
Abstract
Type 2 diabetes (T2D), historically affecting primarily older individuals, now affects younger people. Few studies have analyzed diabetes risk factors among younger individuals, including college students. We investigated risk in that overlooked population. A 2-part diabetes risk assessment survey was administered to University of California Irvine (UCI) students, faculty, and staff for 2 months. Part I, including 26 questions, assessed participants’ nutrition, physical activity, and stress management behaviors. Part II assessed risk according to American Diabetes Association (ADA) Risk Assessment’s 8 demographic and lifestyle questions producing a risk score. Scores and behavioral factors analyzed risk on individual and community levels. Recruitment included emails and flyers promoting the UCI Electronic Educational Environment survey link. According to the ADA Risk Assessment scores of the 915 respondents, only 4% are at high risk of developing T2D. Although these scores indicate a small population at risk, our survey revealed a high prevalence of individuals practicing multiple unhealthy lifestyle behaviors associated with diabetes. These multiple behaviors may lead to high percentages of college students developing T2D, despite current low ADA risk status. We conclude the ADA Risk Assessment is geared toward an older demographic and may reflect short-term risk rather than longer-term risks.
‘The number of individuals with diabetes in 2012 was 29.1 million, 9.3% of the total population, an increase of 3.3 million Americans since 2010.’
The 2014 National Diabetes Statistics Report indicated an alarming change in diabetes in America. The number of individuals with diabetes in 2012 was 29.1 million, 9.3% of the total population, an increase of 3.3 million Americans since 2010. 1 The incidence of diabetes in 2012 was 1.7 million new diagnoses/year in adults aged 20 years and older. 1 Among the 29.1 million individuals with diabetes, 8.1 million are undiagnosed and potentially unaware of their diabetes risk. 1 In addition, 86 million Americans have prediabetes, for those ages 20 and older. 1 These statistics and lack of diagnosis highlight the need for more widespread prevention. Furthermore, while the total number and percentage of Americans living with diabetes has increased, elderly adults with diabetes has remained at 11.8 million, or 25.9% of the population aged 65 years or older. This indicates that the age range with the greatest growth in diabetes prevalence is those under 65 years old, including college-aged students. There is a growing need to address a population previously not considered at a high risk for diabetes. Developing an accessible and comprehendible diabetes risk assessment could increase diabetes awareness and provide guidance to those practicing at-risk behaviors.
Risk factors that have an established association with diabetes include age, family history, race/ethnicity, obesity, nutrition, adequate sleep, and physical activity. 2 Minority populations such as Asian Americans have a 9.0% risk for developing type 2 diabetes (T2D) in their lifetimes, compared to a 7.6% risk for non-Hispanic whites. 2 Asian Americans comprise over 50% of the University of California Irvine (UCI) campus population. Hispanics, which comprises approximately 21% of the UCI undergraduate campus population, have a 12.8% lifetime risk of developing diabetes. 2 The UCI campus community includes a spectrum of ages, including a large student population not traditionally perceived as high risk due to young age. In addition to the campus’ demographics, the typical and expected behavioral norms of college students are not necessarily healthy. The busy, technology-centered lives of the UCI students and employees may be paired with sedentary lifestyles and unhealthy eating habits. Diet and nutrition play a significant role in an individual’s risk for developing T2D. The added sugars from heavily processed convenience foods, often consumed while studying, cause sharp fluctuations in blood glucose levels, reducing sensitivity to insulin over time. The UCI population is frequently exposed to convenience foods and beverages on and off campus, encouraging a diet of highly processed foods devoid of nutrients and filled with refined carbohydrates and excess sugars. College stressors also contribute to lack of sleep and increased stress, both of which have an association with increased metabolic stress. These behaviors may feel out of the students’ control, but with proper health instruction these could be minimized, and their effect on diabetes risk reduced in this population. The purpose of our research was to better understand the diabetes risk of younger individuals in a college environment, by investigating associations between the lifestyles of the UCI campus community and their diabetes risk according to the American Diabetes Association (ADA) Risk Assessment.
