
Abstract
Objective
Oxidative stress likely contributes to the pathogenesis of prediabetes. The oxidative balance score is an emerging metric for quantifying exposure to dietary and lifestyle oxidative stress. This study aimed to investigate the association between oxidative balance score and the prevalence of prediabetes, impaired fasting glucose, and impaired glucose tolerance based on data from the National Health and Nutrition Examination Survey 1999–2018.
Methods
In this cross-sectional study, the oxidative balance score was derived from 16 dietary and 4 lifestyle components, as outlined in previous research. Prediabetes, impaired fasting glucose, and impaired glucose tolerance were diagnosed based on the American Diabetes Association criteria. Multivariate logistic regression models were employed to analyze these associations.
Results
In total, 22,960 participants with a mean age of 44.7 years were included in this study. In fully adjusted models, dietary oxidative balance score, lifestyle oxidative balance score, and overall oxidative balance score were all inversely associated with the prevalence of prediabetes among the general US adult population (odds ratios and 95% confidence intervals of 0.956 (0.949, 0.963), 0.914 (0.891, 0.937), and 0.957 (0.950, 0.964), respectively; all p <0.0001). Compared with quartile 1, dietary oxidative balance score, lifestyle oxidative balance score, and overall oxidative balance score at quartile 4 were all associated with a significantly lower prevalence of prediabetes (odds ratios and 95% confidence intervals 0.515 (0.449, 0.591), 0.834 (0.740, 0.940), and 0.505 (0.440, 0.579), respectively; all p for trend <0.0001). Similar results were observed for impaired fasting glucose and impaired glucose tolerance. Restricted cubic spline analysis showed that most of the associations were nonlinear and that significant negative correlations were observed only after a certain threshold. Stratified and sensitivity analyses confirmed the robustness of the findings.
Conclusions
Adherence to an antioxidant-rich diet and healthy lifestyle may aid in the prevention of prediabetes, impaired fasting glucose, and impaired glucose tolerance among the general US adult population. Further cohort studies are needed to validate these findings.
Keywords
Introduction
Prediabetes is an intermediate stage between normoglycemia and diabetes mellitus (DM), characterized by impaired fasting glucose (IFG) and impaired glucose tolerance (IGT). 1 In 2021, the global prevalence rates of IFG and IGT in individuals aged 20–79 years were estimated at 5.8% and 9.1%, with projections indicating increases to 6.5% and 10.0% by 2045, respectively. 2 Over one-third of US adults have prediabetes, with notable disparities based on race/ethnicity, age, and education level.3,4 Increasing evidence indicates that prediabetes is a distinct clinicopathologic entity associated with a broad spectrum of organ and tissue damage, and it is currently recognized in the International Classification of Diseases system, Tenth Revision (R73). 5 Prediabetes is a major risk factor for the development of diabetes, with 5%–10% of individuals exhibiting progression from prediabetes to diabetes annually, and it is linked to the early onset of diabetic complications. 6 Furthermore, prediabetes is associated with elevated risks of cardiovascular events and all-cause mortality. 7 Early intervention through dietary and lifestyle modifications may help prevent prediabetes, thereby reducing disease burden and the risk of progression to diabetes. 8
Prediabetes is associated with inflammation and increased burden of oxidative stress.9,10 Hyperglycemia may induce chronic low-grade inflammation and elevated production of reactive oxygen species (ROS). In turn, heightened oxidative stress promotes insulin resistance and dysregulated insulin secretion. 11 A real-world study demonstrated that certain oxidative stress and inflammatory markers were positively correlated with glucose intolerance in individuals with prediabetes, whereas reduced levels of glutathione, an antioxidant, were negatively correlated with glucose intolerance. 12 Moreover, several conditions linked to prediabetes, such as type 2 DM, 13 obesity, metabolic syndrome, 14 and fatty liver disease, 15 are characterized by chronic inflammation. Antioxidant-rich diets ameliorate inflammatory burden. 16 Some observational clinical studies have suggested that dietary antioxidant capacity is inversely associated with prediabetes incidence, although conflicting findings have been reported.17–19 Furthermore, greater adherence to antioxidant-rich lifestyles, such as regular physical activity, has been associated with a reduced prevalence of prediabetes, whereas potential prooxidants, including elevated body mass index (BMI) and smoking, are associated with significantly heightened prediabetes risk.20–22 Hence, it is necessary to determine the association between oxidative stress and the prevalence of prediabetes. However, dietary or lifestyle components individually may not accurately reflect an individual’s integrated prooxidant and antioxidant balance and thus may explain the inconsistent findings.
The oxidative balance score (OBS) is a validated composite tool that quantifies both antioxidant and prooxidant exposures. It is derived from 16 dietary and 4 lifestyle components, comprising 5 pro-oxidative and 15 antioxidative components. 23 The OBS fully accounts for the antioxidative and pro-oxidative properties of food and behavior; the scores assigned to antioxidative components reflect their beneficial protective effects, whereas pro-oxidative components are inversely scored to indicate their potential to enhance oxidative stress risk. A higher OBS indicates enhanced antioxidant potential in the body. Compared with the separate assessment of exogenous antioxidants or prooxidants, OBS dynamically reflects an individual’s oxidative stress exposure by integrating the synergistic or antagonistic interactions between dietary and behavioral factors. 24 A substantial body of epidemiological evidence indicates that OBS is strongly linked to the onset and progression of various diseases, including multiple cancers, depression, and chronic kidney disease.25–27 However, the relationship between OBS and the prevalence of prediabetes, IFG, and IGT in the general population remains underexplored. Investigating this relationship could help elucidate the public health significance of adherence to an antioxidant-rich diet and lifestyle, as assessed by OBS, in preventing prediabetes, offering new insights into reducing the disease burden.
