
Abstract
Plant-based diets may positively impact body composition and cardiometabolic risk factors. An online 8-week plant-based dietary and lifestyle worksite intervention was implemented in spring 2021 among staff (n = 52) at a public university in the southwestern United States. Participants attended weekly online small group counseling sessions and healthy living workshops with cooking classes. All measures and fasting blood draws were completed at baseline and 8-week post-intervention with changes analyzed using paired sample t-tests. Multiple linear regressions examined associations among knowledge gained and online attendance with outcomes. Results from paired sample t-tests indicated numerous statistically significant improvements from baseline to 8-week post-intervention: total cholesterol (mg/dL) (MBL = 193 ± 39, MPI = 176 ± 36), low-density lipoprotein cholesterol (LDL-C) (mg/dL) (MBL = 110 ± 33, MPI = 98 ± 30), body mass index (BMI) (kg/m2) (MBL = 26.3 ± 6.3, MPI = 25.9 ± 6.1), fat mass (lb) (MBL = 62.0 ± 29.4, MPI = 60.3 ± 28.4), fat-free mass (lb) (MBL = 104.1 ± 29.4, MPI = 102.4 ± 19.6), phase angle (MBL = 5.1 ± .6, MPI = 5.0 ± .6), and diet quality (MBL = 62.4 ± 12.5, MPI = 75.2 ± 10.3). High-density lipoprotein cholestero l(HDL-C) decreased significantly (MBL = 65 ± 18, MPI = 61 ± 18). Knowledge negatively predicted LDL-C (B = −.226, P = .048) and positively predicted diet quality (B = .155, P = .021). Attendance at group sessions positively predicted phase angle (B = .055, P = .038). Findings demonstrate how a plant-based lifestyle can improve cardiometabolic health by reducing risk factors for chronic disease and enhancing body composition. Clinicians can support patients by encouraging plant-based diets.
Plant-based diets focusing on nutrient-dense whole foods can lead to improved diet quality because they emphasize the consumption of fruits, vegetables, nuts, legumes, and whole grains.
Introduction
Preventable chronic health conditions kill 41 million people globally each year, totaling 71% of all deaths. 1 In the United States (U.S.), chronic health conditions account for 85% of healthcare spending 2 with more than half of all U.S. adults having at least one chronic health condition. 3 Cardiometabolic risk factors associated with chronic health conditions (e.g., cardiovascular disease (CVD), type 2 diabetes mellitus, and hypertension) 4 include abdominal adiposity, elevated high-sensitivity C-reactive protein (hsCRP), and dyslipidemia. 5 Collectively, the clustering of these diseases and risk factors can result in a shortened lifespan.5,6
Consumption of a plant-based diet has been shown to reduce several metabolic risk factors associated with preventable chronic conditions. A meta-analysis of 40 observational studies evaluating cardiometabolic outcomes indicated that individuals following a vegan diet had significantly lower waist circumference, BMI values, fasting glucose levels, LDL-cholesterol, and triglycerides compared to those consuming an omnivorous diet. 7 These data support the growing need to encourage plant-based dietary interventions to prevent and mitigate non-communicable diseases and cardiometabolic risk factors that can lead to susceptibility to infectious diseases8,9 and shortened lifespan.
