
Abstract
Keywords
healthcare providers may underestimate their patients’ willingness to pursue lifestyle modification as a method of disease management.
Introduction
The etiology behind the worsening obesity epidemic in the United States is complex. Contributing factors include a progressively more obesogenic environment 1 characterized by poor diet with overall caloric excess, a largely sedentary lifestyle, and inequality in social determinants of health 2 among others. Of these, poor diet has been identified as the country’s leading risk for mortality from chronic diseases and the third leading risk for disability-adjusted life years, a measurement that involves years lived with a disability and years of life lost. 3 In the Unites States, roughly 74% of adults and 40% of children and adolescents are overweight or obese. 4 Excess weight is strongly associated with debilitating chronic conditions like cardiovascular disease, diabetes, and cancer. Obesity and its related chronic health conditions also put a strain on our healthcare system, costing an estimated $400 billion annually. 2 These detrimental health conditions are largely preventable with healthy dietary patterns. A high intake of fruits and vegetables is associated in a dose-response manner with decreased risk of cardiovascular disease, cancer, and all-cause mortality. 5 However, only about 12.2% of adults meet the recommended daily fruit intake and 9.3% meet the recommended vegetable intake. 6 Meanwhile, American adults consume nearly one and a half times the recommended meat and egg intake 7 which has been associated with increased risk of all-cause mortality 8 cardiovascular events, 9 and cancer. 10 Urging a movement away from the standard American diet may, then, be a reasonable focus for healthcare professionals to target the prevention of obesity and related conditions.
Research5,11-21 consistently supports a whole-foods, plant-based (WFPB) diet for both preventing and treating obesity-related chronic diseases. For the purposes of this study, a WFPB diet is synonymous with a vegan diet consisting primarily of fruits, vegetables, legumes, whole unprocessed grains, nuts, seeds, herbs, and spices and that excludes processed, refined, and animal-based foods. 11 It should be noted that in some dietary research studies, a WFPB diet overlaps with other plant-predominant diet variations such as the Mediterranean diet, vegan diet, and vegetarian diet due to the common emphasis on whole, unprocessed plant foods. A WFPB diet has been demonstrated in studies to enhance myocardial blood flow in established coronary artery disease, 12 improve glycemic control in type 2 diabetes,13-15 and decrease known risk factors for cardiometabolic chronic diseases, including body mass index, LDL cholesterol levels, blood glucose, and blood pressure. 16 Those eating vegetarian plant-based diets also have a lower incidence of ischemic heart disease and cancer than non-vegetarians, 17 which have been identified as the top two causes of death in America.3,4 Further, a higher intake of plant-based protein over animal-based protein has been associated with a lower risk of all-cause mortality and cardiovascular disease mortality. 18 The beneficial effects of a WFPB diet have been appreciable in as few as 16 days of implementation. 13 Keeping this in mind, an evidence-based approach to a WFPB diet could be a very important component of the standard of care for preventing and treating obesity-related chronic diseases.
However, there is a limited body of research exploring acceptability of WFPB dietary modification in clinical practice. Our literature review found two studies from Canada and Australia, developed countries with similar western dietary habits as the United States that are high in processed food and animal products,6,19,20,23 that addressed our area of interest. The Canadian pilot study 21 reported that 72% of the providers at a diabetes clinic were aware of the benefits of a WFPB diet to manage and treat type 2 diabetes, yet only 32% recommended this diet to their patients due to low perceived acceptability. In other studies, plant-based diets have been found to have the same or improved acceptability than a conventional diabetes diet while improving HbA1c, lipid levels, BMI, and glycemic control in patients with diabetes.15,22 The Canadian pilot study 21 also reported that of their 91% of patients who currently did not follow a WFPB diet or variation, about 65% were willing to try a WFPB diet for a short period of time if given appropriate information and education. The Australian study 23 that examined consumers’ perceptions of plant-based diets found that most respondents, 88.3% of which were not vegetarian or semi-vegetarian, perceived health benefits like lower saturated fat intake, increased fiber intake, and disease prevention while citing relatively fewer barriers. These findings suggest that healthcare providers may underestimate their patients’ willingness to pursue lifestyle modification as a method of disease management. However, the limited body of evidence in this area necessitates further research.
This cross-sectional study is the second installment of our two-part study that sought to evaluate WFPB diet perceptions in medical trainees and patients. Our first manuscript 24 evaluated medical trainees’ satisfaction with their current degree of nutrition training in medical school. It also examined medical trainees’ familiarity with a WFPB diet and likelihood to recommend it to patients. Due to the complex nature of the survey questions and the many variables we sought to examine, the remainder of the investigation was carved out for a separate analysis and conclusion. With this second part of our survey-based study, we aim to answer the following questions: Are patients at a primary care clinic willing to implement a WFPB diet for the short-term? How likely are medical students and family medicine residents to recommend a WFPB diet to their patients for the short-term? Lastly, which barriers do patients perceive to adopting a WFPB diet, and which barriers do trainees perceive to recommending a WFPB diet? We hypothesized that a discrepancy would exist between willingness of patients to try a WFPB diet and likelihood that medical trainees would prescribe this diet to their patients. We also hypothesized that a discrepancy would exist between perceived barriers by patients and medical trainees.
Materials and Methods
Instruments
We created two original survey instruments modeled after the instruments used by Lee et al. 21 and Lea et al. 23 Our first survey instrument was used to collect data from patients on healthy diet perceptions, awareness of a WFPB diet, willingness to adopt a WFPB diet short-term, and perceived barriers to the adoption of a WFPB diet short-term. The second survey instrument with largely identical content and format was administered to medical students and family medicine residents for comparison. Both survey instruments can be found in the Supplemental Materials section. Differences between each survey instrument are noted subsequently.
The first section of both surveys was entitled “Demographics/Health Information.” This section in the patient survey included questions about age, biological sex, ethnicity, highest level of education, health insurance, height and weight (used to compute BMI), current health conditions and prescription medications, and a general Likert-scale rating of overall health. The “Demographics/Health Information” section of the student/resident survey included questions about biological sex, level of training, clinical interests, and a general Likert-scale rating of overall health.
The second section entitled “Diet” was identical between the survey instruments. This section consisted of a detailed description of a whole-foods, plant-based (WFPB) diet followed by questions regarding familiarity with a WFPB diet and its health benefits, current or past experiences with a WFPB diet, attempts to follow a healthy diet, advice from healthcare providers about healthy diets, and effects a healthier diet might have on overall health. The response options for these items were Yes/No. An optional free-text box was included for respondents’ opinions about a WFPB diet.
