
Abstract
An estimated one third of American adults have prediabetes; over 30 million have type 2 diabetes mellitus. Health and wellness coaching is an emerging tool for preventing and treating chronic disease. Mastering Diabetes (MD) promotes a low-fat, plant-based, whole-food diet, utilizing online education, day-to-day accountability and support, and video conferencing. This pilot study provides a retrospective view of the effectiveness of MD to treat diabetes. Current and former clients of MD were invited to participate in a survey. On completion of the online consent, subjects were asked a series of questions in a REDCap-based survey: age, gender, enrollment date in MD, changes in weight, HbA1c, medication use, overall health, and current level of adherence to achieved changes. Overall, 253 (8.9%) participants responded to the survey; 80.6% were females, mean age was 56 years. Most of those responding (78.4%, P < .001) reported weight loss; 68.8% (P < .001) reported decreased HbA1c; 52.4% reported decreased medication use; 86.8% reported continued health improvement since having participated in MD; and 83.5% found the online program very helpful. This study demonstrated improvement in HbA1c and weight in participants in an online health and wellness coaching. Study limitations prevent drawing generalizable conclusions; further prospective evaluation is needed.
‘Health and wellness coaching (HWC) is an emerging tool for preventing and treating chronic disease.’
An estimated one third of American adults have prediabetes (PreDB) and over 30 million have diagnosed type 2 diabetes mellitus (T2DM). 1 T2DM cost the American health care system $327 billion in 2017. 2 High rates of obesity, an important risk factor for diabetes, also contributes to rising health care costs; obese adults spend 42% more on direct health care costs than normal weight adults. 3 Hospital in-patient care accounts for 43% of the total cost of diabetes. 4 For those living with T2DM, the risk of long-term complications including cardiovascular disease, chronic kidney disease, and amputations increases the need for hospitalization.4,5 PreDB is associated with increased risk of heart and kidney disease, even before the definition of T2DM is met.6,7
PreDB and T2DM are often preventable and reversible diseases when the appropriate lifestyle measures are taken. 8 The Diabetes Prevention Program successfully demonstrated that lifestyle can slow or prevent the onset of T2DM in patients with PreDB. 9 Other programs that transition patients to a plant-based diet have effectively improved glycemia in patients with PreDB and T2DM.10,11 However, the majority of patients with PreDB do not receive appropriate dietary education, coaching, accountability, or support early in the disease process to prevent the progression to T2DM. 5 In addition, the standard American diet is inconsistent with evidence-based research that has demonstrated the effectiveness of a plant-based, whole-food diet for preventing and reversing insulin resistance, T2DM, cardiovascular disease, and promoting long-term, sustainable weight loss.10,12-22
Health and wellness coaching (HWC) is an emerging tool for preventing and treating chronic disease.23,24 HWC strategies use a patient-centered approach to create a long-term sustainable lifestyle change. 3 One such program, Mastering Diabetes (MD), promotes a low-fat, plant-based, whole-food diet, utilizing recorded online education, day-to-day support via private online forums, and live interactive coaching from the MD coaching staff. MD’s stated goals are to teach people living with all forms of diabetes (including type 1, type 1.5, PreDB, type 2, and gestational diabetes) how to use a low-fat, plant-based, whole-food diet to reverse insulin resistance, reduce glycosylated hemoglobin (HbA1c), reduce fasting glucose, normalize body mass index (BMI), and reduce triglycerides, low density lipoprotein cholesterol, and blood pressure.
The online coaching program is a self-paced program that provides 16 weeks of instruction about how to transition to a low-fat, plant-based, whole-food diet, using a comprehensive online course with videos, recipes, and downloadable worksheets. In addition to the 16-week online course, clients are provided with continued support for 365 days via online discussion forums and live video conference coaching. Clients are provided with access to forums that are managed by MD coaches, and are invited to live video conference coaching sessions twice per month. MD coaching staff has a wide range of educational backgrounds and coaching certifications, and includes a PhD in nutritional biochemistry, a registered nurse, a Food for Life instructor, and a coach certified via eCornell University. A physician referral is not required to participate in the program, although many clients choose to work with a plant-based physician during their involvement in the MD program. The purpose of this pilot study was to perform a retrospective analysis of the effectiveness of MD to improve HbA1c and body weight, with the intent to provide a basis for a more rigorous prospective study.