There are five geographic regions called Blue Zones where people regularly live over the age of one hundred with optimal quality of life and low incidence of chronic disease and cardiometabolic risk factors. Since lifestyle is a critical component of healthy aging, interest has grown in learning the common lifestyle trends among these populations. This led to the formation of the 9 Blue Zones principles, referred to as the Power 9®: move naturally, know your purpose, downshift (i.e., find ways to relax and unwind), eat until 80% full, consume a plant-based diet, drink red wine moderately and regularly, create a healthy social network, connect with your spirituality, and prioritize family. 10 In Okinawa, Japan, a comparison between the Okinawa population study and the Framingham Offspring Study revealed that CVD prevalence was twelve times greater in Framingham men and women than in their Okinawan counterparts. 11 Furthermore, an Okinawan centenarian biopsy found no pathological evidence of coronary heart disease and a complete absence of coronary calcification, an early indicator of arteriosclerosis. 12 The Okinawan diet comprises 90% of calories from carbohydrates in the form of vegetables, which creates a nutrient-dense diet high in vitamins, minerals, and phytonutrients.13-15
Applying the Power 9® Blue Zones principles and focusing on consuming a plant-based diet was the foundation of this virtual worksite pilot intervention study, conducted during the COVID-19 pandemic. This study promoted lifestyle and dietary changes, which employers desire because employees who adopt healthier lifestyles lower their risk of developing costly chronic diseases while improving productivity. 16 The goals of this study were to determine if knowledge of the Power 9® Blue Zones principles and a plant-based diet, attendance at weekly Zoom workshops and wellness counseling sessions, and improvements in diet quality as measured by the Healthy Eating Index-2015 (HEI-2015), are associated with changes in cardiometabolic risk factors.
Methods
Study Design
Using a pre-post experimental design, an 8-week virtual worksite pilot intervention enrolled 64 participants and comprised workshops, small group counseling sessions, and emailed newsletters/updates. Participants were employees of a mid-sized public university in the southwestern United States. Eight workshops were conducted weekly via Zoom, lasted 45 minutes, and consisted of an educational component, and an interactive cooking demonstration. Nutrition education component topics included plant-based nutritional basics and eating away-from-home, Power 9® Blue Zones Principles, cooking in a global kitchen, mental health, physical activity, and the environmental impact of a plant-based diet. Participants were informed that “plant-based” referred to primarily consuming products and foods that were plant-based (e.g., fruits, vegetables, whole grains, beans, and legumes). However, participants were not precluded from consuming dairy or meat products. For the weekly interactive cooking demonstrations, participants were encouraged to purchase ingredients in advance and cook the meal in their kitchens while following the guidance of the chef. A keynote speaker, Joel Fuhrman, MD, presented at the first and last workshop. The small group counselling sessions were conducted six times, had approximately 10 participants per group, lasted 45 minutes, and were facilitated by coaches who encouraged behavior change. The coaches were trained in motivational interviewing, a collaborative, goal-oriented communication style designed to strengthen personal motivation by eliciting a person’s reasons for change. 17 Each session centered on a discussion of a Blue Zone principle, reviewed material covered in previous workshops, and created weekly goals for the group. Eight emails were sent weekly over the course of the intervention. Each email contained a one-page handout of the featured Blue Zone principle of the week with daily life implementation strategies, plant-based recipes for breakfast, lunch, dinner, and snacks, and any questionnaire completion reminders. The intervention was conducted in Spring 2021; thus, the high prevalence of COVID-19 required participants to use a virtual platform for the weekly workshops and wellness counseling sessions. Live-streamed workshops took place over the Zoom platform in a home kitchen, with recordings available for those who could not attend or who wanted to re-watch the demonstrations.
Participants completed baseline and post-intervention measures including questionnaires, cardiometabolic assessments, anthropometrics, body composition, and 24-hour dietary recalls using ASA24, a standardized and validated dietary assessment tool developed by the National Cancer Institute that guides participants and uses probing questions to obtain greater recall accuracy (https://epi.grants.cancer.gov/asa24/). Participants completed 3 ASA24 dietary recalls the week before the first workshop (1 weekend and 2 weekday recalls) and repeated another 3 ASA24 dietary recalls immediately following the last workshop (1 weekend and 2 weekday recalls). Data from the 24-hour dietary recalls were used to generate HEI-2015 total scores, a measure of diet quality. Fasting blood draws were conducted by nursing students under the supervision of nursing professors who were registered nurses, at the worksite (i.e., university) before and after the 8-week intervention. Height and weight data were collected using the Seca® 284, a digital measuring station for height and weight with wireless transmission for transfer to the Seca® mBCA 515 for calculating Body Mass Index (BMI) (https://www.seca.com/en_ae/products/all-products/product-details/seca284dp.html). Body composition measures, including fat mass, fat-free mass, skeletal muscle mass, and phase angle, were measured using a Seca® medical Body Composition Analyzer (mBCA 515) at baseline and post-intervention. The mBCA 515 determines body composition based on the measurement of electrical characteristics of the human body over five regions, including left and right arms and legs, and the torso (https://www.seca.com/en_ee/products/all-products/product-details/seca515.html). The mBCA 515 is validated against whole-body magnetic resonance imaging (MRI) and dual X-ray absorptiometry (DXA). 18
Participants received incentives for participation in the study including a plant-based cookbook and participation points towards the university-sponsored Employee Assistance and Wellness (EAW) program, which contributed towards a yearly cash award. Participants also had a chance to win one of 3 raffle prizes upon completing the questionnaires and ASA24 dietary recalls. All study procedures were approved by the [BLINDED FOR REVIEW] Institutional Research Board.
