
Abstract
Community-based interventions using an ad libitum Whole Food Plant-Based Diet (WFPB) effectively promote weight loss and reduce cardiovascular risk factors. Although in-person delivery fosters valuable social interaction, it also increases costs and limits scalability. This pilot study evaluated a 5-week, remotely delivered WFPB intervention with online community support among 18 women with overweight or obesity, 16 of who completed outcome measures. Participants received WFPB meal plans, attended weekly remote sessions, and posted daily meal photos in a dedicated Facebook group, to facilitate interaction between participants. Weight, fat mass, body mass index, lipid profile, and blood pressure were assessed at baseline, Week 5, and Week 12 (7 weeks post-intervention). At Week 5, mean weight loss was 4.99 ± 1.84 kg (P < .001), with 80% of participants losing an additional 2.63 ± 1.58 kg during follow-up. By Week 12, total weight loss averaged 6.86 ± 3.00 kg, with 80% from fat mass. Significant reductions in total and LDL cholesterol (P < .001) and systolic blood pressure (P < .001) persisted. High online group engagement correlated with greater post-intervention weight loss (r = 0.62, P < .05). These findings support the feasibility of digitally delivered WFPB programs for improving weight and cardiometabolic health, and warrant future large-scale, extended trials to confirm and refine their long-term effectiveness and generalizability.
Keywords
“Participants demonstrated statistically significant improvements in anthropometric and cardiometabolic markers after the intervention, with sustained benefits observed in most measures at Week 12.”
Introduction
Obesity remains among the leading causes of morbidity and mortality worldwide, affecting 890 million adults in 2022 with expectation to exceed one billion before the year 2030.1,2 Obesity is a risk factor for cardiovascular disease, including coronary artery disease and hypertension, as well as metabolic disorders such as type 2 diabetes. 3 Excess adipose tissue contributes to chronic low-grade inflammation, insulin resistance, and dyslipidemia, all of which exacerbate cardiovascular risk.4,5 Furthermore, obesity has been linked to worse outcomes in infectious diseases, including COVID-19, underscoring its broad health implications. 6 Given the significant burden of obesity-related heart disease and the limitations of pharmacological or surgical interventions alone, lifestyle-based strategies are essential for both prevention and treatment. Dietary interventions, in particular, play a critical role in addressing obesity and its cardiometabolic consequences, highlighting the need for sustainable, evidence-based nutritional approaches. 7
The Whole Food Plant-Based Diet (WFPB) has demonstrated the ability to promote sustainable weight loss and improve cardiometabolic health. 8 WFPB emphasizes fruits, vegetables, whole grains, and legumes while minimizing or eliminating refined foods, oils, and animal products.7,9 As such, they are naturally lower in calorie density and higher in fiber and phytonutrients—allowing individuals to reduce total energy intake without strict portion control or calorie counting. This allows to consume WFPB meals freely until comfortably satiated (eating ad libitum) and still achieve calorie deficit and weight loss.7,10-12 Beyond weight management, numerous studies have shown that WFPB eating patterns can reduce plasma cholesterol levels, improve insulin sensitivity, lower blood pressure and induce positive changes in gut microbiota.8,13-16 In certain contexts, such dietary changes may even contribute to the reversal of advanced cardiovascular disease.17,18 Large epidemiological investigations, including Adventist Health Studies, also link predominantly plant-based diets with lower risk of chronic diseases. 19
Community-based in-person programs have proven particularly effective in achieving empowering participants to make and maintain dietary changes. Initiatives such as the Complete Health Improvement Program (CHIP) and the BROAD Study, have demonstrated that structured, group-oriented support is associated with greater adherence and more pronounced benefits in body weight and cardiometabolic markers.8,10,20 More recent interventions serve as further evidence of the efficacy of an in-person community-based WFPB interventions for weight loss and health improvements.21,22
CHIP program and the BROAD study are particularly notable, CHIP for being the most widely studied, with over 25 peer-reviewed studies published, and BROAD for achieving the greater weight loss after 6 and 12 months than any other trial not limiting energy intake or mandating exercise.8,10 The BROAD study enrolled 33 adults (67 % women; mean age 56 years) who were overweight or obese and had at least one comorbidity—type 2 diabetes, heart disease, hypertension, or elevated cholesterol. Participants adopted a low-fat (7-15 % of total energy) WFPB diet centered on whole grains, legumes, vegetables and fruits while excluding animal products, added oils, high-fat plant foods, and processed items. Eating to satiety was encouraged; no calorie limits were imposed. A 50 μg vitamin B12 supplement was provided daily. The 12-week program delivered two 2-hour group sessions per week that combined cooking demonstrations, health education, and facilitated discussion, along with special events to reinforce engagement and adherence. 8
The CHIP program has been delivered in communities across North America, Australia and in Europe to over 60000 individuals.10,23 The intervention design has evolved over time; however the core format remains the same and consists of 16 to 18 in-person group meetings in which a pre-recorded educational video is paired with interactive components—culinary demonstrations, guided physical activity, and group discussion. Early sessions introduce the etiology of chronic disease and the benefits of lifestyle change, while later sessions focus on overcoming barriers and maintaining new behaviors. CHIP advocates a low-fat, WFPB dietary pattern rich in whole grains, legumes, fruits, and vegetables, while discouraging foods high in cholesterol, fat, refined sugars, and salt. 10
Despite their success, these in-person programs can be limited by high costs and geographic barriers that reduce their scalability and may not be available in epidemiologically unfavorable conditions. All these factors highlight the need for effective remotely delivered lifestyle interventions, available to broader populations at lower cost, without the need for in-person attendance.6,24 Telehealth interventions for weight management are increasingly common but still understudied in the specific context of WFPB.24,25 Moreover, remotely delivered programs may struggle to replicate the natural sense of community and real-time peer support that can make face-to-face models more effective.8,24,26
To address these gaps, we developed a remotely delivered 5-week WFPB intervention supplemented by online community support, combining dietary education, practical strategies for meal preparation, and active social media engagement. The primary objective of this pilot study was to evaluate the short-term (5-week) and medium-term (12-week) effects of this remotely delivered, community-supported WFPB intervention on body weight, body composition, lipid profile, and blood pressure. We hypothesized that a virtual community setting, alongside structured WFPB meal plans and regular group sessions, would help participants achieve clinically meaningful weight loss and improve cardiovascular risk factors, in line with the CHIP program and the BROAD study.8,10
Methods
Study Design and Setting
This single-arm pilot study was conducted to evaluate the effectiveness of a 5-week remotely delivered whole food plant-based (WFPB) weight loss intervention, followed by a 7-week non-intervention period (12 weeks total). The study was carried out between March and June 2024, with all measurements and sample collection taking place at the Institute of Nutrition and Genomics of the Slovak University of Agriculture in Nitra, Slovakia. Written informed consent was obtained from all participants prior to the participation and the study protocol was approved by the independent Ethics committee of Specialized Hospital of St. Svorad Zobor (approval number: 20230512/1). For the full text of Informed consent and the Ethics committee approval see Appendix A and Appendix B.
Participants
Eligibility Criteria
To reduce sample heterogeneity and allow more precise assessment of this intervention, this pilot study focused on women only. Eligible participants were adult women (≥18 years) with self-reported overweight or obesity who maintained a relatively stable weight (±3 kg) in the preceding 3 months. Participants on stable antihypertensive, thyroid, or lipid-lowering medications were eligible. They were instructed to report any medication changes during the study to enable appropriate tracking and data interpretation. Individuals were excluded if they were pregnant or lactating, had a self-reported history of liver or kidney disease, or could not commit to firmly scheduled online group sessions and evaluation dates.
Sample Size Determination
Since this was a pilot feasibility study, formal power calculations were not performed. Methodological guidance indicates that ≈12-25 participants per arm (or total in a single-arm design) are sufficient for feasibility objectives: the “12-per-group” rule of Julious, 27 simulation studies by Whitehead et al. recommending 15-25 per arm, 28 and the CONSORT extension for pilot/feasibility trials, 29 all converge on this range. Our target of 25 enrollments, yielding 16 complete-case participants, therefore sits comfortably within accepted methodological recommendations.
