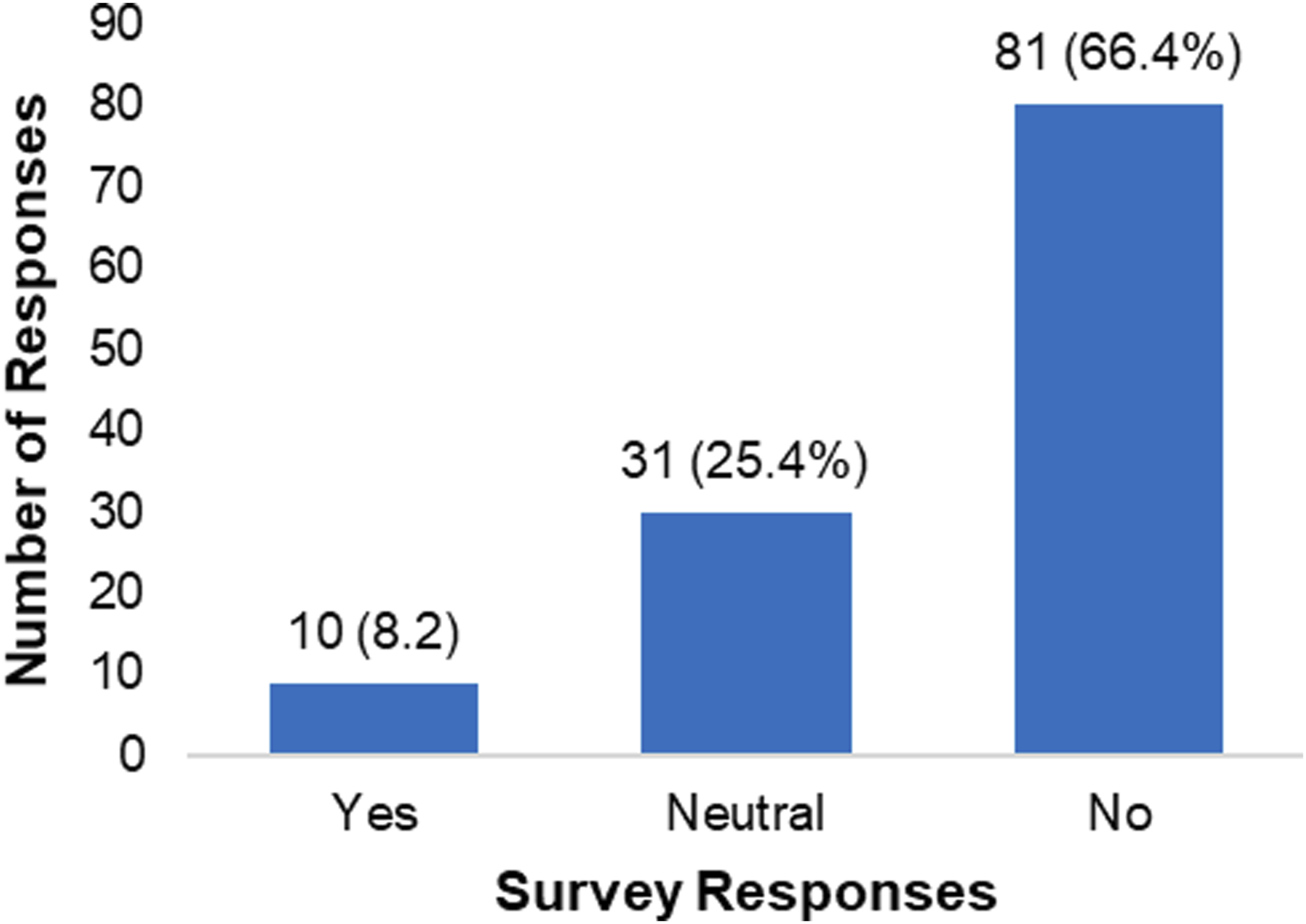
Was the subject of nutrition covered sufficiently during your education to properly educate your patients?