Methods
Study Design
The research was approved by the University of California-Irvine Institutional Review Board (IRB Number 2013-9880). The cross-sectional survey was conducted for 8½ weeks, January through March 2014 (the survey is available online at http://ajl.sagepub.com/content/by/supplemental-data).
Sample Population
All active members of the UCI campus population with a valid UCInetID and password were eligible for participation in the survey. The campus community has a variety of ages and ethnicities, and the distribution of ages and ethnicities of participants were identified in the survey.
Data Collection
The survey was provided online through UCI’s Electronic Educational Environment Survey Tool, and promotion of the survey was done through flyers, Zotmail, YouTube Video Promo, Facebook, and social media postings and mass emailing. Gift incentives included the chance to win one of six $10 Veggie Grill gift cards.
Variables Measured
The Diabetes Risk Assessment of the UC Irvine Campus Population is composed of 2 parts. Part I included questions on lifestyle and behaviors factors, including the following:
Campus status
Ethnicity
Place of residence
Hours of sleep per night
Consumption of fruits and vegetables
Dietary habits
Physical activity
Knowledge of resting heart rate and target heart rate
Stress manifestation
Stress management
In the survey, examples were included to define physical activity levels. Light physical activity included leisurely walking. Moderate physical activity included dancing, briskly walking, swimming, and bicycling. Vigorous-intense physical activity included running, fast swimming, fast cycling, and aerobic exercises.
