
Abstract
Background
Due to the deleterious effects on psychological health and wellbeing spurred by the pandemic, utilization of telehealth-based care increased over the past few years. The rapid transition from in-person to telehealth-based health service delivery has yet to be fully understood. The aim of the current study was to examine telehealth use for psychological help-seeking among college students using the Multi-theory Model of health behavior change (MTM) as a theoretical framework.
Methods
A cross-sectional and survey-based study was conducted among students at a large US university (N = 356). Valid and reliable scales were used to measure domains of psychological distress and MTM constructs. Participants were grouped based on past 12-month utilization of telehealth for any mental, emotional, or substance use problems.
Results
Roughly 67% of the sample reported that they needed help dealing with psychological distress, and 56.1%,43.3%, and 38.7% screened positive for anxiety, depression, and suicidal ideation, respectively. Depression, anxiety, and suicidal ideation were positively associated with past 12-month telehealth-based help-seeking. Past 12-month telehealth users reported greater advantages, confidence, and emotion direction toward telehealth-based psychological help-seeking than their counterparts. Participants also perceived higher exhibition of behavioral skills and greater social support to aid help-seeking than their counterparts. Advantages and disadvantages as well as behavioral confidence predicted intentions for telehealth-based help-seeking after controlling for anxiety, depression, suicidal ideation, perceived stigma, and perceived need for help among both groups.
Conclusion
The MTM theoretical framework is a valuable framework for predicting telehealth-based psychological help-seeking among college students. Such framework can be used to design and implement mental health programing.
“Providing social support and encouragement for telehealth use for psychological help-seeking may be key for sustenance of the behavior.”
Introduction
Mental health disorders are the single most influential factor on students’ academic performance, with concentration, motivation, and social interactions identified as important contributions to student success. 1 This is an important public health crisis due to the increase in mental health problems (anxiety disorders, depression, psychological distress, addictive behaviors) among university students in the past several years, with developmental changes, peer pressure, and academic stressors highlighted among triggering factors and stigmatizing attitudes acting as key barriers to mental health help-seeking. 2 Some suggest that college students may also exhibit higher levels of psychological distress, which includes a combination of anxiety and depression, 3 than other adults4-6; as many as 30-90% of college student samples have reported psycholgoical distress, and females have been identifed to be at increased risk, compared to males.4-8 This is particularly concerning given that 71% of college students have reported increases in stress and anxiety during the COVID-19 global pandemic. 9
During March 2020, colleges and communities experienced closures and lockdowns, respectively, due to public health measures taken to reduce the spread of the COVID-19 pandemic. While these measures were expected to save lives by reducing morbidity and mortality attributed to the virus, it was not without psychological consequences. Research has indicated that overall psychological wellbeing declined during the pandemic due to social isolation and lack of access to mental health resources,10-14 lifestyle risk factors such as excessive physical inactivity leading to sedentary behaviors15,16 as well as challenges in maintaining healthy lifestyle behaviors including exercise, and stress management. 16 Research also suggests that participants have experienced increases in severe symptoms of anxiety, depression, and stress as a result of the pandemic.12,13 Moreover, other studies have reported sleep disturbance, distress, and post-traumatic stress disorders (PTSD) in young people to be associated the pandemic.10-12 The fear and uncertainty of being infected with the virus; COVID-19 mitigation strategies (widespread travel restrictions, global disruption of academic activities, ban on mass gatherings and physical distancing) which had increased social isolation and loneliness; racial discrimination, COVID-19 related economic hardship, and hindrance to the provision of traditional psychological interventions10,14,17-22 have been reported to worsen the “physiological stress response” 16 of the Covid-19 pandemic leading to insomia, anxiety disorders and other mentally related outcomes. 16 A study evaluating the mental health of Canadian university students’ pre- and post-COVID-19, found students with no previous mental health concerns to report significant increases in depressive symptoms, anxiety, and ‘perceived stress’. 11
During the pandemic, opportunities for face-to-face psychological interventions for psychological distress became challenging; however, widespread accessibility of internet services and smartphone availability afforded the provision of safer online mental health services. 22 By offering online information and affording patients technologies for communication (internet, web-based, mobile-based, and digital applications), telehealth has been utilized for mental health information seeking and treatment of psychological problems.2,23 Even before the COVID-19 pandemic, telehealth has been highly utilized mental health information seeking and support,24,25 for patient management, access to education as well as specialty providers,26,27 due to its accessibility, anonymity, confidentiality, privacy, cost, and reduced stigmatization preferred by young audiences.2,28,29 Thus, telehealth is a viable option to help students with psychological distress access the healthcare they need.2,28,30,31
