
Abstract
Objectives: The purpose of this retrospective study is to further the limited body of evidence regarding the effects of a group-based boxing intervention for those with Parkinson’s disease (PD).
Design: A retrospective cohort study was performed analyzing data collected on outcome measures at 6-month intervals up to 2 years. Individuals participated in the standardized “Rock Steady Boxing” (RSB) program for up to 24 months. Every 6 months, measures were taken of balance (Fullerton Advanced Balance [FAB] Scale), functional mobility (Timed-Up and Go [TUG]), lower extremity strength (30-second Chair Stand [30CST]), and gait speed (10 Meter Walk Test [10MWT]).
Methods: Statistical significance (P < .05) was determined by a two-tailed t test. Data were collected from RSB-affiliated programs at 4 locations across the southeastern United States. Current and/or past participants in RSB with baseline and at least one subsequent outcome measure were included, resulting in 68 participants (54 male, 14 female, and mean age of 71.2 years ± 8.56 standard deviation).
Results: Statistically significant improvements in FAB scale, TUG, and 30CST over time were found at both 6- and 12-month time points. Significant changes continued through 18 months for FAB and 30CST. No significant changes in 10MWT were observed; however, a moderate effect size was observed at the 1-year point.
Conclusions: Participants with PD were able to achieve statistically significant improvements in standard measures of functional mobility, balance, and strength within the timeline of this study. Limitations include the retrospective nature, an inability to monitor adherence, and lack of control over pharmaceutical or other interventions.
A Retrospective Analysis of Group-Based Boxing Exercise on Measures of Physical Mobility in Patients With Parkinson Disease long-term participation in a circuit-based, non-contact boxing regimen is correlated with improvements over time on measures of functional mobility, balance, and lower extremity strength
Introduction
Parkinson’s disease (PD) is characterized as a progressive, multi-system, neurodegenerative disorder characterized by motor deficits 1 and dopamine depletion. 2 Approximately 60 000 new diagnoses are made within the United States each year.3,4 The cardinal symptoms of PD include bradykinesia, resting tremor, rigidity, and postural instability. 5 While individuals typically respond well to treatment, PD is progressive and generally requires an increasing amount of medication and symptom management further into the disease process. 3 Numerous studies have assessed and demonstrated benefits of independent exercise and group-based exercise, in the management of motor and cognitive symptoms associated with PD.6-10
Traditional exercises—including strength, flexibility, aerobic training, and balance training—have been shown to have positive impacts on those with PD on measures of muscle strength, endurance, gait, physical fitness and function, balance control, postural instability, transfers, freezing of gait, and reduction in the number of falls. 6 Non-traditional exercises have shown improvements in gait speed,8,11-13 quality of life (QOL),8,11,14-17 dynamic and static balance,11,13,15,17 functional mobility,14,15,17 and motor scores based on the Unified Parkinson’s Disease Rating Scale (UPDRS).11,13-15,17 “Rock Steady Boxing” (RSB) is a commercially marketed, group-based exercise incorporating traditional/non-traditional exercises for strength, endurance, and balance training with non-contact boxing activities. 18 There is limited published research on the effects of this type of exercise on patients with PD. Research has demonstrated improvements in static and dynamic balance, balance confidence, gait parameters, functional mobility, endurance, lower extremity strength, PD-specific disability, and QOL with participation in RSB.18-20 Those results indicate that significant improvements in gait velocity and gait endurance were found only in the boxing group when compared to traditional exercises for individuals with PD. 18 Due to the regimented nature of the RSB program and the previously published scientific results, we aim to expand on this area of research to identify potential effects of this intervention over a longer period of time and with a greater number of subjects compared to previous studies. Our goal was to use tests of motor function, impairments and activity limitations commonly used in physical rehabilitation to evaluate the potential for improvement in these areas using this group-based boxing exercise program. We hypothesize that significant improvements to standardized measures of balance, strength, and functional mobility will be observed in PD participants of this circuit-oriented, non-contact boxing routine.
Methods
Study Design
A retrospective, multicenter analysis was conducted using records from 4 facilities in the southeastern United States. The study was approved by the Institutional Review Board of the last authors’ academic institution, and all data were de-identified prior to receipt from the facilities to protect the identity and personal information of the participants.
