
Abstract
Diabetes is a major public health problem that affects certain ethnicities disproportionately. Physical activity (PA) (exercise) is a key component necessary for the prevention and treatment of type 2 diabetes. Adults with and without diabetes may face challenges that interfere with following exercise recommendations. This article reviews the relationships among PA, race/ethnicity, behaviors, and health outcomes of adults with prediabetes and type 2 diabetes. The authors review recent cross-sectional and intervention studies and assess their relevance to clinical practice. This is a focused review of the literature from January 2010 to September 2012 on the relationship among PA, type 2 diabetes, and race/ ethnicity with respect to the following components: (1) PA and the likelihood of persons with prediabetes developing diabetes; (2) PA and improvements in health outcomes of persons with prediabetes; (3) PA and improvements in health outcomes of persons with type 2 diabetes; and (4) enablers of and barriers to PA for persons with type 2 diabetes. The initiation of effective PA programs designed to reduce the incidence of type 2 diabetes or improve diabetes outcomes rely on a critical interpretation of current research findings.
Although physical activity (PA) is fundamental for the management of type 2 diabetes and may help delay the onset of diabetes, individuals with diabetes face considerable challenges, both psychosocial and biophysical, that may interfere with following exercise recommendations.
Introduction
Diabetes is a worldwide epidemic, primarily because of the increase in prevalence of type 2 diabetes (90%-95% of the cases of diabetes) and is estimated to affect 25.8 million people (8.3%) in the United States; it disproportionately affects blacks, Hispanics, and Asian Americans. 1 Diabetes is the seventh leading cause of death in the United States, and persons with diabetes are twice as likely to die from cardiovascular diseases compared with their counterparts. 1 Although physical activity (PA) is fundamental for the management of type 2 diabetes and may help delay the onset of diabetes, 2 individuals with diabetes face considerable challenges, both psychosocial and biophysical, that may interfere with following exercise recommendations. According to the Office of Vital and Health Statistics, only 21.9% of US adults engaged in light to moderate PA 5 days per week, whereas 39.7% do not participate in any leisure PA. 3 Higher physical inactivity was reported for individuals with diabetes (42%) as compared with those free of diabetes (27%), based on a representative population from a state survey in South Carolina. 4 PA level was negatively correlated with having diabetes, adjusting for age, gender, and race/ethnicity in a nationally representative sample. 5 Figure 1 depicts the percentage of adults at risk for diabetes, with diabetes, and without diabetes who engaged in PA (at least 30 minutes of moderate or vigorous exercise at least 3 times per week), based on a nationally representative sample. 6 A higher percentage of adults (65%) without diabetes and at a minimum risk for diabetes exercised or performed PA as compared with adults with diabetes (38%) who performed PA. 6 As risk factors for diabetes increased (advanced age, overweight, ethnic minority, hypertension, and family history of cardiovascular disease), the percentage engaged in PA decreased for those free of diabetes. 6
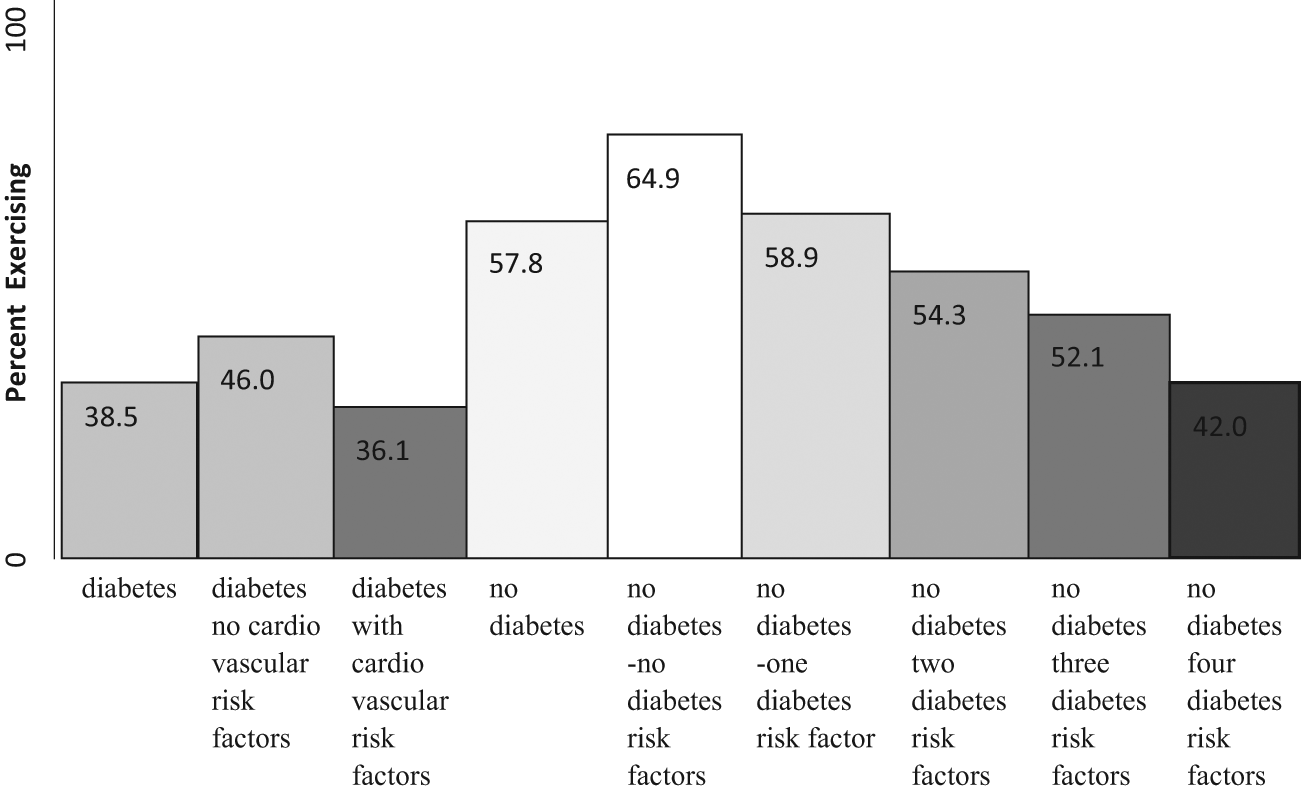
Percentage of US adults reporting moderate/vigorous exercise for 30 minutes at least 3 times per week, by diabetes statusa.