The third section was entitled “Motivation” in the patient survey and “Recommendation in the student/resident survey. This section asked patients whether they would try a WFPB diet for 3 weeks for 9 specific reasons: to lose weight, to lower blood pressure to normal levels, to manage or cure diabetes, to manage or cure heart disease, to slow down or prevent cancer, to lower cholesterol to normal levels, to lower saturated fat intake, to stop taking prescription medications, and to prevent chronic diseases. Answer choices were given in a Likert-style response format designed after the stages of change model,
26
a theoretical framework frequently used in the clinical setting to guide behavior change and lifestyle modification. The answer choices with the corresponding stage of change were as follows: Definitely will NOT try for this reason: Precontemplation. Will think about trying for this reason: Contemplation. Will probably try for this reason: Preparation. Definitely will try for this reason: Action. I have tried or am already trying for this reason: Maintenance.
The student/resident version asked how likely the respondent would be to recommend a WFPB diet for 3 weeks for the same 9 specific reasons. Both surveys included a question about general willingness to try or recommend a WFPB diet with 5-point Likert-style response choices ranging from definitely to definitely not. An optional free-text box was provided for other factors that might motivate respondents to either try a WFPB diet or recommend a WFPB diet.
The fourth section was entitled “Barriers” and provided 19 potential barriers to adopting a WFPB diet. Patients were given 5-point Likert-style response choice items to indicate the extent to which they agreed with each barrier to trying a WFPB diet for 3 weeks. Students and residents were given the same Likert-style response choices to describe the extent to which they believed each barrier would get in patients’ way of trying a WFPB diet for 3 weeks. Another optional text box was provided for additional barriers not listed.
The final section in the patient survey was entitled “Additional Information.” This section asked patients about 8 specific factors that would provide additional help for trying a WFPB diet for 3 weeks. These items were also anchored with strongly disagree to strongly agree. Two additional free-text boxes were provided for patients to request sources of additional evidence and identify sources of trustworthy evidence.
The final section of the student/resident survey was entitled “curriculum” and included questions about nutrition in medical school curriculum. The findings of this portion of the student/resident survey were discussed in detail in our first manuscript 24 and will not be covered here.
Procedures
Our study took place at the University of Louisville School of Medicine and affiliated entities in Louisville, Kentucky, a southern state whose estimated vegetarian or vegetarian-variation following is roughly 6%. 25 The affiliated entities included the University of Louisville Family Medicine residency program and the Cardinal Station Medical Center, a primary care clinic in Louisville, Kentucky that provides care to members of the community and students of the University. After being granted exemption by the University of Louisville Institutional Review Board, an online version of the original student survey was emailed to first through fourth year medical students via a URL link with 3 email reminders every two weeks throughout the data collection period. An informed consent letter was included as an attachment to each email which described our research project and stated that by completing the online survey, participants were providing consent to take part in our study. Qualtrics, an electronic survey tool, was utilized in order to protect the security and anonymity of individual students’ responses. An identical survey was given as a hard paper copy to residents in the University of Louisville Department of Family Medicine during a weekly meeting and collected by a member of the research team using an unlabeled envelope.
A mirrored survey tool with appropriate changes to reflect the patient perspective was offered as a hard paper copy to patients in the waiting room of the Cardinal Station Medical Center primary care clinic. An informed consent document, which described our research project, was stapled to the front of the survey packet. This informed consent document stated that by completing the survey, each patient was granting their informed consent to participate in our study. Patients were offered the survey while they waited for their appointments. Patients were also offered a choice of fresh fruit or granola bar for completing the survey. The completed survey packets were collected in a secure, unlabeled envelope by a member of the research team stationed in the waiting room. The hard paper copies were then securely stored in a locked cabinet for the duration of the data collection period. Responses from the paper copies were tabulated at the end of the data collection period using Microsoft Excel. The patient survey packets did not contain any identifiable traits and were handled in a manner that preserved respondent anonymity. It should be noted that these data were collected in the fall of 2019, prior to the coronavirus pandemic.
Inclusion criteria for the student/resident participants were first through fourth year medical students at the University of Louisville School of Medicine and first through third year family medicine residents at the University of Louisville School of Medicine. Other parties at the University of Louisville School of Medicine, such as staff, faculty, and physicians were excluded from the study. Inclusion criteria for the patient participants were adult patients at the University of Louisville-affiliated Cardinal Station Medical Center primary care clinic. Exclusion criteria were children under the age of 18, adult patients with developmental, intellectual, or physical disabilities that hindered the subject’s ability to read or understand the survey tool, patients unable to read or understand English, and other such conditions that interfered with thorough understanding of the survey tool.
Data Analysis
Quantitative data from the patient, student, and resident surveys were analyzed using SPSS version 27.0. For the patient surveys, the patients’ demographic information was summarized with frequency and percentages. For items with Likert-scaled format responses frequencies, percentages, means and standard deviations are presented. A comparison of reasons patients might try a WFPB diet by 1) a dichotomized Likert scale format response item that assessed overall health as self-described healthy or unhealthy, 2) presence or absence of chronic health conditions, and 3) patients’ body mass index (BMI) dichotomized as normal or overweight/obese was assessed using the Mann-Whitney U exact statistic. Analogously, comparisons between medical trainees and patients on various Likert type items were also assessed using the Mann-Whitney U statistic. All P-values were 2-tailed and significance was set at convention at P<.05.
Qualitative data from the patient survey were analyzed using Dedoose. Free-text responses were coded as positive, negative, neutral, or not understandable. The responses within the positive and negative categories were then subdivided further. The responses from the final free-text box in the Additional Information section were tabulated exactly as written. Frequency of responses within each code, co-occurrences of codes, and individual quotes were used to supplement quantitative data. Codes were not mutually exclusive as multiple codes could be used to describe one response.
Qualitative data from the student/resident survey were also analyzed using Dedoose. All free-text responses in the Diet, Recommendations, and Barriers sections were coded as positive, negative, or neutral. Both positive and negative categories were then sub-coded into 8 groups with further subcategorization as warranted. Results of this analysis were used to compare to qualitative responses from the patient surveys. Free-text responses in the Curriculum and Additional Information/General Comments are not pertinent to the purposes of this article and have been omitted from discussion. 24
Results
Quantitative Data
Patient Demographic Information.