Recruitment and Enrollment
Recruitment was conducted using social media advertisements targeting adult women in the Nitra region of Slovakia, due to proximity to the Institute of Nutrition and Genomics, where study assessments were conducted. The recruitment continued for 2 weeks until the threshold of 25 eligible participants was reached. An additional 34 applicants were excluded after screening based on the eligibility criteria detailed in Figure 1. The 25 eligible participants were invited for baseline measurements, and 18 attended. Among these 18, 16 completed all three scheduled assessments, at baseline (W0), week 5 (W5), and week 12 (W12). The remaining two participants did not provide a full set of measurements for any outcome variable and were therefore excluded from all analyses, which were conducted on a complete-case, per-outcome basis. Full details of participant flow are presented in Figure 1. Participant flow chart.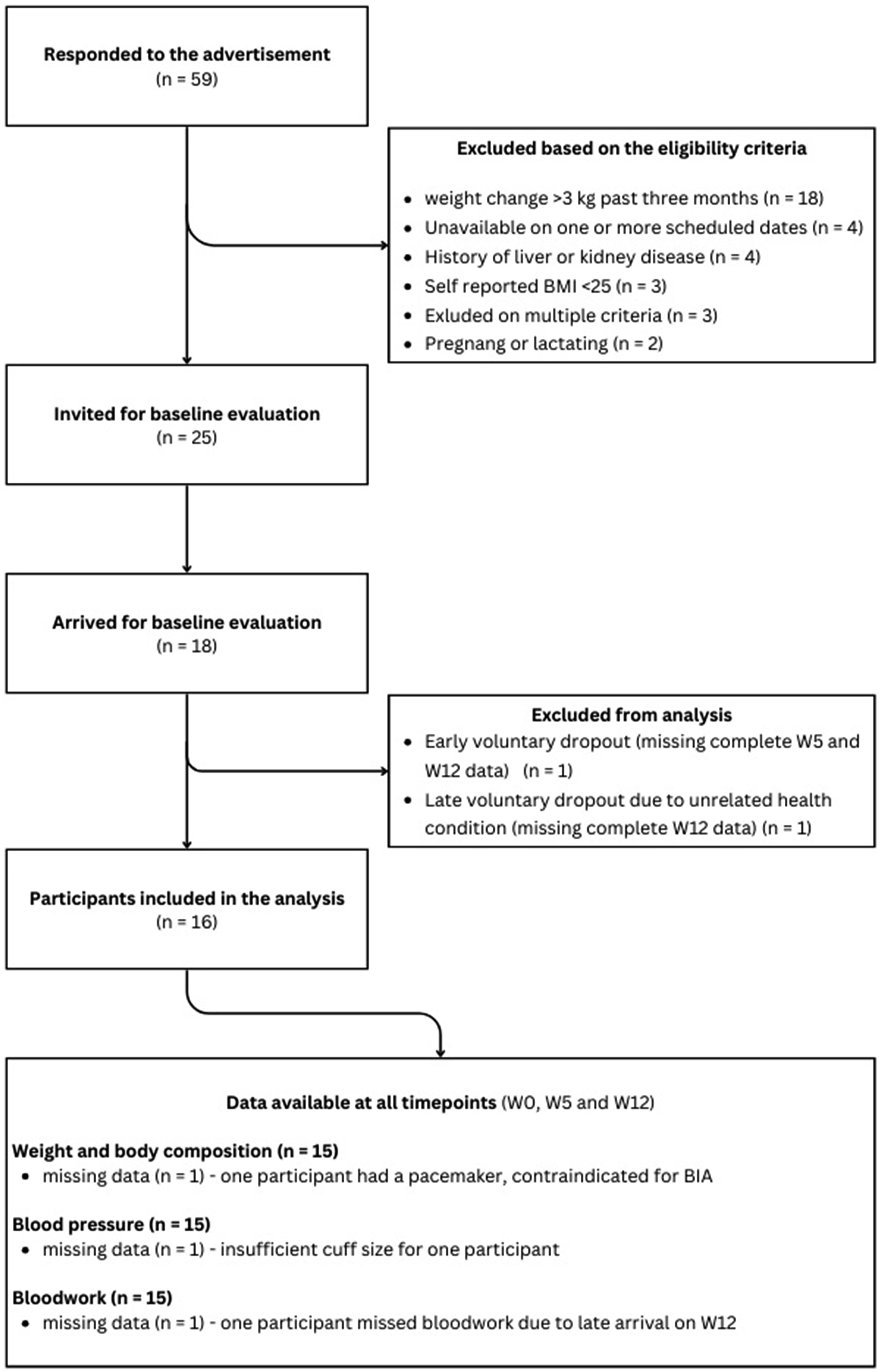
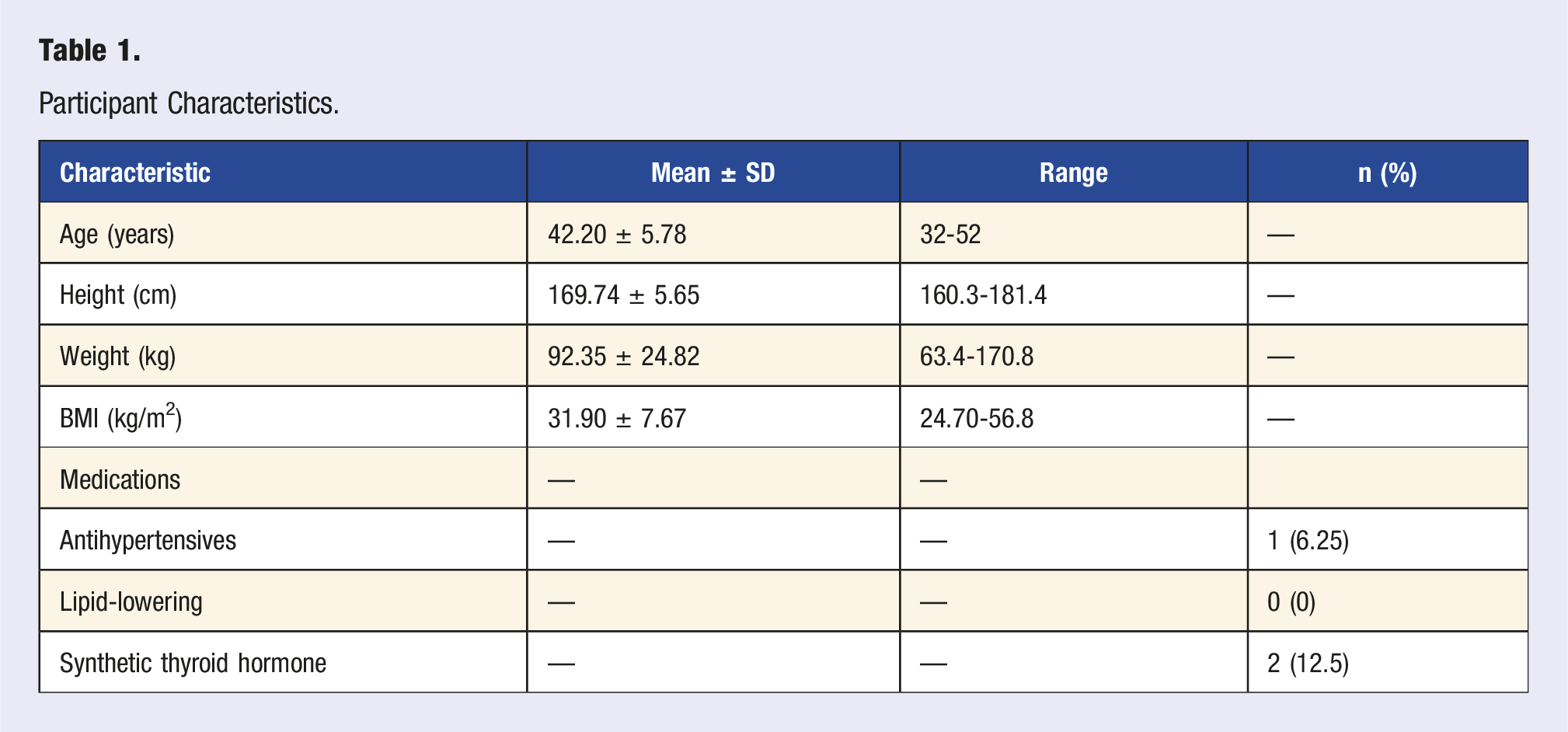
Participant Characteristics
Participant Characteristics.
Intervention
Content and Delivery
Interventional Content Outline.