PA has been considered a modifiable risk factor of diabetes and diabetes outcomes; yet the relationships among PA, diabetes risk, diabetes outcomes, and race/ethnicity have not been established. Moreover, summary of findings from recent studies are necessary to determine the direction of efforts that are most likely to contribute toward a reduction in the incidence of diabetes and improvement in diabetes health outcomes. Of particular interest are studies that measure these relationships by race/ethnicity. We conducted a focused review of the literature from January 2010 to September 2012 on the relationship among PA, type 2 diabetes, and race/ethnicity with respect to the following components: (1) PA and the likelihood of persons with prediabetes developing diabetes, (2) PA and improvements in health outcomes of persons with prediabetes, (3) PA and improvements in health outcomes of persons with type 2 diabetes, and (4) enablers of and barriers to PA for persons with type 2 diabetes.
PA and Developing Type 2 Diabetes
Individuals who have an elevated risk for developing type 2 diabetes include children and adults with a family history of diabetes; persons with cardiometabolic risk factors such as obesity, high triglycerides, high low-density lipoprotein cholesterol (LDL-C), low high-density lipoprotein cholesterol (HDL-C), high waist circumference, and high mean arterial pressure; and persons diagnosed with prediabetes, defined as a hemoglobin A1c level above normal but below the classification for diabetes by the American Diabetes Association—5.7% to 6.4% or a fasting blood glucose level of 100 to 125 mg/dL. 7 PA has been implicated in the development of type 2 diabetes for several populations, throughout the literature, by observational and prospective studies (Figure 2).
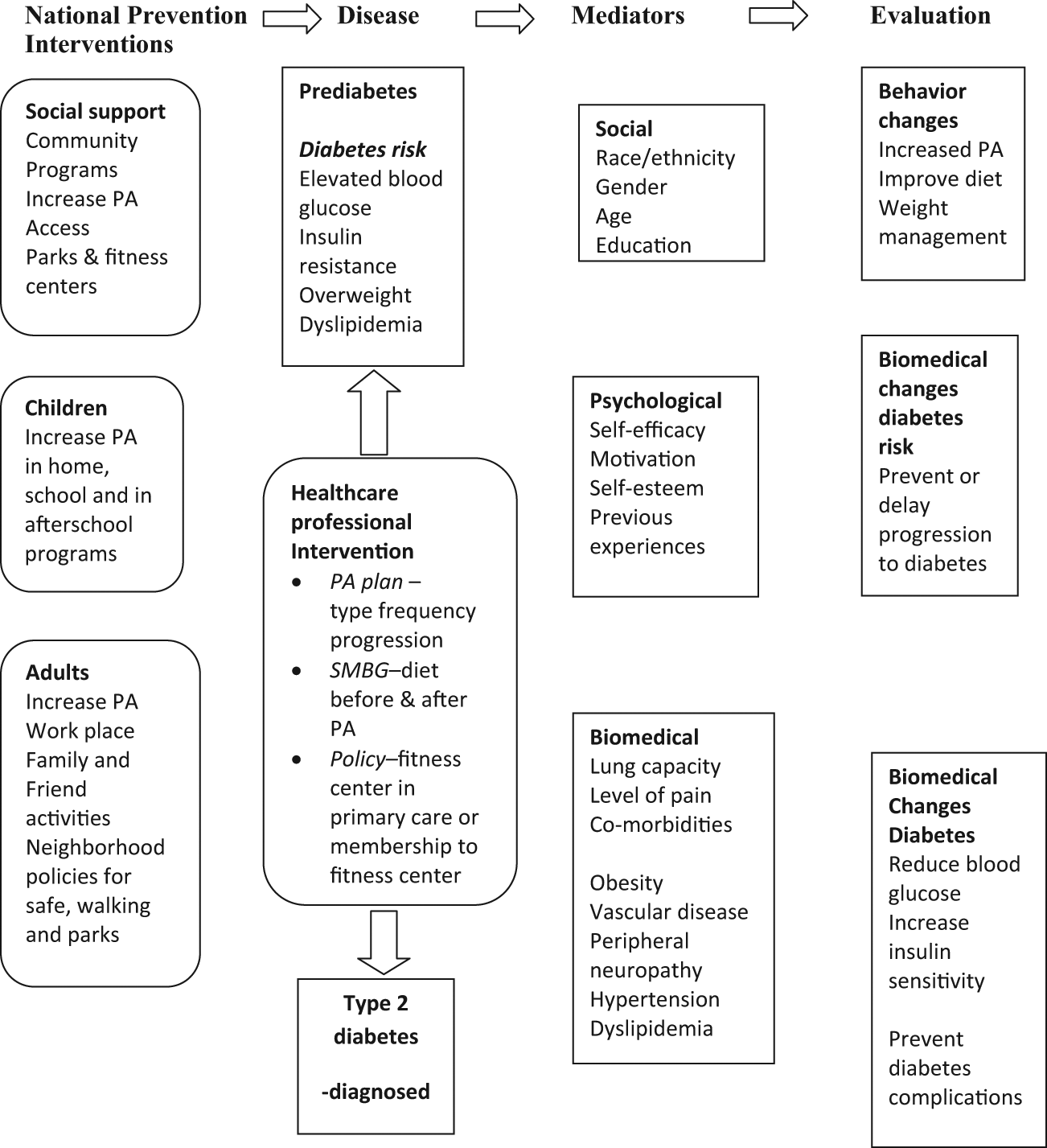
Points of intervention: physical activity (PA) and type 2 diabetes.