This study aimed to examine the association between OBS and the prevalence of prediabetes, IFG, and IGT in the general US adult population using nationally representative data from the National Health and Nutrition Examination Survey (NHANES), a large serial cross-sectional survey. We also investigated potential nonlinear or dose–response associations and the presence of inequalities across different subgroups.
Methods
Study design and population
NHANES is a major epidemiological program conducted by the National Center for Health Statistics (NCHS) that collects data through a series of questionnaires and physical examinations. It has been conducted in continuous biennial cycles since 1999 to assess the health and nutritional status of noninstitutionalized US citizens. NHANES employs a complex, multistage probability sampling cluster design to draw a sample of approximately 5000 participants per year from across the country, producing nationally representative estimates by applying appropriate weighting. Thus, NHANES is a national, multiethnic, serial population-based cross-sectional survey. All NHANES study protocols were approved by the NCHS Ethics Review Board, and all participants provided written informed consent. Detailed NHANES study designs and data are publicly available at www.cdc.gov/nchs/nhanes/. The NHANES database is publicly accessible and contains de-identified patient data; therefore, this study was granted an exemption for ethical approval by the Ethics Committee of the Central Hospital Affiliated to Shenyang Medical College. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 28
In this cross-sectional study, we initially identified 45,848 nondiabetic adults from the NHANES 1999–2018 dataset. Participants were then excluded based on the following criteria: (a) 1547 pregnant women; (b) 1693 individuals with missing prediabetes diagnosis data; (c) 17,555 individuals with missing OBS data; and (d) 2093 individuals with missing covariates. After applying these exclusion criteria, a total of 22,960 participants were included in the final analysis (Figure 1). This study was conducted in accordance with the ethical principles of the Helsinki Declaration of 1975, as revised in 2013.

Flowchart of study population selection from NHANES 1999–2018. NHANES: National Health and Nutrition Examination Survey.
OBS assessment
The OBS was developed through multiple observational studies as a comprehensive measure to capture the net oxidative impact of various prooxidant and antioxidant exposures.29,30 The OBS is composed of 16 dietary and 4 lifestyle components that together provide a comprehensive measure of an individual’s oxidative balance. The dietary components include fiber, carotene, riboflavin, niacin, vitamin B6, total folate, vitamin B12, vitamin C, vitamin E, calcium, magnesium, zinc, copper, selenium, total fat, and iron, while the lifestyle components encompass physical activity, BMI, alcohol intake, and serum cotinine. 31 Among these 20 components, 5 components, namely, dietary total fat, dietary iron, BMI, alcohol, and serum cotinine, are classified as prooxidants, whereas the remaining components are considered antioxidants. Consequently, a higher OBS indicates a predominance of antioxidant exposure, reflecting enhanced antioxidant capacity in the individual’s diet and lifestyle.
Dietary OBS components were assessed based on a combination of two 24-h dietary recall intakes and the United States Department of Agriculture Food and Nutrient Database for Dietary Studies. 32 Physical activity was assessed according to metabolic equivalents (MET), with total MET for each participant being the sum of the self-reported time spent in each physical activity (min/week) on the Physical Activity Questionnaire multiplied by the MET score for each activity. 33 The BMI was calculated by dividing the body weight (kg) by the square of body height (m), as determined by skilled staff at the mobile examination centers. Serum cotinine level was considered as a proxy for active and passive smoking exposure. Alcohol intake (g/day (d)) was self-reported from dietary interviews.
The OBS for each participant was calculated based on established protocols detailed in previous studies, incorporating dietary and lifestyle components validated for oxidative stress assessment. 29 All other factors, excluding alcohol intake, were stratified into tertiles by sex, with antioxidants scored from 0 to 2 (low to high intake) and prooxidants scored inversely (high to low intake).29,34 Alcohol intake was evaluated using established criteria: (a) heavy drinkers (≥30 g/d for men, ≥15 g/d for women) received 0 points; (b) moderate drinkers (0–30 g/d for men, 0–15 g/d for women) received 1 point; and (c) nondrinkers received 2 points. 35 Specific assessment schemes are presented in Table S1.36,37 The overall OBS was computed by summing the scores of both antioxidant and prooxidant components, resulting in a total score ranging from 0 to 40, with higher scores indicating greater antioxidant dominance.
Definition of prediabetes
Prediabetes was assessed in accordance with a self-reported history of prediabetes or the defining criteria of the American Diabetes Association (ADA) and the absence of diabetes. 38 Self-reported prediabetes was obtained from the Diabetes Questionnaire. In laboratory tests, the presence of prediabetes was indicated by IFG (fasting blood glucose level: 5.6–6.9 mmol/L), IGT (2-h oral glucose tolerance test blood glucose level: 7.8–11.0 mmol/L), or glycated hemoglobin HbA1c level of 5.7%–6.4%, according to the ADA criteria. 39
Covariates
Covariates of interest included age, sex (male/female), race/ethnicity (Mexican American/non-Hispanic Black/non-Hispanic White/Other Hispanic/Other race), education level (lower than high school diploma/high school diploma /higher than high school diploma), household income-to-poverty ratio (PIR), marital status (non-single/single), dietary energy intake (kcal/d), hypertension (no/yes), and cardiovascular disease (CVD; no/yes). Information on demographic variables was obtained from self-reports in the NHANES demographic file. PIR was defined as the ratio of family income, as determined by the Consumer Price Index, to the federally recognized poverty level. 40 Daily energy intake was obtained via the Total Nutrient Intake file from the NHANES dietary recall questionnaire. Hypertension was assessed according to self-reported history, blood pressure level of ≥140/90 mmHg, or intake of antihypertensive medications. 41 CVD history was obtained based on self-reported questionnaires and included coronary heart disease, congestive heart failure, angina, stroke, and heart attack.
