
Abstract
One-third of U.S. adults have prediabetes, but only 11% are aware of their condition. Many do not receive education or treatment. The purpose of this study is to understand family medicine providers’ and patients’ attitudes, knowledge, and behaviors regarding prediabetes and its management, to guide future management interventions. Cross-sectional surveys of providers (n = 54, 57% response rate) and patients with prediabetes (n = 148, 16.5% response rate) were administered at a large urban academic family medicine practice. Nearly all providers agree prediabetes screening is important, but over half were unaware of the national Diabetes Prevention Program (DPP) and most do not prescribe metformin to eligible patients. Over half of patients reported being told they have prediabetes but <5% had been referred to DPP and over half were unaware of medication options. In open-ended responses, providers suggested nutrition counseling resources and an improved DPP referral process to improve prediabetes care. Patients requested clear diagnosis, education on treatment options, and nutritional counseling. This study indicates that notable gaps continue to exist in provider and patient understanding and management of prediabetes, suggesting that interventions to improve prediabetes care should include more effective counseling on diagnosis and treatment and expanding access to nutrition and educational resources.
“Primary care providers and patients both agree that prediabetes diagnosis is important and motivates lifestyle changes.”
Nearly one-third of American adults have prediabetes, diagnosed as a hemoglobin A1C of 5.7–6.4%. 1 Data from prospective cohort studies show an estimated 31–45% lifetime risk of progressing from prediabetes to type 2 diabetes (T2DM).2,3 Screening and appropriate management, which include metformin and/or offering intensive lifestyle modification, such as the Diabetes Prevention Program (DPP) or other lifestyle modification program, can delay or prevent the progression from prediabetes to T2DM.4,5
Several provider-level barriers impede the delivery of optimal primary care for prediabetes. A significant minority of primary care providers believe that prediabetes is not a serious health concern. 6 The US Preventive Services Task Force (USPSTF) recommends screening for prediabetes in asymptomatic adults aged 35 to 70 years who are overweight or obese. 7 The American Diabetes Association (ADA) recommends screening for prediabetes in all adults 35 years or older, regardless of risk factors, and in all adults who are overweight or obese with 1 or more risk factors, regardless of age. 4 This recommendation is based on evidence that links obesity to insulin resistance and dysglycemia.8,9 Despite these recommendations from the USPSTF and ADA, prediabetes screening remains underutilized. 10
To manage prediabetes and prevent T2DM, the ADA recommends referral to an intensive lifestyle behavior change program, such as the DPP, dietary interventions, and consideration of metformin therapy. 11 However, relatively few primary care physicians offer patients prediabetes management options such as DPP/lifestyle modification or metformin. A 2019 provider survey and chart review of 15 520 patients with prediabetes in an academic health system found that only 20.4% of eligible patients were prescribed metformin, and none were referred to DPP. 10 National surveys of primary care physicians report similar low levels of prediabetes management.12,13 Reasons provided for not employing these management strategies include perceptions that patients are unwilling to engage in behavior changes, low awareness of DPP or other lifestyle modification programs, and lack of these programs in their region.12-14 These studies did not explore what prediabetes management support providers would like from their practices, such as educational materials, nutrition counseling, or an onsite DPP.
To date, several qualitative studies have examined primary care patients’ prediabetes perceptions on and willingness to initiate management strategies. Prediabetes diagnosis alone is often insufficient for motivating diet and physical activity changes among patients. 15 Patients reported that their providers were not always explicit about the implications of their prediabetes diagnosis and available management options, 14 and were not always aware of these options.14,16 While a number of patients were receptive to discussions of medication or lifestyle modification,14,16 they also noted barriers to DPP participation, including transportation and the substantial time commitment.14,17 However, no surveys have been conducted of primary care patients with prediabetes to determine what prediabetes management support they would like from their primary care practice.
Overall, a gap exists between current prediabetes recommendations and the care patients are receiving, and in our understanding of the prediabetes management support that providers and patients feel is most needed and feasible to implement in primary care. Our study’s aims were to: 1. Understand provider and patient knowledge of, and attitudes towards, prediabetes screening, diagnosis, risk, and management options in our practice; 2. Understand what prediabetes management providers currently offer patients, and provider- and patient-level management barriers; and 3. Elicit providers’ and patients’ suggestions for practice-based prediabetes management support to inform a targeted intervention.