Single-Time-Point Studies of PA and Diabetes Risk in Children and Adults
Few studies measure PA with prediabetes in children by race/ethnicity. PA has been associated with a reduction in cardiometabolic risk in children. 8 The authors reported that PA may be protective for prediabetes in cases of high adiposity, based on a metabolic syndrome risk score in a cross-sectional study of 46 boys and girls aged 7 to 12 years. 8 On the other hand, there are several studies on adult populations associating PA with prediabetes (refer to the section “Prospective studies of PA with impaired fasting glucose and diabetes,” below). A cross-sectional study found a gender interaction with metabolic syndrome and PA. 9 The odds of having metabolic syndrome with physical inactivity was significant for men—odds ratio (OR) = 2.27; confidence interval (CI) = 1.22, 6.29—after adjustments but not for women— OR = 1.95 (0.85, 4.45)—in a Japanese cohort (n = 483) aged 30 to 64 years. 9 This study indicated that the relationship between PA and cardiometabolic risk may vary by age and gender. What is missing in the literature are studies comparing PA and metabolic risk factors for type 2 diabetes by race/ethnicity. Recent evidence suggests that race/ethnicity genetic differences, measured by ancestry informative markers for African American and Hispanic women, were associated with differences in common obesity indicators—BMI and waist and hip circumferences—whereas, there were no race/ethnicity differences in the waist-to-hip ratio. 10 The investigators concluded that the waist-to-hip ratio may be a better obesity indicator because their findings agree with an earlier study in Chinese adults. 10 Considering the evidence from earlier studies, PA has been recommended by the American Diabetes Association as a means of preventing type 2 diabetes; however, the amount, type, and level of PA may differ across races/ethnicities and may be confounded by family history of diabetes, age, and gender. 7
Prospective Studies of PA with Impaired Fasting Glucose and Diabetes
Lower levels of PA have been associated with a higher risk of developing diabetes across all strata of obesity levels in adults of different nationalities. A lower 5-year risk of incidence of impaired fasting blood glucose was associated with higher PA, measured by total steps for an Australian population of 11 247 adults aged ≥25 years. 11 The investigators suggested that every 1000 step increment was associated with a 13% lower likelihood of the 5-year incidence of impaired fasting blood glucose. 11 A major strength of this study was the use of an objective measure of PA over a relatively long time period (5 years). Moderate- to vigorous-intensity PA at least once per week was associated with a reduced risk of developing type 2 diabetes based on a national sample of English adults (n = 7466) aged ≥50 years; however, PA was self-reported and could have been over- or underestimated. 12 The incidence of diabetes was lower for a cohort of obese US adults (n = 1826), initially free of cardiovascular disease and diabetes, in the upper 3 quartiles of steps per day compared with the lowest quartile. 13 After a 2-year follow-up of adults initially free of diabetes from the United States and Canada, those who were newly diagnosed with diabetes were more likely to be black, have a higher BMI, report smoking, be less physically active, watch more television, and obtain less sleep. 14 Spanish individuals with impaired fasting blood glucose, aged 45 to 75 years, who were administered a lifestyle intervention that included PA had a 8.9 case per 100 incidence of diabetes as compared with the standard care group, with 13.4 cases per 100. 15 Both interventions included dietary and PA recommendations; therefore, the effect of PA could not be separated from dietary effects. The risk for developing type 2 diabetes was less for those whose total PA was equal to or greater than 150 minutes per week as compared with those with less than 150 minutes per week for Chinese adults. 16 This study compared groups by family history of diabetes and used the International Physical Activity Questionnaire, an appropriate PA questionnaire, validated for their population. The relative reduction in the risk of type 2 diabetes over the course of 16 years was lowered by 13% for men and 7% for women, with an increase in PA energy expenditure of 460 kJ/d (110 kcal/d) for men and 365 kJ/d (87.2 kcal/d) for women. 17 This represented a 1-category increase in PA, based on 4 possible levels of PA for a case-cohort study across 8 Northern European countries. 17 To its merit, this European study collected data on a large sample (n = 346 055) of a homogeneous population (primarily Caucasian). PA was by self-report, and the resulting categories (inactive, moderately inactive, moderately active, and active) were based on answers to 3 questions of PA over a 12-month period from a validated questionnaire. As such, the quantification of PA into an energy expenditure of kilojoules per day produced estimates, at best, and may be biased by sociodemographic factors. The investigators found that hazard ratios for diabetes were higher for physically inactive men and women across all strata of BMI. 17 Many of these studies suggest that PA plays a role in the prevention of prediabetes and type 2 diabetes; however, inconsistencies in the measurement of PA and combining multiple lifestyle recommendations make comparisons between and within race/ethnicity challenging. For example, measuring steps does not take into account aerobic effort. Moreover, it is not known what modality and level of PA (high, moderate, or low-impact aerobics and/or strength training) may be more effective for certain populations.