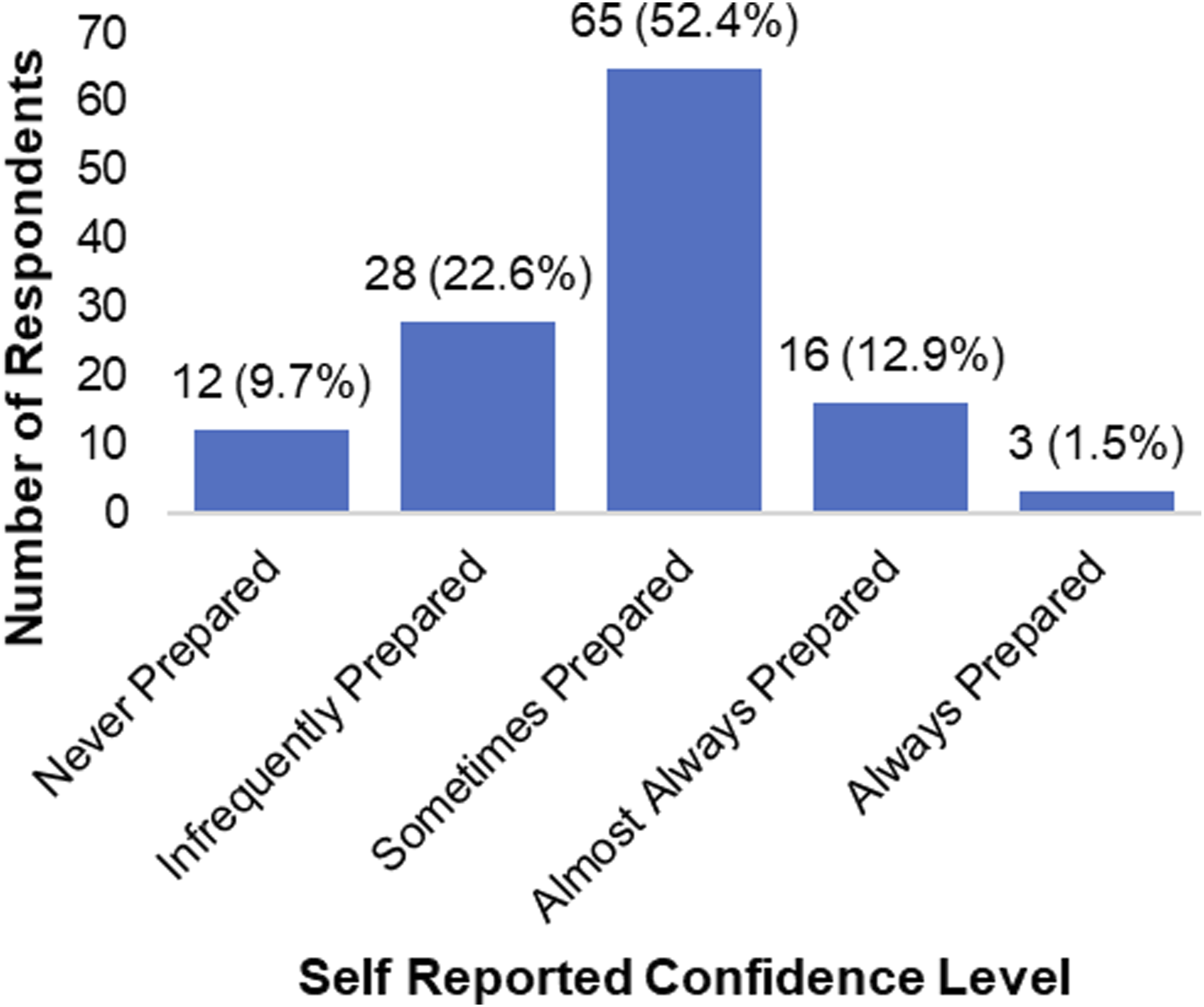
How prepared to you feel you are to discuss nutrition related topics with your patients?