Participants
A standardized email was sent to 240 RSB-affiliated locations across the southeastern United States requesting patient data which included the primary outcome measures (Fullerton Advanced Balance [FAB], Timed-Up and Go [TUG], 30-second Chair Stand [30CST], and 10 Meter Walk Test [10MWT]). Demographic data including age, year diagnosed with PD, gender, medications, and co-morbidities were requested, in addition to data collected on outcome measures. Of those 240 locations, 4 facilities provided measures for past and/or current participants enrolled in the RSB program. Records were included in the study if the participant had a diagnosis of PD and was an active or a previously active member of a RSB-affiliated center with baseline and subsequent outcome measures. Participant records were excluded from data analysis if they lacked a baseline outcome measure and a subsequent outcome assessment at a later time period. After the inclusion and exclusion criteria were applied, the records of 54 men and 14 women with a mean age of 71.2 years (± 8.56 standard deviation) were included in the data analysis. The 4 boxing facilities provided de-identified data without transferring personally identifiable patient information to the investigators.
Outcome Measures
Participants included in the study had the following outcome measures assessed at baseline (n = 68), 6 months (n = 50), 12 months (n = 42), 18 months (n = 17), and 24 months (n = 8): Timed-Up and Go (TUG), 10MWT, 30CST, and the Fullerton Advanced Balance Scale (FAB Scale). These outcome measures were recorded by trained non-clinical staff at the RSB-affiliated institutions. Affiliate coaches of Rock Steady Boxing, Inc. have been trained on the administration of the outcome measures recommended by the organization to be utilized to track the functional progress of program participants. Affiliate coaches are trained by either a physician, a physical therapist, or an Exercise is Medicine certified exercise professional by American College of Sports Medicine. Each RSB-affiliated facility has the freedom to select the outcome measures that will be administered in their location. Clinical information such as UPDRS score was not included as an outcome measure because it evaluates numerous non-motor symptoms. The TUG measures the time for a participant to rise from a chair, walk 3 m, turn around, and return to a seated position in the chair. The 10MWT is performed by measuring the total time taken to ambulate 6 m at an individual’s comfortable or fast gait speeds. The 30CST encourages the participant to complete as many sit-to-stands as possible in a 30-second period without the use of their arms. A score of zero is automatically scored if the participant uses their arms during the test. The FAB Scale is made up of 10 items including static and dynamic postural control, feedforward/feedback postural control, and sensory reception and integration. 20 Outcome measures at each time point were measured against the baselines only of the patients that participated in that time point.
Intervention
The original exercise protocol by Rock Steady Boxing, Inc. recommends that each participant attend classes 2 to 3 times a week, for a maximum of 90 minutes each class. Each RSB-affiliated site has the flexibility to adjust their daily workout depending on the needs of each affiliated site and the needs of the program participants. The RSB-affiliated sites in this study have the participants exercise between 75 and 90 minutes each class session in a group setting led by an RSB certified instructor. The different sites offered different numbers of classes to participants with a minimum of 5 classes available each week in one location and a maximum of 13 classes available in another location. While the exercise protocols are different from class to class, RSB-related activities generally include aerobic training with walking laps around the gym or jumping ropes, resistance exercises with free weights and resistance bands, agility exercises including footwork patterns or large amplitude stepping, non-contact boxing with the use of punching gloves and punching bags, hand–eye coordination or manual dexterity activities, and stretching of the entire body.
Data Analysis
Paired sample two-tailed t-tests identified within-group differences across time periods, with each 6-month time point compared to an adjusted baseline to account for participants who were not assessed at every time point. Results were considered significant at a P-value < .05. Cohen’s D was used to calculate effect sizes. IBM SPSS Statistics for Windows version 25 (IBM Corp. Armonk, NY) was used to perform the statistical testing.