Methods
Setting
Surveys were distributed from January 2021 to May 2021 to patients and providers of a large urban academic family medicine practice in [blinded for review]. This clinic serves over 30 000 patients making 80 000 visits annually. During the time of this study, 82–83% of all patients had an active patient portal. At the time of the study, there was no standard operating procedure for prediabetes diagnosis and treatment. Providers ordered screening bloodwork at their own discretion. This clinic has a relationship with the Center for Urban Health, which offers a DPP. There was a process for DPP referral that was established electronically, although this process was not widely used.
Study Design and Population
This study used cross-sectional survey data. Eligible participants included family medicine providers as well as adult patients seen within the past year with A1C in the last 6 months meeting criteria for prediabetes (5.7–6.4%). Patients who were pregnant, had a diagnosis of type 1 or type 2 diabetes, or were non-English speaking were excluded. Providers were given the opportunity to exclude certain patients who they preferred not to be contacted for participation. All study procedures and materials were approved by the [blinded for review] Institutional Review Board. Participants were not compensated.
Provider Survey
To develop our surveys, we conducted a focused literature search and incorporated or adapted questions from four published surveys on provider attitudes and knowledge of prediabetes.6,10,14,17 The study team generated questions on demographics and select questions in other domains. The final survey contained 20 items; domains included provider demographics, prediabetes knowledge, attitudes, and management, DPP awareness, and barriers to prediabetes treatment (Appendix, Exhibit A). The survey included multiple-choice and 5-point Likert scale responses (strongly agree to strongly disagree) and an open-ended question created by the study team on how the practice could improve prediabetes management. The survey was distributed via email to primary care providers (PCPs, n = 65), including attending and resident physicians and nurse practitioners. One reminder was sent.
Patient Survey