Part II consisted of the official ADA Risk Assessment. 3 Part II evaluates individuals’ risk of T2D by assigning a score based on responses to survey questions. A score of 6 and above indicates high risk for T2D. Risk factors assessed in Part II included the following:
Age
Sex
Family/personal health history
Physical activity
Weight
Ethnicity
Data Analysis
Rcmdr was used for statistical analysis. Statistical measures and tests included χ2 tests, odds ratios, and summary statistics, with an α level of .05 and 2-sided P values for all tests. Nominal and ordinal variables were coded for a number for calculations. Compilation of graphs and tables were performed on Microsoft Excel and Word.
Results
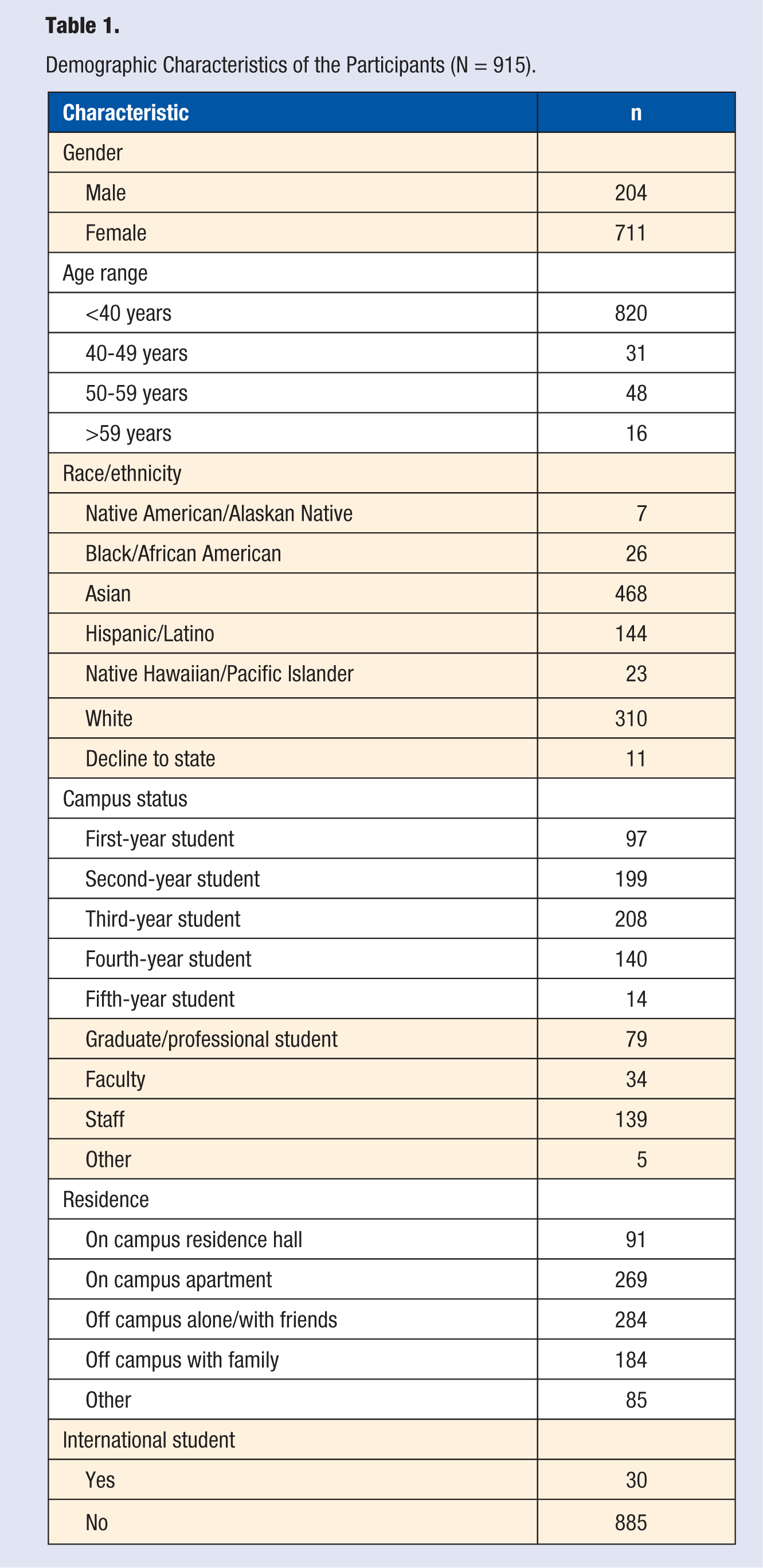
A total of 915 UCI community members participated. A demographic breakdown of the participants is found in Table 1. Ninety percent of the survey participants were less than 40 years old, and 81% were students, 51% of the respondents were Asian American, and 16% were Hispanic/Latino, roughly similar to their proportions in the UCI student body. Despite the fact that only 4% of the participants were identified as high risk for T2D according to Part II ADA Risk Assessment, a variety of high-risk behaviors were prevalent according to our survey. Significant correlations were observed between health behaviors, specifically the high association of practicing multiple high-risk behaviors.
Demographic Characteristics of the Participants (N = 915).
Significant correlations were found between the following: daily breakfast consumption and hours of sleep, vegetable consumption and type of diet, days engaged in vigorous physical activity and the number of meals consumed per day, and fast food consumption and buying fast food meals on campus. These daily behaviors have long-term effects that can lead to the increased risk of T2D onset, especially when multiple unhealthy behaviors are conducted together. 4