Results
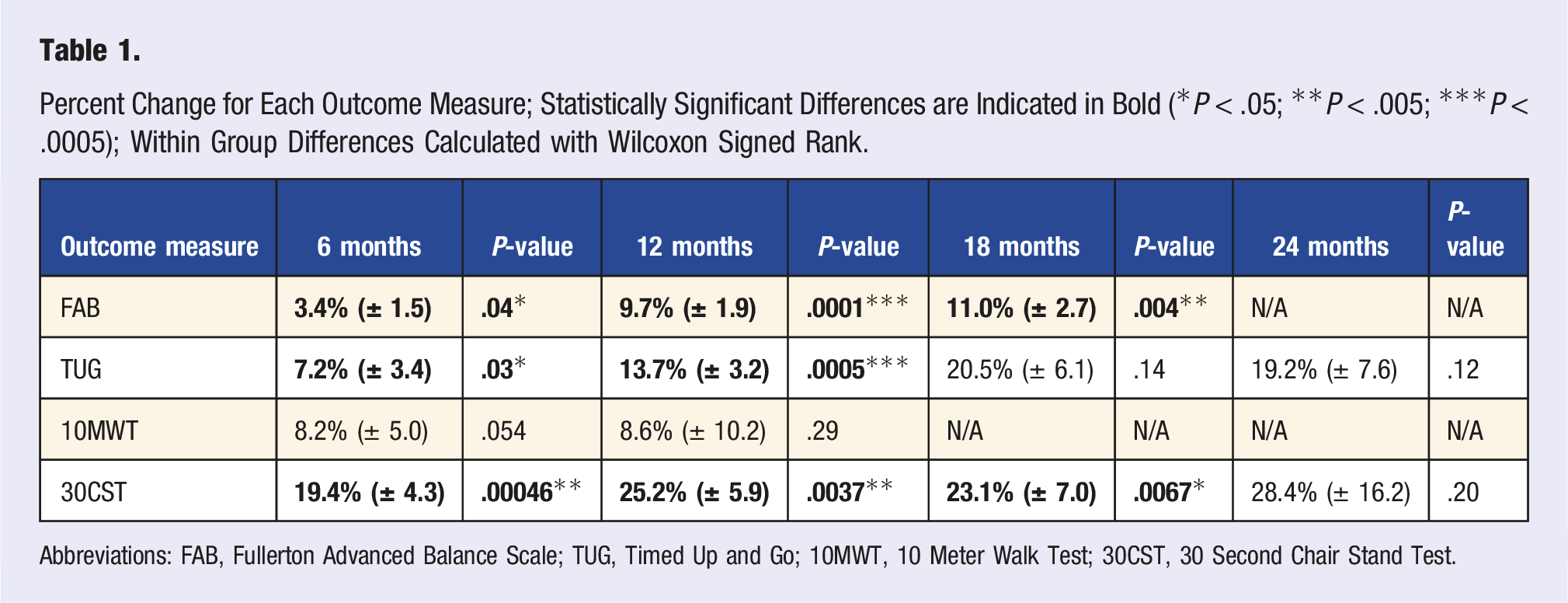
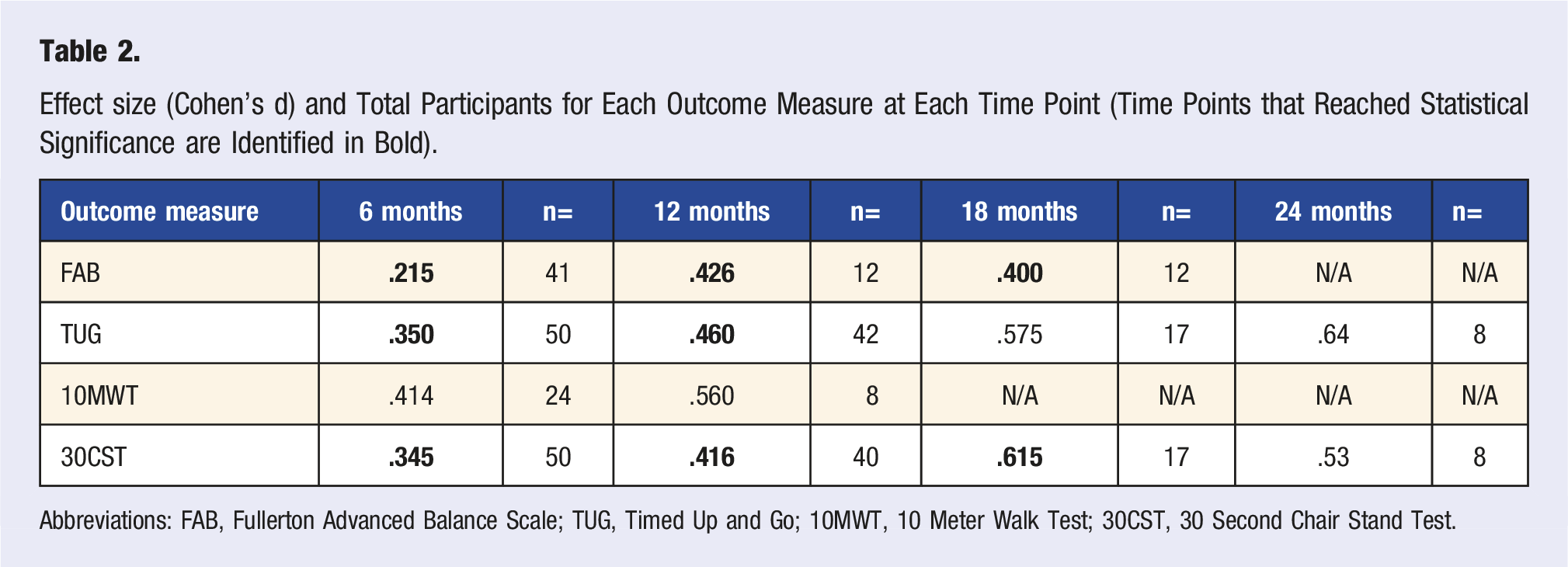
Statistically significant within-group differences were exhibited at the 6-month time in measures of FAB Scale (P = .04, 3.4% improvement), TUG (P = .03, 7.2% improvement), and 30CST (P = .0009, 19.4% improvement) Figure 1 and Table 1). While statistically significant differences were not seen at the 6-month period for the 10MWT (P = .054), the trend was toward a positive change in gait speed, evident by an average sub-significant decrease of .45 s to complete this outcome measure (or an increase of .16 m/s in gait speed). At the 12-month time, improvements in measures of FAB Scale (P = .00001, 9.7% improvement), TUG (P = .0005, 13.7% improvement), and 30CST (P = .0037, 25.2% improvement) were seen. Statistically significant improvements were not shown at the 12-month period for the 10MWT (P = .29), but as was the case at the 6-month point, a trend toward positive changes in gait speed were observed with an average sub-significant decrease of .54 s to this outcome measure (or an increase of .2 m/s in gait