The patient survey synthesized or adapted questions from existing surveys or studies on patient attitudes and knowledge of prediabetes.14,18,19 The study team generated questions on demographics and select questions in other domains. The survey contained 33 items, assessing domains including patient demographics, awareness of diagnosis and risk, prediabetes knowledge and attitudes, experiences with DPP, and prediabetes experiences with their PCP (Appendix, Exhibit B). The patient survey included multiple-choice and Likert scale questions, and the same open-ended question as the provider survey. The survey was distributed to patients (n = 898) via secure patient portal used by >80% of the clinic’s patients. One reminder was sent.
Data Analysis
Qualtrics (Provo, UT, USA) was used to administer the survey and obtain anonymous data. IBM SPSS Statistics, IBM Corp., Armonk, NY, USA was used to examine all descriptive data and quantitative survey items. For analysis, we grouped the strongly agree and agree responses and disagree and strongly disagree responses. Descriptive statistics were generated and summarized for demographics and each of the provider and patient knowledge, attitudes, and experiences items. Differences in provider responses by resident vs attending status and years in practice were measured using Chi-square and t-tests. To determine whether our study population and our clinic’s larger population of patients with prediabetes differed by gender and age, a Chi-square test and t-test were performed, respectively. Chi-square tests were also performed to determine whether patients who were aware and unaware of their prediabetes diagnosis differed in their knowledge, attitudes, and experiences. Thematic analysis was conducted for open-ended responses, by discussion and agreement among three researchers. 20
Results
Provider Survey
Demographics
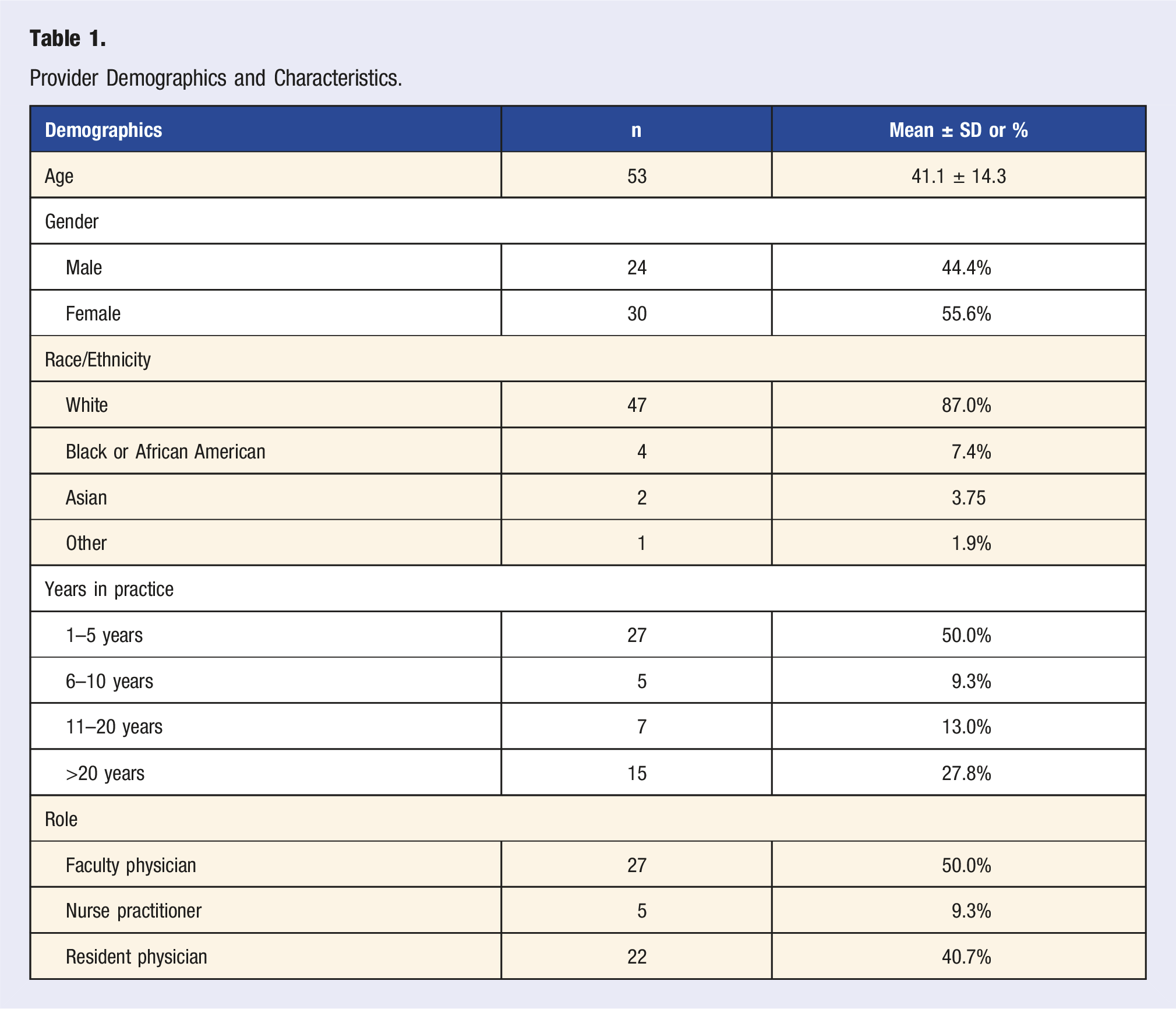
Provider Demographics and Characteristics.
Knowledge and Attitudes
Most providers (90.7%) considered diabetes screening a high priority. The majority of providers also considered the diagnosis of prediabetes effective for both increasing patient awareness of their need for lifestyle modification (96.3%) and for motivating lifestyle modification (92.6%). Although most providers acknowledged the effectiveness of lifestyle modification in treating prediabetes (92.6%), only 66.7% recognized the effectiveness of metformin in preventing T2DM. This data can be found in the Appendix (Exhibit C). There were no statistical differences in responses between resident and faculty physicians, except that a greater portion of faculty were familiar with the DPP (56.3% vs 27.3%, P = .037). The only difference based on years in practice was that longer practice was associated with being familiar with the DPP (P < .001).