Statistical analyses
We weighted all analyses in this study according to the NHANES analytic guidelines to account for the NHANES complex study design. 42 All data are publicly accessible in the official NHANES website. We first sorted, cleaned, and combined the data in cycles. Then, data analysis was performed using R (version 4.2.3; R Foundation for Statistical Computing, Vienna, Austria) and Free Statistics software (version 2.1; Beijing Fengrui Kelin Medical Technology Co., Ltd., Beijing, China), with a two-sided p-value <0.05 indicating statistical significance. In baseline analyses, data were presented as mean ± standard error (continuous variables) or number (percentage) (categorical variables), and differences across groups for continuous and categorical variables were detected using weighted t-tests and chi-square tests, respectively. Multiple multivariate logistic regression models were developed to explore the associations of overall OBS, dietary OBS, and lifestyle OBS with the prevalence of prediabetes, IFG, and IGT among the general US adult population. Crude models were not adjusted for any covariates; model 1 was adjusted for age, sex, and race/ethnicity; and model 2 was similar to model 1 and was additionally adjusted for education level, PIR, marital status, dietary energy intake, hypertension, and CVD. Fully adjusted restricted cubic spline (RCS) models were used to detect potential nonlinear correlations and select the appropriate number of knots (n = 4) for smooth curve fitting. Stratified analyses were performed to explore whether these associations remained stable across subgroups (age, sex, race/ethnicity, education, PIR, marital status, dietary energy intake, hypertension, and CVD) and detect potential effect modifiers using interaction analyses. In sensitivity analyses, we excluded self-reported prediabetes and explored whether there exists an association between OBS and the prevalence of undiagnosed prediabetes.
Results
Baseline characteristics
A total of 22,960 participants were included in this study with a mean age of 44.7 years and a mean OBS of 21.109. The prevalence of prediabetes was approximately 36%. Compared with the control population, individuals with prediabetes were older and more likely to be male, non-Hispanic Black, and non-single, with an education level lower than high school diploma, and have hypertension and CVD. Notably, patients with prediabetes had significantly lower overall OBS, dietary OBS, and lifestyle OBS (all p < 0.0001) (Table 1).
Baseline analysis according to prediabetes status, based on data collected from NHANES 1999–2018.

Data are presented as mean ± standard error (continuous variables) or number (percentage) (categorical variables). Differences across groups for continuous and categorical variables were detected using weighted t-tests and chi-square tests, respectively.
NHANES: National Health and Nutrition Examination Survey; PIR: family income-to-poverty ratio; OBS: oxidative balance score; CVD: cardiovascular disease.
Association of OBS with the prevalence of prediabetes, IFG, and IGT
Dietary OBS, lifestyle OBS, and overall OBS were all negatively associated with the prevalence of prediabetes among the general US adult population in both crude and partially adjusted models. After adjusting for all confounders, dietary OBS, lifestyle OBS, and overall OBS remained inversely associated with the prevalence of prediabetes (dietary OBS: odds ratio (OR) and 95% confidence interval (CI) = 0.956 (0.949, 0.963), p < 0.0001; lifestyle OBS: 0.914 (0.891, 0.937), p < 0.0001; and overall OBS: 0.957 (0.950, 0.964), p < 0.0001). Compared with quartile 1 (Q1), dietary OBS at Q2, Q3, and Q4 were all associated with a significantly lower prevalence of prediabetes (OR = 0.844, 0.775, and 0.515, respectively; p for trend <0.0001). Compared with Q1, lifestyle OBS at Q4 was associated with a significantly lower prevalence of prediabetes (OR = 0.834, p = 0.0036; p for trend <0.0001). Similarly, compared with Q1, overall OBS at Q2, Q3, and Q4 were all associated with a significantly lower prevalence of prediabetes (OR = 0.779, 0.764, and 0.505, respectively; p for trend <0.0001) (Table 2).
Association of OBS with the prevalence of prediabetes in the general US adult population, based on data collected from NHANES 1999–2018.

Crude models were not adjusted for any covariates; model 1 was adjusted for age, sex, and race/ethnicity; model 2 was similar to model 1 and was additionally adjusted for education level, PIR, marital status, dietary energy intake, hypertension, and CVD.
OBS: oxidative balance score; NHANES: National Health and Nutrition Examination Survey; OR: odds ratio; CI: confidence interval; CVD: cardiovascular disease; PIR: family income-to-poverty ratio; Ref.: reference
In model 2, dietary OBS, lifestyle OBS, and overall OBS were all inversely associated with the prevalence of IFG in the general population (dietary OBS: OR and 95% CI = 0.936 (0.922, 0.952), p < 0.0001; lifestyle OBS: 0.797 (0.759, 0.836), p < 0.0001; overall OBS: 0.931 (0.917, 0.946), p < 0.0001). Higher dietary OBS, lifestyle OBS, and overall OBS were all associated with a significantly lower prevalence of IFG (all p for trend <0.0001) (Table 3). Similarly, dietary OBS, lifestyle OBS, and overall OBS were all negatively associated with the prevalence of IGT among the general US adult population (OR = 0.978, 0.844, and 0.973, respectively). Compared with Q1, dietary OBS, lifestyle OBS, and overall OBS at Q4 were all associated with a significantly lower prevalence of IGT (OR = 0.753, 0.643, and 0.630; p for trend = 0.0032, <0.0001, and 0.0002, respectively) (Table 4).
Association of OBS with the prevalence of IFG among the general US adult population, based on data collected from NHANES 1999–2018.