Study Population and Recruitment
Recruitment occurred through employee listservs, employee word-of-mouth, and the university’s EAW program. Applicants completed an eligibility questionnaire to determine if they met the inclusionary criteria, which included employment at the university, being aged 18 years or older, expressing an interest in consuming a plant-based diet, and applying Power 9® Blue Zones-based principles in their everyday living. Exclusion criteria included currently consuming an exclusively plant-based diet, currently participating in a weight loss program, and/or inability to attend weekly workshop sessions virtually or watch the Zoom recordings.
Assessments
The following cardiometabolic measures were analyzed from the fasting blood samples collected at baseline and after completion of the 8-week intervention: total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), LDL/HDL ratio, very low-density lipoprotein cholesterol (VLDL-C), hsCRP, and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR). Participants’ height and weight were collected using the Seca® 284, with electronic data transferred to the Seca® mBCA 515 for determining BMI. Data collected from the Seca® medical Body Composition Analyzer (mBCA 515) included fat mass, fat-free mass, skeletal muscle mass, and phase angle, a calculation representing a mathematical relationship between resistance and reactance with higher values consistent with greater muscle mass.
The baseline questionnaire determined each participant’s wellness counseling group placement predicated on current eating patterns. The baseline and post-intervention questionnaires were used to collect self-reported demographic data including age, biological sex, gender identity, marital status, education level, race, and income. Other questions included dietary lifestyle and eating patterns, knowledge of a plant-based lifestyle and Power 9® Blue Zones principles, and health status (e.g., presence of auto-immune disease, pregnancy status, physical activity level, smoking behavior, and medical history).
The impact of the intervention was evaluated by examining the associations among knowledge of a plant-based lifestyle and Power 9® Blue Zones principles and participant attendance at weekly Zoom workshops and wellness counseling sessions with cardiometabolic risk factors and HEI-2015 total scores. Using SAS 9.4 (SAS Institute Inc), the HEI scoring macro generated HEI-2015 total scores (https://epi.grants.cancer.gov/hei/sas-code.html), which range from 0–100, with higher scores representing greater consistency with the Dietary Guidelines for Americans (https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf).
Statistical Analyses
Means and standard deviations were calculated for all continuous variables. Frequencies were determined for all categorical variables. Normality was evaluated for all continuous variables. Variables that were log transformed due to non-normal distributions included TG, VLDL-C, hsCRP, and HOMA-IR. Paired samples t-tests were conducted to determine if the intervention (i.e., gaining knowledge of Power 9® Blue Zones principles and a plant-based lifestyle paired with weekly wellness coaching) elicited differences over time for all cardiometabolic, anthropometric, body composition and diet quality outcomes. To determine if attendance at weekly workshops and small group sessions impacted changes in cardiometabolic, anthropometric, body composition and diet quality outcomes over time, multiple linear regression models were used to examine cardiometabolic, anthropometric, body composition and diet quality outcomes at 8-week, using baseline values of cardiometabolic, anthropometric, body composition and diet quality variables as covariates, and small group session attendance and workshop attendance as predictors. All analyses were conducted using IBM SPSS Statistics (Version 27).