Methods
Current and former clients of MD were invited to participate in a survey by email. Interested clients could click a link that directed them to a REDCap-based survey. On completion of the online informed consent, subjects were asked a series of questions regarding their age, gender, enrollment date in MD, changes in body weight, changes in HbA1c, changes in medication use, changes in overall health, whether they thought that the MD program was helpful, and their current level of adherence to principles taught in the program (see the appendix).
Clients of MD were instructed to eat a nutrient-dense, low-fat, plant-based, whole-food diet consisting of mainly fruits, vegetables, legumes, and whole grains. Clients were instructed to maintain a total dietary fat intake between 10% and 15%, and to eat between 70% and 80% of their diet from carbohydrate-rich whole foods. MD encourages clients to minimize high-fat plant foods including avocadoes, nuts, seeds, olives, and coconuts and minimize or eliminate animal foods including red meat, white meat, dairy products, and fish. In addition, clients were encouraged to eliminate nut, seed, and vegetable oils completely, and minimize their intake of refined carbohydrate-rich foods including breads, cereals, conventional pastas, and pastries. Clients were also discouraged from eating foods containing added sugars, flours, and added salt.
Data Analysis
Descriptive statistics was performed to describe and summarize the data. Using Fishers exact test, bivariate analysis was performed to evaluate association between gender and study variables. Overall means and standard deviation (SD) were computed for body weight and HbA1c at baseline and post-intervention. The magnitude of change for both body weight and HbA1c level was calculated using mean change (Δ Mean; baseline mean − post-intervention mean) and percent mean change (Δ %; 100 * mean change/baseline mean). Additionally, stratified means and SD were computed for HbA1c level and the corresponding Δ Mean and Δ % were reported. A one-sample t test was performed using Δ % changes to determine if the changes were statistically significant. For both overall and stratified analysis, P values <.05 were considered statistically significant. All analyses were performed using SAS University edition.
Results
Email invitations were sent to 2839 clients of MD (951 former clients, 1888 current clients); 253 (8.9%) responded to most questions; 49 (19.4%) were males, and 204 (80.6%) females. Age range was 18 to 90 years, with a mean of 56.36 years, SD 12.19 (Table 1). The number of respondents to each question ranges from 248 to 250 for the nonordinal questions, with 168 supplying pre and post ordinal weight measurements and 142 providing pre and post HbA1c values.
Characteristics of the Study Population.
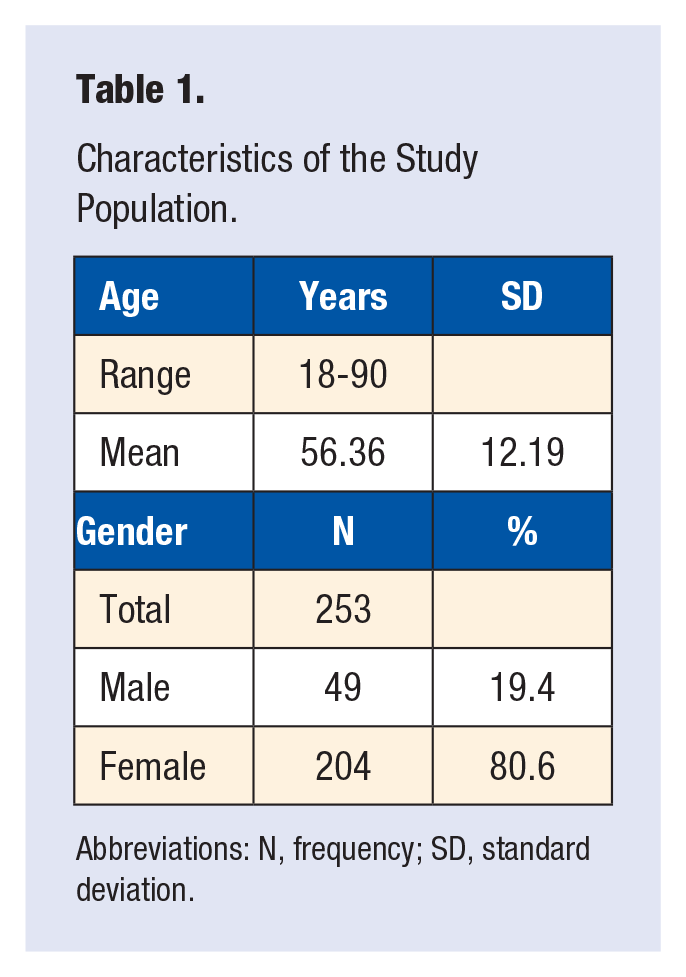
Abbreviations: N, frequency; SD, standard deviation.