Crude models were not adjusted for any covariates; model 1 was adjusted for age, sex, and race/ethnicity; model 2 was similar to model 1 and was additionally adjusted for education level, PIR, marital status, dietary energy intake, hypertension, and CVD.
OBS: oxidative balance score; NHANES: National Health and Nutrition Examination Survey; OR: odds ratio; CI: confidence interval; IFG: impaired fasting glucose; CVD: cardiovascular disease; PIR: family income-to-poverty ratio; Ref.: reference
Association of OBS with the prevalence of IGT among the general US adult population, based on data collected from NHANES 1999–2018.

Crude models were not adjusted for any covariates; model 1 was adjusted for age, sex, and race/ethnicity; model 2 was similar to model 1 and was additionally adjusted for education level, PIR, marital status, dietary energy intake, hypertension, and CVD.
OBS: oxidative balance score; IGT: impaired glucose tolerance; NHANES: National Health and Nutrition Examination Survey; OR: odds ratio; CI: confidence interval; CVD: cardiovascular disease; PIR: family income-to-poverty ratio; Ref.: reference
RCS analysis
RCS analysis showed that dietary OBS, lifestyle OBS, and overall OBS were all nonlinearly associated with the prevalence of prediabetes (all p for nonlinearity <0.0001) (Figure 2(a) to (c)). Similarly, dietary OBS was nonlinearly associated with the prevalence of IFG (p for nonlinearity = 0.0001; Figure 2(d)), whereas lifestyle OBS was linearly associated with the prevalence of IFG (p = 0.0622) (Figure 2(e)). Overall OBS was also nonlinearly associated with IFG prevalence (p for nonlinearity < 0.0001; Figure 2(f)). A similar pattern was observed for IGT. Dietary OBS was nonlinearly associated with the prevalence of IGT (p for nonlinearity = 0.0040; Figure 2(g)), lifestyle OBS was linearly associated with the prevalence of IGT (p for nonlinearity = 0.0944; Figure 2(h)), and overall OBS showed a nonlinear association (p for nonlinearity =0.0012; Figure 2(i)).
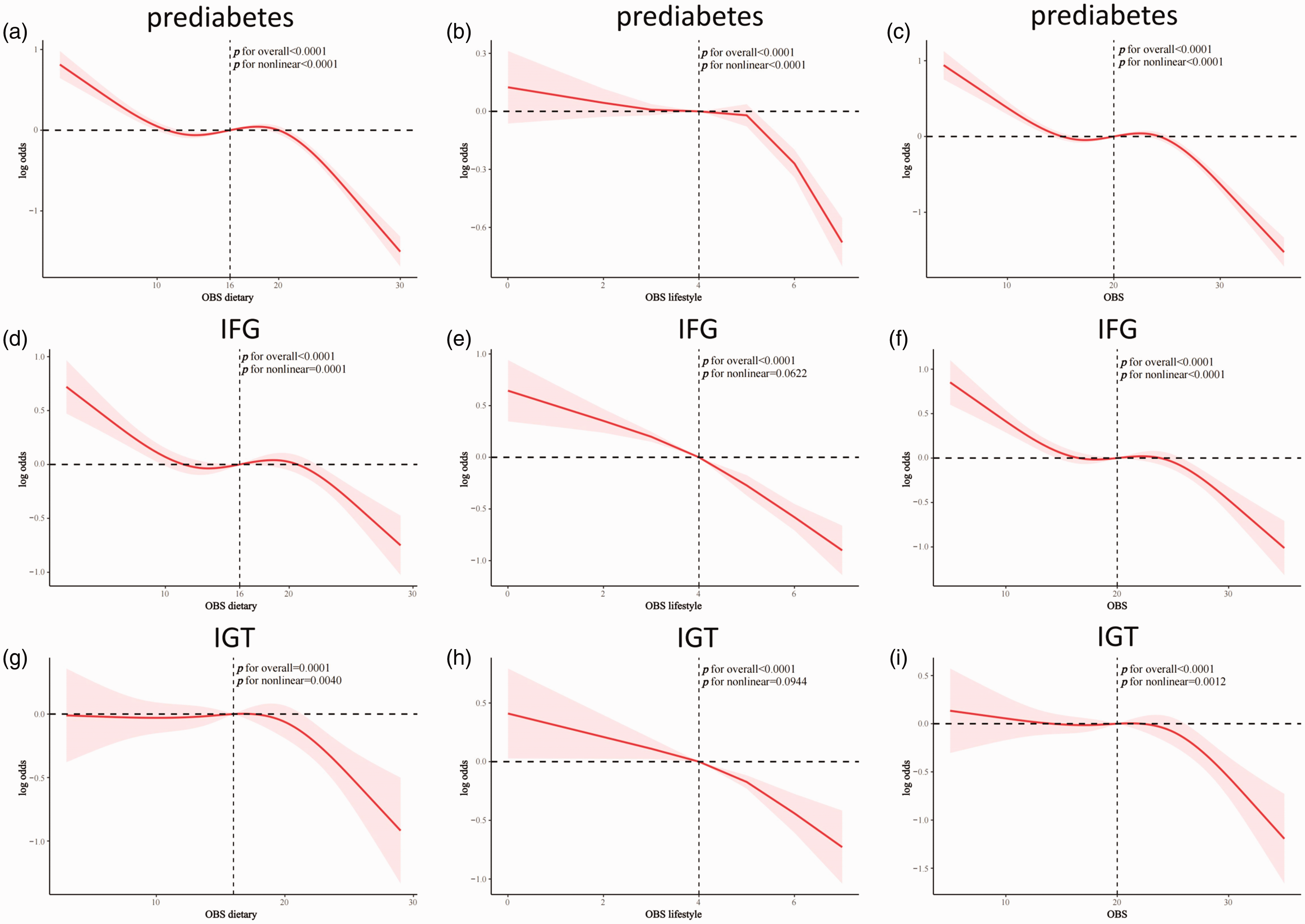
RCS analysis of the association of OBS with the prevalence of prediabetes, IFG, and IGT among the general US adult population. (a) Dietary OBS and prediabetes; (b) Lifestyle OBS and prediabetes; (c) Overall OBS and prediabetes; (d) Dietary OBS and IFG; (e) Lifestyle OBS and IFG; (f) Overall OBS and IFG; (g) Dietary OBS and IGT; (h) Lifestyle OBS and IGT and (i) Overall OBS and IGT. RCS: restricted cubic spline; OBS: oxidative balance score; IFG: impaired fasting glucose; IGT: impaired glucose tolerance.