Results
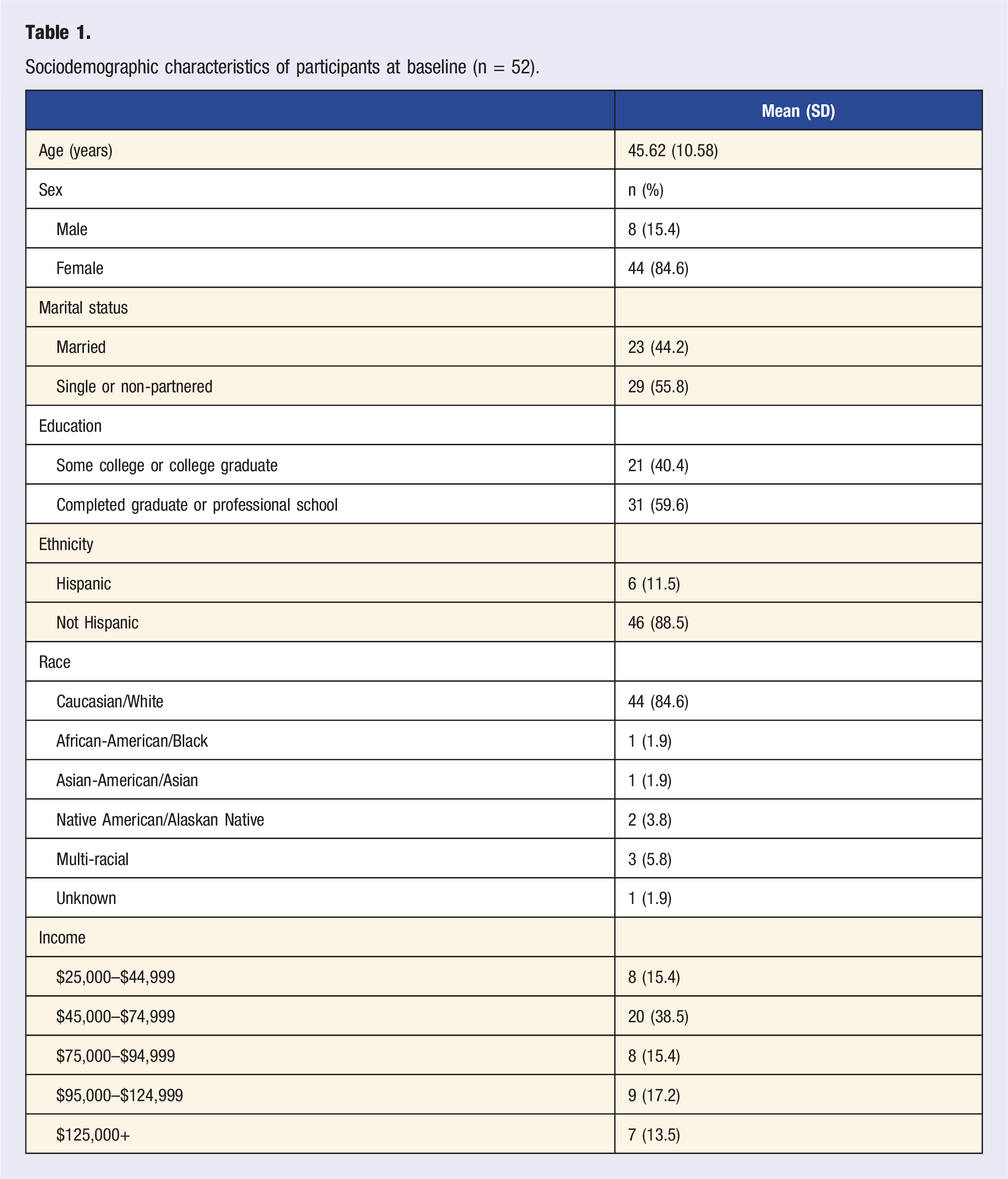
Sociodemographic characteristics of participants at baseline (n = 52).