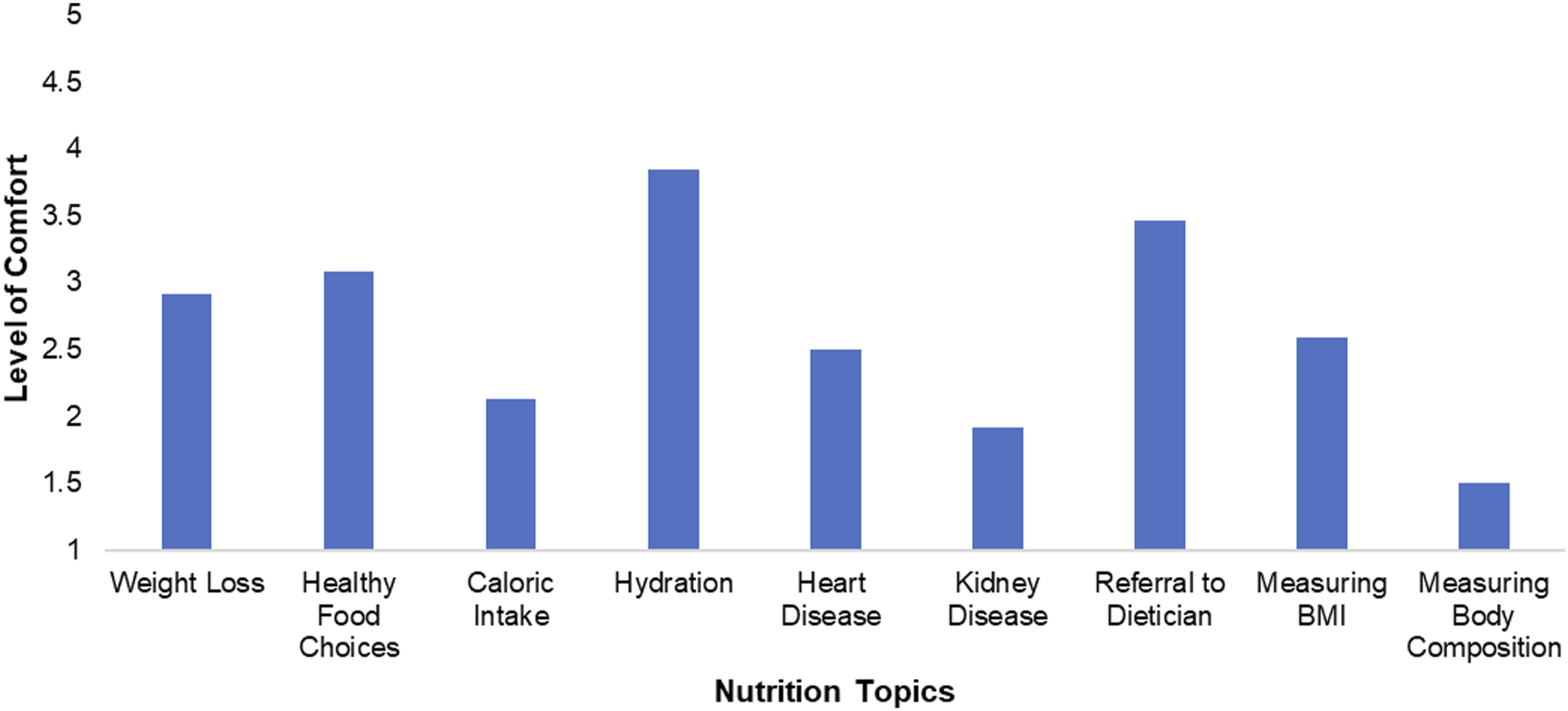
Average level of comfort on nutrition related topics, 1(Never comfortable), 2 (Uncomfortable in most situations), 3 (Comfortable in some situations), 4 (Comfortable in almost all situations), 5 (Comfortable in every situation).
Analyzing specific individual survey questions revealed there was a significant positive correlation between the number of nutrition courses taken during their physical therapy education and comfort when asked by a patient for nutrition advice (rho = .29, P = .001), comfort in assessing body composition (rho = .25, P = .006) and in how prepared they felt overall when discussing nutrition related topics (rho = .25, P = .005). There were significant correlations between the number of nutrition related continuing education courses taken and how often physical therapists educated patients on weight loss (rho = .26, P = .004,) and making healthy food choices (rho = .29, P = .001,) as well as how often patients ask them for advice on nutrition (rho = .25, P = .005). There was also a correlation between physical therapists who believed that the subject of nutrition was covered sufficiently during their PT education and feeling more prepared when discussing nutrition related topics with their patients (P = .003,) as well as feeling more comfortable if asked for advice on nutrition by patients. (P = .003). The number of years that physical therapists were licensed for was significantly correlated with their comfort level of referring a patient to a registered dietitian (P = .029).