Applications of PA Interventions to Primary Care
A review of the major lifestyle intervention trials aimed at reducing the incidence of type 2 diabetes by the innovators of the Finish Diabetes Prevention Study suggests that US adults with impaired fasting glucose may lower their risk for type 2 diabetes nearly 50% by following dietary and PA recommendations but that translating trials to clinical practice may be challenging. 18 Improvements in exercise and biomarkers were also not evident when comparing community lifestyle programs with standard care in a retrospective study of persons with prediabetes or type 2 diabetes in a Dutch population. 19 The authors conclude that measures to improve adherence to dietary and PA recommendations necessary for glycemic control are not apparent in community primary care settings and that implementation will be a challenge. 19
PA and Health Outcomes of Persons with Prediabetes
In an effort to address the obesity epidemic and related health issues, numerous observational and intervention studies have been performed on children and adults, measuring biometric and behavioral outcomes. Of late, several studies have been conducted on minority populations in the United States and in Europe. A nutrition education program that promoted PA improved insulin resistance and inflammatory outcomes in a prospective study of Asian Indian adolescents. 20 Compared with the control group, those receiving a parent-involved, individual counseling, school-based nutrition/PA education program had smaller waist circumferences, improved β cell function, and lower C-reactive protein (systemic inflammation). 20 Voluntary participation in PA improved in a predominantly African American and Hispanic cohort of physician-recommended, obese children (aged 10-14 years) by a 12-week, social cognitive theory–based intervention. 21 The investigators reported improvements in self-efficacy that were associated with increases in PA (days per week with the recommended 60 minutes of PA). 21 Partly because of the small sample size (n = 23), biomarkers, such as lipids, BMI, and glucose/insulin ratio correlated in the expected direction with PA but did not reach statistical significance. 21 A community participatory action model and pilot study for diabetes prevention in low-income, immigrant Hispanics showed a statistically significant improvement in lowering BMI (by 0.2 kg/m2) for the intervention group as compared with the control group. 22 By the researchers’ own admission, the change was modest 22 ; however, the increase in PA, encouraged by community peer leaders, may have longer-reaching effects.
Although the finding for PA and health outcomes for minorities with prediabetes support community participation and peer leader strategies, few studies have been conducted testing these strategies in Caucasian cohorts. For a northern European cohort at risk for diabetes, there were no improvements in aerobic capacity by either the physician-coached arm or the combined physician-coached plus group intervention arm. 23 Although PA training and motivational counseling was included, both approaches were conducted by health care professionals and did not include peer leaders. 23
Apart from the method and type of lifestyle counseling, there is a question as to what is most effective for glycemic control in adults with prediabetes: exercise, calorie restriction, glucose-lowering drugs, or a combination of all treatments. Coker et al 24 found that exercise with weight loss improved glucose metabolism (hepatic and peripheral insulin resistance) and reduced visceral fat more than comparable weight loss without exercise in a randomized control trial of obese, older adults (aged 50-80 years) free of cardiovascular disease or diabetes. A 12-week intervention with exercise and calorie restriction (500 kcal/d) improved free fatty acid–induced hepatic insulin resistance in obese adults with impaired glucose tolerance. 25 The comparison group maintaining a eucaloric diet with exercise did not have any improvement in free fatty acid–induced hepatic insulin resistance. Their results suggest that both exercise and lowering calorie intake may prevent lipid accumulation in the liver for northern European adults with prediabetes. 25 Improvements were found in insulin sensitivity regardless of treatment arm in a randomized control 12-week intervention comparing (1) antihyperglycemic medication alone; (2) exercise training with medication; and (3) exercise training with placebo in a primarily Caucasian cohort of US adults with prediabetes. 26 Generalizations of these findings suggesting the equality of medication with exercise for adults with prediabetes should be made with caution; particularly because the sample size was small (n = 27, approximately 8 per group) and the participants were mostly Caucasian (with 3 African Americans and 2 Hispanics). 26 The current literature indicates that PA has a role in the improvement of biomarkers for persons with prediabetes; albeit, the specifics regarding the modality, duration, and frequency of PA; the combination of PA with diet and medication; and these benefits for different race/ethnic populations remains unclear.
