
Abstract
Background: The Complete Health Improvement Program (CHIP) has demonstrated effectiveness in improving multiple cardiovascular disease risk factors. CHIP promotes physical activity, as well as a plant-based whole-food diet. The study objective is to evaluate the effectiveness of CHIP on improving levels of physical activity. Methods: CHIP participants had biomarkers measured at baseline and after the 11th session, consisting of level of physical activity, blood pressure (BP), body mass index (BMI), fasting blood sugar (FBS), and lipid panel. Pre and post data were analyzed using paired t-tests. Results. CHIP demonstrated significant increase in level of physical activity (P < .001) and decreased BMI, FBS, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglycerides (all P < .001). Increased levels of physical activity correlated with decreased BMI (P < .001), but not with other biomarkers. Conclusion: CHIP is effective in producing increased level of physical activity and improvement in multiple biomarkers. The increase in physical activity is correlated with decreased BMI.
CHIP effectively increases levels of physical activity and improvement in multiple biomarkers; the physical activity level is correlated with decreased BMI.
Introduction
Cardiovascular disease (CVD) is the leading cause of death globally and carries a broad array of impacts on the individual and society. 1 Modifiable risk factors for CVD include smoking, hypertension, obesity, sedentary lifestyle, and poor nutrition, reflected in lipids levels and glycemia. 1
Physical activity plays an important role in improving multiple CVD modifiable risk factors; sedentary behavior, hypertension, dyslipidemia, hyperglycemia, and elevated body mass index (BMI), thereby decreasing the risk of atherosclerosis.2-6 Improvements in diet and exercise combined have a much greater impact on improving body mass index (BMI) and lipids than either individually.5,7
The Complete Health Improvement Program (CHIP) is a comprehensive program that seeks to reduce CVD risk through promotion of a plant-based diet, increased physical activity, and improved health literacy. 8 It has documented effectiveness globally, and particularly in this study population in Appalachia, Ohio.8,9 Much of the research in this program has focused on diet combined with exercise to demonstrated reductions in CVD risk factors.
The purpose of this study was to evaluate the effectiveness of CHIP to specifically change levels of physical activity, and to identify correlations between the changes in physical activity and other CVD risk factors.
Methods
Retrospective data were evaluated from consenting CHIP participants in Athens, Ohio from 2011 to 2021. CHIP classes were provided by Live Healthy Appalachia, a local nonprofit organization that promotes healthy eating and active lifestyles in the region. As part of the enrollment process, CHIP participants were asked to sign a consent permitting use of their personal data to be de-identified and aggregated for analytical purposes. Approval for this study was obtained from the Ohio University Institutional Review Board (16-X-44) and registered with ClinicalTrials.gov (NCT03025451).
Complete Health Improvement Program Intervention
CHIP has been utilized in clinics and communities for over 25 years to empower participants to choose healthy lifestyle practices to prevent, arrest, and reverse chronic lifestyle-related disease, and has gone through many modifications. 8 In this study, participants took part in 16–18 sessions over 2–4 months. Prerecorded videos and group activities were used for instruction. Group activities consisted of group discussions, physical activity, and cooking demonstrations.
Participants were instructed to work toward at least 30 min of moderate physical activity or 10,000 steps daily. Strength and resistance training for 20–30 min 2–3 days a week was also recommended.
Participants were also encouraged to follow a minimally processed, predominantly plant-based, whole-food diet, focused on vegetables, fruits, cooked whole grains, legumes, and limited nuts and seeds. Dietary objectives of CHIP were daily consumption of fat as less than 20% of daily calories, less than 10 teaspoons of added sugar, less than 2000 mg of added salt, cholesterol less than 50 mg, and 35–40 g of fiber. Also recommended were daily stress reduction techniques.
Data Collection
At the beginning of the program, and again after the 11th session, participants completed a health history, including a multiple-choice question on physical activity: What is your level of exercise beyond your everyday occupation? Choice options were none, mild (2–3 days/week), moderate (3–5 days/week), and vigorous (4–6 days/week).
Participants also had fasting venous blood samples collected at the local community hospital using a standard technique, and analyzed for total cholesterol (TC), triglyceride (TG), low-density lipoprotein (LDL-C), high-density lipoprotein (HDL-C), and blood glucose (BG) on commercial analyzers. BMI and blood pressure (BP) were measured by trained medical professionals near the time of the blood draws. Data was stored in a password-encrypted database located at Live Healthy Appalachia.