speed). At the 18-month time span, only the FAB Scale (P = .0004, 11.0% improvement) and 30CST (P = .0067, 28.4% improvement) demonstrated statistically significant changes. No statistically significant improvements were found at the 24-month time in measures of TUG or 30CST, while data were not obtained for the FAB at this time span, or for the 10MWT at the 18-month or 24-month times. Despite this finding, moderate effect sizes (.53-.64) were determined at the 24 month period for the TUG and 30CST as shown in Table 2, and sample size calculation suggests significance could be approached with an n = 36 for the TUG and n = 21 for the 30CST using a priori analysis with G Power 3.1.9.2. Small to moderate effects were found with all outcome measures, with greater effect sizes found at later time points (Table 2). Time-use activity behaviours are distinct but related and are also part of circadian regulation. Abbreviation: METs, metabolic equivalents. Percent Change for Each Outcome Measure; Statistically Significant Differences are Indicated in Bold (*P < .05; **P < .005; ***P < .0005); Within Group Differences Calculated with Wilcoxon Signed Rank. Abbreviations: FAB, Fullerton Advanced Balance Scale; TUG, Timed Up and Go; 10MWT, 10 Meter Walk Test; 30CST, 30 Second Chair Stand Test. Effect size (Cohen’s d) and Total Participants for Each Outcome Measure at Each Time Point (Time Points that Reached Statistical Significance are Identified in Bold). Abbreviations: FAB, Fullerton Advanced Balance Scale; TUG, Timed Up and Go; 10MWT, 10 Meter Walk Test; 30CST, 30 Second Chair Stand Test.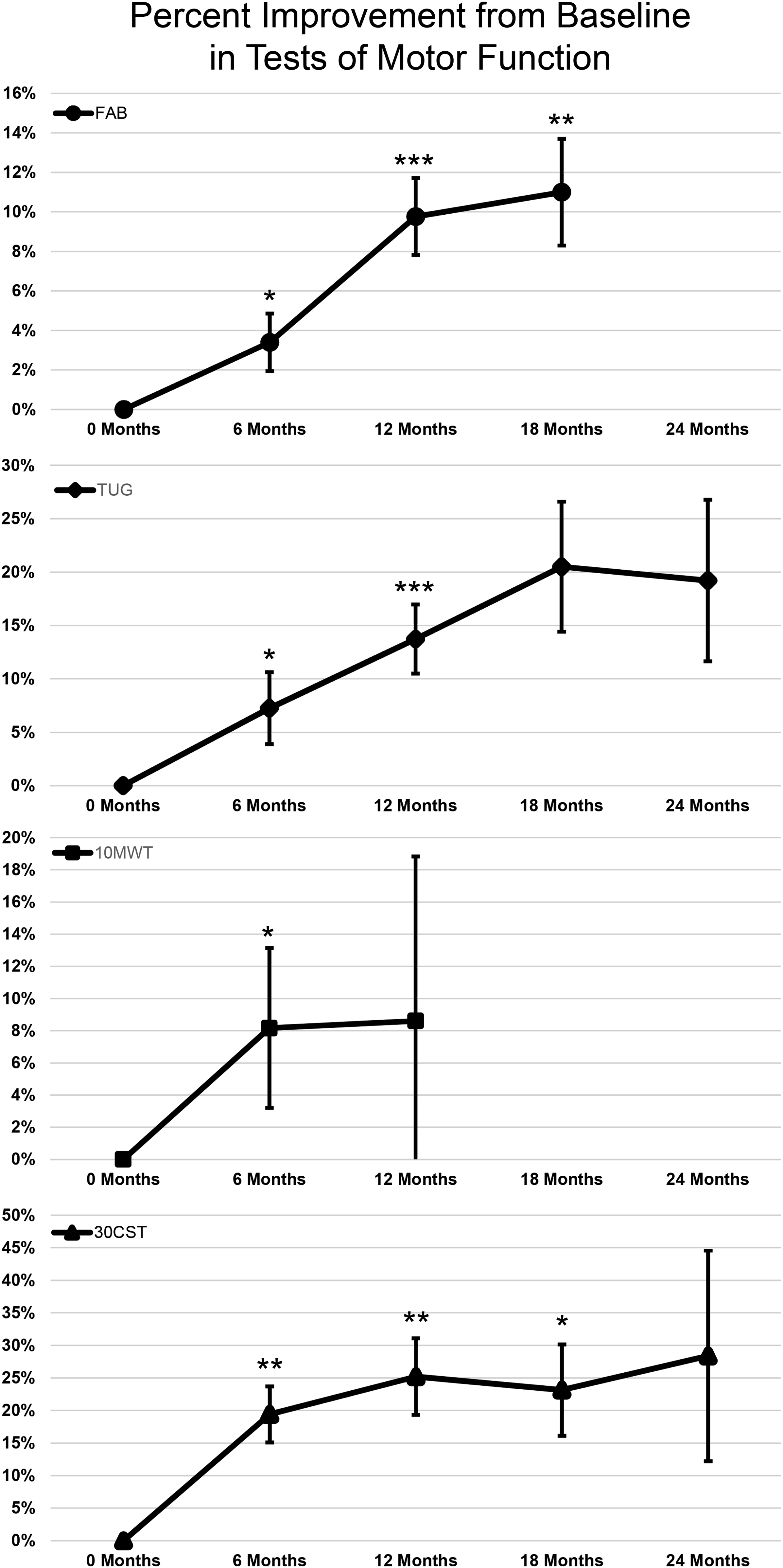
Discussion
Significant improvements were observed for measures of balance, strength, and functional mobility for subjects participating in a circuit-oriented, non-contact boxing program incorporating these skills. All measures besides the 10MWT demonstrated significant improvements at multiple time points up to 18 months after beginning this intervention. The mean percent change increased at each time point for all outcome measures to the 24-month time point. The average percent of remaining participants in the study at 6, 12, 18, and 24 months was 70%, 49%, 17%, and 6%, respectively.