PA and Health Outcomes of Persons with Type 2 Diabetes
The promotion of glycemic control is one of the main reasons why PA is vital to maintaining health for persons with type 2 diabetes. Glycemic control is measured by percentage of glycated hemoglobin (A1C), where A1C < 7.0 is considered good glycemic control for persons with diabetes. 7 Earlier, prospective studies have established that glycemic control is inversely associated with microvascular and macrovascular complications for persons with insulin-dependent (type 1) 27 and type 2 diabetes. 28 An overly tight control of A1C, below 6.0%, was shown to be associated with increased mortality in the Actions to Control Cardiovascular Risks in Diabetes (ACCORD) trial, which led to a discontinuation of the intensive treatment arm. 29 The results of this trial and others suggest that severe glycemic control may lead to hypoglycemia and large variability of blood glucose, which are predictors of cardiovascular events and mortality. 30 PA may play a role in glycemic control measured by postprandial glucose. It was found that 7 days of aerobic training reduced glycemic variability and postprandial glucose with no change in fitness or adiposity in 13 sedentary, overweight volunteers with type 2 diabetes. This study was promising; however, long-term studies with larger sample sizes across race/ethnicity are needed. 30
There are several mechanisms by which PA aids glycemic control. PA can reduce free fatty acid–induced hepatic insulin resistance, which has been shown in obese adults with impaired glucose tolerance.24,25 Another means by which PA facilitates glycemic control is by facilitating skeletal muscle glucose uptake and use. PA increases the production of glucose transporter 4 (GLUT4) and increases muscle insulin sensitivity. As such, PA has been considered a treatment option for type 2 diabetes. 31 In addition to obesity, metabolic syndrome, a cluster of cardiovascular risk factors, is prevalent in persons with type 2 diabetes. Metabolic syndrome has been defined by the International Diabetes Federation as the presence of central obesity plus 2 other cardiovascular risk factors in areas of abnormal glucose and insulin metabolism, dyslipidemia, and hypertension. 32 Although PA interventions have measured health outcomes for persons with diabetes, few have compared persons with both type 2 diabetes and metabolic syndrome.
In an elderly cohort of Japanese adults with type 2 diabetes, lack of PA has been associated with higher prevalence of metabolic syndrome. 33 PA has been shown to have an anti-inflammatory effect for a modest cohort (n = 82) of Italians with type 2 diabetes and metabolic syndrome. Greater reductions in C-reactive protein and interleukin-6 were found for the high-intensity aerobic and resistance trained group as compared with the sedentary group, independent of weight loss. 34 This study clearly delineated the modalities of exercise counseling into 4 groups: no counseling; low-impact aerobics; high-intensity aerobics; and both high-intensity aerobics and resistance training. 34 The study estimated energy expenditure at baseline by self-report; however, energy expenditure was measured by exercise equipment workload, time, and standard equations. 34
Much of the focus of recent PA interventions has been on reducing sedentary behavior and improving diabetes outcomes in populations of several nations, regardless of baseline metabolic characteristics. The quality of life was positively associated with increasing exercise volume (metabolic equivalence per hour per week) for Italians with type 2 diabetes in a 6-month, randomized controlled trial of counseling with supervised exercise versus counseling only. 35 To their credit, the investigators used both aerobic and resistance training and quantified participants’ efforts by standard equations used to calculate maximal oxygen consumption.
In a cohort of 64 Korean women with type 2 diabetes enrolled in a 12-week intervention, improvements in insulin sensitivity and visceral fat area were observed for the PA and diet and PA groups only but not in the control group. 36 Improvements in A1C were found in the diet and PA interventions groups as compared with the control group. 36 On completion of the study, 45% in the diet group, 57% in the diet and PA group, and 5.6% in the control group were able to reduced or stopped diabetes medications were possible. 36 The reduction of diabetes medication for the PA without diet group (15.4%) was not statistically different from the control group. 36 The PA component of this study, brisk walking for 120 minutes, every day, was first taught by a professional exercise therapist who demonstrated the procedure to the participants. 36 A professional dietitian counseled the diet and diet and PA groups to reduce their energy intake to 1200 kcal/d. 36 Although the study showed significant health benefits, it lacks a follow-up to test adherence to dietary and PA recommendations. Maintaining these dietary restrictions and time effort for PA beyond the 12-week study may have been unrealistic in free-living Koreans.
Another study that compared PA or PA/diet and glycemic outcomes was the Early Activity for Diabetes randomized controlled trial (Early ACTID). 37 This 12-month trial was performed on English adults aged 30 to 80 years for whom diabetes was newly diagnosed (5-8 months) in 3 arms: usual care, diet, and diet plus PA. 37 The PA component for ACTID was brisk walking for 30 minutes, 5 days per week (150 min/wk) as opposed to 850 min/wk for the Korean study. In agreement with Koo and colleagues’ study of Korean women, 36 results from the ACTID trial showed that A1C and insulin resistance improved, and use of diabetes medications were reduced for the diet and diet plus PA groups. 37 The investigators concluded that PA added no additional benefit to the intense dietary component where 5% to 10% of body weight was lost. 37 Albeit, A1C, insulin resistance, and BMI yielded better results for those participants with higher as compared with lower baseline values. 37 The role of PA during weight maintenance has yet to be established for this cohort.
A 12-week self-monitoring lifestyle intervention in German adults aged ≤75 years in the overweight or obese category (BMI ≥ 27) and with type 2 diabetes resulted in modest but significant improvements of A1C (−0.2, −0.3), weight (−1.8, −2.3), systolic blood pressure (−2.6, −3.0), diastolic blood pressure (−1.8, −5.2), and LDL cholesterol (−3.6, −5.9) for all participants and for completers, respectively. 38 The intervention involved staff contact of less than 1 hour of total contact time spread over 4 telephone calls. 38 Materials provided included a manual, tape measure, step counter, and glucose meter with test strips. 38 By self-report, participants increased their steps per day as well as PA level from baseline to completion. 38 Limitations of the study were having no control group, exclusion of individuals with no experience in self-monitoring blood glucose, and lack of follow-up. 38 Moreover, weight loss and consequent biomarker improvements attributed to diet and PA changes could not be distinguished in this study. To its merit, this type of intervention is low cost ($200 per participant as estimated by the investigators 38 ) as compared with lifestyle interventions that have in-person counseling professionals.
