
Abstract
Across the US, chronic illnesses, including cancer and cardiovascular disease, largely result from poor lifestyle decisions such as diet, tobacco/alcohol use, and physical inactivity. Medical students' healthy lifestyle habits drastically decline during medical school, which can result in severe medical conditions, future poor patient outcomes, and burnout. However, little evidence exists on what perceived barriers medical students hold on lifestyle behaviors or how well they understand the relationship between specific lifestyle behaviors and their impact on health. This study included data from a self-selected sample of 127 medical students aged 22-41 years. Measures included the perceived health impact of 14 different lifestyle and dietary behaviors, self-reported barriers to lifestyle behaviors, and basic demographic questions. Results showed an average correlation of −.004 between participants' perceived impact and the actual impact of the behaviors on health (SD = .25; CI = −.047 - .039). Results also identified perceived barriers across behaviors that impact health. Data suggests that medical students have insufficient knowledge of the impact of lifestyle behaviors on health. Interventions targeting a medical student population should include information on how to overcome perceived barriers and the impact of lifestyle behaviors on health. Incorporating such information will bolster future interventions' effectiveness.
“Understanding the perceived barriers to healthier lifestyle behaviors among medical students is essential for designing effective health promotion strategies.”
Introduction
An unhealthy lifestyle, including physical inactivity, tobacco use, and poor diet, is a leading cause of morbidity and mortality (e.g., cancer and heart disease). 1 Studies have shown that these lifestyle behaviors contribute to 60% of premature deaths and lead to 10 years longer life expectancy free of major chronic diseases. 2 These factors are modifiable, yet less than 2.7% of Americans engage in a healthy lifestyle. 3 One approach to reducing the number of deaths caused by chronic health conditions is to promote a healthier lifestyle, particularly in primary care settings.
While the data on the relationship between lifestyle decisions and chronic illnesses is well documented, the efforts made by the medical community can be improved to address patients’ lifestyles. 4 With the potential advantages of lives saved, increased quality of life, and significant economic advantages for the health care system, it would be beneficial if more physicians incorporated lifestyle medicine into their daily patient care. One reason more physicians do not do so may be because they are uninformed. Only 27% of medical schools in the U.S. provide a minimum of 25 hours of nutritional teaching.5,6 Primary care residency programs teach an average of only 2.8 hours on how to counsel patients on obesity, nutrition, and physical activity. 7 If medical students lack knowledge of the impact of lifestyle behaviors on health, this suggests medical students would be unprepared to have productive conversations with their future patients concerning preventative behaviors. A lack of knowledge could also contribute to a medical student's unhealthy lifestyle. Evidence is required to reveal how knowledgeable medical students are concerning preventative behaviors.
Poor lifestyle behaviors among medical students are concerning not only for their own health but also for their future patients. Health coaching from medical professionals can improve the health outcomes of patients. 8 Doctors' habits, views, and strategies for a healthy lifestyle are all predictors of how they communicate lifestyle decisions with their patients.9,10 If medical students carry their bad habits throughout their careers, their patients are less likely to engage in preventative behaviors. For example, evidence suggests that a lack of education in medical school makes physicians ill-equipped to support patients with obesity. 11
While it would be exceedingly valuable for medical students to have an accurate understanding of the impact of lifestyle behaviors, little evidence is available as to whether medical students are informed. Medical students' understanding of the impact of specific lifestyle behaviors on health is important since this knowledge will impact how prevention behaviors will be communicated with their future patients. 8 Identifying what information needs to be presented will help inform future intervention content, thereby strengthening the likelihood of its effectiveness.
Research Aims and Questions
The aim of this study was two-fold. First, it was designed to measure how calibrated medical students are regarding lifestyle behaviors and their impact on morbidity and mortality. To the extent students are calibrated on the impact of lifestyle behaviors, they are more equipped to make decisions aligned with their goals and values. Second, this study was designed to identify perceived challenges associated with engaging in lifestyle behaviors that are key for health. An intervention designed to increase informed decision-making regarding preventative behaviors would have greater success if it were to address the perceived challenges.