The TUG, which demonstrated significant improvements at 6 and 12 months, has previously been determined to be a reliable and valid measure of mobility in persons with PD and is commonly used to assess lower limb function, mobility, and fall risk.21,22 A cut-off value of 11.5 seconds has been proposed representing the specificity (62%) and sensitivity (66%) to discriminate between fallers and non-fallers with PD. The TUG has been shown to have an excellent test–retest reliability (ICC of .80) in patients with PD. 23 The Minimal Detectable Change (MDC) 24 of the TUG was determined to be 3.5 seconds for those with PD. 23 While few individuals of our study reached this MDC of 3.5 seconds, our mean baseline TUG time of 8.40 s was much lower than the mean TUG score of 14.8 s from a previously published study of 25 subjects with PD and an average H&Y stage of II. 25 Mean TUG score at 6 and 12 months were 7.45 s and 7.72 s, respectively. Participants with good motor function may self-select for exercise-based therapy, and it may have been less feasible for our population studied to improve by the MDC of 3.5 s when they began with a significantly faster TUG time than what may be normal for those with PD.
The 10MWT is a measure of gait speed, which is a significant predictor of health and functional status; and it is an important predictor of future falls for those with PD.26,27 In a study on gait speed of individuals with PD (n = 37), the Minimal Clinically Important Difference (MCID) for the 10MWT is .18 m/s for comfortable gait speed and .25 m/s for fast gait speed. 28 The MCID, 24 unlike the MDC, is the minimal change in a measure that is the smallest change in a treatment outcome that an individual patient would identify as clinically important. The same study found that the 10MWT has an excellent test–retest reliability both for comfortable (ICC = .96) and fast gait speed (ICC = .97). 28 The 10MWT in individuals with PD was found to have high test–retest reliability for comfortable (ICC = .98) and fast gait speed (ICC = .99). 29 Our initial baseline mean average was 1.40 m/s, with mean times of 1.57 m/s and 1.59 m/s at 6 and 12 months, respectively. While the changes in 10MWT did not reach significance at 6 or 12 months, 11 of 24 (∼46%) participants reached the MCID for comfortable and fast gait speed at 6 months and 3 of 8 (37.5%) individuals reached the MCID for both at 12 months. A moderate effect size (.56) was also found at the 12-month time.
Lower extremity strength has often been measured repeatedly using sit-to-stand testing.30-32 Other studies have found the 30CTS to be a reliable and valid indicator of lower extremity strength in this geriatric population. 30 A study of the psychometric properties of the 30CST in individuals (n = 22) in the early stages of PD (Hoehn and Yahr stages I-III) determined that the 30CST had an excellent test–retest reliability (ICC = .94) and that the MDC was 3 repetitions. 33 The results of the study also indicated that the 30CST may be superior to the 5-time sit-to-stand to document clinical change. Statistically significant changes were found up to 18 months with average scores of 15.6, 13.6, and 17.17 found at 6, 12, and 18 months, respectively. Twenty of 50 (40%) individuals at 6 months reached the MDC and 18 of 40 (45%) individuals at 12 months.
The FAB Scale was originally developed as an assessment of postural control in the higher functioning elderly but was found to be reliable and valid to assess postural control in those with PD. 34 The FAB Scale has been validated to assess postural control and balance disturbances in patients with PD. 34 The FAB Scale has been found to have an excellent interrater and test–retest reliability (ICC = .99). There is an excellent correlation with the Mini-BESTest (Spearman r = .87) and TUG test item of the MiniBESTest (Spearman r = .83) in assessing postural control in patients with PD. Our present study is the first time that the FAB Scale has been used in a study of RSB participants and unlike the BBS used in previous RSB studies, contains an evaluation of reactive postural control, and assesses postural stability while performing a secondary task, shown to be impaired in those with PD. It also contains more difficult dynamic balance challenges such as stepping up, onto, and over a 6-inch bench; tandem walk; and a two-footed jump. The BBS has a ceiling effect, with 17.6% of participants scoring a 56/56, while the FAB Scale was determined to have a minimal ceiling effect. 34 It was found that patients are rated 26.9% higher with the BBS compared to the FAB Scale and that 4 participants who scored the maximal BBS reported at least 1 fall in the last 6 months, while no participants who scored the maximal value on the FAB Scale had fallen in the last 6 months. No normative data or MDC have been established using the FAB Scale for patients with PD. The mean initial baseline of our study was 28.6 points with mean scores of 29.9, 31.9, and 32.3 found at 6, 12, and 18 months, respectively. While we cannot determine clinical significance according to an established MCID or MDC, the changes were deemed statistically significant for all 3 months.