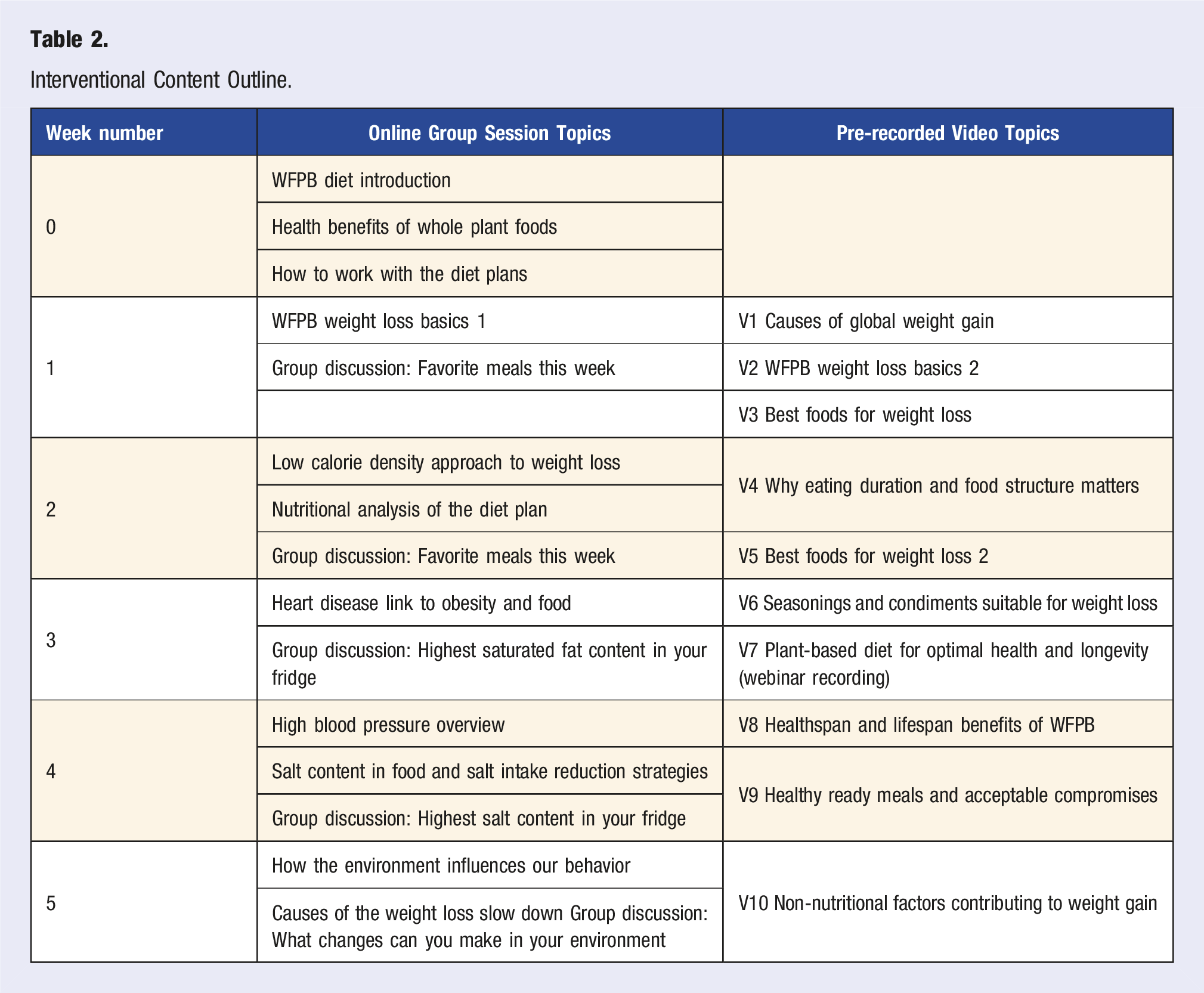
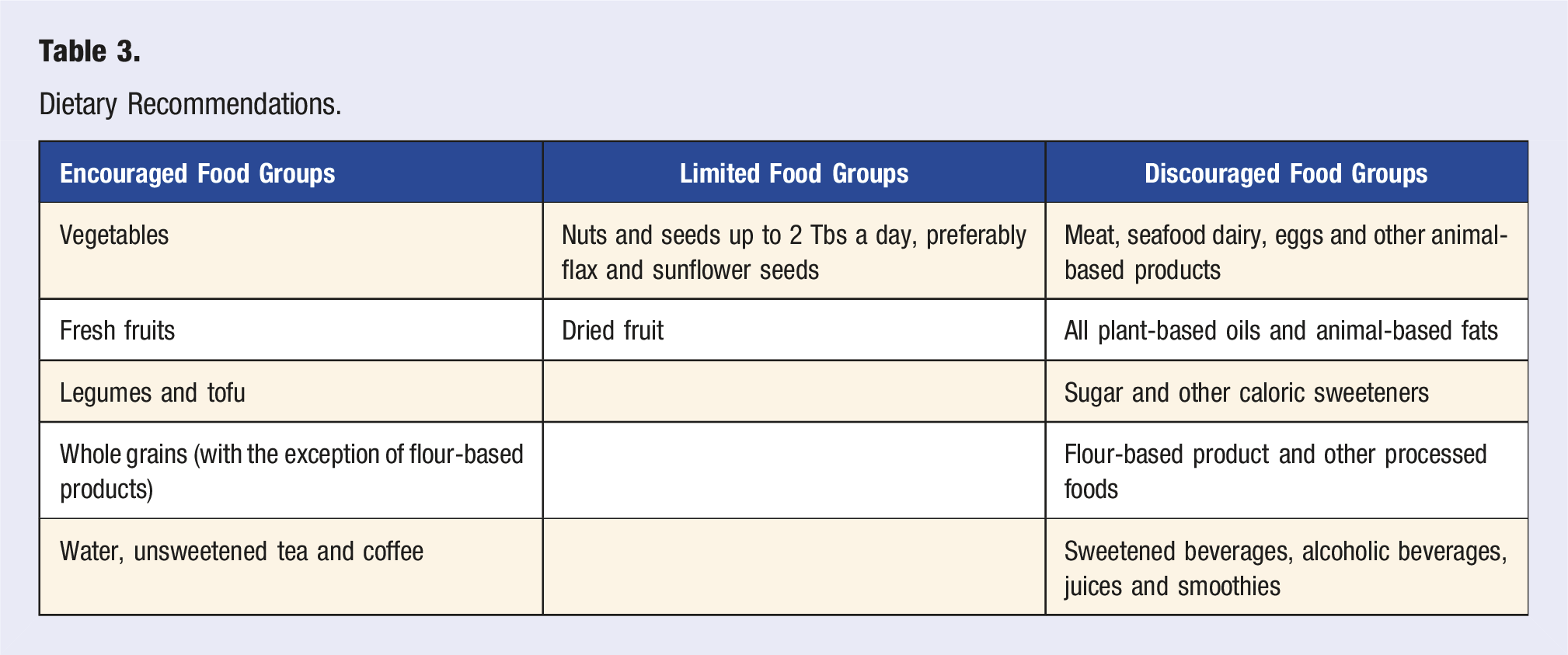
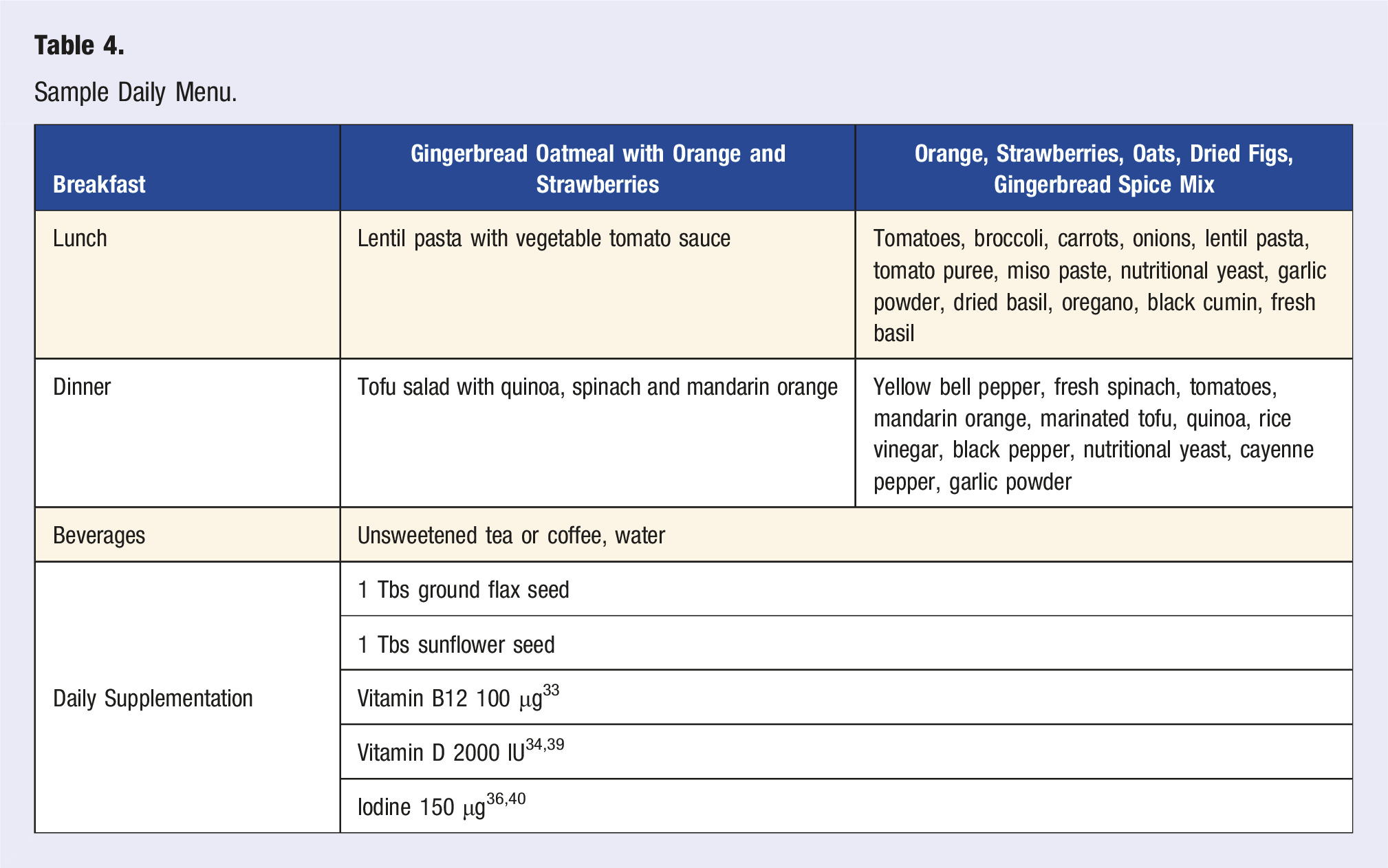
Participants received weekly diet plans (recipes, shopping lists) based on vegetables, fruits, whole grains, legumes, and tofu. Sample ratios and quantities of ingredients were provided to simplify meal preparation, but participants were instructed to eat to satiety (ad libitum). No food or financial compensation for grocery shopping was provided, as diet plans contained foods widely available in Slovakia and plant-based diets may even reduce overall grocery expenses. 30
Dietary Recommendations.
Sample Daily Menu.
Online Community Support
A private, invite-only Facebook group was created to foster participant interaction throughout the intervention. The lead author, serving as the group moderator, posted reminders about upcoming live sessions and commented on participant meal photos to offer encouragement, suggest improvements, and answer questions. Aside from these moderator contributions, no other structured prompts were provided, allowing participants to organically interact with one another. Number of posts, comments, and reactions submitted by each participant during both the 5-week intervention and the subsequent 7-week non-intervention period were manually counted.
Measurements and Data Collection
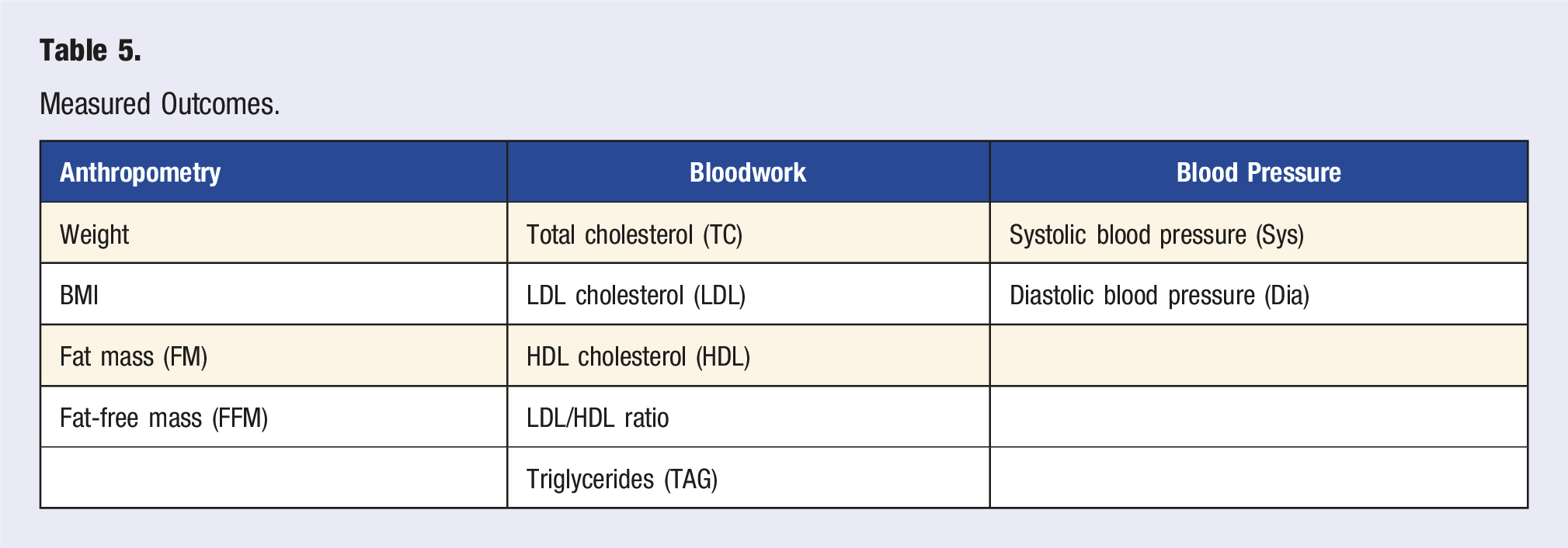
Measured Outcomes.
Blood Pressure
Upon arrival, participants were taken to the large classroom and were seated at the individual desks, allowing for the optimum position for the blood pressure measurement, with feet flat on the floor and arms supported at heart level. Participants remained seated for at least 5 minutes after which they were instructed to remain silent and one blood pressure reading was taken using the OMRON M7 Intelli IT (OMRON HEALTHCARE Co, Ltd., Japan).
Anthropometry and Body Composition