Despite the numerous advantages found to be associated with the utilization of telehealth in mental help seeking, studies have identified barriers to its use. While telehealth has been viewed as an alternative to traditional care, others are of the opinion that it should be considered complementary (not be replaced by) to traditional face-to-face consultation.2,24,25 Other documented concerns regarding telehealth use include reliability, accuracy of online information, privacy issues, credibility of digital applications, and difficulties with nonverbal communication.2,32,33
Theoretical Framework
The multi-theory model (MTM) was conceptualized exclusively for health behavior change with empirically tested constructs proven to be effective in predicting and influencing health behavior change.34-37 The MTM assumes that health behavior change involves two components: initiation (adoption of a one-time behavior) and sustenance or continuation (long-term performance) of the behavior change. 35 The multi-theory model has three constructs influencing initiation of health behavior change. The first is participatory dialogue, which is essentially a ‘two-way communication’ focused on the advantages outweighing disadvantages of the health behavior change (i.e., telehealth-based psychological help seeking). The second is behavioral confidence, which is the assumption that college students will seek telehealth-based psychological help in the future based on internal and external factors that are important to the individual (such as availability, accessibility of telehealth-based psychological resources). Finally, the third construct is changes to physical environment. Further these MTM constructs that influence initiation of a behavior change are believed to influence behavioral intention, which is the immediate predecessor of behavior change. 35
Based on the MTM, the sustenance or continuation of the health behavior change is related to three constructs: 1) emotional transformation, 2) practice for change, and 3) changes in the social environment. Emotional transformation involves a persons’ emotions toward a behavior, such as unitization of telehealth-based psychological help seeking. Practice for change involves experiencing continuous thoughts about the health behavior change coupled with overcoming existing barriers. Lastly, changes in the social environment include helpful relationships and social support.
The multi-theory model (MTM) has been shown to efficaciously predict, explain, and alter health behaviors 36 ; however, to date, no research has explored its utilization as a framework for understanding telehealth-based psychological help-seeking among college students. Therefore, the purpose of this study was to examine telehealth-based psychological help seeking among a sample of college students using the MTM as a theoretical framework. The multi-theory model (MTM) as a behavioral change theoretical framework 38 can offer lifestyle intervention levels that are useful for health practitioners and primary care givers in promoting health and preventing psychological disorders among young people.
Methods
Study Design and Protocol
The current study was a descriptive, quantitative, cross-sectional, and survey-based in design and was conducted in February 2021 among college students in a large public university in the Southern U.S. The inclusion criteria included 18 years or older, current enrollment in any of the University’s programs, ability to comprehend English language, and access to the internet. The study was approved by the sponsoring university’s institutional review board (protocol # 2102313710). Informed consent information which contained the aims of the study, the study significance, and the rights of the participants to withdraw at any time without facing any repercussions was provided to all participants, followed by explicit request for consent. Participants who agreed to participate were directed to the anonymous online questionnaire that prevented ballot boxing by allowing one response per I.P address.
The study utilized the convenience sampling method, and recruitment was done through a once weekly advertisement in the University’s daily e-news bulletin for duration of 3 weeks. The recruitment advert which contained an anonymous survey link with the details of the study was sent out to students who were currently enrolled and who had a valid University email address. The anonymous survey link, once clicked on, connected participants with the Qualtrics interface, and provided access to fill out the web-based survey. At the end of the survey, students were asked of their willingness to participate in a drawing to win one of five e-gift cards and if they answered yes, were directed to a separate e-survey which requested only an email address for contact purposes. The purpose of the separate link for the gift card was to prevent linking the email address provided to the previously recorded survey data.
Measures
Utilizing the MTM theoretical framework, a survey instrument was developed to assess the likelihood of initiation and sustenance of psychological help seeking behaviors. Psychological help-seeking was defined as attempts to access help or therapy services for emotional, mental, or behavioral health (e.g. substance use or compulsive behaviors) problem in the form of in-person office visits or virtually through use of electronic technology (i.e. telehealth) from formal sources (e.g. professional counselors, therapists, psychiatrists, psychologists or other physician/doctor).
MTM Theoretical Framework
The survey instrument consisted of seven items that addressed participants’ demographics and 33 items that assessed the seven constructs of the MTM (participatory dialogue – advantages and disadvantages, behavioral confidence, physical environment, emotional transformation, practice for change, and changes in the social environment). Each MTM item was scored on a 5-point Likert scale (0-4). Multi-item subscales were additively composited to produce variable metrics.