A high percentage of the respondents were not reaching the healthy amount of 8 hours of sleep per night, 78% of undergraduates indicated 7 or less hours of sleep, 73% of faculty and staff indicated 7 or less hours of sleep, and 66% of graduate students indicated 7 or less hours of sleep. There was a correlation found between students who reported not consuming breakfast daily and getting 7 or less hours of sleep per night (P = .002859). Of the students who do not eat breakfast 79% of them also sleep 7 or less hours (Figure 1). While sleep plays a role in the body’s metabolism and helps stabilize blood glucose, a balanced breakfast also has a vital role in stabilizing blood sugar.5,6 Those who are neither getting adequate amounts of sleep nor beginning their day with breakfast are increasing their chances of metabolic stress, and increasing their risk of diabetes. 6
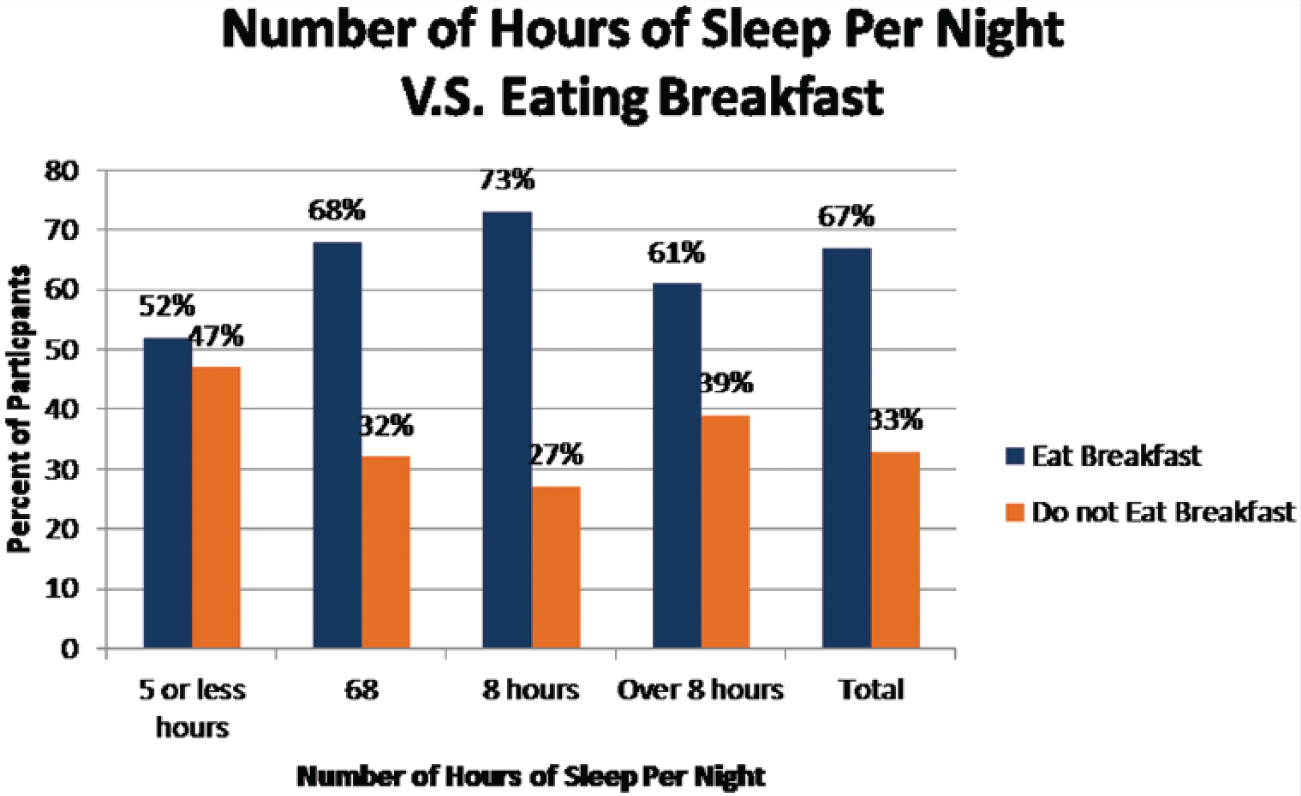
Number of Hours of Sleep per Night Versus Eating Breakfast.
Produce consumption is a key factor in blood glucose regulation and a healthy lifestyle.7,8 There was an association between self-identified eating type and the number of daily fruit servings (P < .001). A majority, 72.97%, of omnivores ate only 0 to 2 servings of fruit a day, and 52.27% of vegetarians ate 0 to 2 servings of fruit a day. There was another strong association, between self-identified eating type and daily vegetable consumption (P < .001). A total of 65.32% of omnivores ate only 0 to 2 servings of vegetables a day, and 43.18% of vegetarians ate 0 to 2 servings of vegetables a day (Figure 2). Unexpectedly, even among vegetarians many did not consume recommended amounts of produce.