Methods
Participants and Procedure
The study period was March 2021. Responses from participants at all stages of medical school were included. All medical students at one Midwestern university were contacted to participate in the study. Participants were invited through email to complete an online survey. One hundred and twenty-seven participants were collected. Participants needed to be 18 years of age or older. The study featured a self-report online questionnaire that included questions with a Likert scale and open-ended response options. Ethical approval for the study was obtained from Michigan State University in February 2021. Participation was entirely voluntary.
Materials
Qualitative and quantitative data were collected to identify students’ calibration on lifestyle behavior impact and to identify perceived barriers that limit students from engaging in healthy behaviors. A questionnaire was developed to measure calibration, which consisted of 14 items. Fourteen (no influence 0–10 very high influence) Likert scale survey items were asked to measure the perceived impact of key lifestyle behaviors on morbidity and mortality. See the example items below.
For the US population, how much do each of the following behaviors influence health (morbidity/mortality) on a 0–10 scale, 0 being no influence and 10 being very high
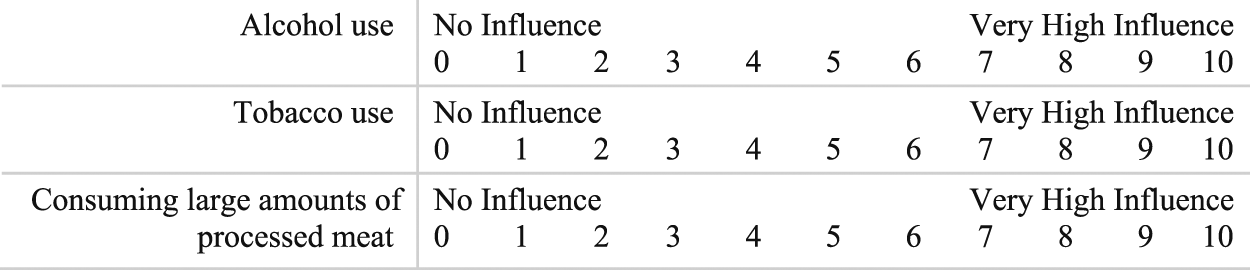
Following these questions, 14 open-ended questions were asked. For example, “List the challenges you have to consuming more vegetables:” or “List the challenges you have to engaging in more physical activity:” Qualitative data was collected to identify the most common perceived barriers to healthier lifestyle behaviors. Two independent coders analyzed