A majority of those responding (78.4%) reported lost weight; 68.8% decreased HbA1c levels; 52.4% decreased medication use; 86.8% reported that their health continued to improve since having participated in MD; and 83.5% found the program very helpful (Table 2). The bivariate analysis found no significant association between gender and loss of body weight or improved HbA1c levels (Table 2).
Results Combined and by Gender.
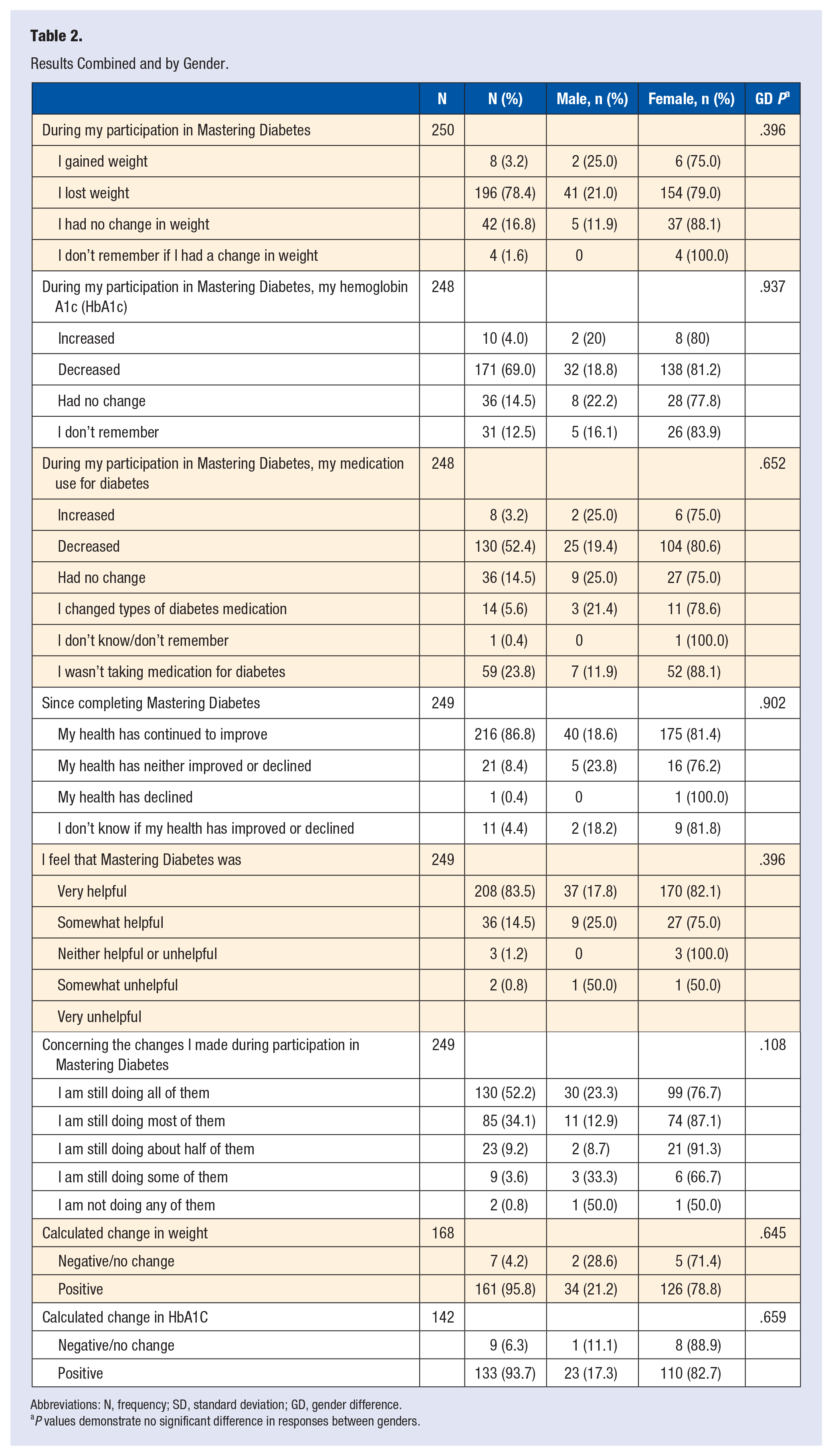
Abbreviations: N, frequency; SD, standard deviation; GD, gender difference.