Participatory Dialogue
Participatory dialogue, the first construct in the initiation component of the MTM framework was assessed using six items each that examined participatory dialogue: advantages and disadvantages, with each item scored on a 5-point Likert scale (from 0-4) and a total possible score range of 0 to 24 units for advantages and disadvantages.37,39 The participatory dialogue score was obtained by subtracting the summed disadvantage score from the summed advantage score, a high advantage score and a low disadvantage score indicative of the likelihood of initiating psychological help seeking and the participatory dialogue score ranged from −24 to +24 units. 39 Sample item for participatory dialogue-advantages included “if you incorporate psychological help-seeking services …you will get the help you need” while sample item for participatory dialogue-disadvantages included “if you incorporate psychological help-seeking services you might…not be able to afford it”. Responses ranged from never, almost never, sometimes, fairly often to very often.
Behavioral Confidence
Behavioral confidence, the sureness that the behavioral change will be initiated with internal and external sources as drivers, 39 was assessed using six items that were scored on a 5-point Likert scale, with a total score that ranged from 0 to 24.37,39 Example of sample item used to assess behavioral confidence included “how sure are you that you can engage in psychological help-seeking despite finding it hard to talk about what is bothering you”.
Physical Environment
Changes in the physical environment (such as availability, accessibility of psychological resources) was assessed using three items with a score that ranged from 0 to 12.37,39 Changes in physical environment sample item included “how sure are you that you can find any needed resources to help you engage in psychological help seeking?”
The sustenance component of the MTM theoretical framework consisting of three constructs emotional transformation, practice for change and changes in the social environment 39 were each assessed. Emotional transformation (the direction of emotions towards psychological help seeking) was measured using three items, and scores ranged from 0-12. Sample item included “how sure are you that you can direct your emotions/feelings to the goal of engaging in psychological help-seeking as needed?” Practice for change was assessed with the use of four items and had scores that ranged from 0 to 16 with sample item “how sure are you that you can self-monitor your thoughts in order to engage in psychological help seeking when it is needed? Changes in the social environment was assessed using three items, had a score range of 0-12 units and a sample item “how sure are you that you can get the help of a family member to support you in psychological help seeking services as needed. 39
The MTM survey instrument’s face and content validity were assessed by a panel of six subject matter, instrumentation, and target group experts, with feedback provided and subsequent modifications made prior to the final survey instrument which utilized appropriate language that was clear, corresponding to the Flesch-Kincaid Grade Level five.37,40 To establish construct validity, confirmatory factor analysis using maximum likelihood estimation which resulted in a single factor solution for all subscales, with factor loadings above .32 and all Eigenvalues above 1.0. Further, Cronbach’s alpha evaluated internal consistency of the instrument subscales, using ≥ .70 as the established threshold for acceptability. 40
Statistical Analysis
The minimum sample size was calculated using G*power v. 3.1 software Power (University of Kiel, Germany), with an alpha level of .05, power .80, effect size of .15 (medium) and 6 predictors. After factoring in 10% incomplete entries or missing values, a minimum sample of 108 was obtained. All data analyses were carried out in SPSS Version 25 (IBM Corp). Means, standard deviations and frequencies were calculated for study variables where appropriate. Pearson’s product moment correlation analysis evaluated relationships between theory variables. Ordinary least squares multiple regression analyses were used to determine the MTMs ability to predict initiation and sustenance of telehealth-based help-seeking. Multiple regression models incorporated and controlled for sociodemographic variables which exhibited a significant bivariate relationship to criterion measures. Separate modeling was conducted based on those with a prior history of telehealth utilization and those without such experience.
Results
Descriptive Characteristics of the Study Sample (N = 356).