For the body composition and anthropometric measurements, participants were sent to the separate room, one at a time. First height was measured using a Bodyson ultrasonic height meter (ADE GmbH & Co., Hamburg, Germany) and subsequently weight and body composition was measured using the multi-frequency bioelectrical impedance analyzer (BIA) InBody 970 (Biospace, Seoul, South Korea). The InBody 970 used eight different frequencies (1, 5, 50, 250, 500, 1000, 2000 and 3000 kHz) to measure impedance and reactance across multiple segments of the body. To ensure accurate and consistent body composition analysis, participants were asked to be bare foot and in minimal clothing of their choice, with the request to wear the same clothing each evaluation. Body Mass Index (BMI) was calculated as weight in kilograms divided by the square of height in meters.
Blood Biochemistry
At the end a fasting blood sample was obtained from each participant by a medical doctor on-site in a third room. Samples were transported to the Biochemical Laboratory of Specialized Hospital of St. Svorad Zobor and analyzed the same morning. All measured parameters can be found in Table 5.
Outcome Measures
Primary outcomes were changes in body weight, BMI, and body composition (fat mass, fat-free mass). Secondary outcomes included changes in blood pressure and lipid profile. Engagement in the social media group (number of posts, comments, and reactions) was recorded to explore possible correlations with intervention outcomes.
Statistical Analysis
All statistical tests were performed using Microsoft Excel (Microsoft 365 MSO version 2412) and the DATAtab online statistic calculator (https://datatab.net/). Normality of continuous data was evaluated using Shapiro-Wilk tests. Because data were sufficiently normal for this sample size, two-tailed paired t-tests with α = 0.05 were used to compare values from W0 with W5 and W0 with W12 values. Pearson correlations were calculated to explore associations between engagement metrics and changes in weight. Statistical significance was set at P < .05 considered significant. Analyses were conducted on a complete-case, per-outcome basis: for each outcome variable, only participants with non-missing values at all three scheduled time points for that specific outcome were included in its analysis. No imputation was undertaken because the small pilot sample size precluded reliable modeling of missing values.