the qualitative data, grouping responses similar in intent but disparate in phrasing. After initial independent analysis, coding was reviewed and discussed between researchers. Minor discrepancies were resolved. A third coder was available but unnecessary since there were no disputes over groupings.
Finally, basic demographic questions were asked, including age, sex, and race. See supplemental materials1 for the full list of survey items.
Statistical Analyses
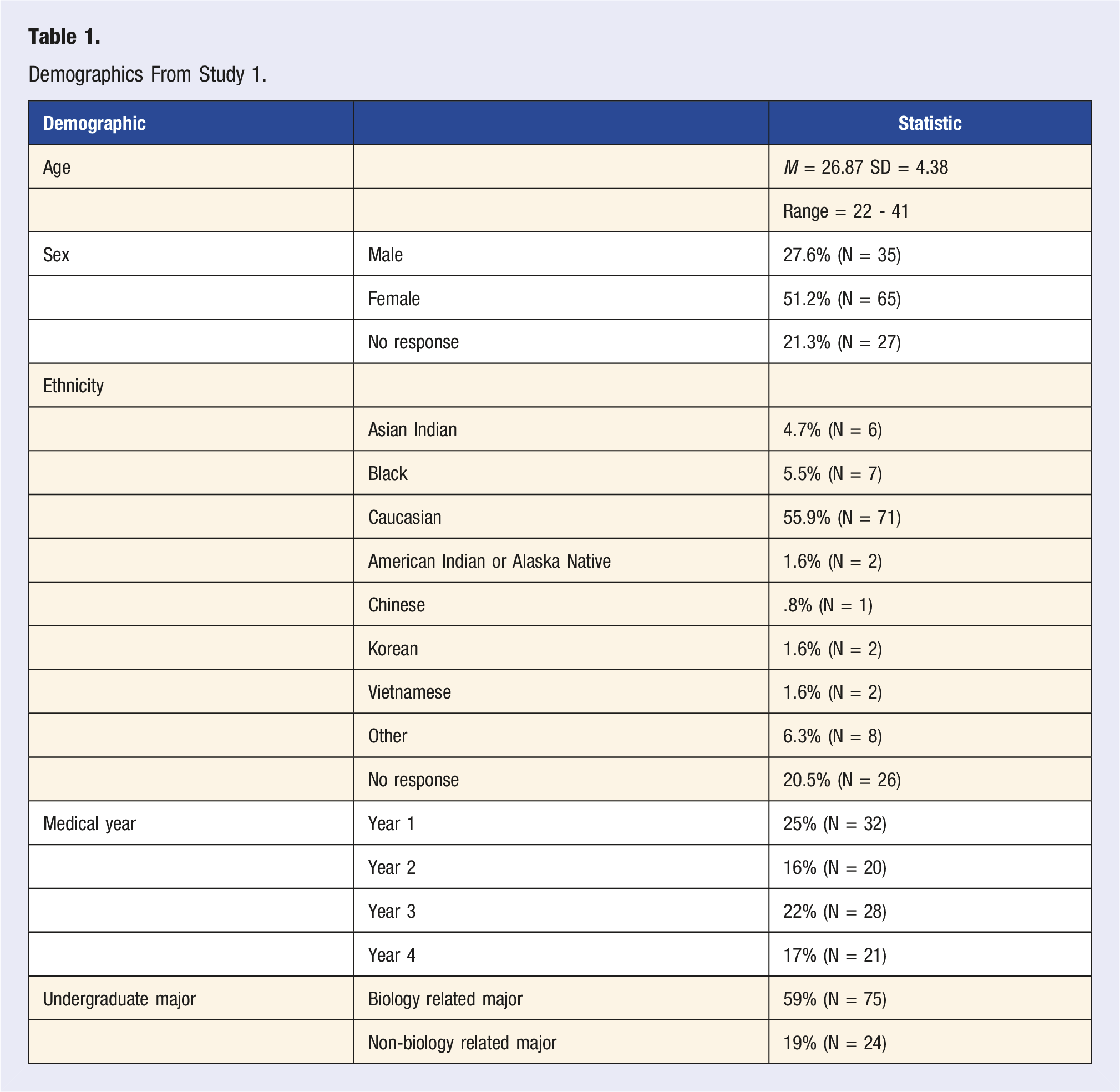
Descriptive statistics were performed with means and frequencies. Demographics are presented as percentages for categorical variables and a mean and standard deviation for the continuous variable. To test whether medical students are calibrated on the impact of lifestyle behaviors on health, Spearman Rho correlations were performed between each participant's ranking and the true impact ranking. The true impact rankings are based on the values provided by the Global Burden of Disease data and rescaled to have a minimum and maximum of 0-10. 12 A min-max scaling was used to rescale the continuous vector (i.e., GBD metric number) to the specified min-max by linearly transforming the data to fit within the desired range (i.e., 0-10). The scales package in R was used to rescale the values. 13 Two independent t-tests were performed to test whether accuracy ratings were impacted by sex or undergraduate major. A Pearson product-moment correlation was used to test whether there was a relationship between age and accuracy ratings. Finally, a one-way Anova was used to test whether the number of years in medical school impacted accuracy ratings. All analyses were conducted through RStudio. 14
Results
Demographics From Study 1.