There is some evidence that a counseling intervention for diabetes self-management that includes a PA component may reduce diabetes complications. A randomized control trial of a lifestyle intervention versus usual care for Japanese adults aged 40 to 70 years with type 2 diabetes followed for 8 years demonstrated a 40% lower incidence of stroke for the intervention as compared with the control group. 39 Although there were no differences in total energy or fat intake between the groups, there was a significantly higher level of PA attributed to the sports/exercise component but not work or leisure activities for the intervention group. 39 There were no differences in the occurrence of coronary heart disease or the progression of retinopathy or nephropathy between the groups. 39 The investigators attribute the limited effect of the intervention in most diabetes outcomes to counseling by a diabetes educator received by the control group as a part of usual care. 39 By the authors’ admission, setting goals for each patient and measurement of their percentage change may have been a better indicator of success than having a group goal. 39
Although type 2 diabetes is rising in younger populations, there are few studies conducted on PA among youth with diabetes. Guillory et al 40 investigated the association of PA with glycemic control in primarily black (42.7%) and Hispanic (44.0%) youth aged 9 to 17 years diagnosed with diabetes within the past 6 months. The investigators used A1C > 8.0% as inadequate glycemic control; however, they found no association with PA and glycemic control. 40 Limitations of this study were its small sample size, cross-sectional nature, and measurement of PA by self-report rather than using objective measures such as those obtained with accelerometers. 40 An intervention study may have been more appropriate because neither group met the recommended level of PA.
Perceived Enablers of and Barriers to PA for Persons with Type 2 Diabetes
Perceived enablers are positive or predisposing factors that initiate and sustain behavior change. 41 Conversely, perceived barriers are negative beliefs that the recommended health behavior is not worth the benefits. 42 In the past several years, there have been an abundance of descriptive studies, including qualitative (focus group interviews), quantitative (cross-sectional studies), and mixed methods (open- and closed-ended questions); interventions; and randomized controlled trials centered on understanding the types of enablers of and barriers to PA for people with diabetes. From these studies, several areas of focus have emerged, including sociodemographics (race/ethnicity, age, gender, and BMI), type of PA (aerobic or resistance training), biomedical barriers, and competition with PA—sedentary activities.
Race/Ethnicity and Sociodemographic Factors as Barriers to PA
African Americans participating in a cross-sectional study of cardiometabolic risk factors in ethnic minorities, who had type 2 diabetes reported performing less PA over a 12-month period than those without diabetes. 43 Sedentary behavior, such as television watching was associated with poorer diet and lower PA. 43 Several studies have targeted African American women in an effort to uncover their enablers of and barriers to engaging in PA as part of diabetes self-management.44-46 In an exploratory, mixed method study of 25 African American women, barriers to PA included not having an exercise partner, unsafe neighborhood, and biomedical problems such as pain from joints and diabetic neuropathy. 44 Free exercise classes, participating in PA with friends, and yard work were enablers for PA for those who participated (20 out of 25). 46 Social support emerged as an enabler, whereas altruistic intentions (greater concern for the health of family than self) and lack of motivation were barriers uncovered by a focus group interview of underactive, urban, African American women. 45 Overall physical environment barriers, including traffic, lack of sidewalks, lack of places to exercise, inadequate street lights, and lack of safety from crime were negatively correlated with PA frequency for a midwestern sample of 50 African American women with type 2 diabetes. 46 For the same sample, self-efficacy for PA and family social support were positively correlated with PA frequency.
Certain enablers and barriers found for African American women may be universal for women of other race/ethnicity. Because the altruism theme together with lack of enjoyment of PA facilities and limited time were cited as barriers to PA for women in earlier studies, Allen et al 47 developed a problem-solving 12-week intervention to increase PA for a cohort of primarily Caucasian women (n = 29) with type 2 diabetes. Women between the ages of 30 and 65 years, with a known history of type 2 diabetes, able to walk 0.25 miles in 10 minutes, and exercising less than twice a week were randomly assigned to either general diabetes education (control group) or enhanced diabetes education (intervention group). 47 Both groups received 90 minutes of general diabetes education, and the enhanced diabetes education group received an additional 90 minutes of problem-solving counseling. 47 The investigators found that both groups increased their PA counts (measured by an activity monitor as a product of frequency and intensity per unit time); however, there were no significant differences between the 2 diabetes education groups, and neither group met PA recommendations of 30 minutes most days of the week. 47 The following limitations of this study were confirmed by the authors: underpowered to detect differences in self-efficacy, duration too short to determine the effect of problem-solving skills over time, and the exclusion of the majority of interested participants who did not meet the inclusion criteria. 47
Viva Bien was a 12-week intervention that aimed to improve lifestyle behaviors and consequent biomarkers of diabetes for US-born women of Latin origin (Latinas; n = 280), 30 to 75 years old, diagnosed with type 2 diabetes (6 months or more). 48 The main objective was to improve psychosocial variables of problem solving. 48 Participants were randomly assigned to usual care (control) or usual care plus the intervention. 48 Although the intervention group had significant improvements in PA (measured by exercising more days of the week) compared with the control group, these differences were not maintained at 12 months. 48 Changes in PA significantly correlated with self-efficacy (r = 0.15) at 6 months; yet the correlation was no longer significant at 12 months (r = 0.02). 48 The strength of this study was the adaptation of an intervention that was successful for Caucasian women by taking into account sociocultural, environmental, and economic factors unique to Latinas. 48 The enablers and barriers for this sample were not assessed, which is a limitation of the study. 48 The authors suggested examination of enablers and barriers that may act as mediators or moderators of behavior change in designing interventions. 48