Mean values and standard deviations (SD) of cardiometabolic variables, anthropometric and body composition measurements, and diet quality score at baseline and post-intervention (8-week) (n = 52).
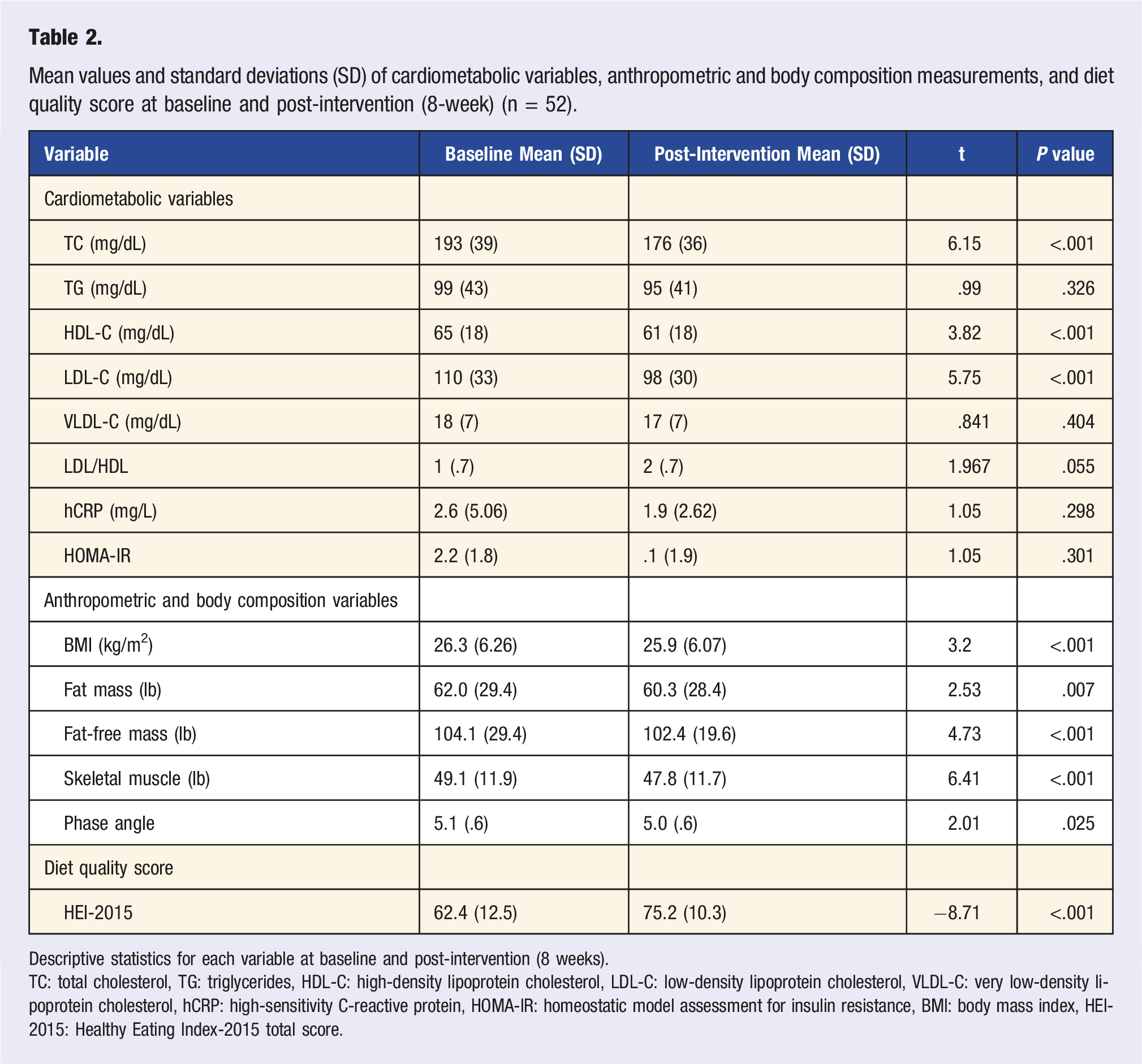
Descriptive statistics for each variable at baseline and post-intervention (8 weeks).