Correlation Between PT Characteristics, Comfort and Frequency.
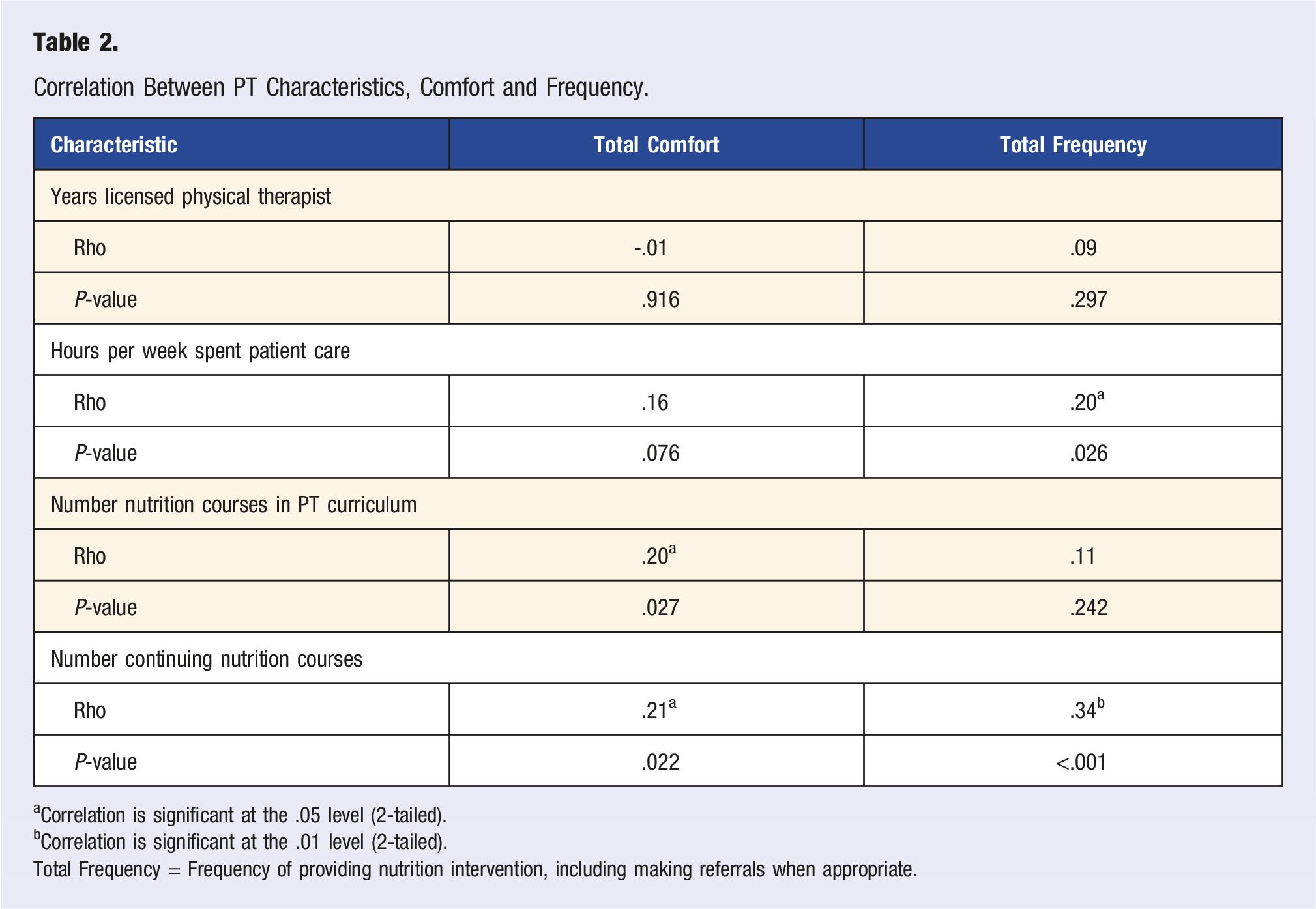
aCorrelation is significant at the .05 level (2-tailed).
bCorrelation is significant at the .01 level (2-tailed).