Data Analysis
Descriptive statistics were performed to describe and summarize the data. The corresponding frequency, percent distribution, mean and standard deviation (SD) were reported. Bivariate analysis was performed using chi square test to compare pre and post physical activity levels to determine if the change in physical activity level was statistically significant. A variable to denote change in physical activity level between pre and post intervention was created. Its negative value indicated that pre intervention physical activity was greater than post intervention. A value of “0” indicated that the level of physical activity did not change. A positive value indicated that post intervention physical activity level was greater than pre intervention. ANOVA was performed to determine association between study variables and change in physical activity level. Paired t-test was performed to determine change in pre and post biomarkers; P value <.05 was considered statistically significant. All analyses were performed using SAS 9.4
Results
Data were analyzed for 710 participants of 37 CHIP classes: 180 (25.4%) male, 530 (74.6%) female, age range of 17 to 84 years, with a mean of 51.9 and SD, 12.87 (Table 1). There was a significant difference in the mean age of males and females (P = .004). For males, the mean age was approximately 54 years, and for females, it was 51 years.
Baseline Characteristics of the Study Population (N = 710).
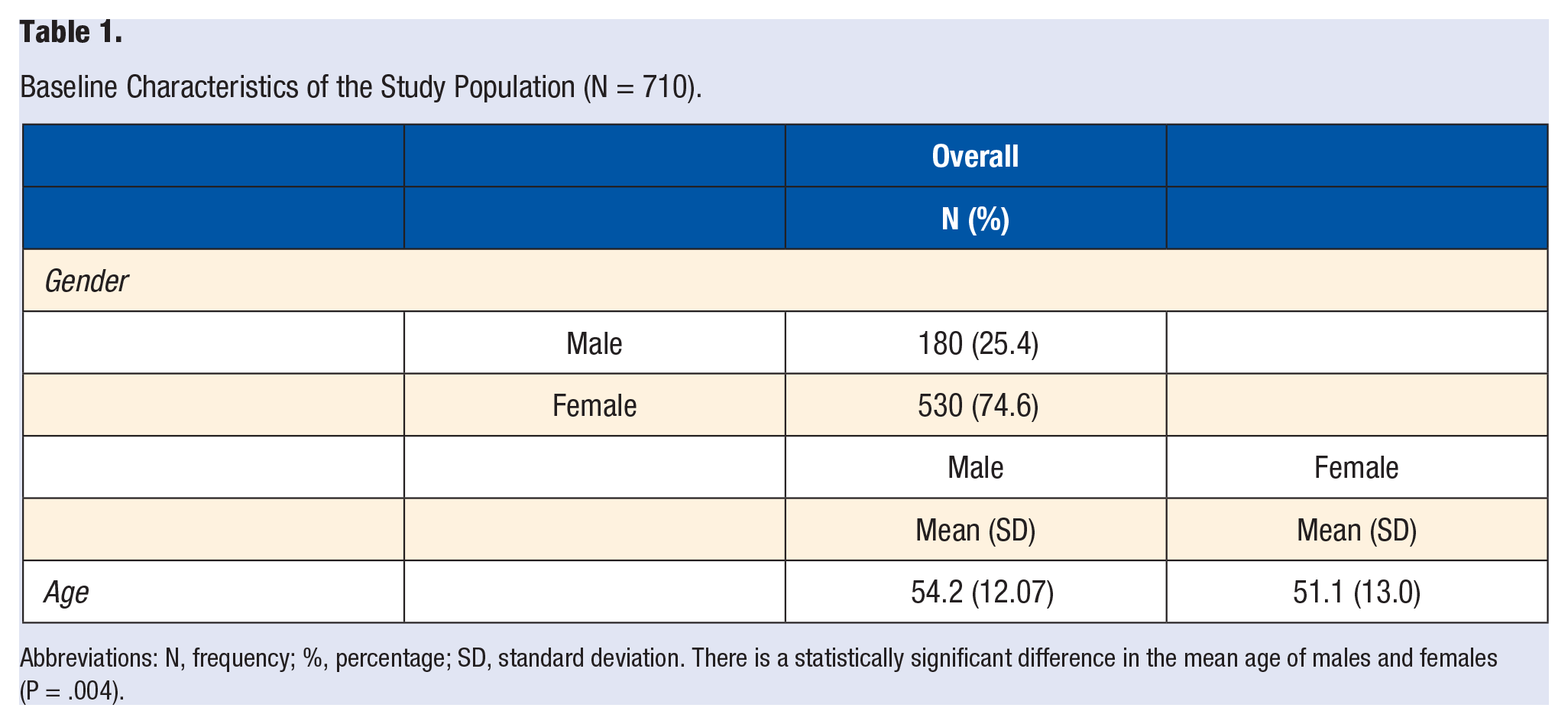
Abbreviations: N, frequency; %, percentage; SD, standard deviation. There is a statistically significant difference in the mean age of males and females (P = .004).