P values demonstrate no significant difference in responses between genders.
Table 3 displays the overall baseline mean, post-intervention mean, Δ Mean, and Δ % for reported body weight and HbA1c levels. The overall mean baseline body weight and SD were 191.11 pounds (46.72), mean post-intervention weight and SD were 171.11 pounds (41.17), Δ Mean for weight was 20.00 pounds, and Δ % mean was 11.69%. The % mean change in body weight was statistically significant (P < .001). The overall mean baseline HbA1c and SD were 8.05% (1.93), mean post-intervention HbA1c and SD were 6.38% (0.97), Δ Mean for HbA1c was 1.67, and Δ % mean was 26.16%. The % mean change in HbA1c was statistically significant (P < .001).
Changes in Weight and HbA1c.
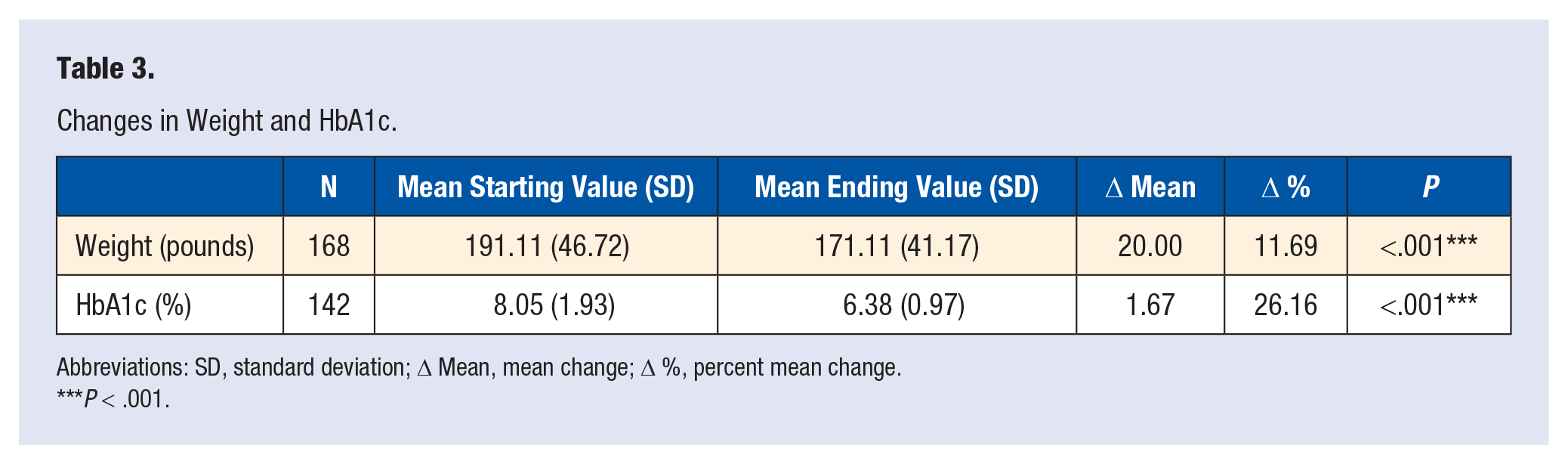
Abbreviations: SD, standard deviation; Δ Mean, mean change; Δ %, percent mean change.
P < .001.
Table 4 displays the stratified baseline mean, post-intervention mean, Δ Mean, and Δ % across different HbA1c categories. The HBA1c category is utilized for convenience of measuring change, but may not represent the actual diagnosis, since it does not take into account initial pretreatment HbA1c or the effect of medication. Among study participants with normal baseline HbA1c levels <5.7%, the mean baseline HbA1c and SD were 5.30 (0.16), mean post-intervention HbA1c and SD were 5.56 (0.48), Δ Mean for HbA1c was 0.26, and Δ % mean was 4.67. The percent mean change in HbA1c was not statistically significant (P = .864). Among PreDB category participants whose baseline HbA1c levels were between 5.7% and 6.4%, the mean baseline HbA1c and SD were 6.10 (0.22), mean post-intervention HbA1c and SD were 5.58 (0.45), Δ Mean for HbA1c was 0.52 (0.19), and Δ % mean was 9.31. The percent mean change in HbA1c was not statistically significant (P = .08). Among study participants with T2DM baseline HbA1c levels >6.4%, the mean baseline HbA1c and SD were 8.63 (1.79), mean post-intervention HbA1c and SD were 6.60 (0.96), Δ Mean for HbA1c was 2.03, and Δ % mean was 30.76. The percent mean change in HbA1c was statistically significant (P < .001).
