
Abstract
“The LMA was shown to be a feasible tool for the implementation of lifestyle medicine in a family medicine ambulatory clinic.”
Introduction
Lifestyle medicine is a patient-centered health care approach that incorporates personal behaviors and evidence-based medicine to both prevent and treat chronic disease. The official lifestyle medicine definition from the American College of Lifestyle Medicine consists of 6 pillars: whole-food plant-based nutrition, physical activity, stress management, avoidance of risky substances, restorative sleep, and social connection. 1 Each of these pillars assesses different areas of wellness in a person’s life, with each contributing to the prevention of both chronic mental and physical illnesses. It has been shown that up to 80% of chronic diseases are preventable through adherence to healthy lifestyle habits. 2 With chronic diseases representing an overwhelming amount of morbidity and mortality in the United States, 2 lifestyle medicine serves to prevent the burden of chronic illness on both the individual and society as a whole.
While the idea of lifestyle medicine is not new, literature investigating its benefits has grown substantially in recent years. One study specifically looking at the prevalence of diabetes as it relates to animal product consumption found that those without animal consumption had the lowest prevalence of diabetes and a statistically significant reduction of diabetes development by 49% when adjusted for confounding factors. 3 Furthermore, a meta-analysis conducted on meat consumption showed each daily serving of meat to be associated with an increase in diabetes risk by 51%. 4 Lifestyle interventions such as smoking cessation, physical activity, and a whole-food plant-based diet have also been shown to decrease the risk of CVD development, 5 with exercise specifically linked to decreased mortality in at-risk patients.6–8 In regard to the sleep and stress management pillars, a lack of sleep and inadequate stress management techniques are linked to affective disorders such as anxiety and depression.9,10 Additionally, depression has been identified as an independent risk factor for CVD and vice versa, 11 with both potentially resulting from the accumulation of stress on the body. 12 These findings highlight the interrelated nature of lifestyle behaviors, chronic physical illness, and chronic mental illness.
With the surmounting evidence demonstrating the health benefits of lifestyle medicine, many professional associations have begun incorporating the tool into their recommendations. Lifestyle modification is often the first treatment modality for chronic disease. The American Medical Association issued a preventative medicine policy in 2010 encouraging physicians to apply competencies of lifestyle medicine into their practice. Despite this, there are many barriers to implementing lifestyle medicine counseling into practice. Many physicians report a lack of confidence and education in lifestyle medicine counseling. 13 In addition to this, a lack of time and perceived difficulty in changing patient behavior were reported as barriers among an overwhelming majority of family medicine physician respondents. 14 This perceived difficulty in changing patient behavior may be due, in part, to the fact that adherence to lifestyle medicine in the general population is currently very low. According to a cross-sectional analysis, less than 50% of the United States population meets the minimum physical activity goal of 150 minutes per week and only 0.52% eat a whole-food plant-based diet. 15
These deterrents could be responsible for the lack of prescribing lifestyle medicine in standard appointments. One study showed that obese patients were only advised to lose weight 36% of the time during regular appointments. 16 Another study demonstrated that only 28% of patients who smoked were offered smoking cessation assistance in the last year. 17 Despite the profound benefits of lifestyle medicine, these findings show that its execution in standard practice has been lacking, with a remedy to perceived barriers yet to be solved. With all the above factors involved, the medical community currently seems to be unprepared for the establishment of lifestyle medicine in daily clinical practice. 18 The need for physicians to develop new strategies to enhance their lifestyle medicine counseling and develop confidence in its implementation is paramount.