TC: total cholesterol, TG: triglycerides, HDL-C: high-density lipoprotein cholesterol, LDL-C: low-density lipoprotein cholesterol, VLDL-C: very low-density lipoprotein cholesterol, hCRP: high-sensitivity C-reactive protein, HOMA-IR: homeostatic model assessment for insulin resistance, BMI: body mass index, HEI-2015: Healthy Eating Index-2015 total score.
Linear regression associations among attendance at workshops, attendance in small group sessions, Blue Zones knowledge, and baseline cardiometabolic variables with cardiometabolic outcomes, body mass index (BMI), body composition, and diet quality at post-intervention (8-week) (n = 52).
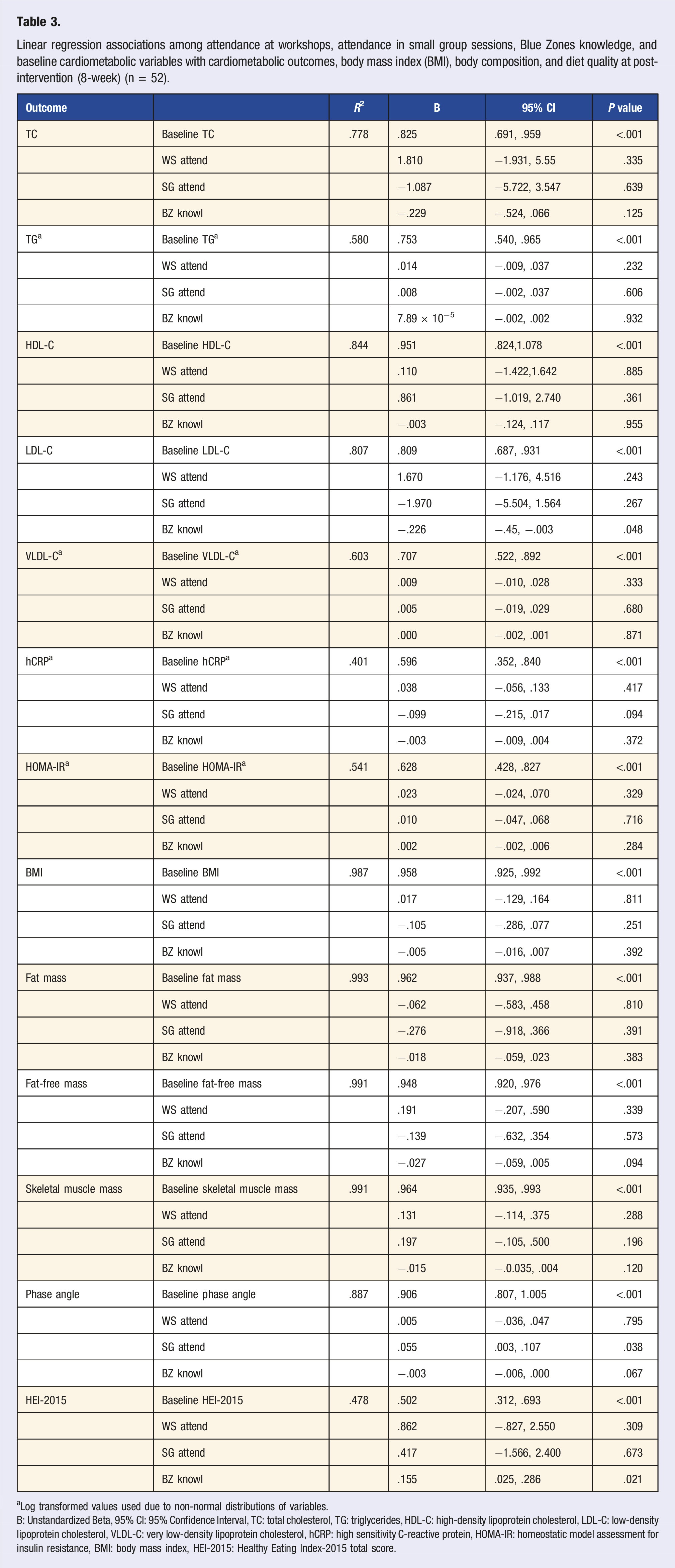
aLog transformed values used due to non-normal distributions of variables.