Current Management Behaviors
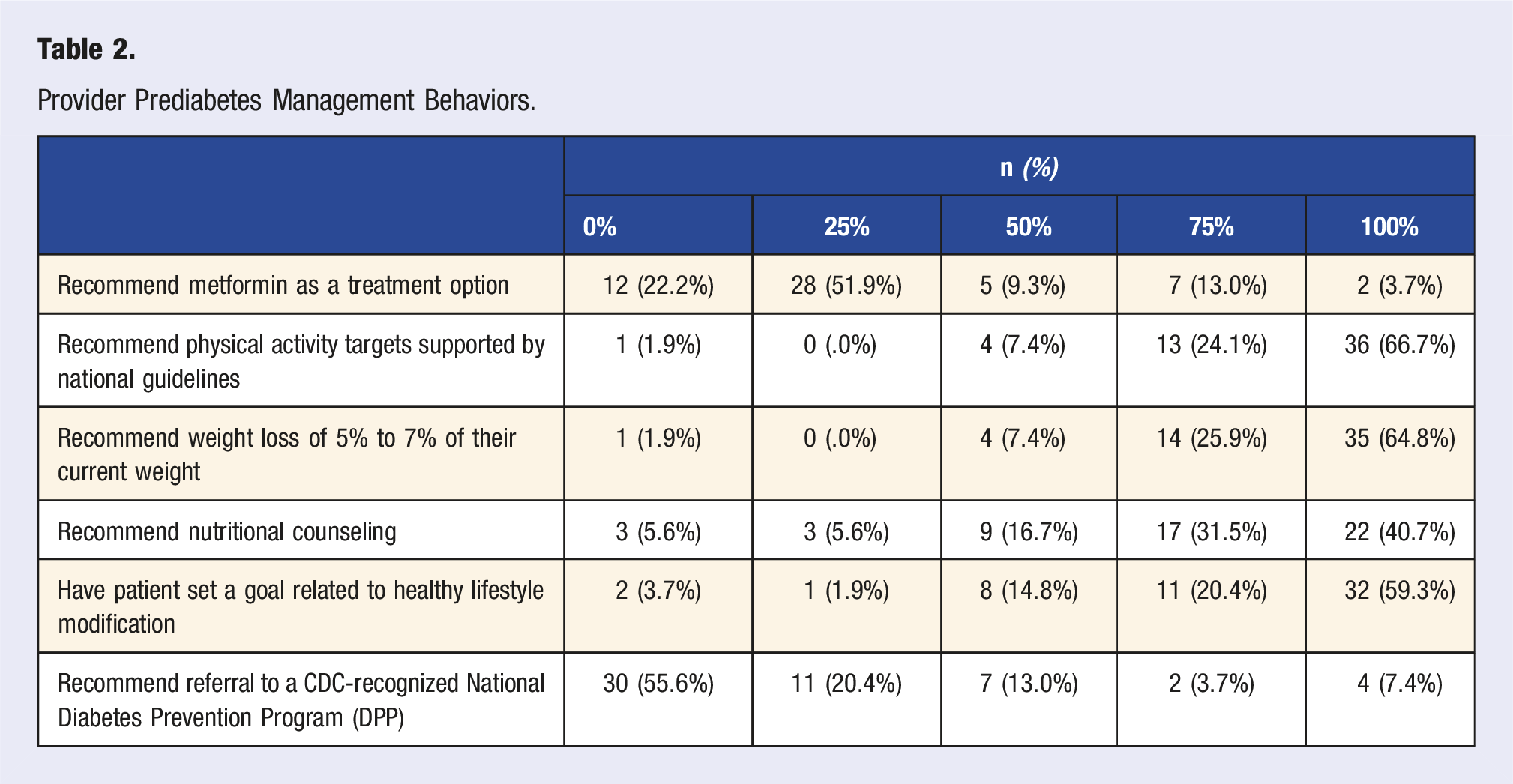
Provider Prediabetes Management Behaviors.
Barriers to Effective Prediabetes Management
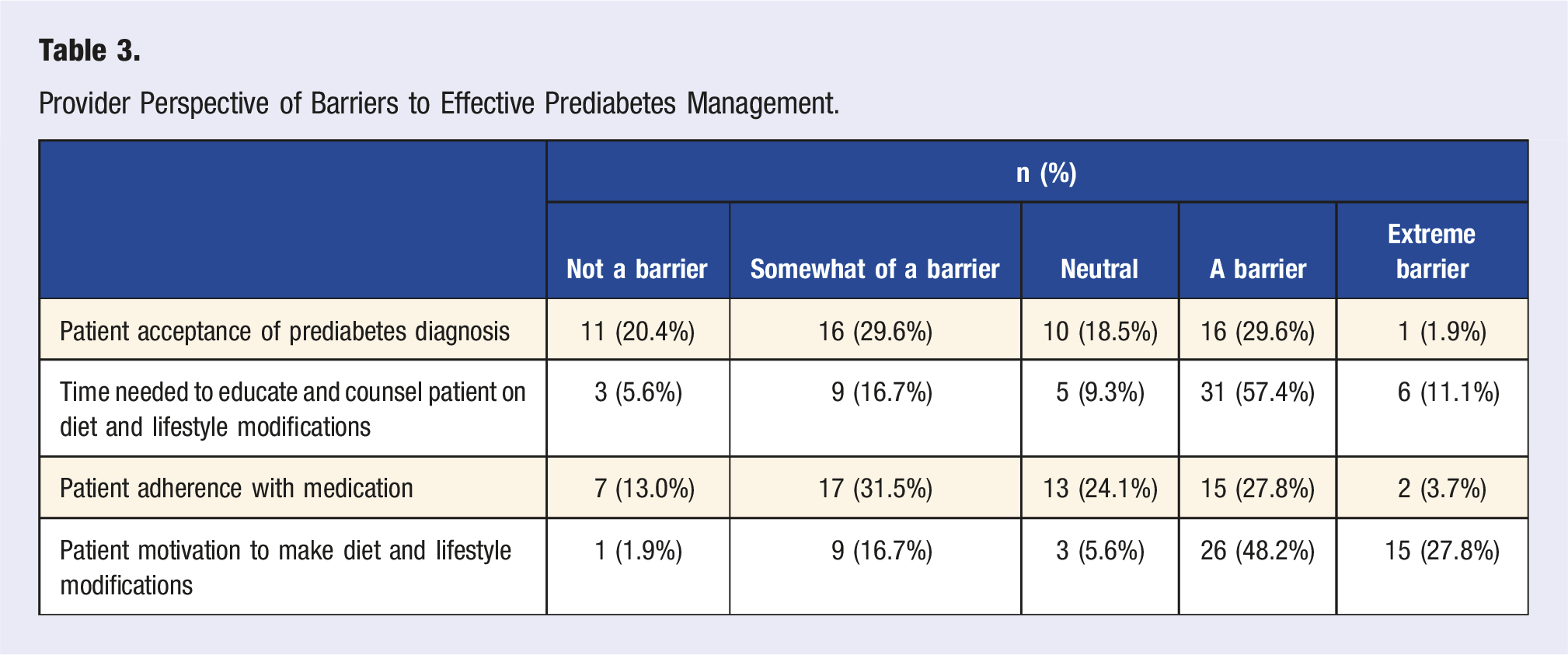
Provider Perspective of Barriers to Effective Prediabetes Management.
Patient Survey
Demographics
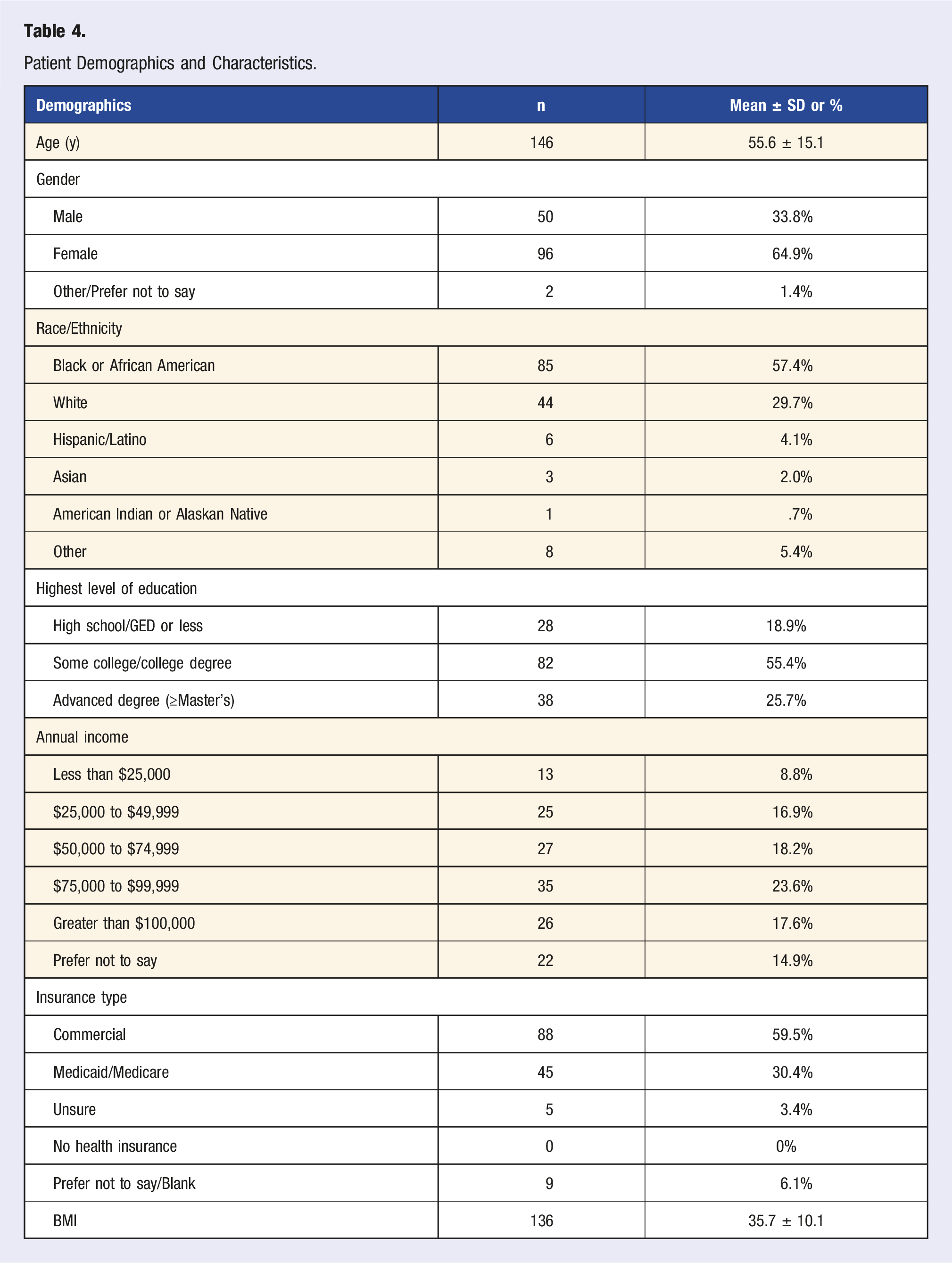
Patient Demographics and Characteristics.
Knowledge and Attitudes
Only about half of respondents reported being told they had prediabetes (59.2%) or were at high risk of developing T2DM (55.4%). Although 71.4% worry about getting T2DM, only 46.9% felt they were more likely to get T2DM compared to other people of their same age and sex. This data can be found in the Appendix (Exhibit D).
More than 90% of patients overestimated the rate of progression from prediabetes to T2DM within 1 year without treatment. Although most patients reported that diet and exercise changes and losing weight are effective to prevent T2DM, 65.5% did not know there is a medication available to help prevent T2DM.
The overwhelming majority (94.6%) felt it is important to know if you have prediabetes. Patients felt that having a diagnosis of prediabetes increases their understanding that they need to make healthy lifestyle changes (90.5% agree) and motivates these changes (84.2%). Most patients felt that they could control their risk of getting T2DM with diet and exercise changes (95.9%). About half (54.7%) would be open to taking daily medication to prevent T2DM.