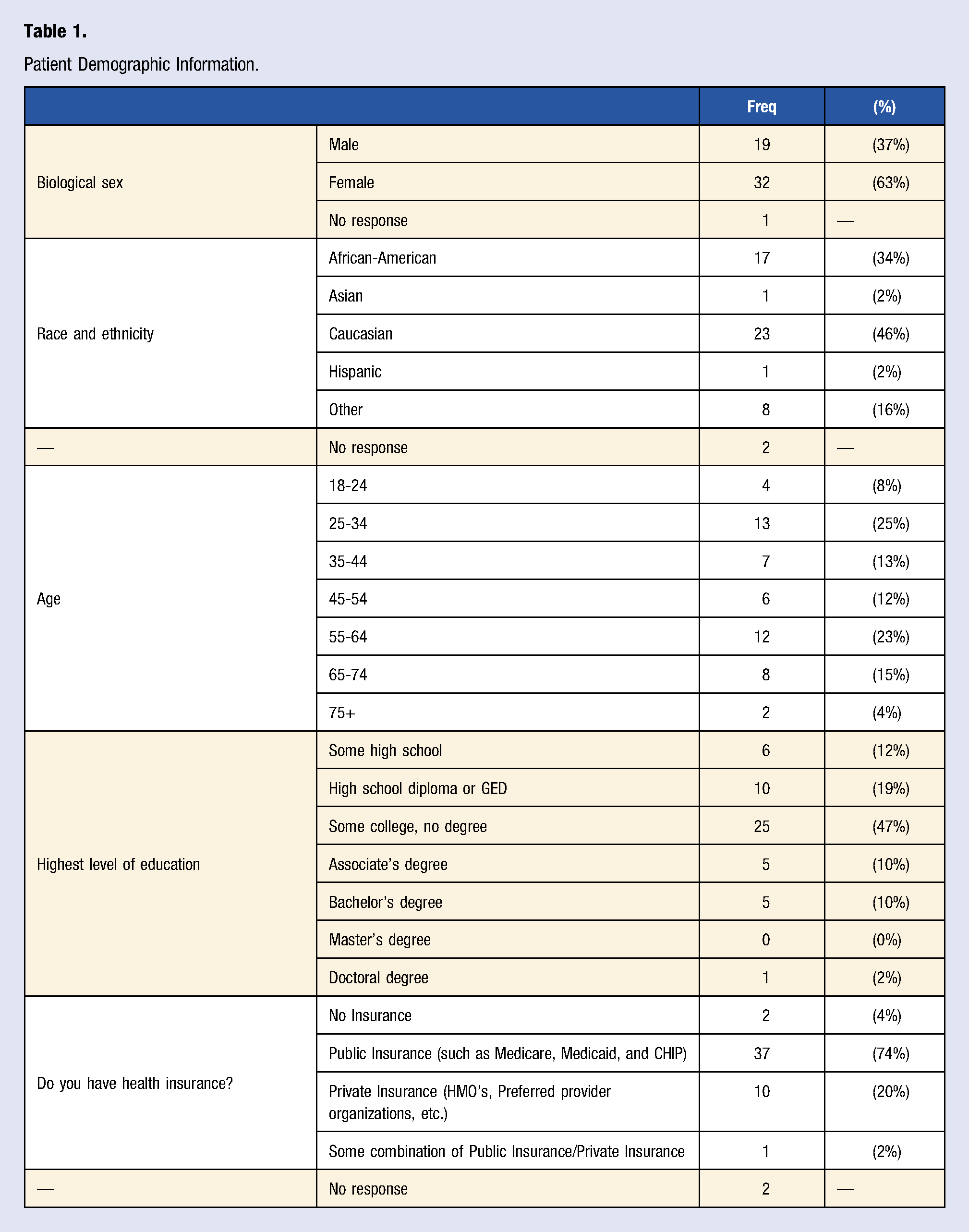
Of the 52 patient respondents, 44 (85%) reported that they had heard of a WFPB diet, 38 (73%) reported familiarity with the health benefits of a WFPB diet, 6 (12%) reported currently following a WFPB diet or variation, and 9 (17%) reported following a WFPB diet or variation in the past, similar to the frequencies of plant-based variation followers in the Canadian 21 and Australian 23 studies. Of the students and residents who responded to the survey, 93% had heard of a WFPB diet, 83% were familiar with the health benefits of a WFPB diet, 26% were currently following a WFPB diet or variation, and 14% had followed a WFPB diet or variation in the past. 23
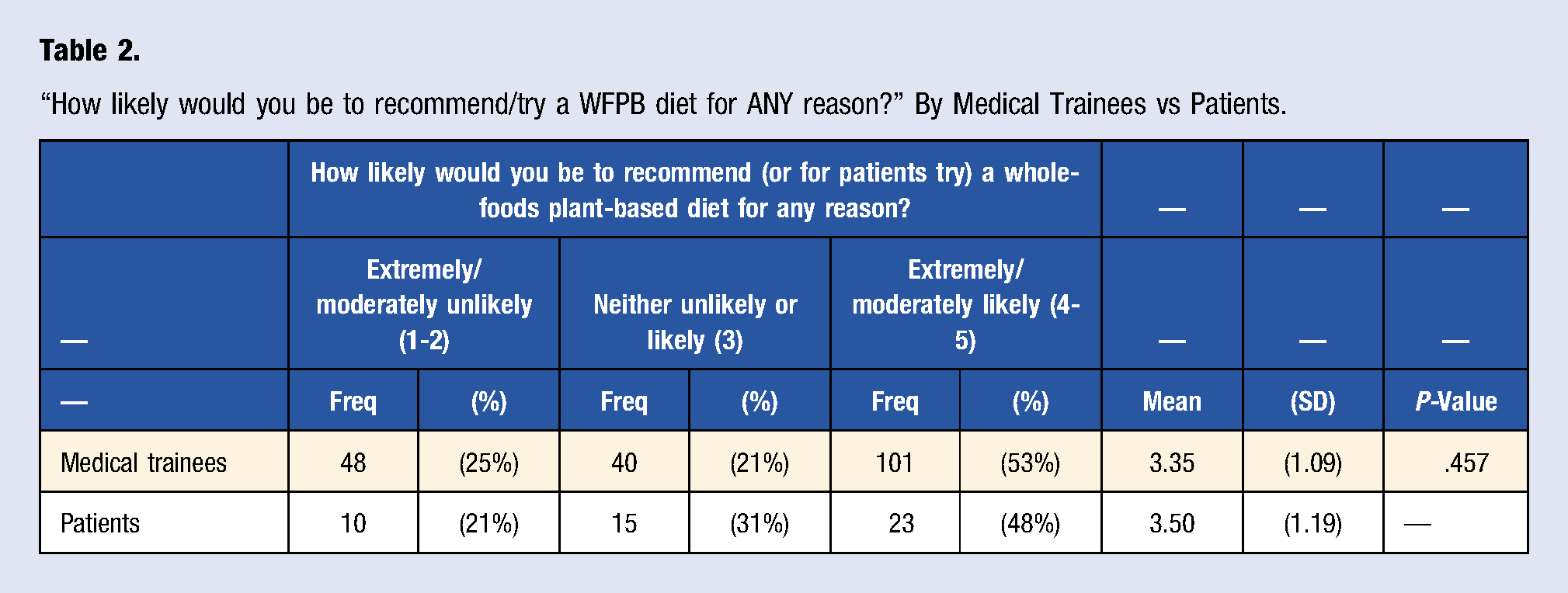
“How likely would you be to recommend/try a WFPB diet for ANY reason?” By Medical Trainees vs Patients.