Stability analysis of the association between OBS and metabolic abnormalities
Interaction analyses demonstrated no significant effect modifiers in any of the associations of OBS with the prevalence of prediabetes, IFG, and IGT (all p for interaction >0.05), suggesting that these associations remained stable across subgroups (age, sex, race/ethnicity, PIR, education, marital status, hypertension, CVD, and dietary energy intake) (Figures 3–5). These findings confirmed the stability and robustness of the findings.
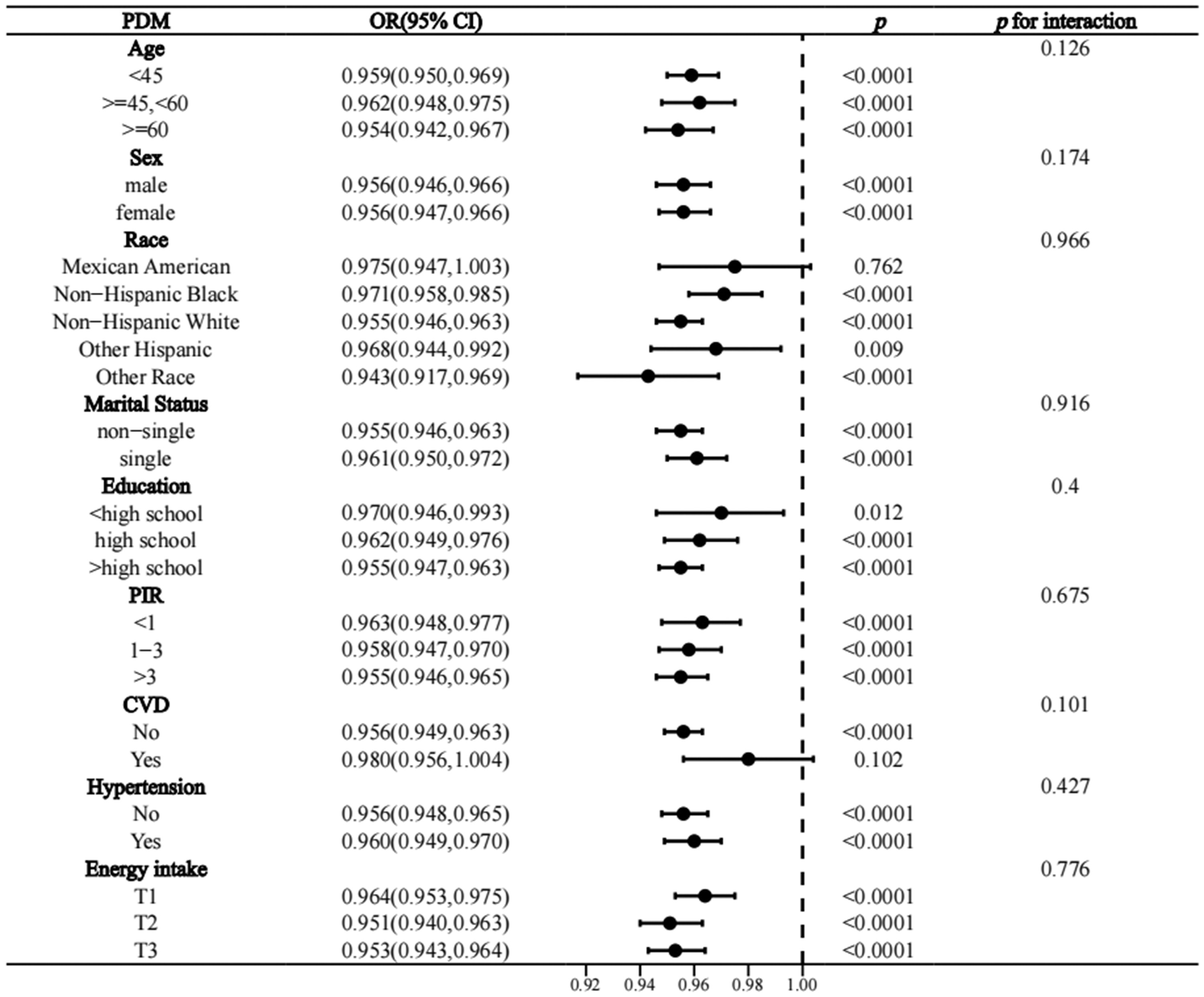
Stratified analysis of the association between OBS and the prevalence of prediabetes among the general US adult population. OBS: oxidative balance score; PIR: family income-to-poverty ratio; CVD: cardiovascular disease; OR: odds ratio; CI: confidence interval.