Changes in HbA1c Stratified by Category a .
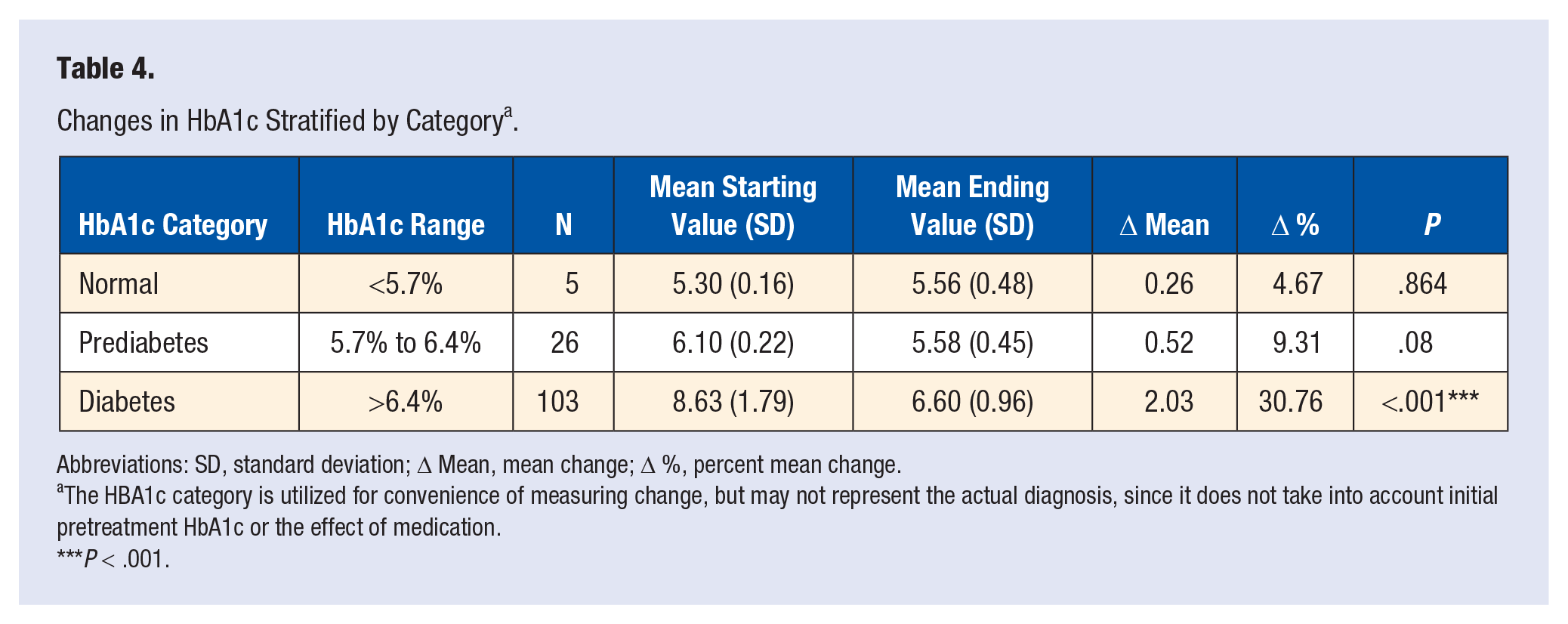
Abbreviations: SD, standard deviation; Δ Mean, mean change; Δ %, percent mean change.
The HBA1c category is utilized for convenience of measuring change, but may not represent the actual diagnosis, since it does not take into account initial pretreatment HbA1c or the effect of medication.
P < .001.
Discussion
This retrospective pilot study demonstrated that the majority of respondents enrolled in MD who completed the surveys reported reductions in HbA1c and body weight. In addition, in participants who completed 1 year of MD, an increased adherence to healthy behaviors learned during the program was observed. It is not known if participants began taking other medications or were involved with other interventions during the time of their participation in MD.