For all knowledge and attitudes items, over half of those aware of their diagnosis (54.7%) felt they were more likely to develop T2DM compared to others of same age and sex vs 36.7% of those unaware (P = .043). Similarly, a larger majority (79.3%) of those aware of their diagnosis reported worrying about getting T2DM compared a smaller majority (59.3%) for those unaware (P = .032).
Treatment Experiences
Of patients who reported receiving recommendations on prediabetes management from their provider (n = 119), more patients were recommended for lifestyle changes (90.8%) or a weight loss program (32.8%) to manage prediabetes (Appendix, Exhibit E). Fewer reported that their provider had recommended a medication (14.3%) or referral to DPP (4.2%). For those who had been referred but were not enrolled in DPP, the majority had never received information on enrollment.
Thematic Analysis of Open-Ended Question
In considering ways the practice could improve prediabetes management, there were three major themes among providers and four major themes among patients.
Providers
Access and Availability to Nutritional and Physical Activity Support
Providers recommended having more nutritional support services, such as an embedded nutritionist or diabetes care and education specialist, and more support for physical activity, such as offering free exercise plans. “Embedded nutritionist(s) in major primary care practices. Cooking classes led by nutritionist.” “Have exercise/walking groups to hold people accountable.”
Access to the National DPP
Providers wanted improved access to the DPP and recommended a standardized easy referral process, education about local DPPs, and more availability for DPP sessions. “It would be very informative for us to have an introduction to DPP resources in our area and how to refer patients to those programs.” “Have more availability for sessions for the DPP program. Patients tell me they have to wait a long time to get enrolled.”
Develop In-House Programming
As an alternative to referral to national DPPs, many providers suggested developing in-house prediabetes programming, such as group visits or group classes. “Create a Centering group aimed at promoting lifestyle modifications and providing motivational and emotional support.” “Offer nutrition counseling groups/lifestyle modification groups that maybe meet once or twice, for patients who would be more willing to do that than the full DPP which is a longer program that might intimidate people. That way, patients have the option to have some extra counseling and then can decide if they want more.”