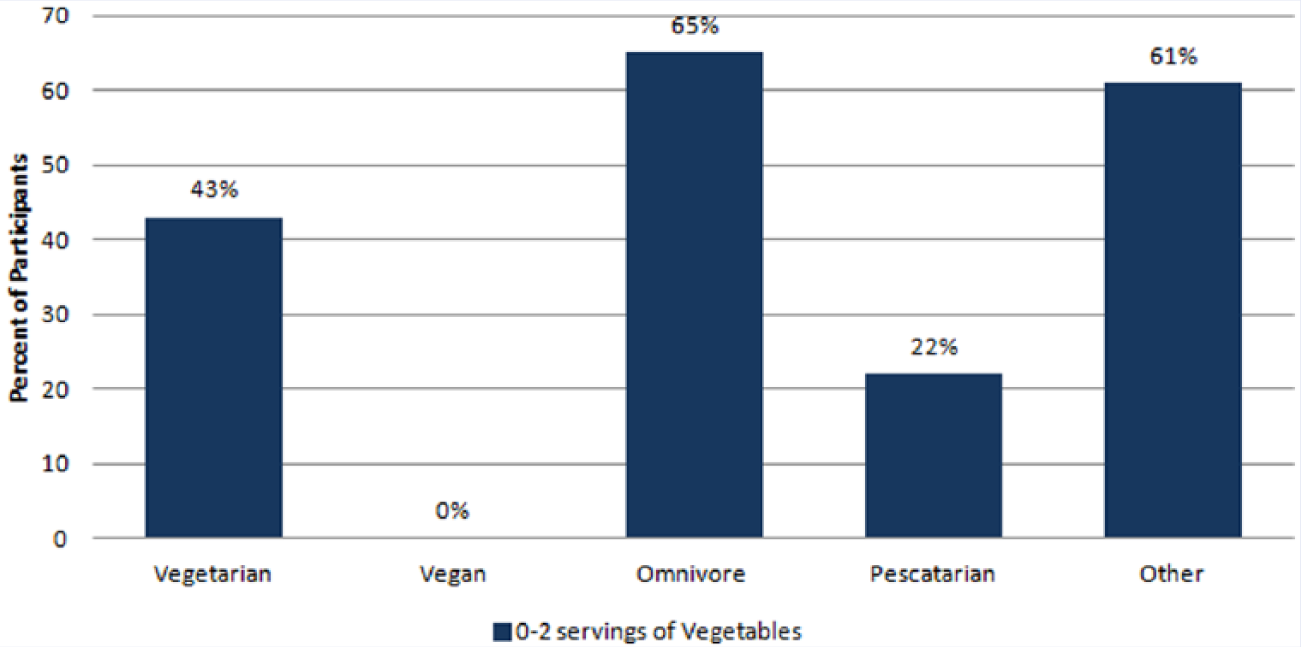
Percentage of Participants’ Vegetable Consumptions.
A college student’s lifestyle often involves inconsistent meal times and portions. Forty-one percent of all respondents ate 1 to 2 big meals per day. Regular physical activity and consumption of several smaller meals over the span of the day has a positive effect on maintaining healthy glucose levels.9,10 Physical activity and meal consumption practices were strongly associated among the campus population (P < .001). Eighty-four percent of those who engage in only 0 to 2 days of vigorous activity consume 1 to 2 big meals per day, while 78% of respondents who eat 6 or more meals per day engage in 3 or more days of vigorous activity (Figure 3). These study data again showed associations between those who exhibited one risky health behavior, such as little physical activity, and participation in an additional risky health behavior.