Complete health improvement program produced decreased BMI, FBS, TC, HDL-c, LDL-c, and TG (all P < .001) from pre to post intervention (Table 2). There was an increase in physical activity from pre to post intervention (P < .001) (Table 3 and 4). There was no statistical difference between change in physical activity and age and gender. Increase in physical activity was correlated with improvement in BMI (P < .001), but there was no correlation with other variables (P > .05) (Table 5).
Comparing Change in Study Parameters Pre and Post Intervention.
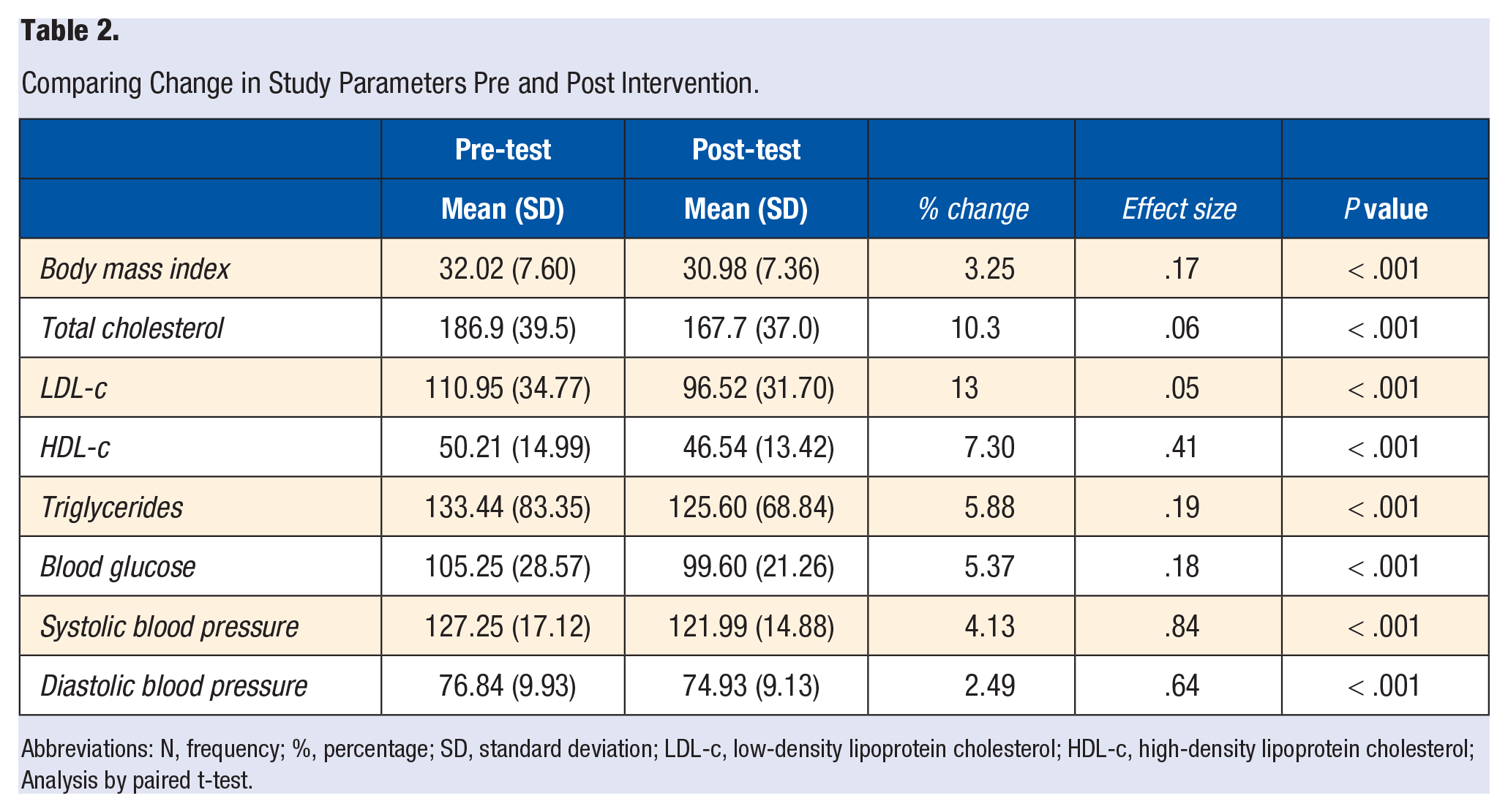
Abbreviations: N, frequency; %, percentage; SD, standard deviation; LDL-c, low-density lipoprotein cholesterol; HDL-c, high-density lipoprotein cholesterol; Analysis by paired t-test.