Results
Anthropometry and Body Composition
During the 5-week intervention, the 15 participants who provided complete anthropometric measurements lost an average of 4.99 ± 1.84 kg, corresponding to −5.4% of their baseline weight (P < .001). Over the subsequent 7-week non-intervention period (W5 to W12), 12 out of 15 (80%) of these participants lost an additional 2.63 ± 1.58 kg (−2.8% from W5), whereas the remaining three (20%) gained 1.13 ± 0.72 kg. By Week 12 (W12), the mean total weight loss from baseline reached 6.86 ± 3.00 kg (−7.4%). Figure 2 illustrates the distribution of individual weight changes, and complete data are available in Table 6. Weight loss data distribution. Full Results.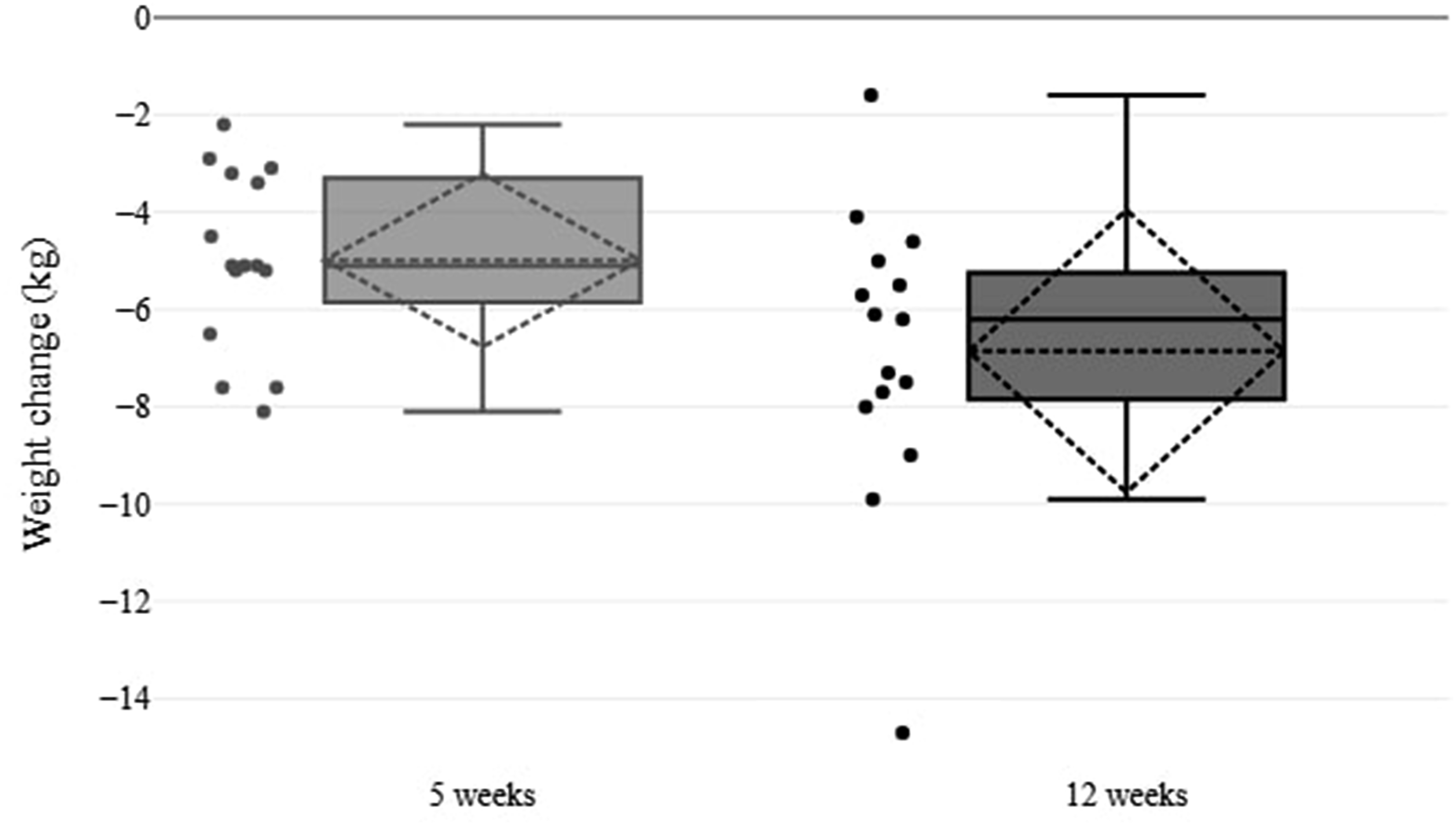
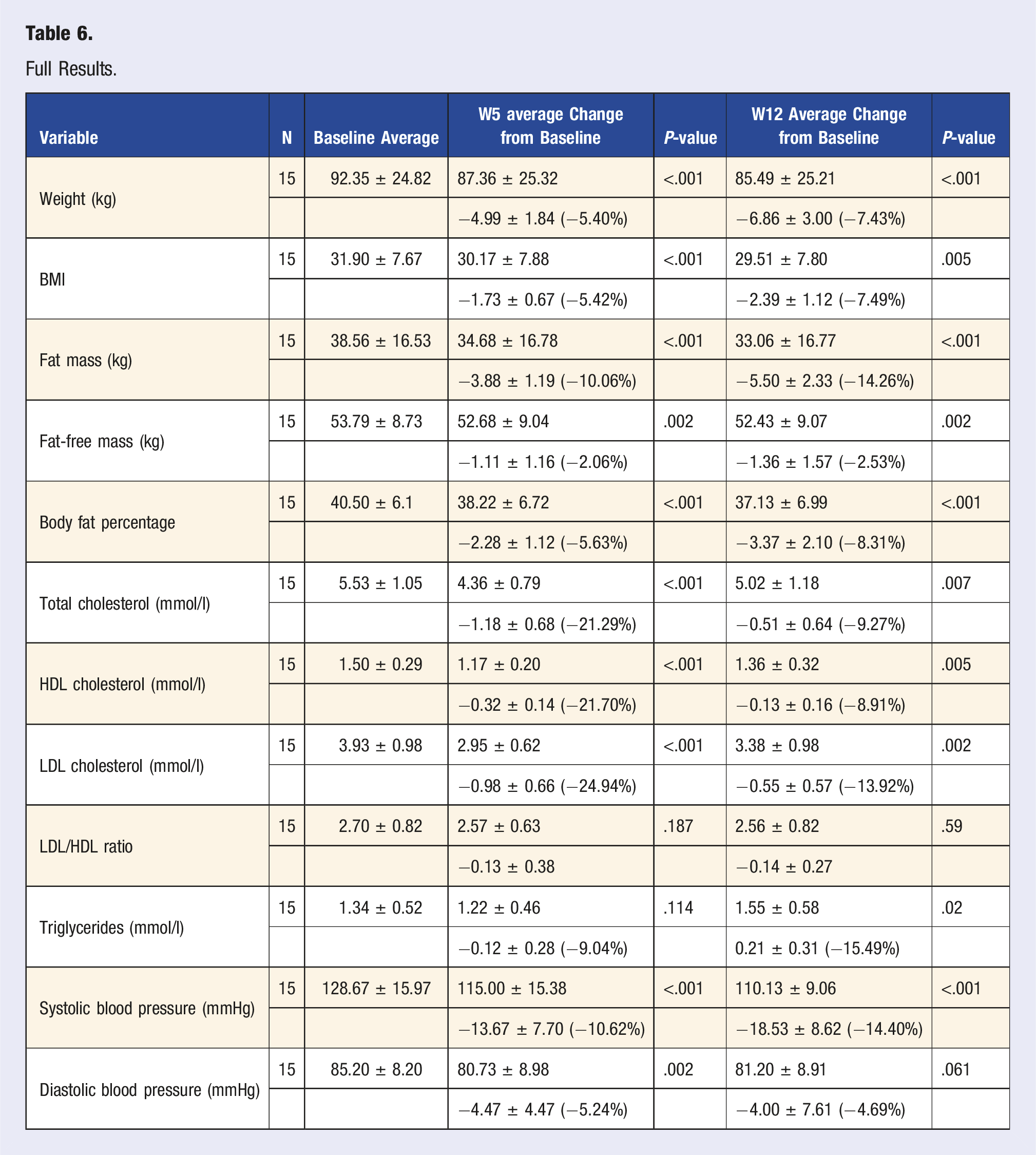
The net 5.50 ± 2.33 kg drop in fat mass (P < .001) at W12 represented a −14.3% change from baseline. Reduction in overall body weight correlated very strongly with reductions in fat mass (r(13) = 0.85, P < .001). Figure 3 provides a scatterplot illustrating this correlation, while Table 6 details all anthropometric measures. Fat mass and weight reduction scatter diagram.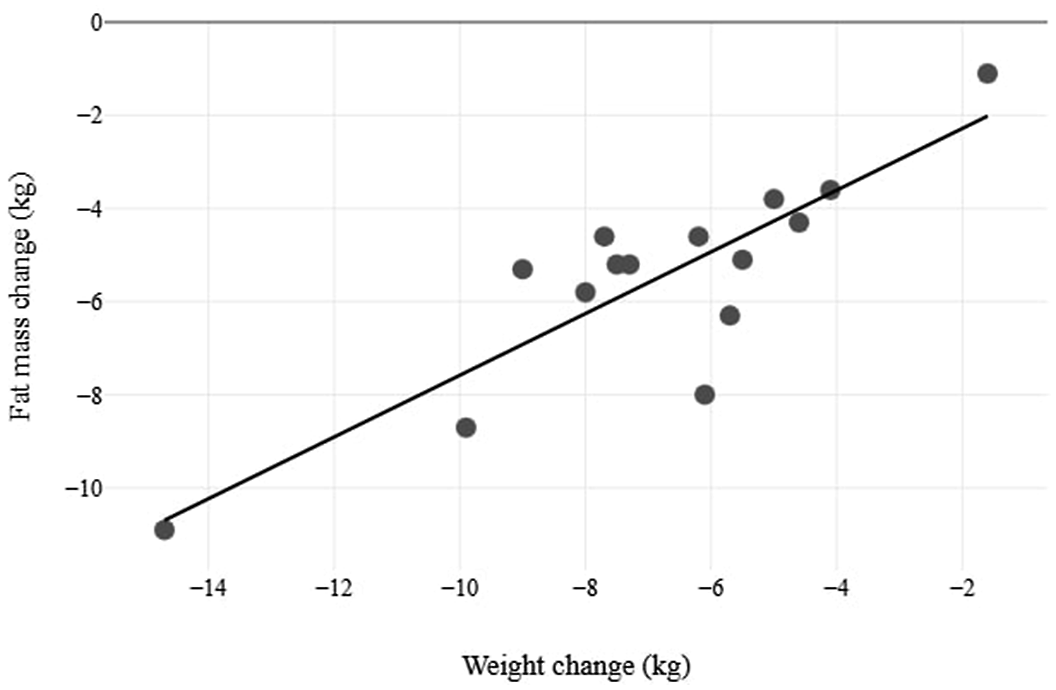
Biochemical Analysis