Given the immense burden of chronic disease, coupled with the low general adherence to lifestyle medicine and lack of application in clinic appointments, new tools to assist physicians to implement lifestyle medicine regularly are urgently needed. In this study, we investigated a proposed mechanism for the incorporation of lifestyle medicine into a standard family medicine practice using the American Academy of Family Physicians (AAFP) Lifestyle Medicine Assessment (LMA) tool. The aims of this study were 2-fold. Our first aim investigated the feasibility of administering the assessment tool and counseling with patients, keeping in mind time constraints for providers. The second aim analyzed if the incorporation of the LMA into a patient appointment improved one’s motivation to change lifestyle behaviors, perception of lifestyle behaviors on well-being, and overall satisfaction with the visit. We hypothesized that within the LMA group, there would be higher levels of motivation to change behaviors and perception of behavior change on well-being after the encounter as compared to before the encounter, whereas these changes would not be seen within the control group. Also, we hypothesized that the LMA group would show increased satisfaction with the visit compared to the control group. With these aims, we hope to address the perceived barriers of prescribing lifestyle medicine within an outpatient clinic and investigate the efficacy of this tool for promoting lifestyle changes.
Methods
Patients were surveyed at Wright State Physicians Family Medicine Health Center in Dayton, Ohio. This facility is a large family medicine clinic with up to 18 family medicine providers. The following protocols were conducted by medical students familiar with lifestyle medicine principles and trained in motivational interviewing skills.
Aim #1: Feasibility of LMA Tool Implementation
In this phase, patients represent a convenience sample, as they were selected based on who was in the clinic at the time of recruitment. Patients were first given the AAFP LMA tool to fill out independently while waiting for the provider. During the visit, their assessment answers were transposed into an Excel sheet that tallied their results from each category and created a diagram showing their progress in each category (Figure 1). Depicts an example of the LMA tool personalized diagram that is created after one takes the LMA. The diagram contains five sectors for the five components: movement, nutrition, recovery, substance use, and connectedness. More color within a component’s sector means that the patient is doing very well within that area, and less color means that the patient can find room for improvement within a given component. This figure was used with permission from: Frates B, Bonnet JP, Joseph R, Peterson JA. Lifestyle Medicine Handbook: An Introduction to the Power of Healthy Habits. 2nd ed. Monterey, CA: Healthy Learning; 2021.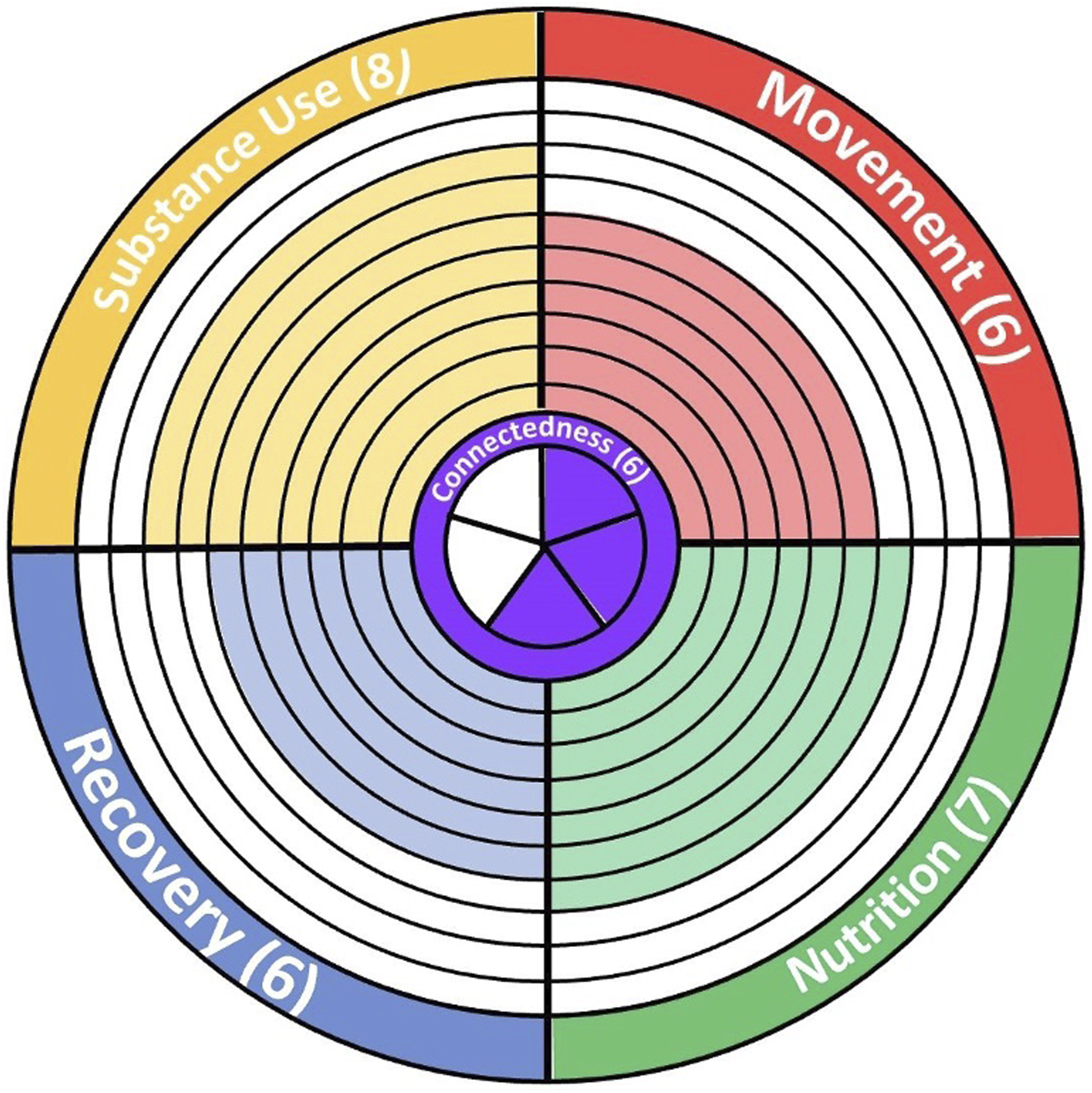