Change in Exercise Level.
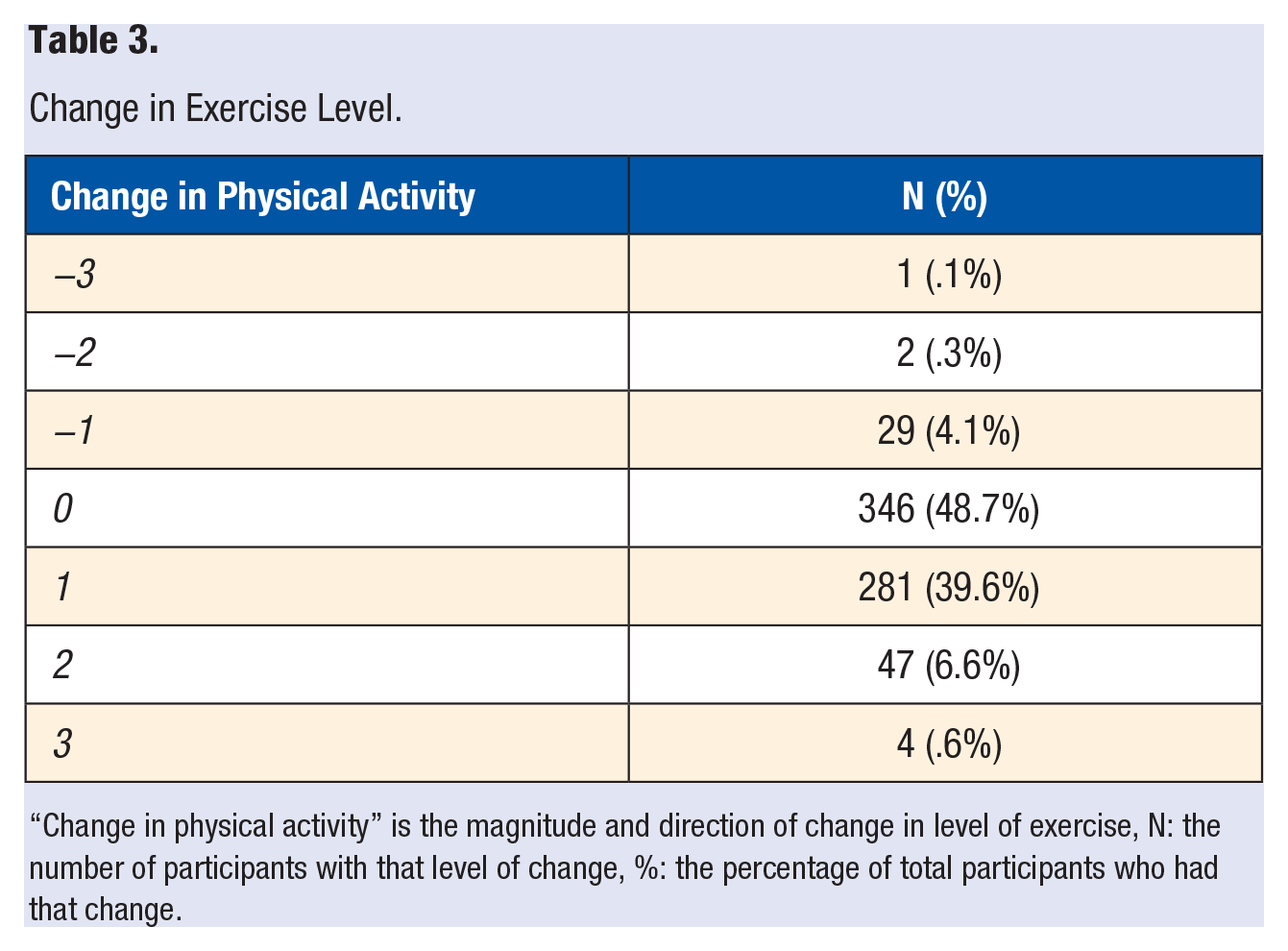
“Change in physical activity” is the magnitude and direction of change in level of exercise, N: the number of participants with that level of change, %: the percentage of total participants who had that change.