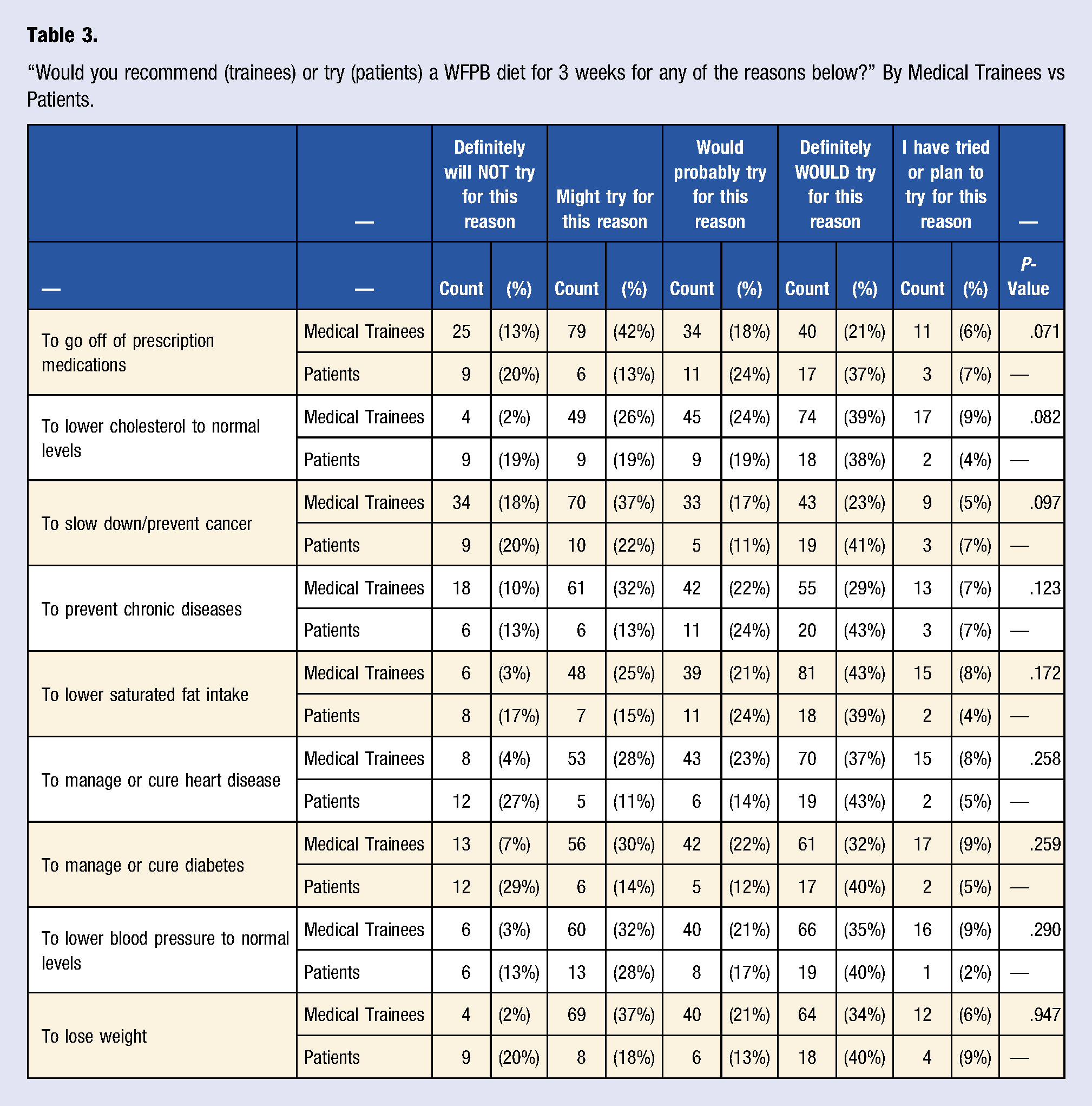
“Would you recommend (trainees) or try (patients) a WFPB diet for 3 weeks for any of the reasons below?” By Medical Trainees vs Patients.
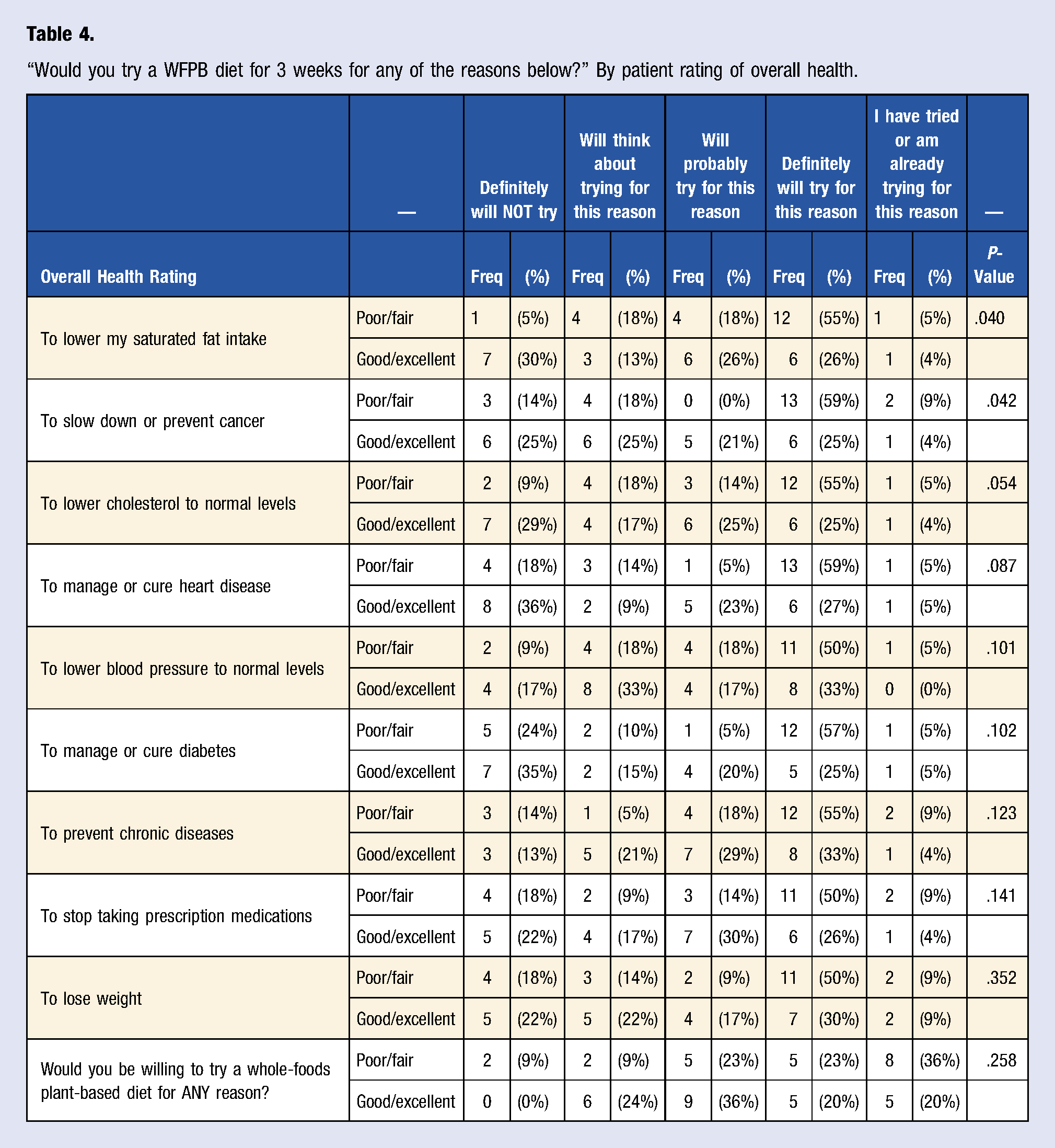
“Would you try a WFPB diet for 3 weeks for any of the reasons below?” By patient rating of overall health.