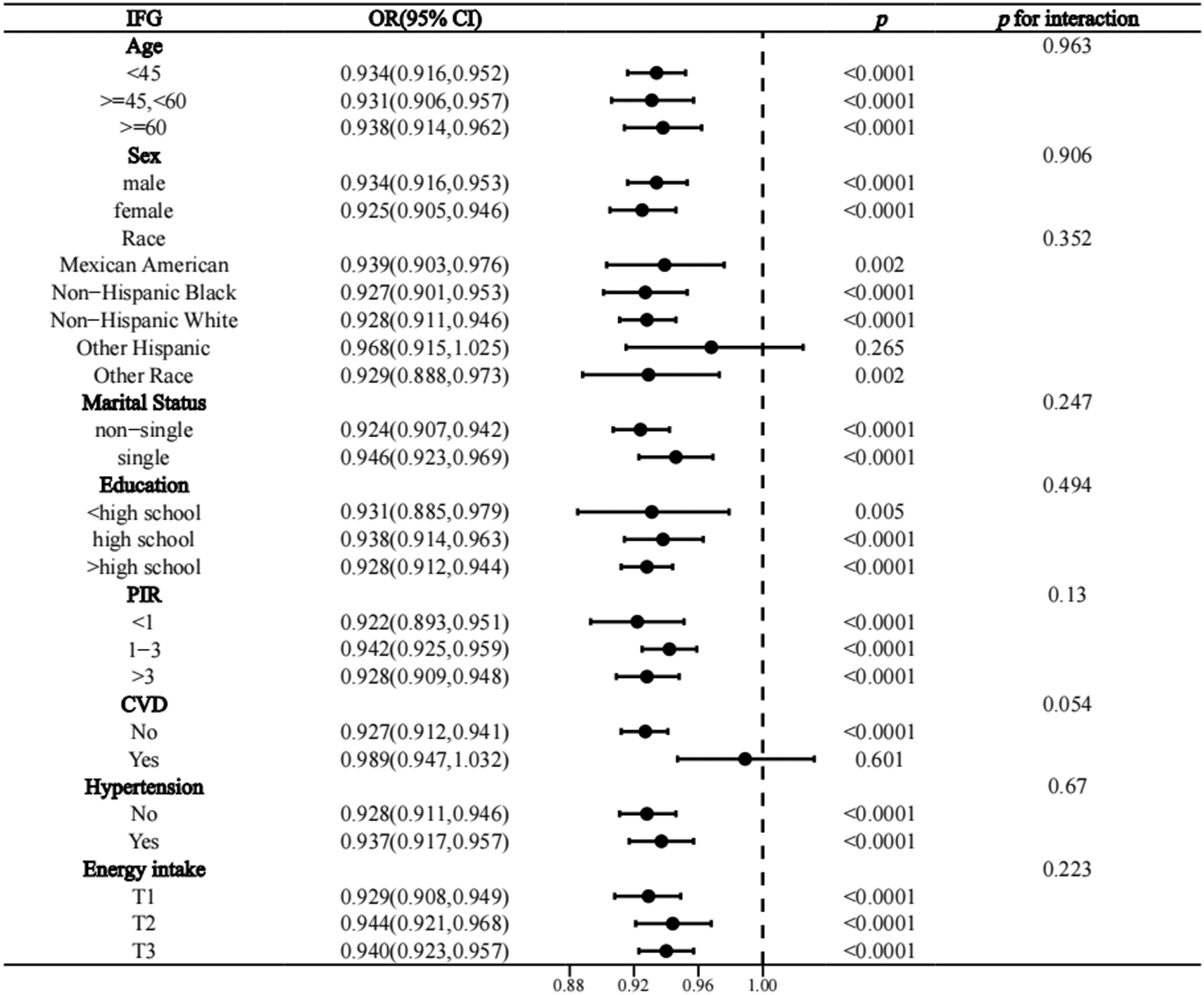
Stratified analysis of the association between OBS and the prevalence of IFG among the general US adult population. PIR: family income-to-poverty ratio; CVD: cardiovascular disease; OR: odds ratio; CI: confidence interval.

Stratified analysis of the association between OBS and the prevalence of IGT among the general US adult population. PIR: family income-to-poverty ratio; CVD: cardiovascular disease; OR: odds ratio; CI: confidence interval.
Sensitivity analyses
In sensitivity analyses, the exclusion of self-reported prediabetes did not significantly alter the results, demonstrating the stability of these findings. In model 2, dietary OBS, lifestyle OBS, and overall OBS were all inversely associated with the prevalence of undiagnosed prediabetes (OR = 0.955, 0.907, and 0.955, respectively). Higher dietary OBS, lifestyle OBS, and overall OBS were all associated with a significantly lower prevalence of undiagnosed prediabetes (all p for trend <0.0001) (Table S2).
Discussion
In a large, national, serial population-based cross-sectional analysis, we found that overall OBS, dietary OBS, and lifestyle OBS were all inversely associated with the prevalence of prediabetes, IFG, and IGT in the general US adult population. Compared with the lowest quartile (Q1), the highest quartiles of overall OBS, dietary OBS, and lifestyle OBS were associated with a significantly lower prevalence of prediabetes, IFG, and IGT. Notably, most of these associations were nonlinear, indicating that a sufficiently high OBS must be maintained to obtain significant beneficial effects on prediabetes in the general population. Stratified and sensitivity analyses confirmed the robustness of these findings. Overall, these findings suggest that adherence to an antioxidant-rich diet and lifestyle patterns can help reduce the prevalence of prediabetes, IFG, and IGT in the general population, highlighting the clinical importance of oxidative balance in prediabetes development.