Patient age and gender were collected via the medical chart. Patients were then asked about which area of lifestyle medicine they felt they could use improvement in. LMA results were shown to the patient, explaining which category scored the lowest and which category scored the highest, using their individual diagram as a visual aid. Patients were then introduced to SMART goals, asked if they would like to create a goal, and guided on how to do so. SMART goals are defined as goals that are specific, measurable, achievable, relevant, and time-bound. For our protocol, this goal could be in any category, regardless of the assessment results. Time for intervention was defined as the time from asking which area of lifestyle medicine could use improvement to the end of the encounter. Each interaction was recorded in the medical chart with the patients’ lowest-scoring category, highest-scoring category, and SMART goal to refer to in the future.
Aim #2: Effect on Motivation, Perception, and Satisfaction
A separate survey analysis was conducted asking about (1) motivation to change certain behaviors, (2) perception of lifestyle changes on overall well-being, and (3) visit satisfaction. The survey distribution was conducted over a 5-week period with participants separated into control and LMA intervention groups through either a random generation coin toss (heads = LMA intervention, tails = control) or a random number generator with numbers 1-10 (even number = LMA intervention, odd number = control). Inclusion criteria for participation were as follows: (1) ages 18 years or older and (2) visit type consisting of annual well-check or follow-up visit. Each participant took a pre-encounter survey asking about age, gender, motivation to change lifestyle behaviors, and perception of changing lifestyle on their overall wellness. Motivation and perception of lifestyle changes were assessed using Likert scale questions. LMA intervention participants received an additional component before the encounter consisting of the LMA itself. The visit encounter was then conducted for each patient, with control participants receiving a standard visit where lifestyle modifications were discussed, and LMA intervention participants receiving lifestyle modification discussion utilizing the LMA they took, their individualized score diagram, and MI using their score diagram to set a SMART goal for lifestyle change. After the encounter took place, each participant in both groups received a post-encounter survey asking about visit satisfaction, motivation to change behaviors, and perception of lifestyle changes on overall wellness, similarly assessed using a Likert scale as in the pre-encounter survey.