By the end of the 5-week intervention, participants exhibited highly significant reductions in LDL, HDL and total cholesterol and in LDL/HDL ratio. Specifically, LDL cholesterol decreased by 24.94% (−0.98 ± 0.66 mmol/l). Although levels partially rebounded during the 7-week follow-up, both LDL and total cholesterol values remained significantly below baseline by Week 12 (P = .007) and the average LDL/HDL ratio even showed a further slight decrease. Average triglycerides showed a modest, non-significant decline during the intervention, but rose significantly above baseline by Week 12 (P = .02). Figure 4 illustrates the cholesterol level changes, and Table 6 summarizes all blood lipid data. Cholesterol levels changes.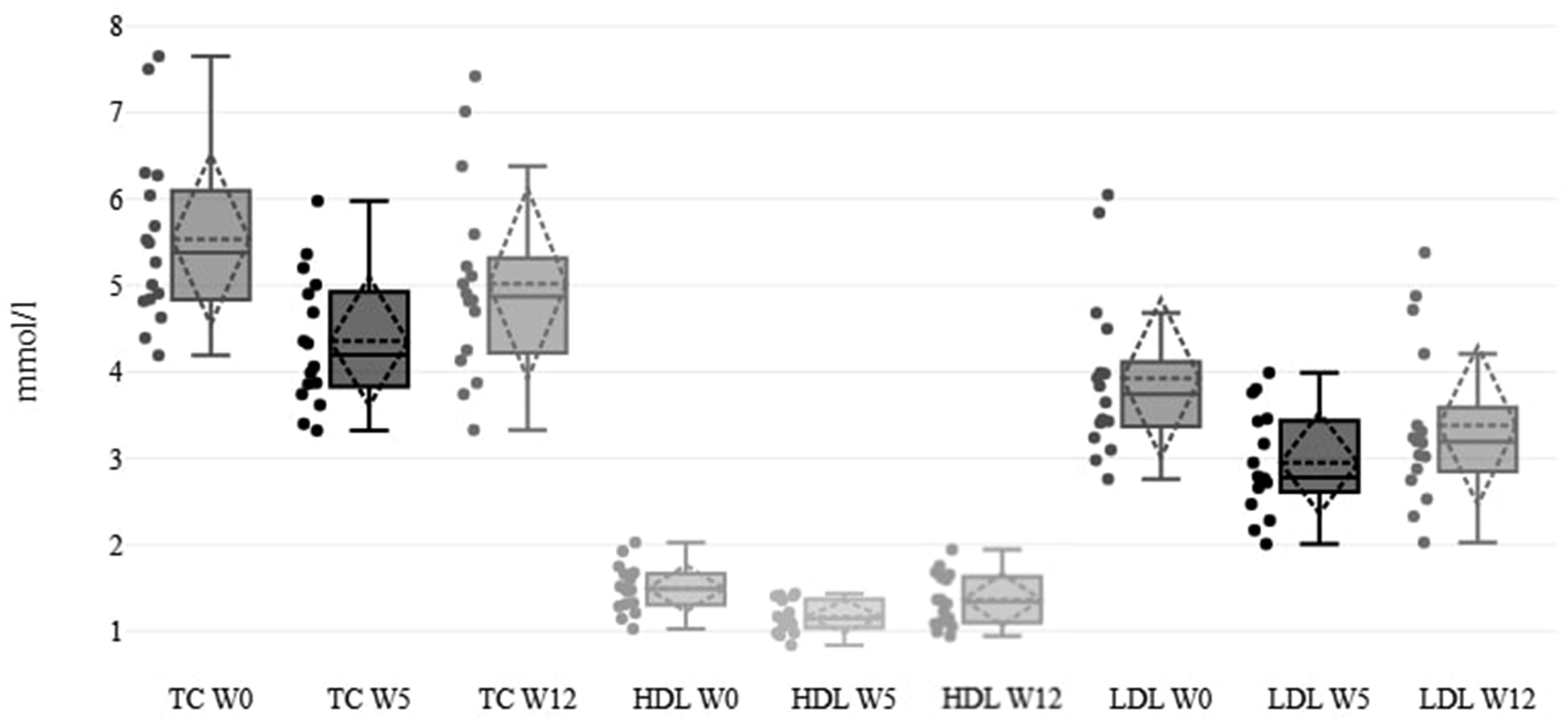
Blood Pressure Monitoring
Systolic blood pressure declined significantly over both study phases, dropping from 128.67 ± 15.97 mmHg at baseline to 115.00 ± 15.38 mmHg at Week 5 (P < .001) and to 110.13 ± 9.06 mmHg by Week 12 (P < .001). Diastolic blood pressure initially decreased from 85.20 ± 8.20 mmHg to 80.73 ± 8.98 mmHg (P = .002), then rebounded slightly to 81.20 ± 8.91 mmHg at Week 12. Figure 5 illustrates these blood pressure trends, with full numerical data in Table 6. Blood pressure changes.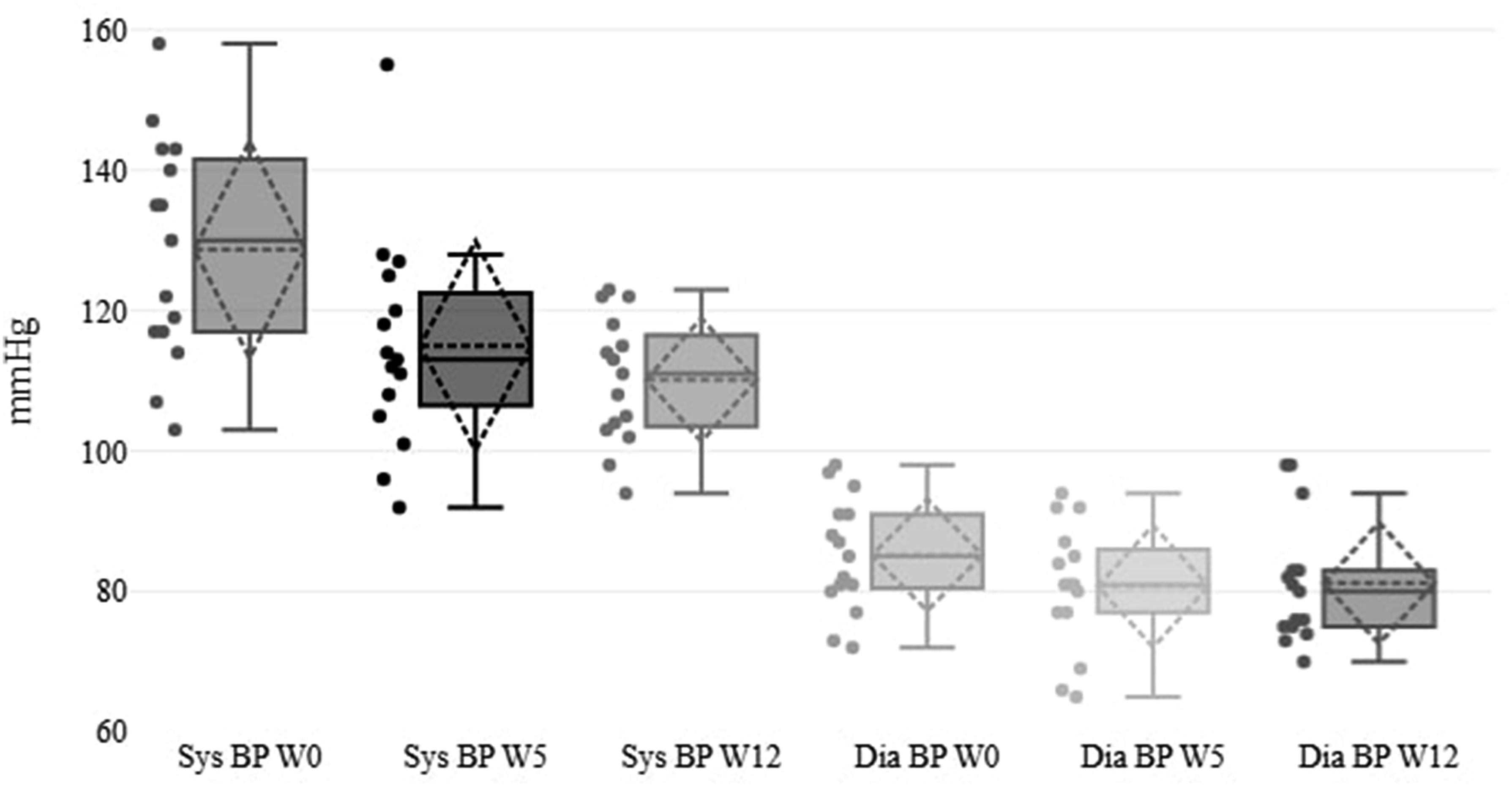
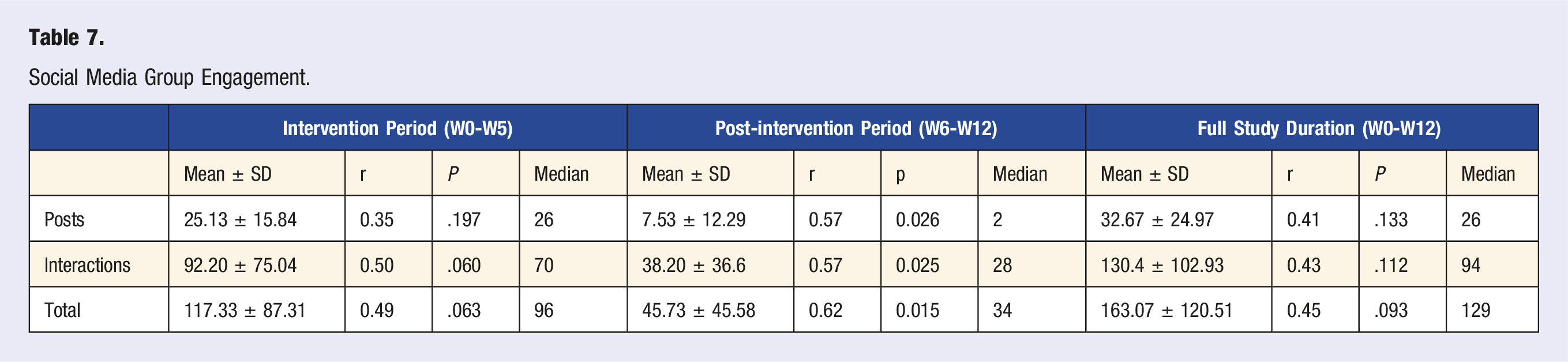
Social Media Group Engagement