Total Frequency = Frequency of providing nutrition intervention, including making referrals when appropriate.
Discussion and Conclusion
The purpose of this study was to examine physical therapist’s education and comfort discussing nutrition related topics as well as frequency of nutrition education given to patients in the Northeast region of the United States. It was hypothesized that there would be a reported lack of comfort, and that nutrition education would be an underutilized resource in clinical practice. This hypothesis was supported by the results of this study.
This study illustrated the lack of comfort many physical therapists feel regarding nutrition related topics and identified the need for more curricular content related to nutrition in accredited Doctor of Physical Therapy programs. Only 8.2% of respondents felt that the topic of nutrition was adequately covered in their curriculum, signifying that most respondents did not feel adequately prepared. There are many potential reasons for these findings, including limited detail within CAPTE guidelines related to nutrition, differences in physical therapy state practice acts, and limited published expert consensus or practice guideline related to this topic. CAPTE and the APTA have released statements indicating physical therapists have a role in nutrition and wellness; however, these statements provide limited specifics. CAPTE requires that Doctor of Physical Therapy students have knowledge and learning experiences in nutrition content, and states “graduating students must be able to provide physical therapy services that address primary, secondary, and tertiary prevention, health promotion, and wellness to individuals, groups, and communities.” 6 These requirements are very broad and as an educator much is left to interpretation on how to proceed in creating specific curricular content. In 2020 a panel of 37 experts informed the development of population health, prevention, health promotion, and wellness competencies for physical therapist professional education. Twenty-five competencies achieved final consensus in 3 broad domains: preventive services and health promotion, foundations of population health, and health systems and policy. The recommended competencies are helpful in highlighting the importance of health promotion and wellness, heath disparities awareness, and community screening and resources. Only one of the competencies, however, directly mentions nutrition. This states, “communicate nutritional recommendations set forth by state, national, and international agencies as a means of promoting healthy eating pattern.” 62 The uncertainty is further confounded by variation in physical therapy state practice acts which outline the physical therapy scope of practice in each state.
This study identified that most physical therapists believed nutrition education should be a part of their patient’s overarching wellness plan but felt a lack of comfort in discussing nutrition topics with their patients. The majority of respondents (84.7%) felt either sometimes, infrequently, or never prepared to discuss nutrition with patients. Respondents reported being uncomfortable in most situations discussing caloric intake, food intake related to kidney disease and assessing body composition. Participants were uncomfortable in most situations to comfortable in some situations when discussing nutrition related to heart disease, weight loss, and measuring BMI.
This lack of confidence leaves a gap in physical therapists’ ability to provide optimal care to our society. Promoting good nutrition habits reduces the risk of obesity, hypertension, stroke, cardiac and renal disease.37-40,42-52 Each of these conditions negatively impacts a patient’s function and quality of life. 63 A multidisciplinary approach including exercise and dietary changes has been shown to positively impact obesity status, body composition, and cardiometabolic risk markers. 63,64 Additionally, nutrition can play a key role in muscle strength, healing and reducing inflammation.3-8,65-72 These are all associated factors of reasons that individuals may receive PT services. With greater knowledge and confidence on the topic of nutrition, physical therapists would likely provide more patient education and facilitate better long-term health outcomes for their patients.