The results of this study are promising, and demonstrate a highly effective approach to reducing body weight and HbA1c using a low-fat, plant-based, whole-food diet. One of the most important and unique aspects of this intervention was that all clients were able to participate in the digital coaching and education platform from their home, using an internet-enabled computer or mobile device. As a result of this program design, clients were given the ability to move through the curriculum at their own pace, and were provided with an extensive support network throughout their transition to a low-fat, plant-based, whole-food diet. Other studies have shown the effectiveness of education and coaching for diabetes management and reversal. Sherman and Ganguli showed a drop in HbA1C from 5.85% to 5.62% as well as weight reduction from 195.2 to 183.7 pounds over the course of 24 months in 17 patients. 24 Melko et al demonstrated the positive outcomes of health coaching on patient satisfaction and decreased medication usage in patients with chronic disease. 23 Rippe discussed the benefits of lifestyle medicine for patients with PreDB and T2DM by incorporating daily habits that become the backbone of long-term sustainable change. 25
A study published by McKenzie et al in 2017 analyzed the effectiveness of a digital coaching and education platform using a very low-carbohydrate ketogenic diet. 26 This study demonstrated the effectiveness in reducing body weight and HbA1c in 262 subjects over the course of 10 weeks of intervention, in which mean HbA1c was reduced by 1.0%, and participants lost an average of 17.6 pounds in the first 10 weeks. Interestingly, C-reactive protein increased, suggesting increased total body inflammation despite improvements in body weight, medication use, and glycemia.
While these results indicate that a ketogenic diet can promote rapid changes in weight and glycemia, there is limited data about the effectiveness of a ketogenic diet in the long-term. One such study performed by the same research group reported data from participants with T2DM following 1 year of intervention utilizing a ketogenic diet, and demonstrated a 1.3% reduction in HbA1c and 30.3 pound average weight loss. 27 In contrast, MD demonstrated a greater reduction in HbA1c (1.81%) and more modest reduction in body weight in clients with T2DM at the beginning of the study, suggesting that a low-fat, plant-based, whole-food diet may improve glycemia better than a ketogenic diet despite reduced weight loss.
The results in this study are consistent with results published in 1979 in which researchers determined the effect of a low-fat, plant-based, whole-food diet on insulin requirements independent of weight loss. 28 To do so, the researchers fed insulin-dependent subjects with diabetes a low-fat, plant-based, whole-food diet and ensured that they remained weight stable throughout the duration of the study. They found that transitioning subjects to a low-fat, plant-based, whole-food diet while remaining weight stable resulted in a 58% average reduction in insulin requirements. Exactly 50% of subjects discontinued insulin completely after only 16 days, and those that continued insulin therapy reduced their dosages between 7% and 98%. These results suggest that while carbohydrate restriction is a commonly accepted dietary intervention to improve glycemia, plant-based diets low in fat significantly improve blood glucose control and reduce insulin requirements.29,30
Another important consideration in this study is that MD achieved a significant reduction in HbA1c and body weight while encouraging clients to increase their intake of whole carbohydrate-rich foods from fruits, vegetables, legumes, and whole grains. Most diabetes education focuses on dramatically reducing carbohydrate intake to between 30 and 75 grams per day as the primary method of improving blood glucose control, despite a growing body of evidence that shows that low-carbohydrate diets high in fat and protein are known to increase insulin resistance and beta cell dysfunction, which in turn can increase the risk for many chronic diseases in the long-term, including cardiovascular disease, many types of cancer, fatty liver disease, and chronic kidney disease.31-43 In addition, a growing body of large-scale epidemiological research shows that diets low in carbohydrate energy not only increase chronic disease risk but also increase the risk of all-cause mortality.44-52
The first studies to report the effect of increased dietary fat on insulin resistance were published as far back as the 1930s. Rabinowitch at the Montreal General Hospital discovered patients who were switched from a low-carbohydrate to a high-carbohydrate diet abundant in vegetables, fruits, grains, and beans reduced their need for insulin rapidly, both with and without calorie restriction. 53 Himsworth reported that patients eating a high-fat diet experience elevated blood glucose values as high as 200 mg/dL in the first hour following an oral glucose tolerance test despite excellent fasting blood glucose values, whereas subjects who ate a high-carbohydrate diet experienced a peak blood glucose value of 120 mg/dL. 54 In the 1950s, Kempner developed the rice-fruit diet in which he fed his patients a low-fat, low-sodium, plant-based diet containing only 4 foods—white rice, fruit, fruit juice, and white sugar. Using this unconventional treatment, Kempner was able to reverse T2DM entirely, and also reversed malignant hypertension, heart disease, kidney disease, and diabetic neuropathy. 55