Statistical Analysis
To analyze the feasibility of our approach in a standard outpatient setting, the mean, median, and range of time for the interactions with the first subset of patients were calculated. Chi-square and Fisher’s Exact tests were conducted to examine differences in gender and age between the intervention and control groups. To analyze if the motivation to change lifestyle behaviors increased from pre-encounter to post-encounter for each study group (i.e., LMA intervention group and control group), one-tailed, paired t-tests were conducted. To analyze if the perceived effect of lifestyle behaviors on well-being increased after the encounter for either group, one-tailed, paired t-tests were conducted. For both above t-tests, the hypothesis was that the intragroup difference would be greater than zero. Independent t-tests were conducted to assess differences in the pre- and post-outcomes (i.e., motivation and perceived effect) between the 2 study groups. Cohen’s D (standardized mean differences) were calculated to estimate effect sizes. ANCOVAs were conducted to examine differences in post-encounter outcomes between the study groups. Each ANCOVA included pre-encounter measure as the covariate. To analyze a difference in satisfaction with the visit between groups, a one-tailed, independent t-test was conducted between groups’ post-encounter data, with the hypothesis being that the difference in group mean scores would be greater than zero. All P-values < .05 were regarded as statistically significant.
Results
Aim 1: Feasibility of Implementation
Demographics of Participants in Phases 1 and 2.
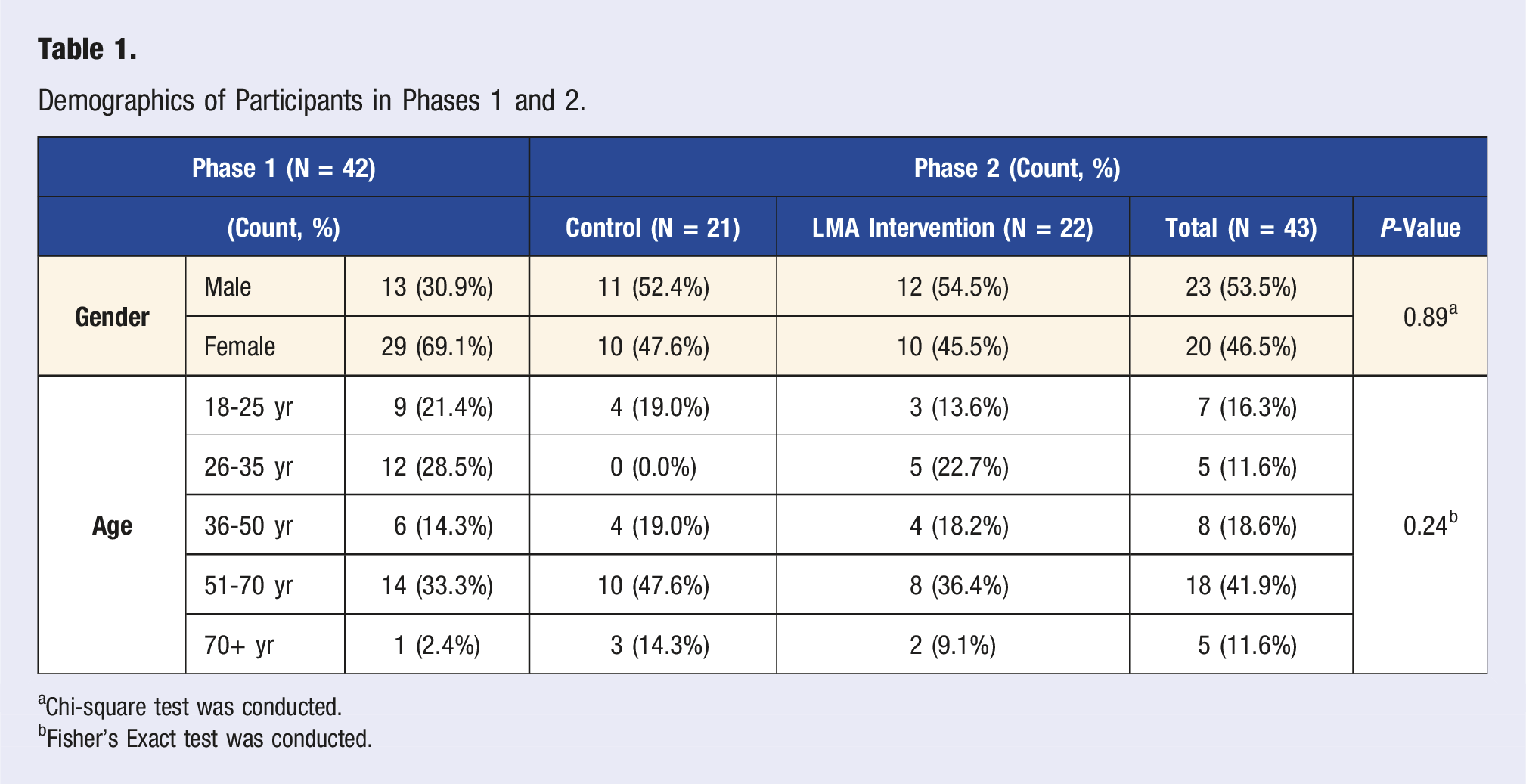
aChi-square test was conducted.
bFisher’s Exact test was conducted.
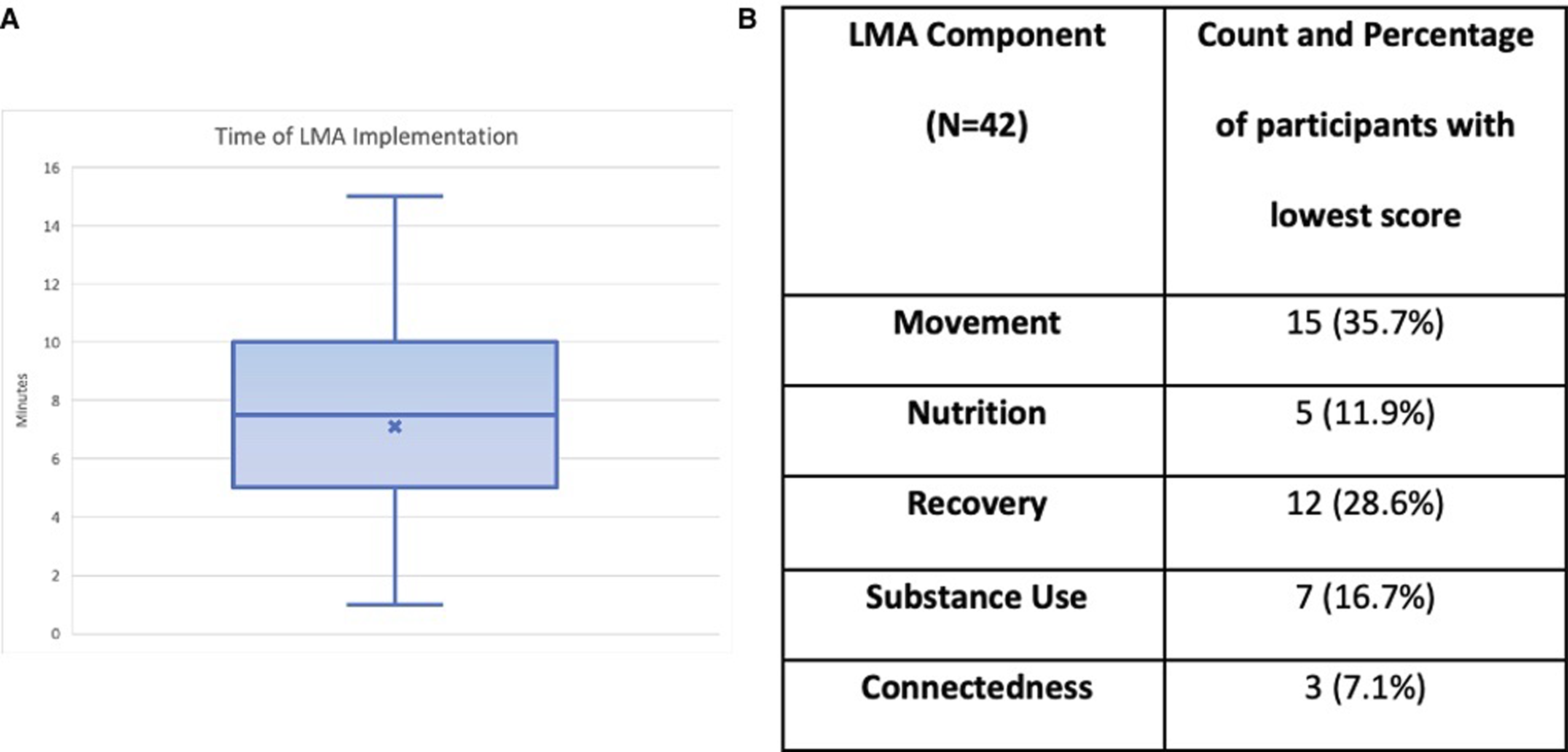
(A) Depicts a cat and whisker plot showing the time taken to implement the LMA/MI protocol in phase 1 of the study. The “x” on the plot represents the mean time of implementation, 7.12 minutes; (B) depicts what lifestyle medicine component the participants in phase 1 scored the lowest in. Scores in each category were within a range of 1-10 based on participants’ responses to the LMA survey questions.
Exercise was the lowest-scoring category for most respondents (35%), with recovery following closely behind (28%) (Figure 2). Substance use scored the lowest for 16% of respondents, nutrition for 12% of respondents, and connectedness for 9% of respondents. Only 36% of respondents were able to accurately predict their lowest-scoring category.
Aim 2: Effect on Motivation, Perception, and Satisfaction
Effect on Motivation, Perception, and Satisfaction.
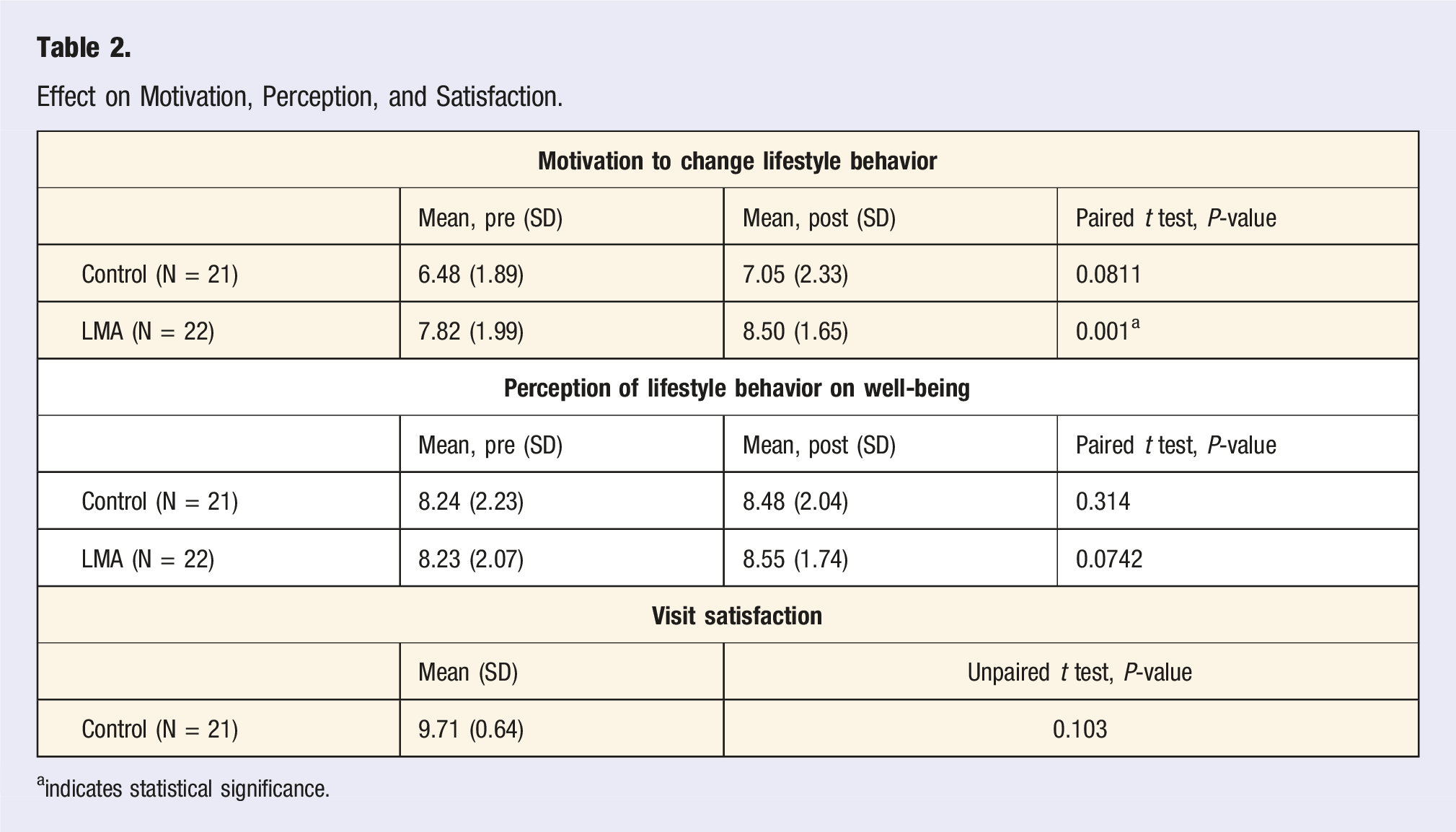
aindicates statistical significance.
Discussion