Change in Levels of Physical Activity.
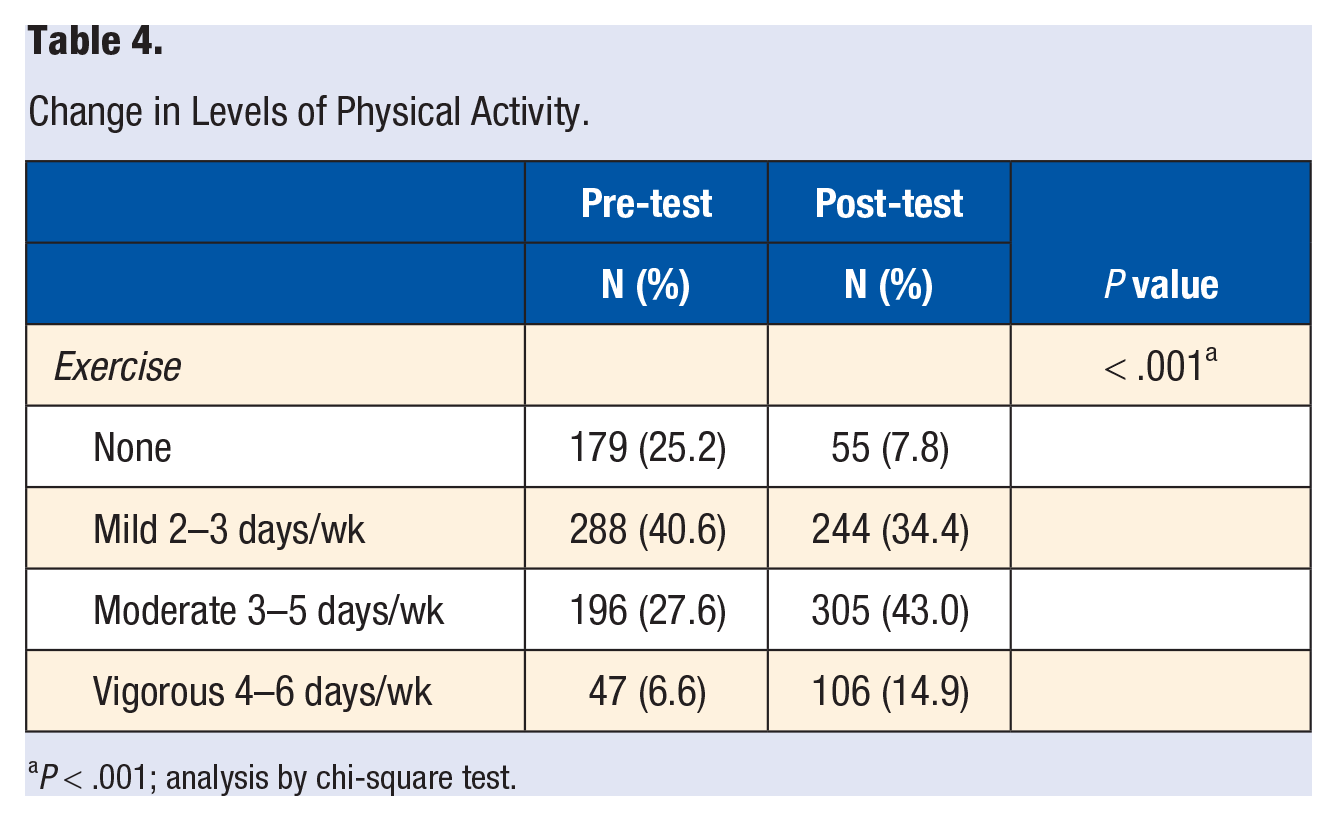
P < .001; analysis by chi-square test.