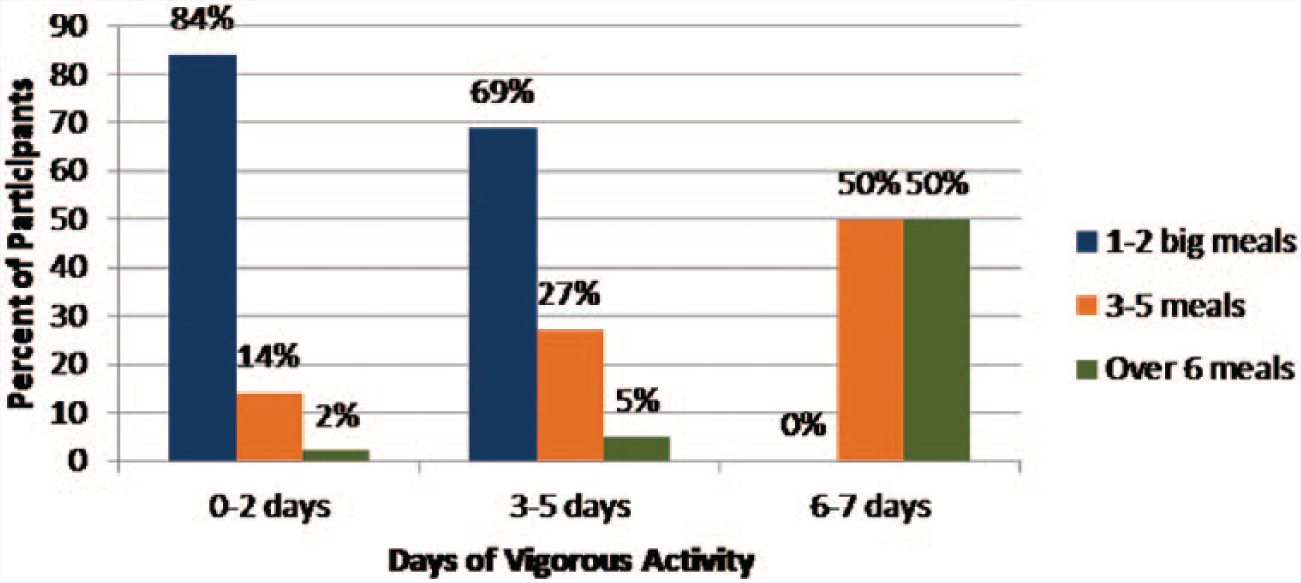
Days of Vigorous Activity Versus Number of Meals per Day.
Physical activity and wellness knowledge are important in maintaining healthy body weight.11,12 There is an association between how often respondents engage in vigorous exercise and whether or not they know their training heart rate (P < .001); 86% those who engaged in vigorous exercise 2 days or less did not know their training heart rate.
According to our survey, 52% of those participants who ate fast food for at least half of their meals also bought over half of their meals from a UCI campus restaurant (P = .009; Figure 4). Processed and fast foods have been shown to increase the risk of many chronic conditions, including diabetes. 13 The fact that the UCI campus population is readily obtaining so much fast food on campus is indicative of the changes that need to happen for a healthier campus.13,14
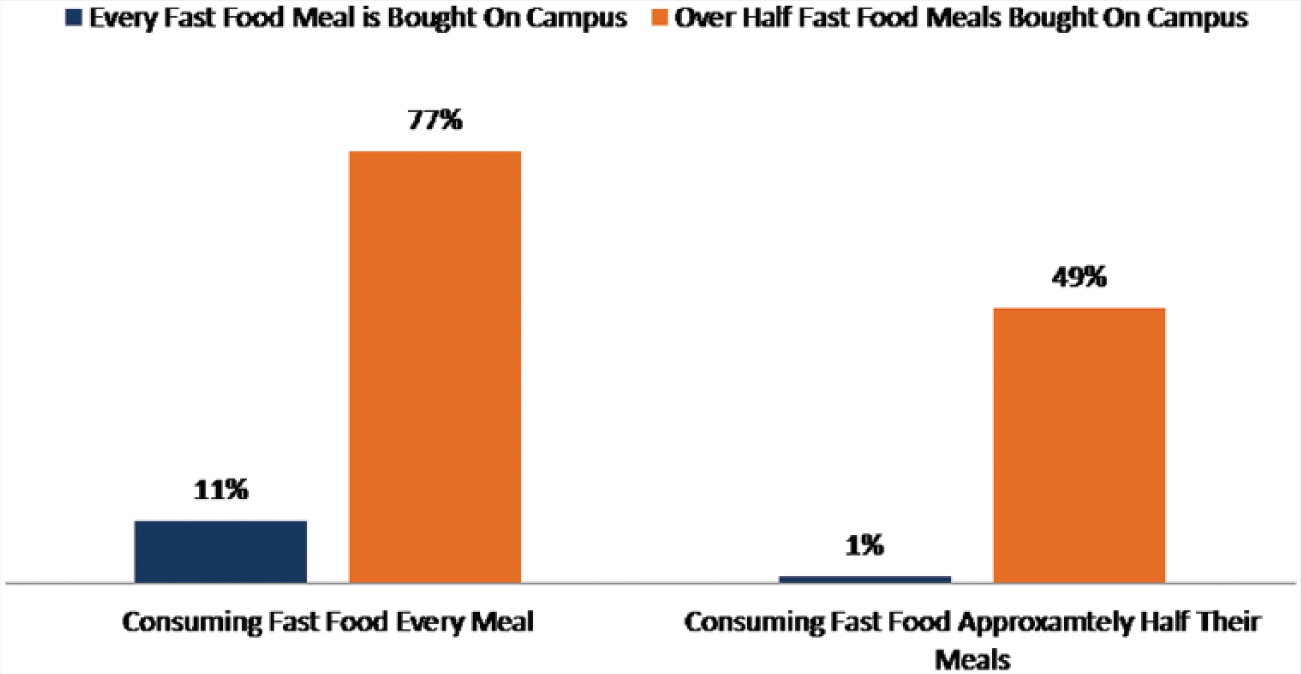
Fast Food Consumption Versus Fast Food Meals Bought On Campus.