With our LMA tool protocol intervention, the average time to implementation was 7.12 minutes. This average supports the overall feasibility of utilizing the LMA tool in an outpatient setting to promote lifestyle change. With the median time of a standard primary care visit being 18.9 minutes, 19 this tool would allow for the introduction of lifestyle medicine in just under half of a typical visit. Physicians can prioritize the best times for lifestyle medicine implementation based on this time requirement. Appointments which are quick follow-ups or yearly check-ups will likely be the best times for implementation, while new-problem or diagnostic visits may not provide enough time for implementation.
Interestingly, patients in our sample were not accurate at predicting what their lowest-scoring category of lifestyle behaviors would be, highlighting the need for direct, objective approaches to present this information. Improved metacognition has been shown to help individuals manage and increase positive health behaviors. 20 Given this, the objective presentation of one’s performance in the 6 pillars of lifestyle medicine with the LMA tool may make individuals more aware of both their strengths and shortcomings, allowing for the introduction of better lifestyle behaviors. The LMA may also allow providers to identify trends in their patient populations to prioritize discussion when there is limited time. The lowest-scoring category in our sample was exercise, so prioritizing a discussion on exercise would have ensured this pillar was addressed.
In the second part of our study, the results show a statistically significant increase in motivation within the LMA intervention group. Given that there was not a significant increase in motivation within the control group before and after the encounter, this suggests that the LMA intervention protocol impacted the patient’s motivation to change lifestyle behaviors, although a direct comparison between the 2 groups was not conducted. In previous literature, motivation has been shown to have a positive association with eventual changed behaviors and outcomes. One study investigating the role of self-efficacy and motivation in adherence to exercise in patients with established coronary artery disease found that motivation was a significant predictor in both 6-month and 12-month adherence to exercise. 21 Another article demonstrated that motivation significantly predicted behavior change for behaviors such as cigarette smoking, coping with stress, food consumption, exercise, and seat belt usage. 22 Given the increased motivation demonstrated after using the LMA tool, this tool could be used as the first step in a longitudinal effort to change patient behavior in a primary care setting.