Over the 12-week study, participants posted an average of 32.67 ± 24.97 times and logged 130.4 ± 102.93 total interactions (comments or reactions) in the dedicated Facebook group. Most of these occurred during the 5-week intervention, when participants were actively encouraged to share daily meal photos. Correlation analyses showed a moderate, non-significant relationship between group engagement and weight loss during the intervention (r = 0.49, P = .063). However, during the post-intervention follow-up, there was a significant high correlation (r = 0.62, P = .015) between engagement and further weight reduction. Figure 6 illustrates this association, and Table 7 provides detailed engagement data. Social media engagement and weight in post-intervention period. Social Media Group Engagement.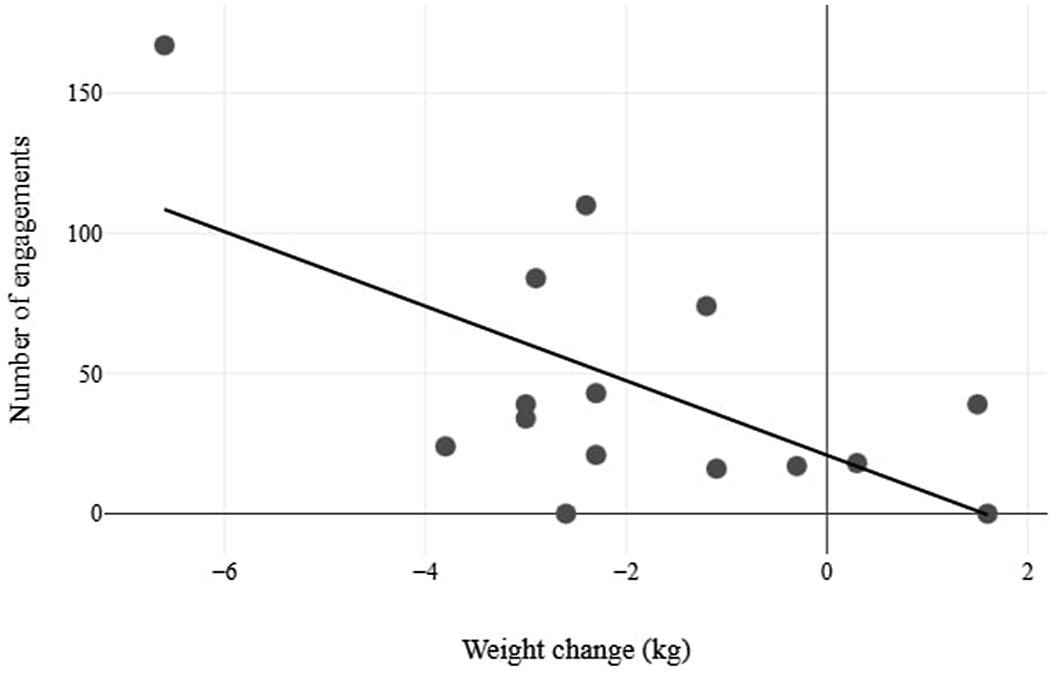
Discussion
This pilot study evaluated the results of a 5-week, remotely delivered whole food plant-based (WFPB) dietary intervention supplemented by online community support, followed by a 7-week non-intervention phase. The primary objectives were to determine short- and medium-term changes in body weight, body composition, lipid profile, and blood pressure. Overall, participants demonstrated statistically significant improvements in anthropometric and cardiometabolic markers after the intervention, with sustained benefits observed in most measures at Week 12.