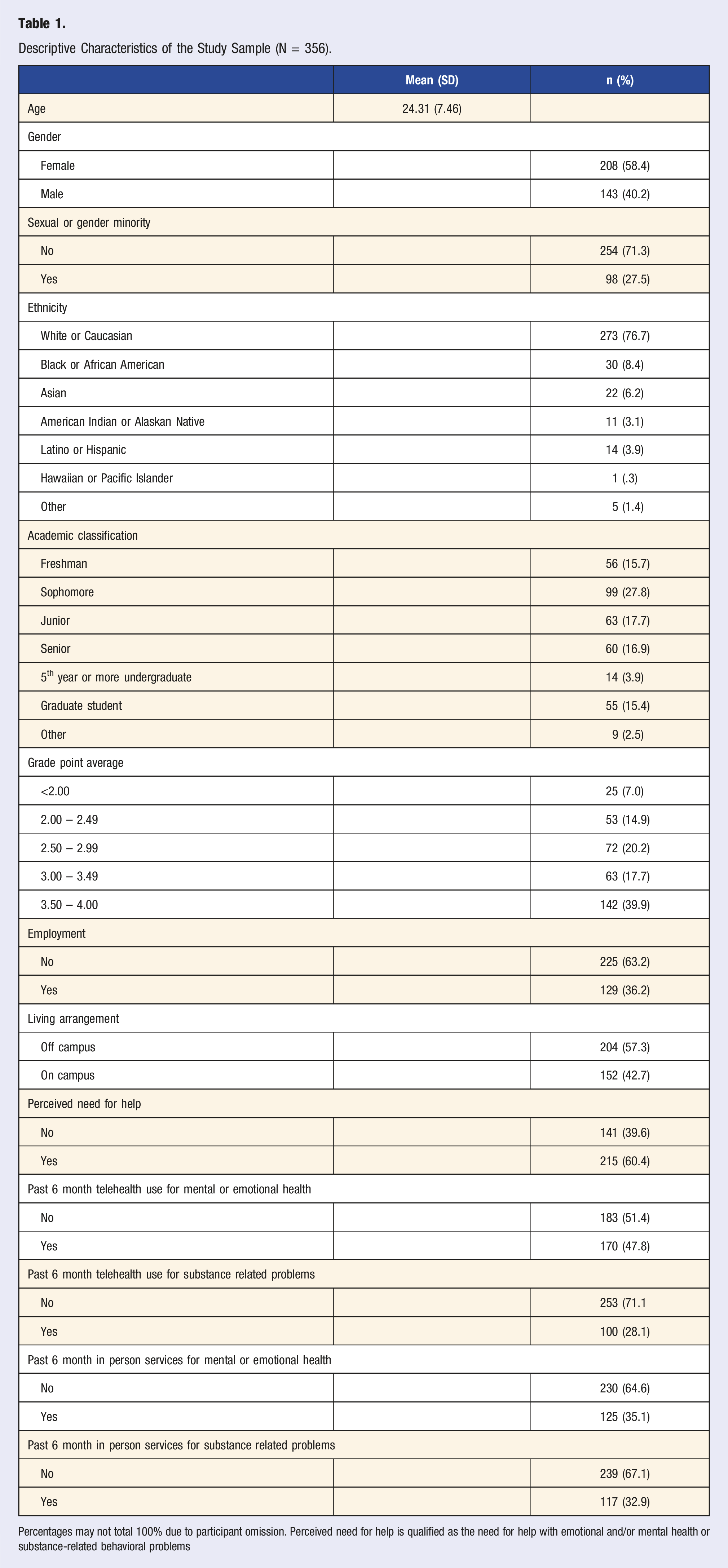
Percentages may not total 100% due to participant omission. Perceived need for help is qualified as the need for help with emotional and/or mental health or substance-related behavioral problems
Descriptive Statistics for Study Variables With Test of Group Means Between With and Without Past Six Month Telehealth Usage.