Mediators of PA, including social support, self-efficacy (in general and toward PA), enablers of and barriers to PA, decision making, goal setting, coping with relapse, and problem-solving strategies, were examined after a 24-month randomized controlled trial in Caucasian adults (n = 92) with type 2 diabetes. 49 The objectives of the telephone counseling versus printed material (usual care) intervention were to positively change psychosocial correlates and to increase PA, as measured by a pedometer (steps/d), an accelerometer (min/d), and a PA questionnaire validated for the Dutch population. 49 Residualized change in PA and psychosocial correlates were used to measure the proportion of the intervention effected mediated by each psychosocial factor. 49 Although several psychosocial factors mediated PA postintervention, different mediators influenced PA 1 year after the intervention (at follow-up). 49 The authors found that the mediators were dependent on the type of PA. 49
A randomized control trial aimed at increasing PA for women who were overweight and 9% of whom had type 2 diabetes was Sisters Taking Action for Real Success (STARS), a behavioral, social support intervention in disadvantaged neighborhoods, which served a primarily African American population. 50 Participants were young adults (aged 25-50 years) who were not taking insulin or had uncontrolled hypertension. 50 This intervention is ongoing for 3 cohorts, and the components were based on the findings of focus groups for PA and healthy eating. They were (will be) randomly assigned to either the intervention group (in-person group education sessions) or the control group (educational mailings). 50 The study arms each received (will receive) 4 weeks of individual counseling and 16 weeks of education sessions (either in person or by mail). In addition, the intervention group received 8 weeks of telephone counseling. 50 The control group was (will be) given the treatment after the study. 50 PA was calculated by metabolic equivalents (METs) from measurements of an accelerometer worn on the participants’ right hip for 7 days. 50 Major barriers for PA addressed for STARS were competing responsibilities, lack of access to safe exercise places, low motivation to exercise, and fear of ridicule because of body size while exercising.
Alberta Diabetes and Physical Activity Trial (ADAPT) is another ongoing PA randomized trial for adults with type 2 diabetes (n = 287). 51 The 12-month trial aims to reach Canadian adults (primarily Caucasian) in a 3-arm design: standard care (Canadian Diabetes Association PA information), enhanced materials (stage-of-change-matched PA, pedometer, and activity log), enhanced plus telephone counseling (4 weekly calls for the first month, biweekly for the next month, and monthly for the duration). 51 The trial will measure PA behavior change and clinical markers to determine the efficacy of a low-cost intervention that incorporates psychosocial determinants. 51 The findings from this study may not be applicable to adults with type 2 diabetes of other races/ethnicities, even if positive results are found.
Several other studies used focus groups and cross-sectional associations to determine enablers of and barriers to PA for Arab women, 52 Japanese adults, 53 Norwegian adults, 54 and older adults 55 with or at risk for type 2 diabetes. A purposeful sample of Emirati National women from primary health care centers (n = 75), aged 20 to 60 years, at risk for type 2 diabetes were interviewed through 8 focus groups concerning weight management enablers and barriers. 52 Social support, such as having other women to walk with and provide motivation, was a major enabler. 52 The main barriers to participation in PA were low social support, low motivation, social and physical restrictions (clothing restrictions for outdoor activities and space for indoor PA), housework, and child care demands. 52 The participants’ suggestions to increase PA among Emirati women included the establishment of culturally sensitive exercise facilities, extended hours of operation and qualified fitness instructors in parks, and the availability of qualified dietitians, walking tracks, and exercise machines at the primary care facilities. 52
A cohort of Japanese adult men who had low PA and high leisure screen time (watching television or DVD, playing video games, and non-work-related Internet use) were more likely to be overweight as compared with their counterparts (high PA and low screen time). 53 These associations were not significant for women. 53 Screen time might be considered a barrier to PA for this population of Japanese men. 53
Self-efficacy and health beliefs for diet and exercise to manage diabetes were assessed from returned mailed questionnaires (425 out of 689, 62% response rate) for a sample of urban- and rural-dwelling Norwegian adults with type 2 diabetes. 54 Exercise management was positively associated with exercise ability expectations, adjusting for possible sociodemographic confounders such as age, gender, disease duration, and diabetes medications. 54 The investigators indicated that the majority of participants reported an overall positive level of exercise expectancies, yet they reported a low level of engaging in PA. The study was limited by data from a single time point, and the definitive causes and effects of enablers and barriers could not be determined. 54
A purposeful sample of mentally alert, older Caucasian adults (n = 32, aged ≥60 years) with type 2 diabetes and at least 1 other chronic disease was selected to determine enablers of and barriers to diabetes self-management. 55 Avoidance of diabetes complications was an enabling factor for following diabetes care recommendations. 55 Prioritizing caring for other chronic conditions over caring for diabetes emerged as a barrier. 55 A closely related barrier was the emotional frustration from conflicting treatment plans, particularly with diet, PA, and medication prescriptions. 55 This study addresses a gap in the literature for comorbidities as a barrier to diabetes care. 55 Further studies are needed to assess enablers of and barriers to PA in other populations with comorbidities. 55
Type of PA as Mediator of PA Behavior
The type of PA, resistance, or aerobic training, together with sociocultural factors may have an effect on PA behavior. That is, the likelihood of performing PA may differ by race/ethnicity, age, gender, and type of PA. A Canadian nationally representative sample of adults with type 2 diabetes, 88% Caucasian, had different PA preferences by age and gender. The investigators reported that a greater proportion of women preferred prescheduled, supervised, and instructed PA and engaging in PA with others as compared with men. 56 Adults ≥65 years of age preferred low-intensity PA without an exercise counselor as compared with adults <65 years of age. 56 Compared with women, men reported performing moderate- to high-impact PA rather than light. 56 The majority of the participants (79.9%) preferred face-to-face counseling in the diabetes center or with an affiliate associated with the center. 56 More than half (58.6%) of the participants wanted a mix of aerobics and resistance training. 56 The investigators offer findings that address an area with little research. Race/ethnicity, enablers and barriers, and sociodemographics should be included in future studies.