Recent evidence from Barnard demonstrates how a low-fat, plant-based, whole-food diet containing approximately 10% fat outperformed a conventional diabetes diet based on the 2003 American Diabetes Association guidelines. Participants were monitored over 22 weeks of intervention, and the researcher observed larger reductions in HbA1c, body weight, and low-density lipoprotein cholesterol than the conventional diabetes diet. 12 When followed for 74 weeks, those in the low-fat, plant-based, whole-food group reduced their HbA1c more than those in the conventional diet group despite equivalent weight loss. 10
A comprehensive review article published in 2017 documented how plant-based diets have been shown to prevent and reverse T2DM in both randomized control trials and other types of large-scale studies. The authors explain how whole grains, legumes, fruits, vegetables, and nuts each have been shown to be protective against T2DM, and demonstrated overwhelming evidence that a whole-food, plant-based diet can protect against the development of T2DM and reverse insulin resistance in those living with PreDB and T2DM. In addition, they demonstrated how a whole-food, plant-based diet can reduce the incidence of diabetes complications and risk factors for other diseases, including coronary artery disease, high cholesterol, high blood pressure, chronic inflammation, chronic kidney disease, and peripheral neuropathy, and reviewed potential mechanisms by which diets rich in whole plant foods and low or absent in animal foods reduce diabetes risk and insulin resistance. 56
Another important consideration in this study is that unlike many weight loss programs, MD did not restrict food intake, as is common in weight loss and diabetes prevention or reversal studies. MD was unique in that no restrictions were placed on total energy intake, and counting calories was discouraged. Instead, the MD dietary protocol encouraged eating to satiety in order to prevent feeling deprived, which is known to cause food cravings and decrease long-term adherence. Recent results from the BROAD study, a similar whole-food, plant-based dietary program demonstrated significant reductions in BMI and cholesterol at 6 and 12 months in the absence of calorie counting and food restriction, suggesting that the type of food eaten may be more important than the necessity to count calories and restrict total energy intake. 13
The MD study demonstrated the effectiveness of utilizing an online coaching program to promote weight loss and reduce HbA1c in patients with PreDB and T2DM. Further investigation is needed to determine the long-term effects of online HWC to promote lifestyle change via a low-fat, plant-based, whole-food diet, and to determine whether such an intervention in free-living humans can promote continued improvements in body weight, glycemia, and chronic disease risk in patients with PreDB and T2DM.
Limitations
This retrospective survey achieved an 8.9% participation rate. Various factors may account for this low response rate. Respondents were most likely those who experienced favorable outcomes resulting in an emotional incentive to participate. It may be that some email addresses were no longer functional. It is possible that the majority of those who received the survey were no longer adherent to the MD program, or may not have remembered their biometrics values before and after the program at the time they received the survey. Values for HbA1c and body weight were self-reported. Height was not collected, limiting the ability to calculate BMI and better stratify results by weight status. Female gender preponderance is a common finding among lifestyle interventions and should be taken into consideration during analysis and application of these findings. 57 Stratification of HbA1c categories may not represent actual disease classification, since these levels may or may not reflect the effect of medication. Some of the survey respondents may not have completed a full year of participation in MD, and therefore their data may have represented preliminary results before achieving maximum benefit. To achieve a more comprehensive picture of program effectiveness, a prospective study is needed.
Conclusion
In those responding, this retrospective study demonstrated significant improvements in HbA1c and body weight in participants in the Mastering Diabetes virtual health and wellness program, as well as reported decreased use in medication, sense of improved health, patient satisfaction, and adherence to lifestyle change. A carefully designed prospective study is needed to better evaluate the effectiveness of this program for patients with all forms of diabetes.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors CK and RB are owners of Mastering Diabetes, and therefore have a significant financial conflict of interest. They did not participate in the data collection or analysis for this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Ohio University Institutional Review Board (18-X-272).
Informed Consent
An online informed consent was obtained for all participants.