Only two providers suggested continued counseling on prediabetes during office visits with patients.
Patients
Education on Prediabetes
Respondents overwhelmingly asked for more education and information regarding prediabetes, including their diagnosis, risk of diabetes, and treatment options. “Be more explicit about the diagnosis.” “Educate on what having diabetes actually means and what interventions do in terms of impacting symptoms.” “Be more assertive in recommending effective methods for reducing risk for diabetes.” “Make people aware of available diabetes prevention programs and medications.” “Discuss pharmaceutical interventions to supplement lifestyle changes.” “Educate patients about programs and resources that are available, especially during doctor visits.”
Referral to Specialist or Programming
Patients requested referrals to specialists such as endocrinology or dieticians and referrals to prediabetes group programs and classes. “Have some kind of classes available so people will [know] the do’s and don’ts to prevent prediabetes.” “Referrals to dietary professionals.” “A program or support is needed to help patients like me to ensure I am doing the right thing.”
Provider and Clinic Support
Patients requested more support from their provider and the clinic, including more transparent communication, aggressive encouragement and counseling on treatment, and regular monitoring. “Give patient direct instructions on how to proceed!” “Actively encourage patients to aggressively pursue diet and exercise programs, and follow up on their efforts to do so.” “Continue to monitor my A1C.”
Education About Nutrition
Patients would like more information on nutrition and diet, with more specific recommendations, either with a fact sheet or with a nutritionist. “I would like an actual menu-based diet to follow for weight loss… just saying ‘Lose weight’ is not enough.” “Have a fact sheet showing what to eat, what exercises you can do to lose weight, and how many days and minutes you should exercise out of a week, etc.” “I think a nutritionist should be assigned to the patient to help them transition into a better healthy eating and lifestyle.”
Discussion
This study describes provider- and patient-reported prediabetes knowledge, attitudes, and experiences with prediabetes management in a large academic family medicine practice. The patient responses represent the largest survey to date of primary care patients with a diagnosis of prediabetes, and its large percentage of Black respondents provides findings on a population at particularly high risk of prediabetes. Our findings also highlight opportunities to improve prediabetes care in the primary care setting.
Our findings regarding provider and patient knowledge and attitudes about prediabetes are similar to those of prior literature. Most providers reported that screening for diabetes is a high priority. In line with Roper, et al., providers feel a prediabetes diagnosis is effective not only to increase patient awareness of needed lifestyle changes but also to motivate those changes. 14 Similarly, the majority of patients feel it is important to know about their diagnosis and that their diagnosis motivates behavior change, again consistent with previous studies. 16 Only half of patients reported having been told they had prediabetes or were at high risk for developing T2DM. This finding may reflect providers failing to discuss a prediabetes diagnosis, errors in patient recall, or labeling an elevated A1C with terms other than “prediabetes.” Given shared beliefs that diagnosis is important and effective but poor rates of patient awareness, our findings underscore a need to label prediabetes.
However, diagnosing prediabetes without clear counseling on the diagnosis and its risks may potentially lead to patients overestimating their risk of progression to T2DM, as was the case in our sample. This finding mirrors prior literature and indicates a need to not only inform patients of their diagnosis but to explain the nature of prediabetes and risk for progression. 16
Treatment options for prediabetes include physical activity targets, healthy diet, weight loss, and/or metformin. 21 Providers and patients surveyed were largely in alignment regarding the treatment options they either recommend or have been offered. Most providers regularly recommend exercise, weight reduction, nutritional counseling, and having the patient set a lifestyle goal, but a minority of providers recommend metformin or refer to DPP regularly. Prior studies also found that providers only have moderate knowledge of prediabetes management and low awareness of DPP. 10 While the majority of patients reported receiving a recommendation for lifestyle changes (diet and exercise), few were recommended for medication or DPP. In fact, many patients report not knowing about a medication available to help prevent T2DM. Recent studies have demonstrated major gaps in receiving counseling, treatment, and referrals to DPP for prediabetes management.22,23 Interestingly, despite providers not commonly recommending metformin, half of patients would be open to taking medication to prevent T2DM. Given the proven efficacy of and patient willingness to try metformin and DPP, providers should counsel patients on all available treatment options.