Calibration
Results showed an average correlation of Violin plot of the medical student sample correlations. Boxplot is included in the plot. The dot is the mean, and the bars report the 95% Confidence Intervals.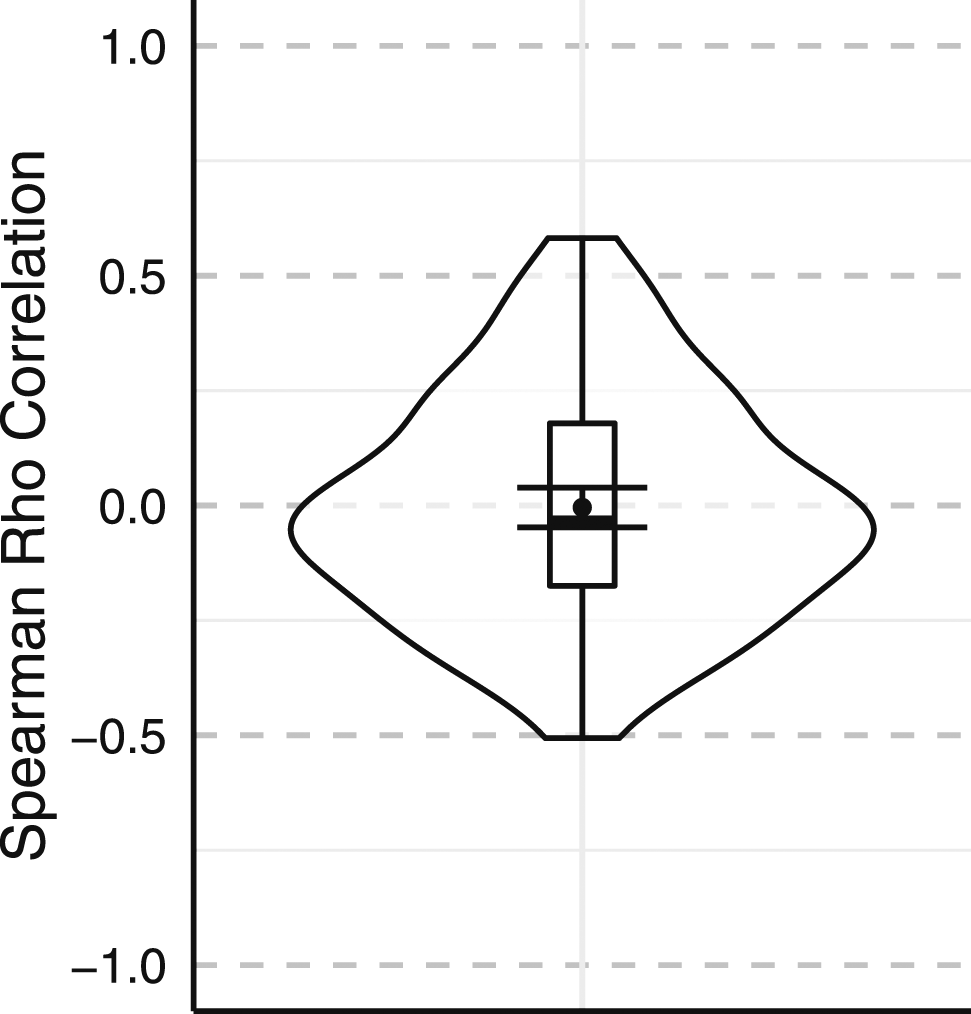
A series of analyses were performed to determine if demographic variables significantly predicted accuracy ratings. There was no significant effect for sex, t(65) =
Barrier Identification
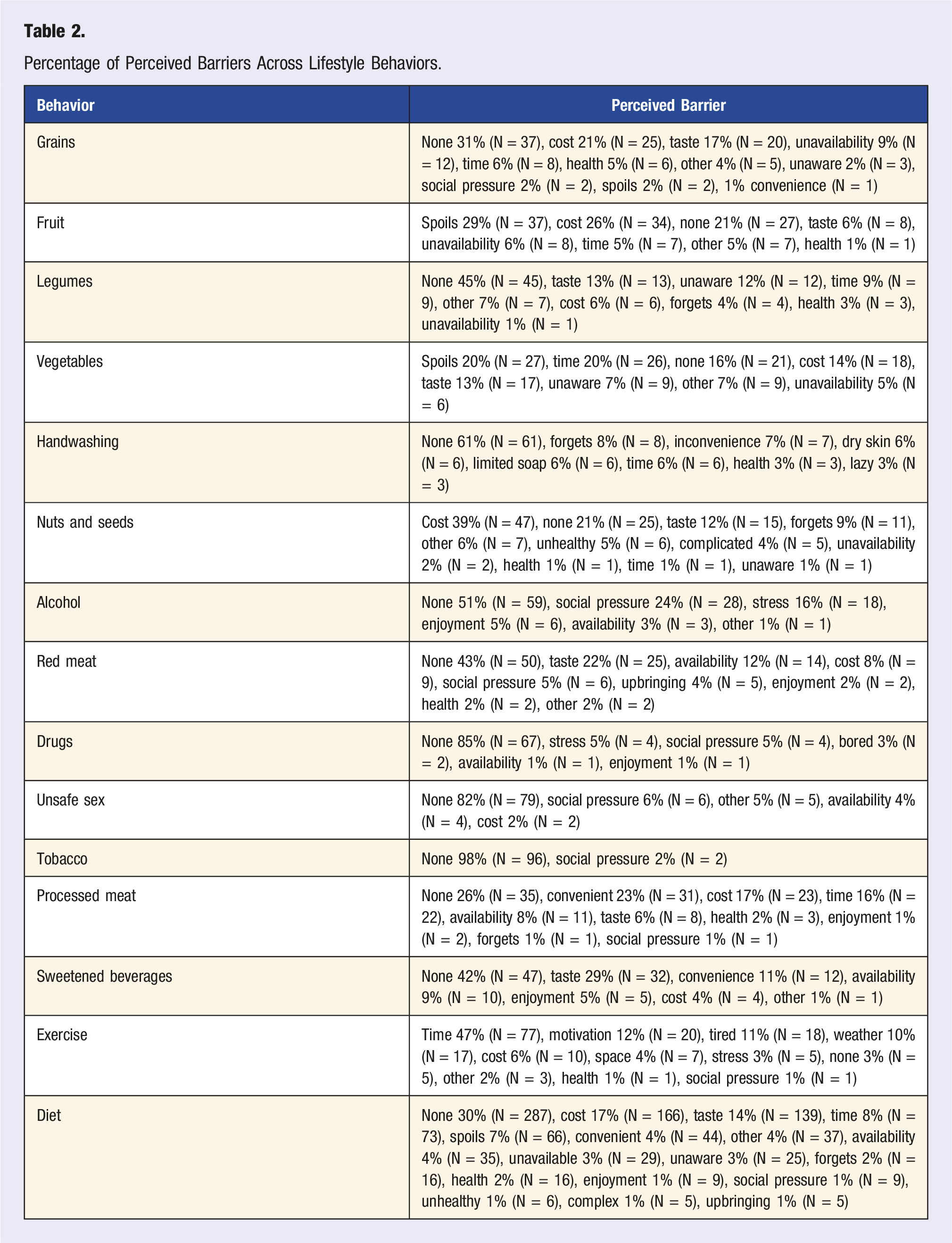
Percentage of Perceived Barriers Across Lifestyle Behaviors.
Discussion
The purpose of this study was (1) to assess how calibrated medical students are on the relationship between lifestyle behaviors and health and (2) to identify perceived barriers to key lifestyle behaviors. The data collected here suggests that medical students do not understand the relative impact of lifestyle behaviors on health. Participants did not rate the importance of behavior on health in-line with current epidemiological evidence. In addition, qualitative data identified perceived barriers for 14 different behaviors. The data collected provides valuable insights into the perceived barriers across various behaviors, shedding light on the factors influencing medical students' choices regarding their diet and other lifestyle habits.
The evidence collected in this study suggests that medical students need more knowledge for future conversations with their patients about preventative behaviors. Since this evidence suggests medical students are uncalibrated as to the impact of lifestyle behaviors on health, they may be less motivated to have preventative behavior conversations with their patients or provide information that causes valuable resources from the patient (e.g., time and energy) to be placed on less impactful behaviors. For example, physicians may emphasize the need for patients to exercise rather than diet, even though diet is a larger determinant of health. 12
The present data suggests medical students hold insufficient knowledge regarding the impact of different lifestyle behaviors on health. This means that medical students are not equipped to make decisions about their limited resources (e.g., time, energy, and money) in-line with their health goals. For example, medical students could spend more money on vegetables and fruit and neglect whole grains even though whole grain consumption has a larger impact on health. 12 An accurate understanding of disease impact is essential for making preventative behavior decisions. 15 Increasing knowledge on the impact of lifestyle behaviors would likely influence motivation to change behavior and help medical students and their future patients make decisions with limited and valuable resources more aligned with their goals and values.