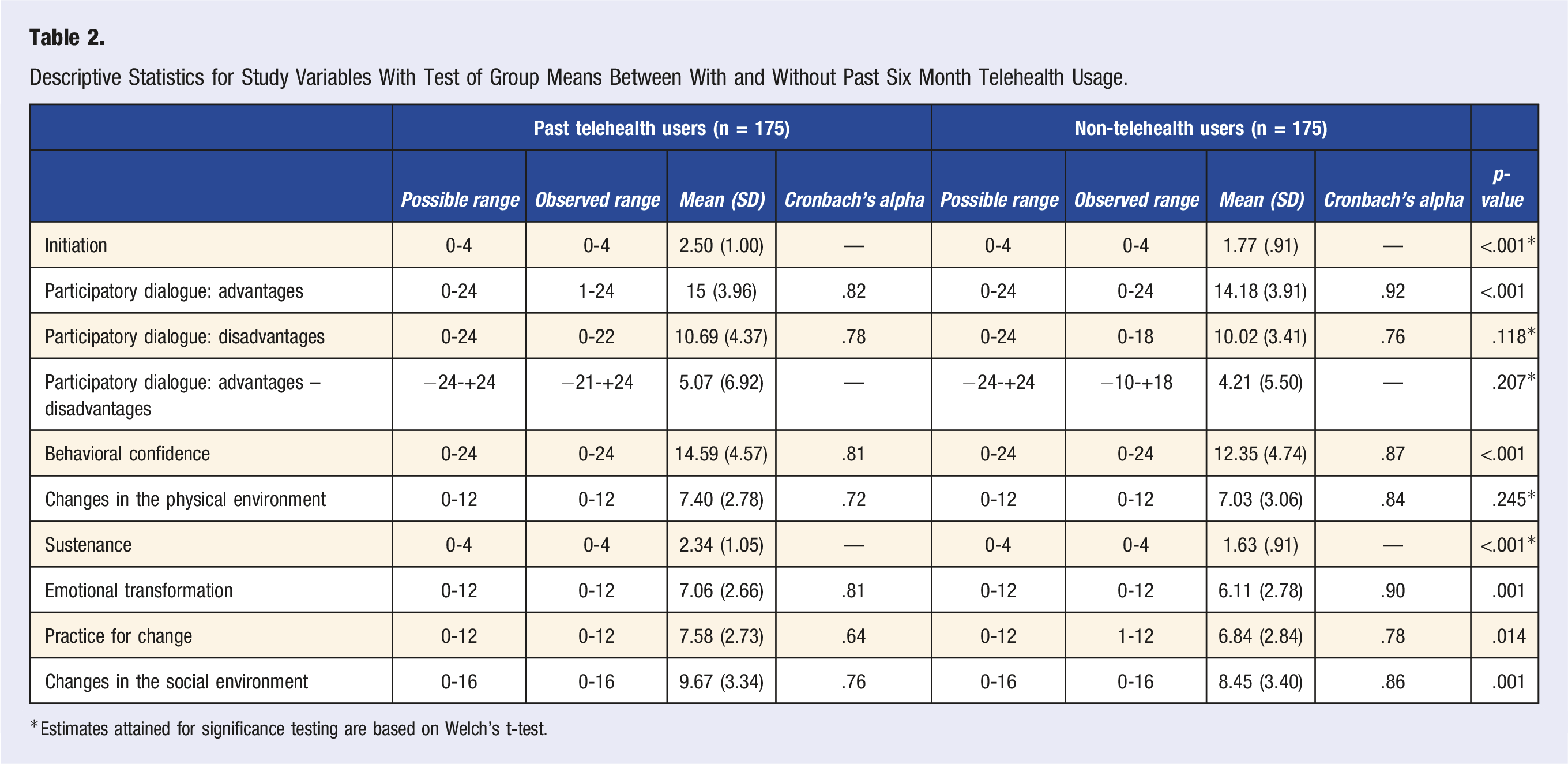
*Estimates attained for significance testing are based on Welch’s t-test.
Zero-Order Correlation Matrix of Study Variables.
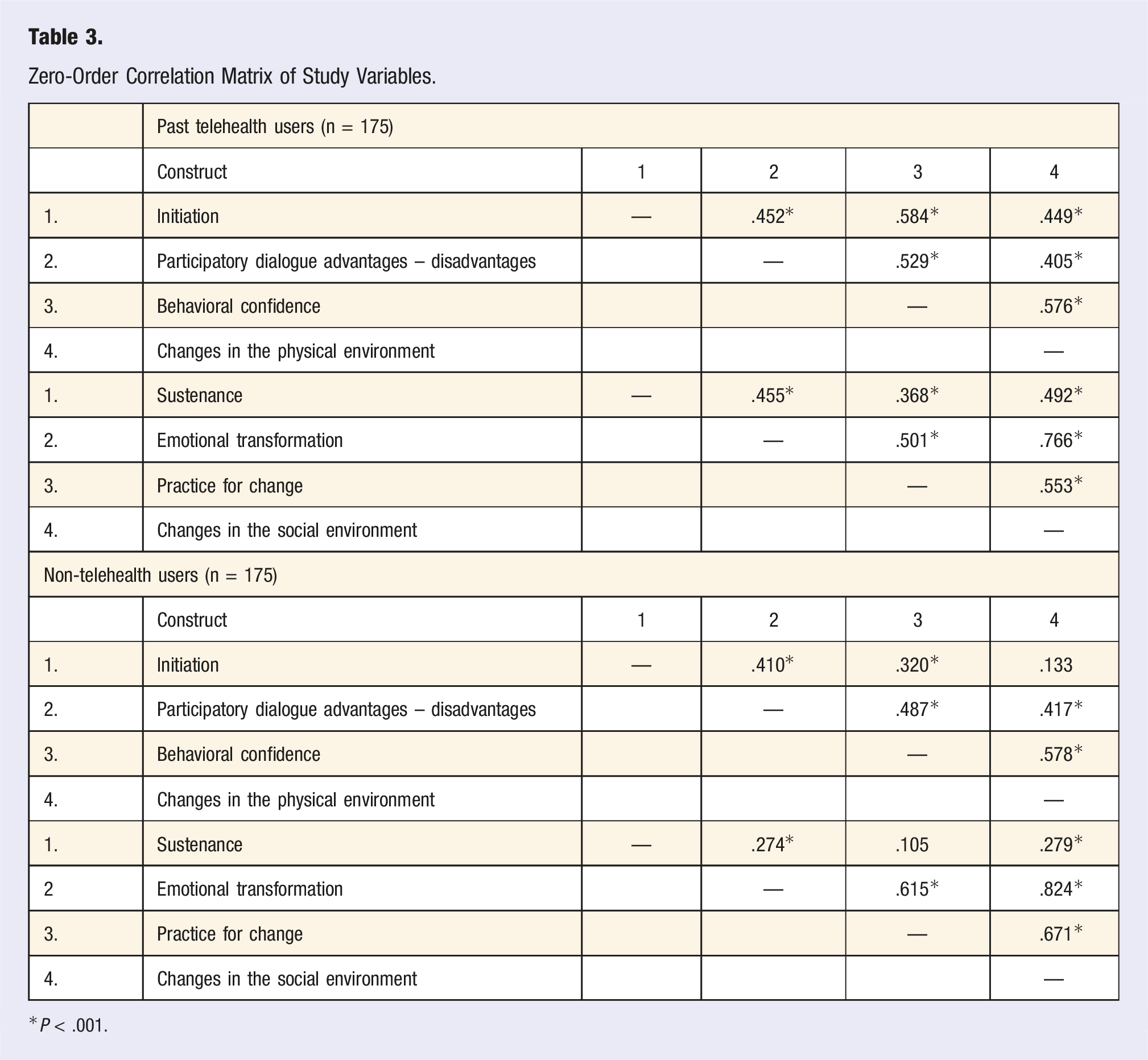
*P < .001.
Multiple Regression Models for Initiation and Sustenance of Telehealth (N = 356).
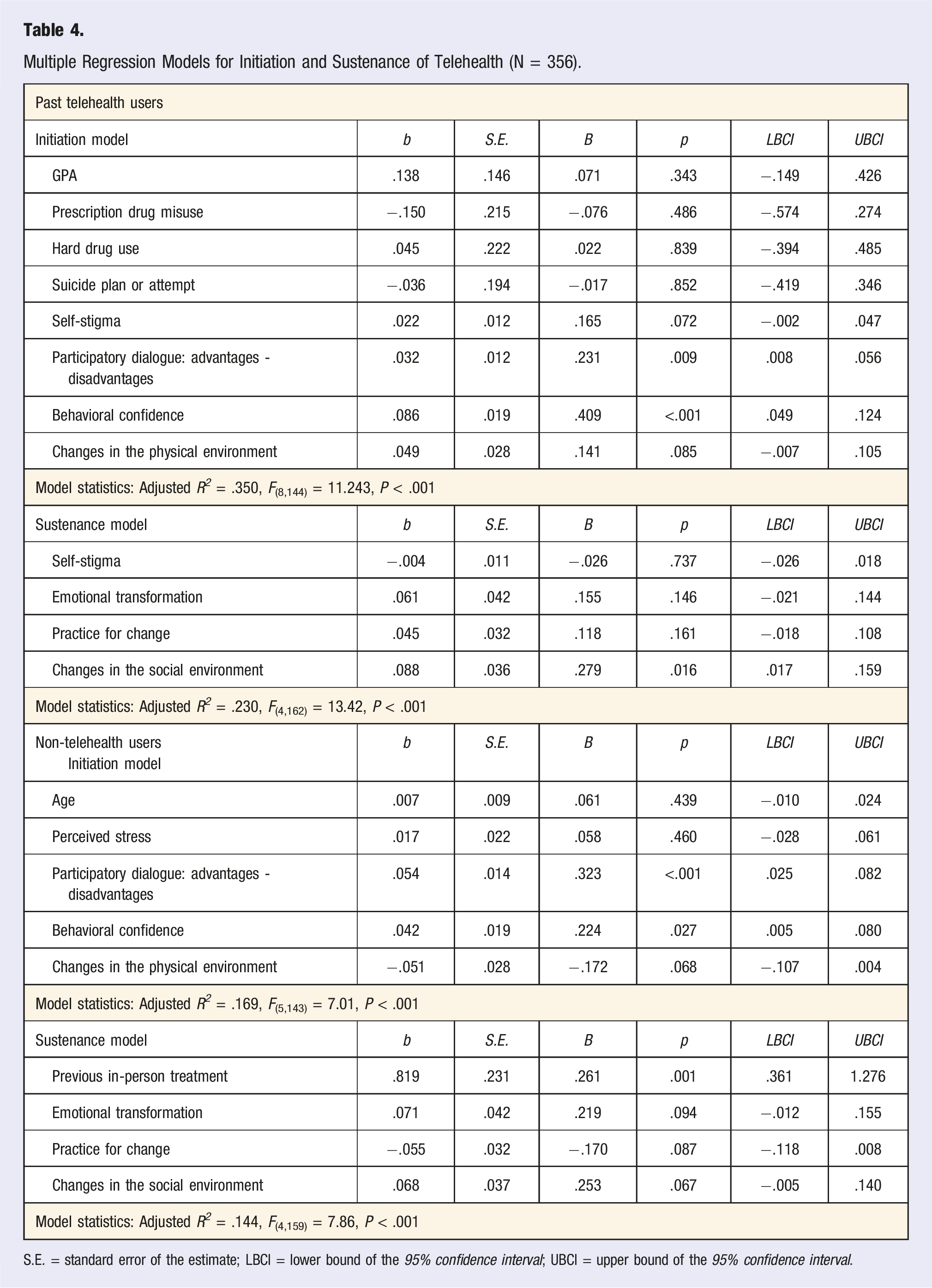
S.E. = standard error of the estimate; LBCI = lower bound of the 95% confidence interval; UBCI = upper bound of the 95% confidence interval.
Finally, among those with a history of previous telehealth utilization, 35% of the variance in initiation of telehealth use was explained (adjusted R2=.350, F(8,144) = 11.24, P < .001). In this multivariate model, participatory dialogue (advantages outweighing disadvantages) (β = .231, P = .009) and behavioral confidence (β = .409, P = <.001) significantly predicted initiation. For the sustenance model, changes in the social environment (β = .279, P = <.016) was the only significant predictor of sustaining telehealth usage (adjusted R2 = .230, F(4,162) = 13.42, P < .001)
Discussion
This study aimed to conceptualize telehealth-based psychological help seeking among college students using the multi-theory model of health behavior change. Overall, the MTM proved to be a useful framework in the assessment and prediction of the intentions to initiate and sustain psychological help seeking behaviors among the sampled college students. Similar to other college student samples,11,18,41 there was a high prevalence of psychological distress among our sample amid the COVID-19 pandemic. Significant increases have been reported in depressive symptoms, anxiety, suicidal ideation, and perceived stress levels among students during