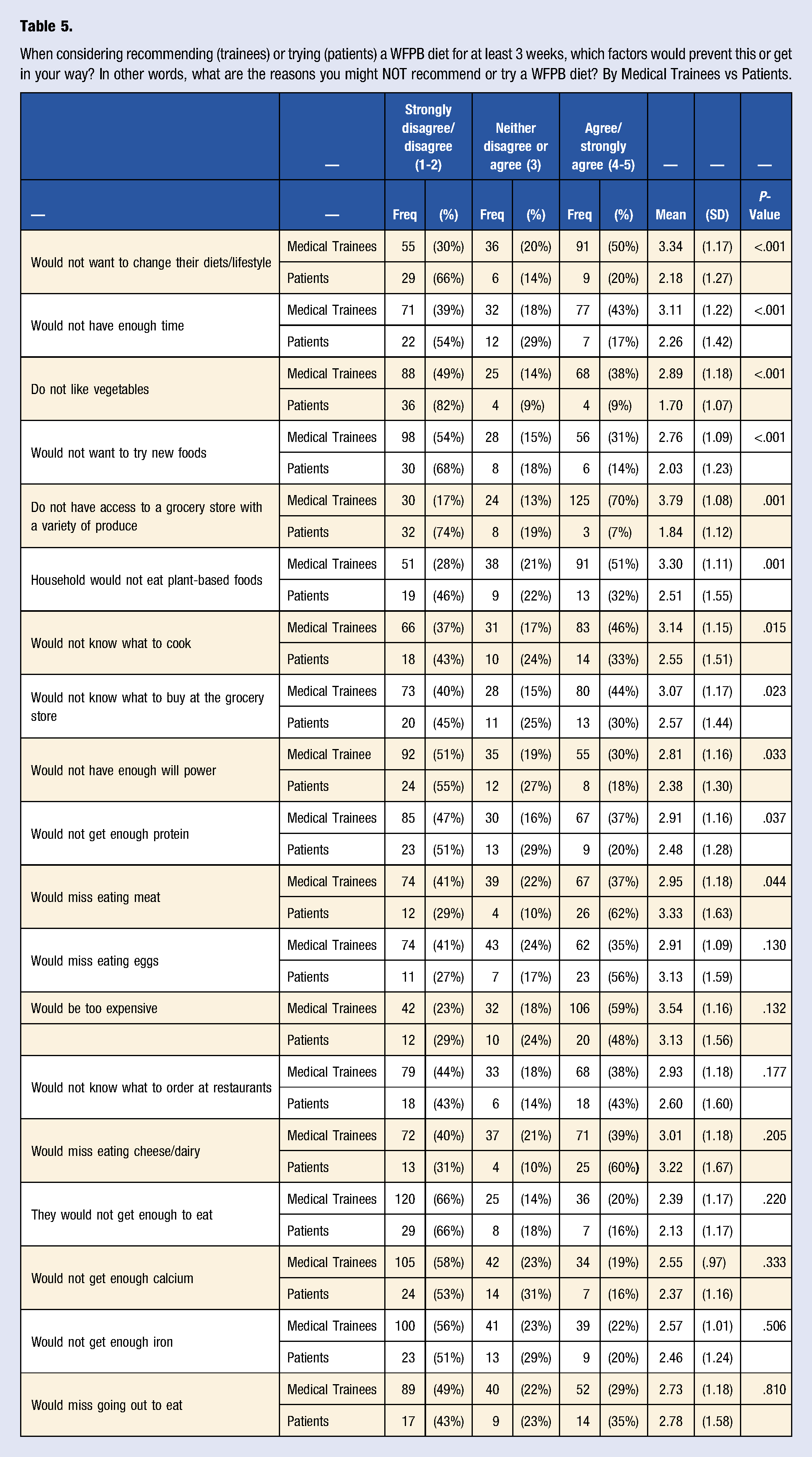
When considering recommending (trainees) or trying (patients) a WFPB diet for at least 3 weeks, which factors would prevent this or get in your way? In other words, what are the reasons you might NOT recommend or try a WFPB diet? By Medical Trainees vs Patients.
We also examined responses from patients with and without the following specific chronic conditions: diabetes, high blood pressure, high cholesterol, and general heart disease (including heart failure, cardiovascular disease, and heart attack) with respect to trying a WFPB diet for the purpose of improving each of the four conditions. No significant differences were found between patients for these 4 conditions (data not shown).