Association Between Biomarker Changes and Change in Physical Activity.
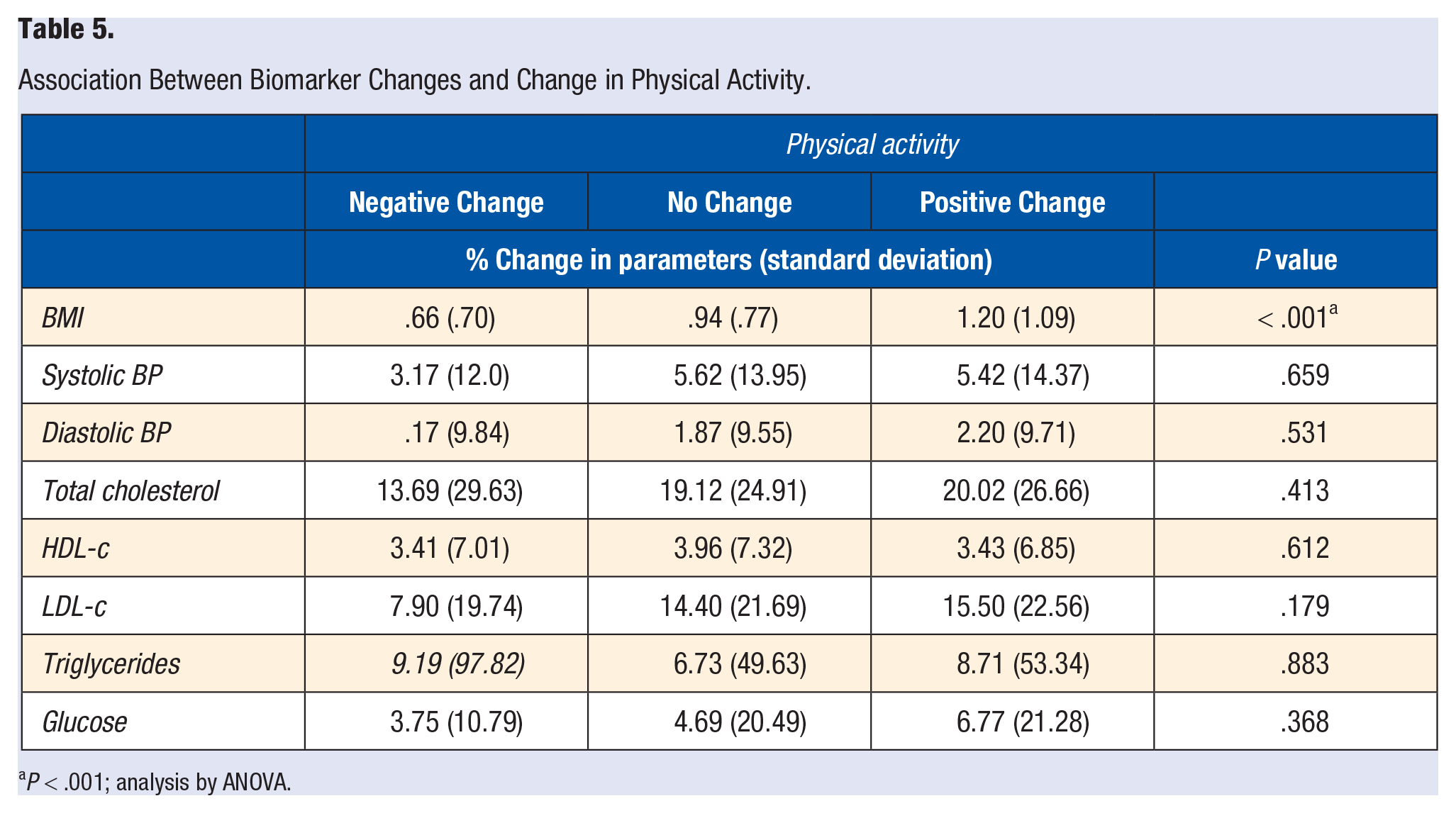
P < .001; analysis by ANOVA.