the pandemic.11,18 For example, a study that examined depression, anxiety, and traumatic stress during COVID, found more than a third of their sample exhibited anxiety symptoms, about 47% had depressive symptoms and one in five students reported suicidal ideation. 41 Further, the combined perceived susceptibility and severity of COVID-19 has led to increased social isolation, which has been associated with loneliness and stigma associated with contracting the disease. These factors are likely associated with elevated psychological dysregulation that has been observed among students.10,14,19-22,41
Further, poor help-seeking rates and utilization of mental health services have been reported among students who are at risk of mental health problems.42,43 In a study that examined mental health need and mental health services utilization, about half of the survey respondents who considered seeking help for the mental health related problems had ever utilized these services. 44 In addition to concerns about mental health and wellbeing, college students who experience psychological distress also report higher prevalence of alcohol and substance abuse than among their counterparts.45-47 Studies that examined mental health and its relation to health risk behaviors have found college students with high alcohol and substance abuse reported higher mental health problems such as self-injurious behaviors, attempts at suicide, psychological distress, poor mental health,45,46,48,49 and psychological distress. 5
The findings of this study showed the constructs of participatory dialogue (advantages outweighing disadvantages) and behavioral confidence to be consistent significant predictors of initiation of telehealth-based psychological help seeking among both groups (those with and without past 12-month telehealth utilization). These findings corroborate past reports that participatory dialogue (that emphasized advantages outweighing disadvantages) and behavioral confidence plays an important role in initiation of healthy lifestyle behaviors, such as exercise and smaller portion size consumption.34,36,50 Studies that examined intention to accept and adopt telehealth-based care, indicated the perception of its usefulness or benefits to be significant and were the proximal determinants of the behavioral intent to accept telehealth.51,52
Findings of studies on telehealth use behaviors have reported perceived ‘ease of use’ which closely relates to self-efficacy51,53 and perceived usefulness to significantly exert a much greater influence on the use of telehealth more than mere changes to the physical environment, including availability and accessibility of telehealth-based psychological resources.51,54 This could offer an explanation for our finding regarding the construct of changes in the physical environment not significantly predicting initiation of telehealth-based psychological help seeking adjusted modeling. Further, seeking help for psychological distress has also been shown to vary among college students 55 with females demonstrating greater likelihood of seeking care than males, and non-white populations less likely than whites to access and use mental health services when faced with mental health problems. 44 Thus, there may additional considerations that about the physical environment or the ease of use and perceived usefulness that should be explored by sub-population.