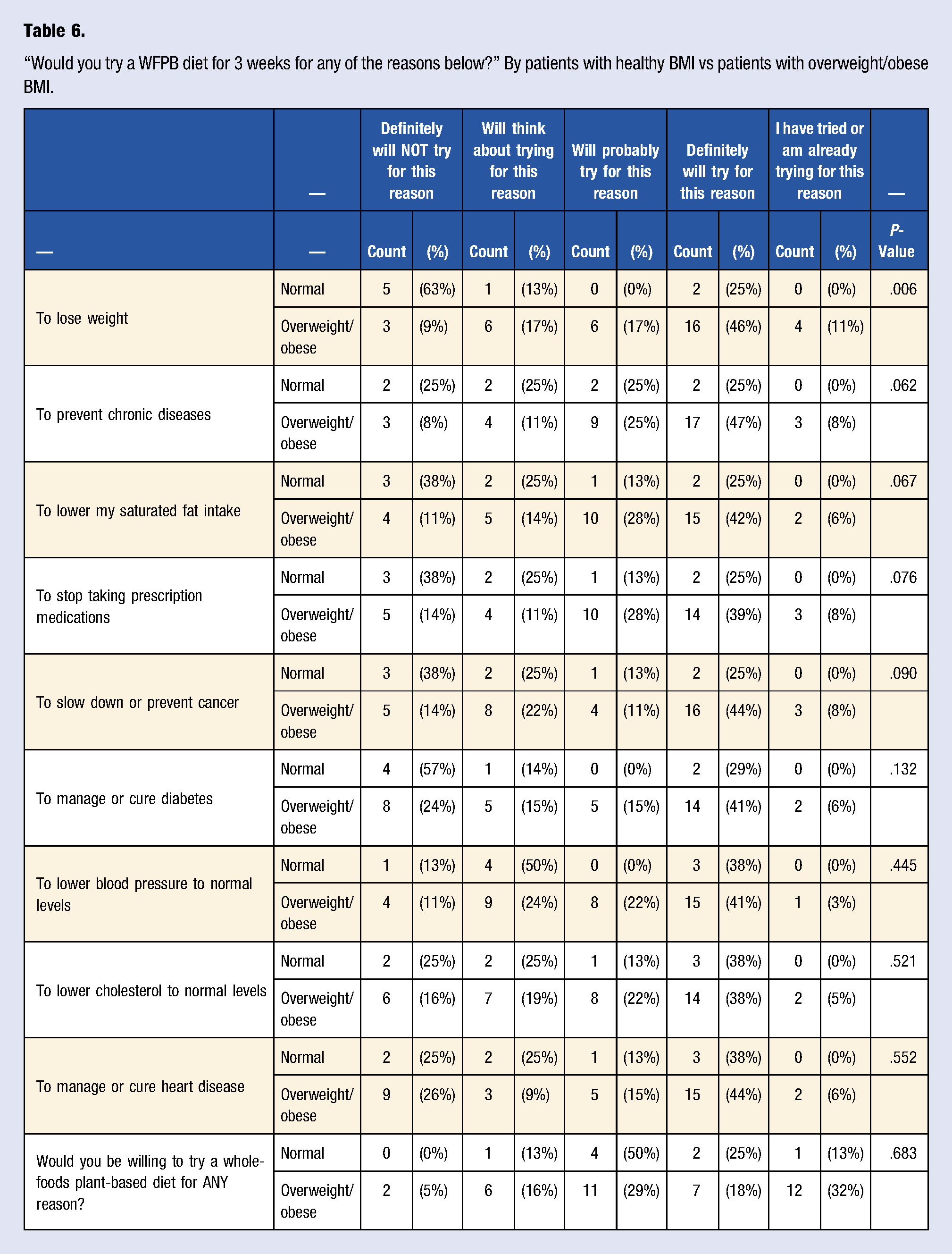
“Would you try a WFPB diet for 3 weeks for any of the reasons below?” By patients with healthy BMI vs patients with overweight/obese BMI.
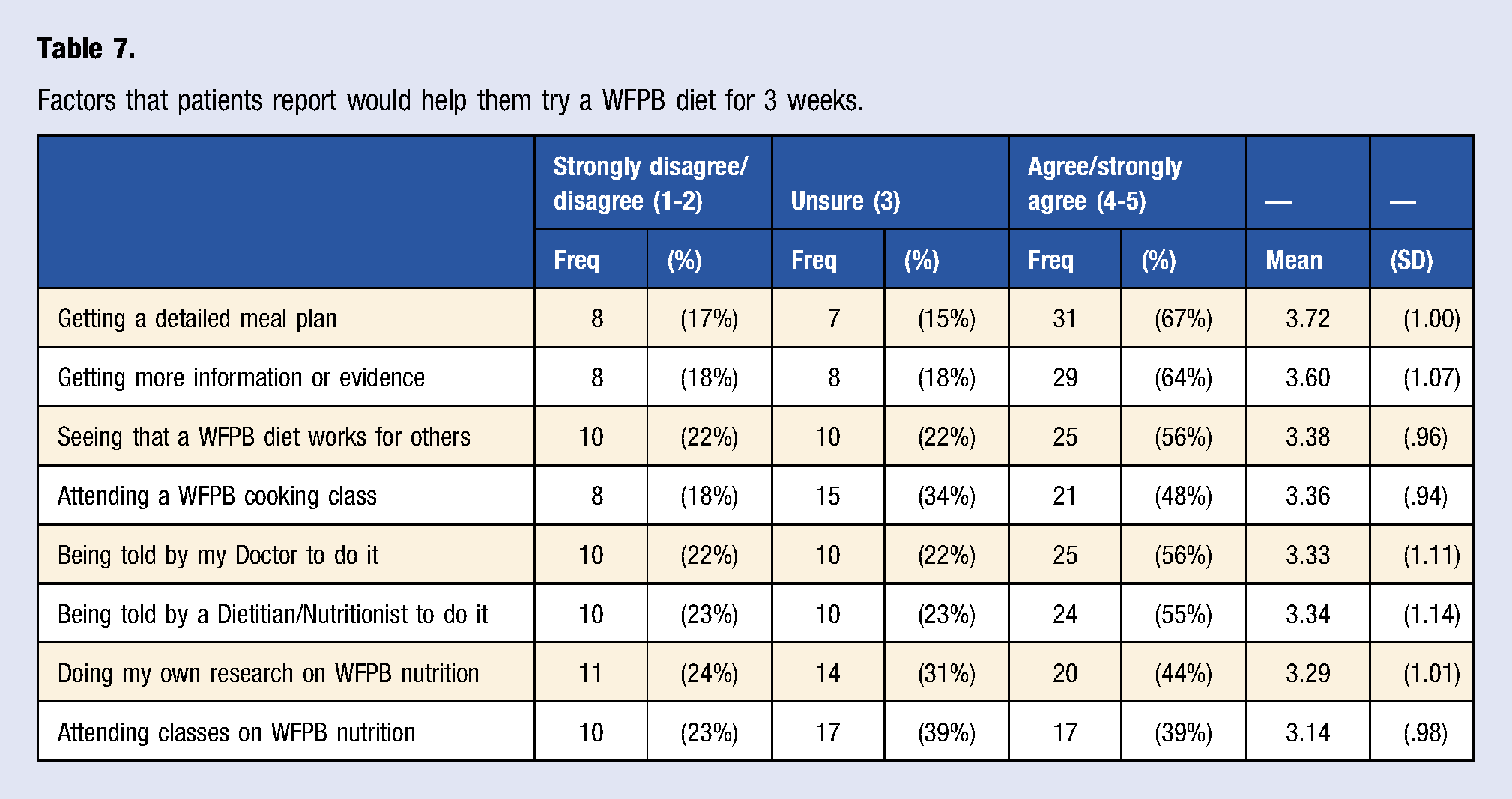
Factors that patients report would help them try a WFPB diet for 3 weeks.