Representative understanding or comprehension is also fundamental for making decisions about engaging in prevention practices. 16 Comprehension not only directly influences the capability of engaging in the appropriate behavior but also influences autonomous motivation to engage in the behavior. 17 Results in the present study can be used to inform the content of future lifestyle interventions, thereby increasing their informed decision-making. Increasing how informed medical students are on the relationship between lifestyle behaviors and health and how to overcome perceived challenges associated with behavior change makes it more likely that medical students and their future patients will make better health decisions.
Several themes could be identified across the barriers reported by the medical students. One prominent theme that emerged across multiple behaviors was the issue of cost. Participants reported financial constraints as a significant barrier to adopting healthier habits. The prevalence of cost-related concerns highlights the need for targeted interventions and support systems to address financial barriers and provide more affordable healthy options for medical students. Interestingly, many participants across various behaviors mentioned “None” for not engaging in healthier lifestyles. This finding suggests that many medical students may not perceive any obstacles hindering their adoption of healthier behaviors. While this lack of perceived barriers is encouraging, it warrants further investigation into what other factors may impact lifestyle behaviors. Taste emerged as a significant barrier to adopting healthier diets. This indicates that students' taste preferences shape their food choices.
Moreover, time constraints were frequently cited as a significant barrier, reflecting medical students' challenges in allocating time for physical activity and maintaining a balanced diet amidst their rigorous academic schedules. Social pressures were mentioned as barriers to alcohol, red meat, drugs, and unsafe sex. This finding underscores the importance of understanding the impact of peer and societal norms on medical students' lifestyle decisions. Addressing these social influences through targeted interventions and educational programs may help promote healthier choices among the student population. The survey identified a need for awareness as a barrier for legumes nuts, and seeds. Providing students with nutritional knowledge and information about healthier options may positively influence these dietary choices. Additionally, the availability of healthier food options was cited as a barrier in various categories, indicating the importance of ensuring easy access to nutritious foods on campus and in surrounding areas.
Understanding the perceived barriers to healthier lifestyle behaviors among medical students is essential for designing effective health promotion strategies. Interventions to improve access to affordable and nutritious foods, address taste preferences, manage time constraints, and reduce social pressures can encourage students to adopt healthier habits. Furthermore, educational initiatives focused on nutritional awareness and the benefits of healthy behaviors may empower students to make informed choices.
There are several limitations to the present study. First, the study only recruited participants from a Midwestern university. Medical students at other locations may have unique challenges to a healthier lifestyle that are not captured by the current sample. This data represents information regarding only one medical school. While evidence suggests that medical schools do not engage in a sufficient amount of lifestyle education, other universities may be informing their students to a larger degree. Therefore, this limits the generalizability of the results, particularly outside of the US. Data was collected through a respondent-driven sampling method and, therefore, may miss medical students who were unwilling or unable to respond to the survey. These students could have unique challenges that are not captured in the present study. The items were not tested for validity and it is unclear whether participants understood one of the items in the calibration questions (i.e., drugs). Some participants may have misinterpreted this item and thought of prescription drugs. Therefore, this item could, in part, skew the results. However, despite these limitations, this study provides a foundation for future research on further samples and demographic groups.
Conclusion
This study suggests that medical students lack sufficient knowledge of the relationship between specific lifestyle behaviors and health. This study also identified many barriers specific to each major lifestyle behavior impacting health. Results from this study can be used to inform future intervention development and medical student curriculum content. Incorporating such information will increase the likelihood of changing medical student behavior and make them more prepared to address patient needs.
Supplemental Material
Supplemental Material - Knowledge and Barriers to a Healthy Lifestyle in Medical Students
Supplemental Material for Knowledge and Barriers to a Healthy Lifestyle in Medical Students by Brittany Nelson, Erich Petushek, and Sarah Teising in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
Ms. Ann-Inger Mortvedt for her thoughtful review of the paper.
Author Contributions
BN conducted the analysis and reporting and was involved in all paper components. EP conceived the idea, directed the research, and was involved in all paper components. ST collected and analyzed data. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Cohodas Fellowsh.
Ethical Statement
Data Availability Statement
All data generated or analyzed during this study is available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.