Changes in the social environment were found to be significantly associated with the sustenance of telehealth-based psychological help seeking among the sampled college students. Similar findings have been reported with other health behaviors in college students (e.g., physical activity), with a higher social support been associated with an increase adoption of healthy behaviors.34,36,56 Some studies have also posited, in addition, a possibility of an indirect influence of the social environment on health behavior change and that the influence might have been exerted through self-efficacy.56,57 Our methods did not specifically examine this possibility. However, among both groups analyzed in the current study, changes in the social environment held a significant positive bivariate correlation with sustenance. Previous utilization of in-person services was a significant predictor of intention to sustain telehealth use among non-telehealth users. It is suggested that absence of prior experience with mental health services (e.g., counseling, in-person mental health care, etc.) reduces the likelihood of telehealth use for mental health, and that increased awareness of and experience with mental health services increase college students’ intentions to use telehealth-based care. 58
Some of the recognizable barriers to seeking care, especially for mental health related problems, include various forms of stigma manifestations,28,31 language barriers, financial barriers,30,32 lack of awareness of available treatment options, doubts about the methods of care, as well as relatively high treatment cost and delayed access to care.44,59 Although, self-stigma was not a significant predictor following covariate adjustment in multivariate modeling, self-stigma for seeking help exhibited a significant negative bivariate association with telehealth-based psychological help seeking. Multivariate confounding may underlie a lack of significance following adjustment. It has been reported that stigma of psychological help-seeking among college students may potentially be reduced using telehealth-based care; however, college students still report perceived stigma despite telehealth use for psychological help seeking. 29 This perceived stigma has been shown to negatively impact their adoption and sustenance of use of e-mental health and traditional psychological services 60 for help seeking. Future research should continue to investigate the role of stigmatic perceptions related to help-seeking behaviors.
Limitations
This study had some limitations. The use of a cross-sectional design limits the establishment of causal associations between variables which could validate theoretical principles whereby cognitive attributes and environment-related constructs precede behavior. The study also utilized self-reported data which has the limitation of measurement bias, over and under-reporting, social facilitation, and acquiescence bias to name a few. Further, the measurement of the likelihood to engage in telehealth-based psychological help seeking (intention for initiation and sustenance) as a proxy for the assessment of actual telehealth use for psychological help seeking (actual behavior) is considered a limitation. However, taking into consideration that intentions have been shown to be a reliable proximal determinant of behavior, 61 the exploration of behavioral intention in this study is fitting. The use of convenience sampling limits the generalizability of the study findings to other populations.
Future Implications
Based on these research findings, designing interventions targeting participatory dialogue at individual, group, and campus levels as well as emphasizing the advantages, reducing perceptions of barriers or disadvantages of telehealth, and building confidence to initiate telehealth use is important for college students' initiation of telehealth-based psychological help-seeking amidst the Covid-19 pandemic. Providing social support and encouragement for telehealth use for psychological help-seeking may be key for sustenance of the behavior. Such social support may be provided via helpful relationships, rapport building, counsellor calls, and a combination of trust, caring, and openness between patients and providers. These future intervention levels (participatory dialogue, emphasizing advantages, reducing perceptions of barriers or disadvantages, as well as providing social support through helpful relationships) are useful in lifestyle medicine practices in the promotion of physical and psychological health. Furthermore, future research studies may consider designs inclusive of random sampling and prospective measurement of actual help-seeking behavior.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.