Providers’ perceived barriers to effective prediabetes management may contribute to poor patient awareness of their diagnosis and knowledge of management options. Providers reported that the biggest barriers were patient motivation to make lifestyle changes and the time needed to educate and counsel patients on lifestyle changes, consistent with a previous physician survey. 6 If providers feel they do not have enough time, and that patient motivation is a major barrier, they may not be intentional, thorough, and clear in explaining to patients their prediabetes diagnosis and management and providing counseling.
Interestingly, the majority of patients reported that having this diagnosis motivates them to make lifestyle changes. Similar to findings from O’Brien et al., 16 patients considered both lifestyle interventions and metformin as acceptable treatments. Given the discrepancy between provider perception of patient motivation and patient self-reported motivation levels, using motivational interviewing to assess a patient’s readiness for change could help identify those patients who are in the “preparation” or “action” stages and ready to implement changes.24,25
Findings from our open-ended question further emphasize the need to better counsel patients on prediabetes. The overwhelming majority of patients simply wanted more education on prediabetes, asking providers to be more explicit about the diagnosis, thorough in reviewing management options, and more assertive and specific in offering recommendations. In contrast, only two providers suggested counseling on prediabetes during office visits. Additionally, patients requested more support from the clinic and their provider, including more aggressive encouragement and regular monitoring. Providers, however, did not suggest additional provider counseling or direct provider support. This may be because providers feel they are doing an adequate job in counseling and supporting their patients or because providers, as discussed earlier, feel they do not have time to do this. Regardless, our data show that patients currently feel they receive inadequate counseling and education around their diagnosis, risk of progression, and management options, consistent with previous literature.14,26
One way to address provider concern for time and patient desire for more education on the diagnosis, risk, and treatment options include using a shared decision aid. A prediabetes shared decision aid has been shown to be feasible, time-effective, and successful in promoting treatment adoption. 27
Both providers and patients voiced a strong need for more instructional nutritional support. Providers suggested having embedded nutritionists while patients asked for fact sheets and menu-based counseling for weight loss. Another area of patient-provider alignment was the possibility of special programming, such as DPP or non-DPP group classes. Given that providers feel time is a major barrier, it is logical that most suggestions offered by providers utilize others to educate and support patients with prediabetes. Implementing the use of non-physician and non-advanced practice providers to support patients with prediabetes has been effective. Peer support programs, use of community health workers, and medical nutrition therapy delivered by dietitians have been shown to be promising.28-30 Other strategies to better support patients include interventions to increase referral to DPP or innovative adaptions of DPP to reduce barriers to treatment.31-33
Strengths of this study include a strong survey response rate among providers and a fair survey response rate among patients. In addition, our study captured both provider and patient perspectives, with both quantitative and qualitative data. Providers with a wide range of experience were represented. Patient participants were diverse in terms of race/ethnicity, education, and income levels. However, the patient survey only included English-speaking patients who are active users of the patient portal. Additionally, our findings may be affected by self-selection bias, recall bias, and social desirability bias. Lastly, our study was conducted at a single clinical site, which may limit generalizability.
Conclusions
Primary care providers and patients both agree that prediabetes diagnosis is important and motivates lifestyle changes. Despite this, patients often are unaware of their diagnosis. Lifestyle modifications are most commonly recommended for patients diagnosed with prediabetes but patients are generally unaware of other treatment options such as referral to DPP or metformin. In our practice, patients are requesting more education on their diagnosis, explanation of all treatment options, and nutritional support. Our findings suggest multiple interventions to improve prediabetes care: increasing provider and patient knowledge on all treatment options, encouraging shared decision-making for patient-centered management, and expanding access to nutrition and prediabetes education resources. These interventions will likely require support of other care team members. In our practice, based on our findings, we have since provided clinician education on current clinical guidelines, developed and disseminated patient education materials on prediabetes, and developed a clinical toolkit for diabetes prevention. Further research is needed to evaluate these interventions and assess the impact on clinical outcomes.
Supplemental Material
Supplemental Material - Patient and Provider Prediabetes Knowledge, Attitudes, and Behaviors in a Large Urban Family Medicine Practice
Supplemental Material for Patient and provider prediabetes knowledge, attitudes, and behaviors in a large urban family medicine practice by Erica Li, MD, MSc, Alexa Waters, MD, Amy Cunningham, PhD, MPH, Alexis Silverio, MPH, Jasmine Han, and Geoffrey Mills, MD, PhD in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors acknowledge the essential contributions of providers and patients who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.