Limitations of Study
The Diabetes Risk Assessment of the UC Irvine Campus Population is a voluntary survey. Respondents may have had a prior interest in health or T2D. The survey did not include questions on smoking or alcohol consumption, questions on stress manifestation through insomnia and digestion problems, or question about participants major, school department, or exact age (age group was reported in Part II of the survey).
Discussion and Conclusion
In order to combat the alarming diabetes increase in young adults, research needs to be done outside of the typical physiological and one risk factor at a time methodology. This population is often overlooked in comparison to children and older adults. Even established diabetes advocacy groups are missing this demographic. The ADA Risk Assessment is geared toward an older demographic and may better reflect short-term risk, as seen in physiologic status, rather than long-term risk of diabetes for younger adults exhibiting risky health behaviors.
Given the increase in diabetes around the nation and specifically in those under the elderly age range, there needs to be a change in how young and middle-aged American adults are targeted for diabetes prevention. This study identified several health behaviors that may be best addressed for young adults if targeted together. Further research on additional college campuses will better explain where the focus needs to be placed on targeting preventive and intervention efforts.
As shown in the study, the ADA Risk Assessment needs to include changes targeting young adults, as the age group believed to be at risk for T2D no longer applies exclusively to middle-aged and elderly adults. Changes made to the ADA Risk Assessment should include questions geared toward specific age groups, and more questions focused on lifestyle factors, such as regular breakfast consumption, and daily servings of fruits and vegetables. Questions on the ADA Risk Assessment such as whether or not a respondent considers themselves to be physically active is subjective and could differ based on cultural background and needs to include specific definitions. These lifestyle factors play a role in the risk of developing T2D as they contribute to the day-to-day health habits.
A preventative focus of T2D risk in young adults would allow young adults to evaluate their risk for T2D before they become middle-aged adults and can help promote a shift toward implementing healthier behaviors and exercise habits when they are still young and healthy.
This research can be replicated on other campuses. The importance of diabetes prevention in young adults rests in raising awareness of risky health behaviors and their effects in the future. Replicating the study on different campuses will provide more diverse results and justification of the need for young adult–targeted risk assessments. This can be completed by surveying college-age students living in different geographic regions, and coming from an array of different cultures, backgrounds, and religions.
The follow-up study of the project, a disease prevention program specifically tailored to the needs of the UCI campus population, uses these results as baseline data to assess the impact of young adult diabetes prevention. This program is currently being conducted through spring 2015.
Footnotes
Acknowledgements
Professor Bic, for guidance, support, and expertise; Professor Bartell, for help in statistical analysis; Allison Hickey and Consuelo Siposs at the ADA, for cooperation and guidance; Dr Ogunseitan and Sarah Link, for help in promoting the survey; and Program in Public Health at UCI for support.
Authors’ Note
Study was presented at UCI UROP Spring Symposium, May 2014; ASPPH Undergraduate Education for Public Health Summit, November 2014; and Building Healthy Academic Communities National Summit, April 2015. This work was supported by the University of California–Irvine Undergraduate Research Opportunities Program (Grant Number 48540s1).