The first OBS regimen was introduced in 2002 and included dietary vitamin C, beta-carotene, and iron. 43 Subsequent extensive clinical studies have continually updated and expanded the components and assessment of OBS regimens, resulting in more than 20 different OBS regimens to date. 24 In this study, we utilized the OBS protocol that has been previously employed and validated in numerous NHANES-related studies, which includes 16 dietary and 4 lifestyle components, to comprehensively assess the oxidative homeostasis of individuals with high consistency and reliability.26,32,35 Accumulating clinical evidence has demonstrated that a higher OBS, which generally indicates a greater intake of antioxidants, is inversely associated with the risk of several chronic diseases. 24 Therefore, OBS can serve as a comprehensive indicator for assessing an individual’s overall health. By calculating OBS, physicians can gain insights into an individual’s dietary and lifestyle habits, thereby offering personalized health advice and guidance.
Notably, several studies have shown that OBS is inversely associated with the prevalence of various metabolic diseases. A cross-sectional analysis using NHANES demonstrated that OBS was negatively associated with the risk of type 2 DM (T2D) in the general US adult population (OR = 0.96, 95% CI = 0.94, 0.99), with sex differences. 44 Prospective cohort studies from Korea have suggested that OBS is negatively associated with the risk of T2D in middle-aged and older populations45,46 and in populations without nonalcoholic fatty liver disease (NAFLD). 47 Notably, a cross-sectional analysis from Iran showed that higher OBS was associated with improved glycemic control (significantly lower HbA1c and fasting glucose levels) in the T2D population. 48 In addition, emerging clinical studies have suggested that OBS is negatively associated with the prevalence of metabolic syndrome (MetS) in the general population; however, inconsistent findings have been reported. Cross-sectional analyses from NHANES suggest that OBS is negatively associated with the prevalence of MetS among the general US adult population.35,49 In addition, OBS was negatively associated with the severity of MetS and all-cause mortality in the MetS population. 49 Consistently, cross-sectional analyses and prospective cohort studies from Korea have shown that OBS is negatively associated with the prevalence and incidence of MetS in the general population, both in men and women. 50 However, a cross-sectional study from Iran indicated that compared with the lowest tertile, OBS at the highest tertile was not associated with MetS prevalence (OR = 0.71, 95% CI = 0.48, 1.03; p = 0.07). 51 We hypothesized that these inconsistent findings may be due to differences in the study populations, sample size, and OBS components. Interestingly, recent observational studies have shown a protective effect of OBS on the hepatic manifestations of MetS and NAFLD. Cross-sectional analyses from NHANES showed that overall OBS, dietary OBS, and lifestyle OBS were all negatively associated with the prevalence of NAFLD, but not with the risk of advanced liver fibrosis.32,52 In addition, a recent population-based study showed that OBS is associated with a reduced risk of CVD prevalence and mortality in the NAFLD population. 53 Consistently, a case–control study from Iran and a cohort study from Korea have demonstrated that OBS is negatively associated with the prevalence of NAFLD in the general population.54,55 Overall, these observational studies suggest that OBS has beneficial effects on various metabolic diseases. However, although OBS has been shown to have clinical relevance in several chronic noncommunicable diseases, its association with the prevalence of prediabetes, IFG, and IGT remains unknown. To the best of our knowledge, this is the first real-world study exploring the association of OBS with the prevalence of prediabetes, IFG, and IGT in the general population. Our study consistently demonstrated that higher overall OBS, dietary OBS, and lifestyle OBS were associated with a reduced prevalence of prediabetes, IFG, and IGT among the general US adult population, suggesting that adherence to antioxidant-rich diets and lifestyles can help prevent prediabetes, thereby reducing subsequent cardiovascular and diabetes risk.
Previous studies have shown a negative association between dietary antioxidant capacity and the prevalence of prediabetes in the general population, although inconsistent findings exist. An observational study from Poland showed that compared with Q1, dietary total antioxidant capacity (DTAC, measured as ferric ion-reducing antioxidant potential (FRAP)) at Q2 and Q3 was associated with a lower prevalence of prediabetes (as measured by IFG level) in the general population, which disappeared at Q4. 17 Evidence from the Rotterdam Study suggested that FRAP was not associated with risk of prediabetes in the general population and in women, but a significant association was observed in men (hazard ratio (HR) = 0.84, 95% CI = 0.72, 0.98). 18 A case–control study from Iran demonstrated that compared with Q1, DTAC at Q4 was associated with reduced prevalence of prediabetes in the general population (OR = 0.18, 95% CI = 0.07, 0.49). 19 Similarly, another case–control study from Iran showed that higher DTAC rather than Healthy Eating Index-2015 was associated with a lower prevalence of prediabetes in the general population (highest tertile compared with lowest tertile: OR = 0.09, 95% CI = 0.02, 0.53). 56 Collectively, these lines of evidence suggest that dietary antioxidant potential is associated with reduced prevalence of prediabetes in the general population. However, evidence on the association of specific individual or combined dietary antioxidants with prediabetes remains sparse.
Some lifestyle habits have been shown to be protective/risk factors for prediabetes. A meta-analysis suggested that being physically active helps slow disease progression in prediabetes (improved IFG, IGT, HbA1c, maximal oxygen uptake, and body composition). 20 A cross-sectional analysis from NHANES showed that higher levels of recreational physical activity were associated with significantly lower prevalence of prediabetes (OR = 0.78, 95% CI = 0.66, 0.94). 57 However, BMI, smoking, and excessive alcohol consumption, which are recognized as prooxidants, may increase the risk of prediabetes. BMI is a major risk factor for prediabetes, 4 and a cohort study showed that cumulative BMI was positively associated with incident prediabetes (HR = 2.093). 21 Accumulating epidemiologic evidence has suggested that smoking increases the risk of prediabetes. 22 A cross-sectional study from Japan suggested that even light-to-moderate alcohol consumption can impair insulin secretion and increase fasting glucose levels in people with normal BMI. 58 Our study provides further evidence that the predominance of an antioxidant lifestyle (physical activity) compared with a prooxidant lifestyle is associated with reduced prevalence of prediabetes, IFG, and IGT in the general population, providing an association between individual integrated lifestyle oxidative stress exposure and the prevalence of prediabetes.