B: Unstandardized Beta, 95% CI: 95% Confidence Interval, TC: total cholesterol, TG: triglycerides, HDL-C: high-density lipoprotein cholesterol, LDL-C: low-density lipoprotein cholesterol, VLDL-C: very low-density lipoprotein cholesterol, hCRP: high sensitivity C-reactive protein, HOMA-IR: homeostatic model assessment for insulin resistance, BMI: body mass index, HEI-2015: Healthy Eating Index-2015 total score.
Discussion
Following an 8-week virtual nutrition intervention, total cholesterol, HDL-C, LDL-C, BMI, fat mass, fat-free mass, skeletal muscle mass, and phase angle decreased significantly. The decreases in blood lipids indicate that plant-based diets benefit dyslipidemia management. Further, due to the ability of plant sterols to reduce circulating total cholesterol and LDL-C via inhibiting cholesterol absorption in the gastrointestinal tract, this dietary pattern can assist with the prevention of CVD and hypertension.19,20 While it may be concerning to observe HDL-C (i.e., “good” cholesterol) decrease, this may occur because the body’s requirements for HDL to metabolize excess cholesterol decline as total cholesterol simultaneously decreases. 21 Although triglycerides, VLDL-C, hsCRP, and HOMA-IR decreased, these changes were not significant.
The decreases seen in BMI and fat mass are potentially impacted by consuming a plant-based diet because fruit and vegetables are nutrient-dense containing lower fat, higher water content, and fiber. 22 Several studies support that increasing fruits and vegetables consumption are a source of weight management that can lead to positive health outcomes and reduced risk of chronic disease.11,23,24 By following a plant-based diet, the consumption of energy-dense foods decreases, reducing fat intake and increasing weight loss. 25 Skeletal muscle loss can be a component of weight loss, especially if resistance exercise such as strength-training is not incorporated into one’s lifestyle. 26 Previous research indicates when transitioning to more of a plant-based diet that results in a significant caloric reduction, individuals should ensure that they pay special attention to total protein intake, incorporate leucine-containing foods, and participate in regular resistance training exercise. 27 This intervention did not explicitly promote aerobic or resistance training; rather, participants were encouraged to follow the Power 9® Blue Zones principle of moving more. Although this intervention did not specifically focus on weight loss, it is observed by the reduction in BMI that this dietary protocol can potentially assist in weight loss, decreasing fat-free mass, and phase angle as well.28,29
HEI-2015 scores significantly increased, demonstrating that participants in this study improved their diet quality during this 8-week intervention. Throughout the intervention, participants received behavior change support to improve their diet quality through the promotion and consumption of fruits, vegetables, nuts, and legumes. Plant-based diets focusing on nutrient-dense whole foods can lead to improved diet quality because they emphasize the consumption of fruits, vegetables, nuts, legumes, and whole grains. Research indicates plant-based diets receive higher HEI-2015 scores when compared to low-carbohydrate dietary protocols by improving micronutrient intake through increased vegetable-based meals.30-33
Results from the linear regression analyses indicated knowledge of Power 9® Blue Zones principles was a statistically significant predictor of post-intervention LDL-C and HEI-2015 total score, with increased knowledge of Power 9® Blue Zones principles resulting in decreased LDL-C and increased HEI-2015 diet scores. Plant-based diets have plant sterol/stanol soy protein and isoflavones that may help reduce cholesterol, resulting in lower CVD-related risk factors such as LDL-C.19,34 Increased knowledge of Power 9® Blue Zones principles and lifestyles exposed participants to more beneficial plant-based dietary approaches. Further, Blue Zones knowledge as a predictor of HEI-2015 diet score suggests that this intervention contributed to improved dietary patterns and behavior change among the participants.