Interpretation of Key Findings
All participants experienced weight loss during the 5-week intervention, with an average reduction of nearly 5 kg. The average 5.40 % weight reduction observed after 5 weeks is on par with thresholds commonly considered clinically relevant for improving metabolic health. 37 Notably, 12 out of 15 (80%) of participants who provided anthropometric data continued to lose weight during the subsequent 7-week non-intervention period, indicating a degree of sustainability once participants transitioned from the structured program to a more autonomous eating pattern. The weight reduction was composed primarily of fat mass (80.17% of total weight lost over 12 weeks), consistent with prior research linking WFPB diet to reductions in adiposity through decreased energy density and enhanced satiety. 12
During the 5-week intervention, there were significant reductions in total cholesterol, LDL cholesterol, and HDL cholesterol (all P < .001), while triglycerides showed a non-significant decline. By Week 12, LDL and total cholesterol remained below baseline despite partial rebounds, whereas triglycerides rose slightly above baseline. Although HDL declined, the LDL/HDL ratio showed a modest improvement (from 2.70 ± 0.82 at baseline to 2.56 ± 0.82 at Week 12), suggesting that the net change in lipid profile remained favorable overall. 38
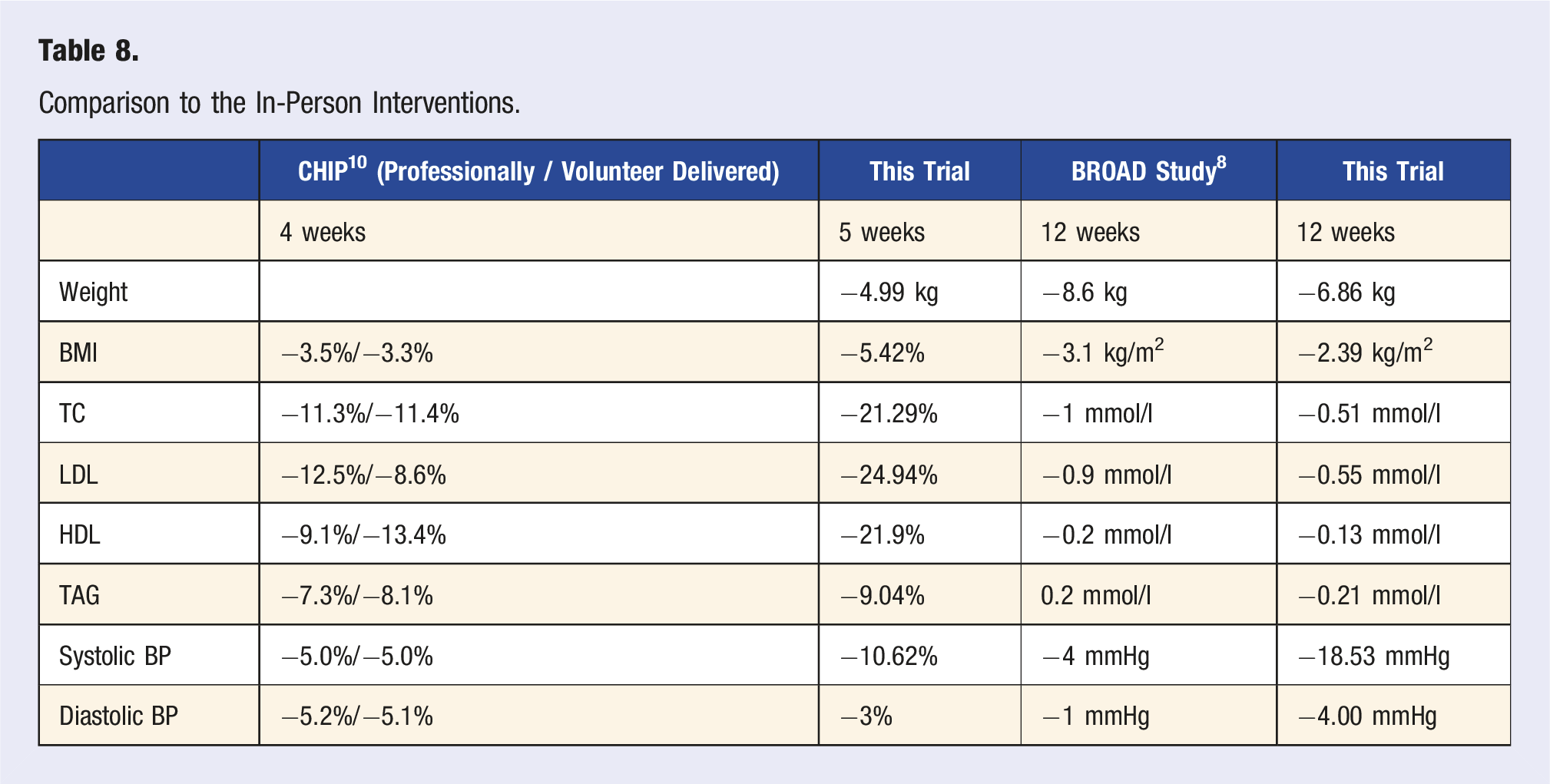
When compared to in-person community-based WFPB interventions, these outcomes are generally in line with previous trials. The CHIP Program reported on average 3.3 % to 3.5 % BMI reduction over 4 weeks, in comparison to 5.42 % reduction in 5 weeks in our trial. 10 Over the 12-week intervention BROAD study reported an 8.6 kg weight reduction compared to 6.86 kg in our trial, where 12 weeks included 7-week non-intervention period. 8 In a more recent WFPB pilot trial delivered via telehealth but without a social component, Chwyl et al 24 observed an average 5.9 kg weight loss at 12-week mark.
Comparison to the In-Person Interventions.
Role of Online Community Engagement
A unique aspect of this program was the online community component. Posting meal photos, commenting, and reacting to others’ posts provided immediate feedback and peer support. Although no significant correlation with weight loss emerged during the intervention phase, engagement strongly correlated with continued weight loss in the follow-up period (r = 0.62, P < .05). This suggests that the social support, motivation, and accountability of the online community might become increasingly important once the formal structure of the intervention ends. Notably, a Facebook group has previously been used as an adjunct to a WFPB intervention by Albert et al. 22 ; however, the effects of this component on outcomes were not evaluated, and the intervention also included in-person meetings. In contrast, our findings offer preliminary evidence that including an online community component in fully remote WFPB intervention may contribute meaningfully to long-term weight maintenance.
Strengths and Limitations
Strengths of the study include its real-world, low-cost design. The remote delivery allowed participants to engage with a structured, evidence-based program regardless of geographic constraints. Comprehensive measures of body composition, lipid profiles, and blood pressure offered a robust assessment of multiple cardiometabolic parameters. However, several limitations must be acknowledged. First, the lack of a control group precludes conclusions about the effect size of the online community component alone. Second, because this was a feasibility trial with a small convenience sample and no a-priori power calculation, it was not sufficiently statistically powered and therefore outcome comparisons—including those with larger interventions such as CHIP and BROAD—should be interpreted as descriptive only. Third, future trials with larger, more diverse samples (including men) are warranted to confirm and extend these findings. Finally, the follow-up period of 7 weeks may not fully capture long-term effect of the intervention on the body weight and cardiometabolic health, and additional research with extended follow-up and randomized controlled designs is warranted.
Conclusions
In summary, this pilot study provides preliminary evidence that a short-term, remotely delivered WFPB diet intervention, reinforced by regular group sessions and online community support, can produce clinically meaningful improvements in body weight, body composition, lipid profile and blood pressure, broadly comparable to the in-person interventions. A significant proportion of these benefits persisted through Week 12, suggesting a level of sustained impact beyond the formal intervention. Importantly, higher engagement in the online community during the non-intervention period was associated with continued weight loss, emphasizing the value of social support in the maintenance of lifestyle changes.
Longer-term research with larger sample and a control group is needed to confirm these findings and elucidate strategies for maximizing adherence and mitigating rebound effects in the post-intervention period. Nevertheless, this study contributes to the growing body of literature supporting WFPB dietary patterns for weight management and cardiometabolic health, while highlighting the feasibility of remotely delivered interventions and introducing the potential of the online community building for more sustainable results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was created with the support of the project Long-term Strategic Research of Prevention, Intervention, and Mechanisms of Obesity and its Comorbidities, IMTS: 313011V344, co-financed by the European Regional Development Fund.
Ethical Statement
Informed Consent
The written informed consent was obtained from all participants prior to the participation. For the full text of both documents see Appendix A and Appendix B