Qualitative Data
The optional free-text question in the Diet section of the patient survey read, “If you have heard of a WFPB diet, what is your opinion of it?” Responses from this question were coded as 8 negatives, 17 positives, and 3 neutral. Of the negative responses, the most common was Personal Preference (8 responses) and other responses included Feasibility (2 responses), Financial (1 response), and Personal Experience (1 response). Of the Positive responses, the most common were Health (9 responses) and General Positive (9 responses). Other Positive responses included Environment (1 response) and Personal Experience (1 response). One response to this question was coded as Not Understandable.
The free-text question in the Motivation section of the patient survey asked, “What other things would help motivate you to try a WFPB diet for 3 weeks?” The most common code was Health (7 responses) which was subdivided further into General Health (4 responses), Health Benefits (2 responses), and To Avoid Health Consequences (1 response). The remaining responses in order of descending frequency were Education (5 responses), Financial (4 responses), Feasibility (3 responses), None (3 responses), Family (2 responses), Personal Experience (2 responses), Time to Think (2 responses), and Aesthetic (1 response).
The free-text question in the Barriers section of the patient survey asked, “Do you have other reasons for not wanting to try a WFPB diet for 3 weeks?” The most common code was None (11 responses). The next most common theme of responses was Personal Preference (3 responses) comprised of statements reflecting enjoyment of meat and animal products. The themes Education, Financial, and Time each garnered 1 response.
When asked about what kind of additional information or evidence respondents desired to help them try a WFPB diet for 3 weeks, the most common theme was information regarding Practical Application (9 responses), including how to choose the right foods and how to prepare WFPB-friendly meals. Respondents also desired Evidence-Based Information (4 responses), Specific Food Ideas (4 responses), and General Information (4 responses). Other themes included Anecdotes (2 responses), such as results from other patients, and None (2 responses). Two responses were coded as Not Understandable.
The final free-text question asked, “What source of Nutrition Information do you think is most trustworthy?” followed by a list of examples including websites, doctors, dietitians, nutritionists, trainers, magazines, and the news. The most common response to this question was Nutritionists (17) followed by Doctors (15) and Dietitians (13). The Media tallied 7 responses which were sub-coded as websites (4) books (1), magazines (1) and the news (1). The remaining responses fell into the categories of Research Articles (4), Trainers (3), and None (1).
The qualitative results from the student/resident survey are reported in greater detail in our first manuscript 24 and will be briefly discussed below.
Discussion and Conclusions
Discussion of Findings
Overall, the majority of our patient population (48%) demonstrated a positive interest in trying a WFPB diet for the short term. Most respondents were familiar with a WFPB diet and reportedly aware of its general health benefits, citing reasons such as “good diet to lose weight,” “seems very healthy,” and “it has a lot of health and environmental benefits...” Very few patients, however, reported trying to implement a WFPB diet or similar variation currently or in the past. These findings are consistent with the limited existing literature examining perceptions and acceptability of WFPB diets of patients and consumers.21,23 When examining more specific reasons for motivation, there were very few significant differences between patient groups with respect to Stage of Change. The few differences identified may not be strong enough to draw noteworthy conclusions. For example, patients with an overweight/obese BMI were more likely to want to try a WFPB diet to lose weight than patients with a healthy BMI, but this may be attributable to the fact that patients with a high BMI are interested in losing weight in general while patients with a healthy BMI are not. An association between a desire to lose weight and the use of a WFPB diet as a means of weight loss cannot be determined in this case. These findings suggest that patients’ willingness to pursue WFPB dietary modification should not be assumed based on overall health status, BMI, current medical conditions, or lack thereof. Rather, the importance of exploring each individual patient’s motivation to try a WFPB dietary pattern should be stressed. One potential approach might be a motivational interviewing technique using the stages of change model. 26 The individualized motivational interviewing method is strongly supported by current research and already used by registered dietitians, doctors, and other healthcare providers as a means of behavioral counseling26,28,29 and could be used as an effective method for helping patients gradually transition to a WFPB diet.
Determining a patient’s behavioral stage of change in the clinical setting must begin with the presentation of a behavioral end goal. This component of the clinical interview is often the duty of the provider, especially when there is a gap in knowledge or experience in the patient. However, previous literature has shown that many providers do not offer a WFPB diet as an option to their patients despite being aware of the associated health benefits due to an assumption of low acceptability. 21 The results of our pilot study contradict this assumption. After being presented with a WFPB diet as a viable option for achieving health goals, patients expressed a desire to obtain more information and to learn more about the practicality of implementing it, consistent with previous studies.21,23 In fact, 56% of patient respondents agreed that being told by their doctor to try a WFPB diet would help them implement it for 3 weeks and 55% of patients agreed that being told by a dietitian or nutritionist would help them implement a WFPB diet for 3 weeks. Our results suggest that it is possible that more patients may take tangible steps toward a WFPB diet with guidance from their healthcare provider if healthcare providers presented a WFPB diet to their patients as an option in the first place.