As shown, the perception of lifestyle changes on well-being and visit satisfaction were not significantly different from the within-group analyses of either the control or LMA intervention groups. While it was postulated that 1 or both factors might be influenced by the LMA protocol, there are plenty of reasons why this may not have been the case. In the LMA protocol, there was no part focusing solely on education about health habits and how they affect one’s health. It is possible that to change one’s perception of lifestyle behaviors on well-being, more explicit education illustrating the direct effects of various behaviors to disease processes must be included. Furthermore, many factors have been shown to influence patient satisfaction, such as wait time, insurance provider, and opinions about staff.23–25 It is possible that some of these factors confounded the above results.
Research Gaps and Areas for Future Study
The findings above reflecting the LMA’s ease of implementation and statistically significant effect on motivation to change behaviors are interesting and revealing. However, in the context of this, the data was limited due to a limited number of participants and short duration of the study. Given that these preliminary results were shown with a small sample size during a limited period, a larger iteration of this study over a longer period is needed to further validate and confirm the results we report.
Additionally, while our study did show that the LMA intervention increased patients’ motivation to change lifestyle behaviors, this finding is cross-sectional and therefore provides no data on how long this motivation lasts or if it translates to action. In a future study, the protocol could be adjusted to add follow-up data assessing motivation to change behaviors and implementation of SMART lifestyle goals at 1, 3, and/or 6 months. With this additional data, the longitudinal aspect of the LMA can be explored and tested.
The LMA tool itself does have some limitations. The tool takes lifestyle data only from the past week into account. If patients are coming in for an illness, this is likely to negatively impact their scores on the LMA tool due to being ill. Another limitation of the LMA tool is that it may not be generalizable. An argument can be made that the questions asked on the LMA tool do not accurately assess categories for all patients. For example, the movement category considers cardiorespiratory and resistance exercises, but for a patient with chronic pain or physical disability, these exercises may not be physically possible. It is important that with the application of the LMA tool, the aspects of wellness be personalized towards the patient’s specific needs and limitations.
Also, a limitation of the study is a potential lack of power to detect small differences within and between the groups. Lastly, participants from the first phase of the study may have participated in the second phase of the study as well, given that the 2 protocols were conducted at different times multiple months apart from one another. Patient identifiers or coded identifiers were not collected with each survey response, so there is no way to confirm that a participant included in the first protocol and results was not also included in the second protocol and results. This theoretically could have influenced survey answers to the pre- and post-encounter surveys conducted. Additionally, patients in the first protocol were recruited based on a convenience sample of who was in the clinic at the time of recruitment, potentially leading to the skewed gender distribution seen and resulting in a population that may not be generalizable to the entire clinic population. Future studies should include coded identifiers to prevent overlap between participants in each protocol and randomization of patient selection for recruitment in the first protocol. These coded identifiers would also be helpful in matching data at follow-up data points, discussed above.
Conclusion
In summary, the LMA was shown to be a feasible tool for the implementation of lifestyle medicine in a family medicine ambulatory clinic. It was associated with a significant increase in patient motivation to change behaviors. This increase in motivation has been an important indicator of actual behavior change in previous literature and may serve as a tool in assisting meaningful discussions between patients and providers on healthy lifestyle modifications. Larger studies are needed to support this preliminary evidence as well as track findings longitudinally, but the results described in this paper are promising for increasing lifestyle medicine guidance in patient care and improving patient outcomes in chronic disease management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data supporting the findings of this study are available upon reasonable request from the corresponding author.