Resistance training may be beneficial for obese adults with type 2 diabetes according to a systematic review, primarily because it increases muscle mass, which improves insulin sensitivity. 57 Although both aerobic and resistance training are recommended for the PA component of diabetes self-management, the authors conclude that for persons with cardiorespiratory issues, resistance training may be less challenging for an initial fitness plan. 57 Biomedical barriers to PA may explain, in part, the reason why individuals with type 2 diabetes and comorbidities engaged in little or no PA. Furthermore, these barriers suggest the need for innovations in exercise. High-intensity, interval training should be considered an option for increasing PA in persons with type 2 diabetes. 58 This exercise type has been proposed as a strategy to reduce the likelihood of a hypoglycemic episode. 58 In fact, enablers and barriers may be mediated by the type of PA with frequency of PA. 49 The exercise plan for patients with type 2 diabetes should include type, frequency, duration, and intensity and be individualized according to the patient’s comorbidities, abilities, and safety concerns. 59 Increasing PA is relatively safe, based on a review of evidence-based PA clearance recommendations for individuals with diabetes and comorbidities. 60 Screening by a qualified exercise physiologist is recommended to determine the type and level of PA effort. 60 Progression of PA intensity (from low to high impact) may be beneficial and outweigh the risks, even though the risk of adverse events is higher for persons with diabetes as a result of macro and micro complications. 60 At present, research is lacking for exercise progression of volume and intensity for persons with type 2 diabetes. 2 Not having definitive guidelines may present a challenge to health care professionals in prescribing exercise. Moreover, patients may be reluctant to embark on an exercise regime without a specific progression plan.
Sedentary Behaviors as Barriers to PA
Leisure-time sedentary behaviors, such as watching television, non-work-related computer time, and playing video games, may compete with PA. For Cuban-, Haitian-, and African American adults with and without type 2 diabetes, the odds of being in the lowest quartile of PA was 3.25 (1.86, 5.68) for watching more than 4 hours of television. 43 For the group with type 2 diabetes, African Americans were more likely to watch 4 or more hours of television as compared with Cuban Americans—OR = 5.13 (3.18, 8.25)—and Haitian Americans—OR = 8.06 (4.48,14.5)—adjusting for confounders. 43 A 2-year prospective study of incidence of diabetes for a group of Seventh Day Adventists (n = 41 387) across the United States and Canada revealed 616 cases of new diabetes (1.5%). 14 The participants who reported new diabetes were more likely to be black (African American, West Indian/Caribbean, and African), watch more television and have lower PA. 14
Conclusions and Future Directions
PA has been demonstrated to have a protective role in the prevention of type 2 diabetes and the improvement of health outcomes for persons with type 2 diabetes for several populations. Implementation of PA programs for diabetes prevention remains challenging, particularly with respect to matching the level and modality of PA with sociodemographics. Effective levels and modalities of PA may not be the same across populations. Several confounders, such as family history of diabetes, race/ethnicity, comorbidities, and environmental-genetic components suggest that PA standards may have to be developed to address each population. Already, the Center for Disease Control and Prevention has set 2 levels of PA: one for prevention (150 min/wk) and another for improving health (200-300 min/wk). 61 For individuals in the overweight and obese categories, more than 150 to 250 min/wk of moderate-intensity PA is recommended to prevent weight gain and maintain weight loss. 62
The risk for type 2 diabetes with PA may not be the same across races/ ethnicities. Admiraal et al 63 found an inverse association between PA and type 2 diabetes for Caucasians but no significant association for persons of Asian Indian origin (Hindustani) and African origin (African Surinamese) after fully adjusting for age, gender, smoking, education, hypertension, and family history of diabetes or cardiovascular disease. Their results suggest that race/ethnicity may be a confounder in the relationship of PA with diabetes and that prospective studies comparing PA between and across races/ethnicities for persons with prediabetes and diabetes are warranted.
Implementation of PA programs designed to reduce the incidence of type 2 diabetes as well as those aimed to improve diabetes outcomes are further challenged by age, gender, and racial/ethnic-specific enablers and barriers. Further research, guided by the literature, is needed to address these issues. Based on this review, the authors recommend community involved interventions designed to prevent diabetes and, for persons with diabetes, those aimed at preventing health-related complications. Participatory-based PA interventions should be designed using the results of needs assessments specific to ethnicities within a community. Although much of the current research has focused on the impediments to PA, findings of facilitators are lacking. A gap remains for the development of new behavioral approaches that serve as motivators for increasing PA for adults at risk for or with diabetes. Moreover, information about these environmental, physical, and psychosocial enablers of PA, specific to individuals and groups, gained from scientific research needs to be disseminated to practitioners as well as the general public.