We found that more than half of our medical trainee population reported a positive likelihood of recommending a WFPB diet to their current and future patients, compared to 32% of providers surveyed in the Canadian pilot study 21 previously discussed. Trainees’ free-text responses most often cited positive health benefits, acceptability, and environmental impacts associated with a WFPB diet. 24 Contrary to our proposed hypothesis, the surveyed patients and medical trainees appear to be similarly likely to try a WFPB diet for 3 weeks or recommend a WFPB diet for 3 weeks, respectively. Phase one of our study demonstrated that despite their willingness to recommend a WFPB diet to their patients, our medical trainee respondents are largely dissatisfied with the degree of nutrition training they had received in medical school and thus lacked confidence in their ability to counsel patients on nutrition in general. 24 The health benefits and chronic disease risk reduction associated with a WFPB diet5,8-18 are inconsequential if physicians are unable to effectively counsel their patients on nutrition. If physicians are to provide their patients with detailed meal plans, more information, and more evidence in support of a WFPB diet, the physicians themselves must become more familiar with this type of dietary pattern. 27 One possible solution is a greater focus on nutrition in medical training, specifically plant-based or plant-predominant nutrition, for chronic disease prevention 24 in order for rising physicians to feel confident in their role as the nutrition experts their patients perceive them to be.30,31
The most striking differences between our patient and medical trainee respondents were the perceived barriers to the implementation of a WFPB diet by patients for 3 weeks, which supported our hypothesis. Patients more commonly reported barriers associated with their personal preferences, most commonly involving the enjoyment of meat and other animal products. One respondent stated, “I think that it would be great. Personally, I have a lack of motivation to exclude meat and animal products from my diet,” while another stated “[g]reat idea but I need viable meat substitutes.” Medical trainees, on the other hand, were more concerned about barriers related to social determinants of health, such as food insecurity and finances: “Patients that live in known food deserts do not have easy access to plant-based foods or grocery stores. If I know that in advance, then I may bring up improving diet, but I would not necessarily recommend a plant-based diet if I know it's not a realistic option” was one of three similar comments. Over half of trainees and 48% of patient respondents agreed that a WFPB diet would be too expensive, despite existing evidence that meat, poultry, and fish tend to have the highest cost per unit weight than legumes, grains, vegetables, and fruits. 32 Keeping these discrepancies in mind, it is vital that providers recognize their own biases and assumptions regarding patients’ willingness to pursue behavior change. A provider’s assumption that a WFPB diet is “too extreme” and “very difficult to implement” might keep him or her from supporting a patient who is actually motivated to try a WFPB diet to improve their health. Ultimately, an emphasis on individualized goal-setting, exploration of barriers unique to each patient, and the provision of appropriate resources should be prioritized to support patients interested in pursuing a WFPB diet. Such individualized health-coaching has been shown to be an effective means of behavior modification and could be a useful tool in this setting. 33
Healthcare providers must, then, familiarize themselves with the characteristics, health benefits, and methods of practical application of a WFPB diet in order to best counsel their patients using an individualized approach. Our patient respondents were interested in learning more about WFPB diets and trusted their doctors for nutrition information. They also trusted frequently unreliable and unverifiable sources of nutrition information like websites, magazines, and the news. As perceived nutrition experts,30,31 doctors are in a position to strongly influence the dietary lifestyle their patients choose to pursue. These doctors, however, are no more familiar with a WFPB diet than the general public 27 and report being uncomfortable with nutrition counseling in general.30-42 Educational materials for physicians and physicians-in-training that focus on a WFPB diet alongside other evidence-based dietary patterns 24 could be developed to address these gaps in knowledge. Improved nutrition education for our country’s incoming physicians could then equip them with the tools necessary to provide their patients with reliable and practical nutritional counseling for chronic disease prevention and management.
Limitations
Our pilot study was limited by the small sample size of both the patient group (n = 52) and the student/resident group (n = 300, 30% response rate). The exclusion of non-English-speaking patients could have also overlooked a subgroup with distinct cultural dietary practices, perceived motivations, and perceived barriers that could have affected our findings. Additionally, our sample size was drawn from a single institution and a single affiliated primary care clinic. Due to the small sample sizes and limited scope of inclusion, our results are difficult to extrapolate to a larger and more diverse population of patients and medical trainees in the United States or abroad.
Another limitation of our study is that the surveys were presented as optional to each of the target populations. Therefore, patients with stronger opinions regarding nutrition were more likely to complete it. Likewise, the medical students and residents with stronger opinions may have been more likely to complete the survey. Additionally, the hypothetical nature of our survey questions makes our results less reliable as no true behavioral patterns among respondents were examined. The presence of reporting bias among patient, student, and resident respondents is another potential limiting factor.
It is important to note that the focus of our study creates a bias in favor of a WFPB diet. 24 The aim of our study was to explore perceptions regarding a WFPB diet specifically among patients and medical trainees. For this reason, similar healthy dietary patterns such as the Mediterranean diet, vegetarian diet, and vegan diet were excluded from our survey. This may have conveyed to our study participants that a WFPB diet is superior to other similar healthy dietary patterns, which could have skewed our results. It cannot be concluded from our study that a WFPB diet is superior to similar plant-predominant dietary patterns. Further study is needed to compare the perceptions of patients to the perceptions of medical trainees regarding other healthy dietary patterns such as the Mediterranean diet, vegetarian diet, and vegan diet.
Conclusions
This survey-based pilot study is the second installment of our two-part study that sought to evaluate WFPB diet perceptions in medical trainees and patients. This phase of our study aimed to evaluate the perceptions of patients and physicians-in-training regarding the implementation of a WFPB dietary pattern for the management of chronic diseases along with the barriers to the implementation of a WFPB dietary pattern. Despite our low sample size, our results demonstrated reasonable patient interest in trying a WFPB diet for a variety of motivational factors. We also found that despite personal preferences, patients tended to be interested in learning more about how to incorporate a WFPB diet into their lives. Although few significant differences were found between medical trainees and patients regarding likelihood of recommending or trying a WFPB diet, respectively, significant differences were noted in perceived barriers. A WFPB diet may, then, be a reasonable goal for many patients who wish to pursue healthy dietary modification. Further research with a larger, more diverse sample size may be helpful in determining areas of focus regarding patient motivations and barriers. Further study could also be directed at revealing additional areas of motivation and barriers that our survey tools did not address.
A whole-foods, plant-based (WFPB) diet consisting primarily of fruits, vegetables, legumes, and whole grains has been shown to be a palatable 15 and effective intervention for the management of the country’s most common chronic conditions.5,11-18,22 However, it is a method of lifestyle modification that healthcare providers are largely unfamiliar with. 27 Meanwhile, those doctors and dietitians who are familiar with a WFPB diet for chronic disease management are still hesitant to recommend it to their patients due to a lack of perceived acceptability, 21 despite a positive interest demonstrated by patients in our study and others.21,23 Patients’ actual acceptability of WFPB dietary modification for general chronic disease management has not been directly compared to their providers’ perceptions prior to our study. The findings of our pilot study have begun to shed light on the discrepancy between patients’ actual views of behavior modification with a WFPB diet and healthcare providers’ perception of the views held by their patients. Our research is the first to directly compare WFPB diet perceptions between patients and doctors-in-training; therefore, further study is warranted. The findings of this study and future research could then be used to develop pertinent education materials focused on WFPB nutrition for patients, medical trainees, and practicing healthcare providers, serving as an important step toward reducing the burden of obesity-related diseases in our country.
Supplemental Material
sj-pdf-1-ajl-10.1177_15598276211041551 – Supplemental Material for Whole-Foods, Plant-Based Diet Perceptions of Medical Trainees Compared to Their Patients: A Cross-Sectional Pilot Study
Supplemental Material, sj-pdf-1-ajl-10.1177_15598276211041551 for Whole-Foods, Plant-Based Diet Perceptions of Medical Trainees Compared to Their Patients: A Cross-Sectional Pilot Study by Kara F. Morton, Diana C. Pantalos, Craig Ziegler and Pradip D. Patel in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors would like to thank Eli Pendleton, MD for his assistance with resident and patient data collection, and Susan Sawning, MSSW and Emily Noonan, PhD for guidance in the qualitative analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.