Discussion
The purpose of this study was to evaluate the effectiveness of CHIP to change levels of physical activity, and to identify correlations between the changes in physical activity and other CVD risk factors. In this study of 710 participants, there was an overall increase in physical activity, which correlated with improvement in BMI, but not with other variables. Although not statistically significant, changes in diastolic BP, TC, LDL-c, TG, and BG tend to be greater with physical activity as compared to no change in physical activity.
Participants who had a decrease in physical activity during the program also demonstrated an improvement in BMI, but to a lesser degree, which is consistent with studies that demonstrate the combined effectiveness of diet and physical activity have a greater effect than diet alone.5,7
Exercise has been shown to be a cost-effective means of lifestyle management of cardiovascular disease.10-13 In 2005, Anderson et al calculated an individual increase in medical expenses of $1543 per year for sedentary people. 14 Conversely, following CDC recommendations would save about $19 of medical expenses per hour of moderate exercise. 15
A sedentary lifestyle has been shown by Owen et al. to be an independent, but easily modifiable, risk factor for a variety of CVDs. 16 Studies have shown that increased exercise has been associated with decrease in diastolic blood pressure, triglycerides, and blood glucose.2,4,17-20 Although exercise alone is effective in producing weight loss, dietary and exercise interventions combined have an even greater impact on BMI.5,7,20,21 By reducing BMI in obese individuals, risk of stroke, and myocardial infarction are reduced. 21
Reductions in various lipid values are seen in studies with diet and exercise modifications resulting in a decrease in myocardial infarction risk.22,23 In this study, very generalized dietary data was collected, making it difficult to evaluate the specific effect of dietary changes as compared to physical activity. Both exercise and plant-based diets are able to decrease triglyceride levels.5,6,24 Triglyceride improvement with CHIP has been documented but prior studies in this particular population have shown less marked improvement.34,35 The reason for this is unclear.
Consistent with other studies on plant-based diets, in this study, HDL-C levels decreased. This has been discussed elsewhere and is thought to be a compensatory response to the dramatic decrease in LDL-C.9,25 The benefits of therapeutically raising HDL-C levels may not provide CVD risk reduction.26,27 Nevertheless, it has also been shown that an improvement in exercise has been associated with an increase in HDL-C. 25 In unpublished 6-month follow-up data on CHIP participants, the principal investigator of this study (DD) found that after the initial drop, HDL-C increases over time, possibly more slowly responding to the increased exercise of CHIP participants. While it is considered typical for HDL-C to rise with continued exercise, confounding factors like gender and cardiovascular status can impact its rate of change.24,28 Further study is needed to elaborate the proportional impact of diet versus exercise on HDL-C.
Limitations/Further Research Needed
Participants self-selected to enroll in CHIP and in this study. The second data collection occurred after the 11th session, which, depending on the particular class, may have been after as little as 3 weeks of onset of intervention, or as long as 12 weeks. Exercise data on the CHIP survey may have been interpreted differently by different participants since each value could be interpreted as number of days per week of exercise, or by intensity of exercise. However, if the participant was consistent in interpreting the question for both data points, a change in number would likely indicate a change in physical activity. It is unclear how quickly the intervention reaches its maximum impact on biomarkers; the data possibly underrepresenting the full benefit of the program. Factors such as race, socioeconomic status, individual behaviors, and environment were also not accounted for. There was a white female predominance in the population, which has been the case in most CHIP studies.
While this study demonstrated an association between physical activity and BMI, specific data on changes in diet and stress management were not collected making it difficult to attribute results of the program specifically to one component of the intervention. Further studies should include more specific dietary data, and could evaluate gender as well as racial differences. Also, knowing medication status before and after the program would be instructive.
Conclusion
CHIP is effective in producing increased level of physical activity and improvement in multiple biomarkers. The increase in physical activity is correlated with decreased BMI. Since CHIP is delivered as a package, including encouragement of a plant-based diet, and practice of stress management techniques, in addition to physical activity, it is difficult to separate out the specific benefits of physical activity on cardiac risk factors.
Footnotes
Author Note
All communications regarding manuscript and reprint requests should be directed to David Drozek.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.