This study further supports and expands upon previous studies related to physical therapy and nutrition patient education. The topic of physical therapists’ comfort and frequency of providing nutrition education has recently grown as a research topic, but remains limited. A study published by Moore et al examined attitudes and beliefs of nutrition in current Doctor of Physical Therapy students and new graduates. Moore et al 6 found only 2.6% of respondents agreed or strongly agreed that their nutrition courses adequately provided them with the proper tools to educate clients on nutrition and 19.2% of total respondents agreed or strongly agreed with feeling comfortable counseling clients. 6 Another study by Zollinger and Katuli, examined knowledge, attitude, and practice of lifestyle screening and education in orthopedic manual physical therapists. Respondents in this study rated their diet and nutrition education on a 1-5 point scale, where 1 represented “Not Covered” and 5 represented “Well Covered” for PT school and post-PT school education. The findings showed that 84.9% reported a rating of 3 or below for PT school education, and 65% rated 3 or below for post-PT school education. The researchers also discovered that 53.9% of participants reported talking to their patients about diet some, a little, or never, while 46.1% indicated moderate or frequent engagement. 73 A survey of Australian practicing physiotherapists examined whether therapists were providing nutrition education and if so, what content was included. Of the physiotherapists surveyed, only 41.5% provided dietary advice and they admitted that one of the barriers they faced was not having the confidence in their understanding to provide accurate advice to clients. 10 The data from our study further supports the data from these studies, as most of our respondents felt that nutrition advice should be a part of the patient’s overarching wellness care, but the majority do not frequently give, nor feel confident in giving, such advice.
The amount of nutrition education a physical therapist received was shown to be beneficial in providing care. The mean reported number of nutrition courses taken during physical therapy curriculum was .8 ± 1.0, and 46% percent of participants reporting taking 0 nutrition courses. Admittedly, the number of courses is only one measure and content may be distributed across many classes within the physical therapy curriculum. However, individuals who reported taking more courses during their curriculum reported being more comfortable when asked for advice by patients and in discussing nutrition related topics overall. The mean reported number of continued education courses taken related to nutrition was .6 ± 1.0 and 62% of participants reported taking 0 continued education courses related to nutrition. Those who reported taking more continued education courses felt more comfortable overall with nutrition topics and had a higher total frequency of discussing these topics with patients. Participants who thought nutrition was covered sufficiently in PT curriculum had the highest comfort level mean score, and they differed from those who responded that nutrition in PT curriculum was not sufficiently covered. Given these reported findings it would be beneficial for programs to enhance curriculum related to nutrition moving forward.
Interesting findings were seen related to referrals to a registered dietitian. Although 48.8% of respondents reported being comfortable making referrals most or all the time, only 16.2% reported making these referrals frequently or all the time when it was appropriate. Our data also showed a correlation between the number of years a physical therapist had practiced and their comfort level with making referrals to registered dietitians. Future research should survey practicing physical therapists more specifically about their referral patterns, how often they refer to registered dietitians and what barriers exist to doing this. By addressing a patients’ health and wellness from multiple professional angles, referrals to registered dietitians help patients in need of a proper nutrition evaluation reach their rehabilitation goals. Further review of this topic could additionally shed light on an issue with interprofessional collaboration within the physical therapy profession.
One limitation of our study was that the samples of participants were specific to one university’s clinical partners and were all from the Northeast region of the United States. It is anticipated that similar findings would be reported throughout the country, but this needs to be further examined. Additionally, this survey gathered preliminary data on overall comfort and frequency of nutrition education with a focus on weight management, cardiovascular and renal health. More research is needed to assess the breadth and depth of nutrition education being given by PTs for multiple body systems and pathologies. Another limitation was that the number of courses taken was examined, but the specific content of nutrition courses was not evaluated. This was done in an effort to collect preliminary data and to increase the ease of survey completion. Future research should further examine how nutrition education is delivered and nutrition content included in physical therapy curriculum across the nation and compare patient outcomes when nutrition education is given vs when it is not.
Our study’s findings were significant due to the benefits that nutrition provides for optimizing a patient's rehabilitation. Unfortunately, many of the physical therapists surveyed felt they either had limitations in knowledge or were uncomfortable talking about the topic of nutrition. Clinicians such as physical therapists have an obligation to provide education to their patients and deficiency on this topic may limit progress and ability to achieve rehabilitation goals.
Practicing physical therapists often believe nutrition is important to their patients’ recovery, but report feeling they lack sufficient education to provide this. Our data suggests that nutrition is not sufficiently covered in physical therapy education, despite clinicians believing it should be part of wellness care. Further research should be done to determine the extent and content of nutrition education in Physical Therapy curricula across the United States.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.