Notably, several real-world studies have shown that OBS is negatively correlated with serum levels of some oxidative stress markers, suggesting that OBS indeed modulates disease risk partly by ameliorating intrinsic levels of oxidative stress in the body. A cross-sectional analysis from Korea showed that OBS was negatively associated with serum gamma-glutamyl transferase levels in the general adult population. 59 Another secondary analysis of two case–control studies showed that OBS was negatively associated with circulating levels of F2-isoprostanes (a marker of oxidative stress) and C-reactive protein (a marker of systemic inflammation). 60 Thus, considering the potential role of oxidative stress and systemic inflammation in the pathogenesis of prediabetes,11,12 OBS may exert a protective effect on the prevalence of prediabetes in the general population through these mechanisms.
Our study revealed a nonlinear threshold effect between OBS and the prevalence of prediabetes, where significant risk reduction occurred only when OBS exceeded a critical level. This phenomenon may reflect a biological “tipping point” in the antioxidant–prooxidant equilibrium. At lower OBS levels, the intake of isolated antioxidants may be insufficient to counteract oxidative damage caused by lifestyle-related factors (e.g. smoking and obesity), leading to excessive ROS production, release of inflammatory cytokines, and impairment of insulin signaling and β-cell function. 61 However, once OBS surpasses the threshold, the synergistic effects of multiple antioxidants and reduced prooxidant exposure may collectively restore redox homeostasis, thereby improving insulin sensitivity. This is consistent with evidence from interventional and observational studies, suggesting that combinatorial antioxidant interventions, rather than single antioxidants, significantly improve glucose tolerance by suppressing nuclear factor kappa B–mediated inflammation and ROS-induced β-cell damage.62–64 Our results emphasize that dietary modifications, lifestyle interventions, and reduction of prooxidant exposure are essential to achieving the OBS threshold required for prediabetes prevention.
Our study has several significant strengths. First, it is a nationally representative, large-sample, multiethnic population-based study, offering potential generalizability and applicability to other populations. Second, the findings were derived from rigorous and standardized statistical analyses, with robustness confirmed through stratified and sensitivity analyses. These findings hold significant clinical relevance, suggesting that adherence to antioxidant-rich diets and lifestyles may aid in the prevention of prediabetes, offering practical and feasible strategies. However, there are certain limitations to our study. First, as a cross-sectional study, this research cannot establish causal relationships and is subject to residual confounding while also limiting the ability to assess the long-term effects of oxidative stress on glucose metabolism. Future prospective cohort studies with repeated OBS measurements are needed to confirm these findings and evaluate dynamic changes in glucose homeostasis. Additionally, interventional studies targeting dietary and lifestyle modifications to improve oxidative balance could provide further insights into potential preventive strategies. Second, self-reported dietary and lifestyle data in NHANES may have introduced recall bias and measurement errors. Finally, the OBS components and their weightings might not fully capture oxidative stress exposure. Future studies should incorporate biomarker-based assessments and environmental exposure data to enhance the accuracy of oxidative stress evaluation.
Conclusion
In a national series of cross-sectional studies, overall OBS, dietary OBS, and lifestyle OBS were all inversely associated with the prevalence of prediabetes, IFG, and IGT among the general US adult population. Higher overall OBS, dietary OBS, and lifestyle OBS were associated with significantly lower prevalence of prediabetes. Most of the associations were nonlinear, suggesting that a sufficiently high OBS must be maintained to achieve a beneficial effect. These findings suggest that adherence to an antioxidant-rich diet and lifestyle assessment via OBS can help prevent prediabetes, IFG, and IGT in the general population. Future well-defined cohort studies are warranted to validate these findings.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251340616 - Supplemental material for Association of oxidative balance scores with the prevalence of prediabetes, impaired fasting glucose, and impaired glucose tolerance in the general US adult population: Evidence from NHANES 1999–2018
Supplemental material, sj-pdf-1-imr-10.1177_03000605251340616 for Association of oxidative balance scores with the prevalence of prediabetes, impaired fasting glucose, and impaired glucose tolerance in the general US adult population: Evidence from NHANES 1999–2018 by Hongpeng Guo, Junjie Zhang, Ying Qi, Chenglin Sun and Ji Wu in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605251340616 - Supplemental material for Association of oxidative balance scores with the prevalence of prediabetes, impaired fasting glucose, and impaired glucose tolerance in the general US adult population: Evidence from NHANES 1999–2018
Supplemental material, sj-pdf-2-imr-10.1177_03000605251340616 for Association of oxidative balance scores with the prevalence of prediabetes, impaired fasting glucose, and impaired glucose tolerance in the general US adult population: Evidence from NHANES 1999–2018 by Hongpeng Guo, Junjie Zhang, Ying Qi, Chenglin Sun and Ji Wu in Journal of International Medical Research
Footnotes
Acknowledgements
We sincerely thank all NHANES participants for their valuable contributions to this study.
Author contributions
Hongpeng Guo conducted the analyses and wrote the manuscript. Junjie Zhang and Ying Qi collected the study data. Chenglin Sun and Ji Wu contributed to study conception and design. All authors have read and approved the final manuscript.
Data availability statement
Declaration of conflicting interests
The authors declare that there is no conflict of interest related to this study.
Funding
This study was supported by the Liaoning Provincial Science and Technology Plan project (Grant no.2022JH2/1013).
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.