Small group attendance was a statistically significant predictor of post-intervention phase angle, with increases in attendance resulting in increased phase angle. Higher values of phase angle represent greater muscle mass. Although results from paired sample t-tests indicated a slight decline (.1 ± .6) in phase angle, attendance appears to mitigate the potential for decreases in muscle mass that often accompany diet-induced weight loss. 26 Creating goals in small group sessions may have held participants accountable for implementing these goals, and thus, increased adherence to consuming a plant-based diet. 35 While attendance and Blue Zones knowledge did not predict any other cardiometabolic, anthropometric, or body composition variables, it should still be encouraged to promote attendance during virtual interventions because participants will gain exposure to educational and practical information via behavioral counseling sessions and workshops.
This study had numerous strengths; one of the primary strengths was the intervention study design, allowing for an assessment of a temporal relationship and the opportunity to make inferences about causality. Another advantage is this study design provided for the assessment of multiple outcomes, including cardiometabolic and body composition variables. Further, the virtual, online-based implementation of the intervention is feasible to reproduce and duplicate. Participant recruitment was facilitated by broad inclusion criteria and limited exclusion criteria as all university staff interested in plant-based lifestyles were eligible to participate. This led to a study sample that more accurately represents the target population. Lastly, the ASA24, a validated dietary recall survey, was used for assessing diet quality. Body composition measurements were collected using a Seca® medical Body Composition Analyzer with a 98% tested accuracy. 20
The intervention was a pilot study, limiting the ability to adequately examine the impact of a plant-based lifestyle on some risk factors. For example, it would be advantageous to assess HOMA-IR in a more extended study design. Due to the COVID-19 pandemic, the intervention was held in a virtual environment. The formation of relationships with participants may have become difficult to maintain due to potential distractions at home and work that could create obstacles in participant engagement. To mitigate this limitation, we divided the study population into six small groups that met weekly and were facilitated by coaches to engage participants and facilitate behavior change. Selection bias may have occurred because participants volunteered for the study, potentially demonstrating greater motivation than the general university staff population. This bias was partially mitigated through a pre-study questionnaire that assessed the required inclusion criterion of an expressed motivation to change. Assessments conducted by the university employee assistance and wellness program indicate that women apply for interventions and programs more than men, which was also true for this study. Although the ASA24 is a validated survey, recall bias may occur during reporting of diet. Using the ASA24 helped mitigate this bias by only allowing participants to enter dietary information from the previous day and providing prompting questions to aid in the recall of food or beverages that would otherwise be missed.
Conclusion
An 8-week virtual worksite nutrition intervention successfully reduced cardiometabolic risk factors in a group of employees during COVID-19. These positive outcomes indicate that using a virtual intervention model is worth expanding to larger samples and other demographic groups. Based on the success of this intervention model, we recommend continued investigation of the impacts of a plant-based dietary pattern on the cardiometabolic risk factors associated with chronic diseases. For example, further research is needed to determine if other variables, such as attitudes or skills acquired, may account for the positive behavior change observed in the intervention. Future studies may further investigate the implications of a plant-based diet on cardiometabolic risk factors and COVID-19. Despite the need for more research, it can be concluded that a weekly Blue Zones nutrition intervention with weekly workshops containing an educational component, interactive cooking demonstration, and small group wellness counseling sessions helps improve overall diet quality and cardiometabolic risk factors associated with chronic disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Eric M. Lehrman 2015 Trust and the Northern Arizona University Department of Health Sciences.
Presentation
This paper was presented as a poster presentation at the 43rd annual conference of the Society of Behavioral Medicine in Baltimore, Maryland on April 8, 2022.
Data Sharing
Data can be shared by individual request.