Improvements in balance, strength, and functional mobility may be related to the nature of the activities performed during each exercise session. These activities incorporate dynamic balance challenges such as multidirectional stepping, single leg balance, changes in base of support, and training on surfaces of varying pliability. Each of these activities differentially challenges the 3 balance systems: visual, somatosensory, and vestibular. This program also includes strengthening activities such as sit-to-stands, squats, and concentric lifting that may explain improvements in the 30CST. While these exercises incorporate and improve balance and strength, both requirements for normalized gait speed, 35 significant changes were not observed in the 10MWT. This may suggest that to significantly improve gait speed, interventions would have to specifically target gait and therefore be task specific. This result differs from previous studies showing statistically significant improvements in gait velocity with this same type of intervention.18,19 Similar findings regarding balance and functional mobility were seen in comparative studies.18-20 A strength of our study was the measurement of lower extremity strength in a multi-center design including numerous geographically separated RSB-affiliated sites with the application of this intervention. While many of the average changes observed for each group were below the MDC for those tests, the aggregate data produced significant positive change in multiple measures of motor function, including balance, mobility, and lower limb strength.
Missing data points were noted for each outcome measure at all time points following the baseline. As this was a retrospective study, we were unable to control for this high degree of drop-out; however, using paired sample t-tests with adjusted baseline scores allowed for us to compensate in our statistical analysis. It also allowed us to include participant’s data that otherwise would have been excluded with measures such as a Repeated Measures ANOVA, which requires complete data points over the continuum for each participant. Using paired sample t-tests allowed us to show that positive, significant, changes did occur with participation in RSB over a longer time and larger participant pool than has previously been analyzed.
Study Limitations
Our study’s strength was in its assessment of the effects of a circuit-based, non-contact boxing program over 24 months for participants with PD using a multi-center design. Our study also included a range of measurements of physical mobility including lower extremity tests. However, the nature of our study limits our ability to generalize effects beyond the group-based exercise cohort targeted in this retrospectively analyzed cohort. As a retrospective, multi-center, single-arm study, we did not compare participation in boxing with a control group such as another intervention or a placebo, nor were we able to control for the participants’ adherence or the potential use of other interventions. Therefore, we are unable to make a conclusion regarding causation. It is feasible that the drop-out rates can be interpreted as a bimodal response in which some participants have strong positive effects while others do not, or that disease progression complicates performance. Future prospective, controlled, and randomized dose response studies are needed before the observed effects can be causally attributed. All outcome measures included in the study were carried out by trained individuals employed by the various number of affiliated RSB locations, but the potential for variation in outcome measurement was present. The data were collected prior to solicitation for inclusion in the research project; but unfortunately, while outcome measure collection included a common standard training by credentialed clinicians, cross-facility standardization of outcome measures could not be validated and test order bias cannot be ruled out. Individuals with notably higher outcome measure performance were recorded for each outcome measure, which may have influenced the statistical significance of some assessments and time points. Instructors at RSB-affiliated programs must go through a standardized certification process; however, there is no guarantee for standardization of RSB class structure. Furthermore, patient participation and adherence in this voluntary RSB program were not recorded so a dose response curve related to time involvement could not be determined. Comparisons at each time point were made to an adjusted baseline to account for decreases in participants assessed at each successive time point, but calculations of effect size and statistical significance indicate sufficient size to justify the conclusions presented here. The Hoen and Yahr stage of each participant was not evaluated, but based on the nature of activities involved in the RSB program, we feel justified in assuming participants ranged from stage I to III. As a result, we cannot make conclusions regarding the effectiveness of participation by Hoen and Yahr stage. While we feel justified in concluding that the motor-based outcome measures significantly improved in the included participants found in this observational study, future studies are needed with additional controls. The scope of our study was to evaluate common measures used in the physical therapy setting while evaluating exercise as an intervention in PD. Future studies should continue to include these measures but also include additional measures such as UPDRS, medication dosage, and brain imaging to identify if there is a neuro-therapeutic effect of the exercise-as-intervention model.
Conclusion
Our study demonstrated that participants were able to achieve statistically significant improvements in measures of functional mobility, balance, and strength. While we cannot conclude that this intervention alone is cause for these findings, we can conclude that long-term participation in a circuit-based, non-contact boxing regimen is correlated with improvements over time on measures of functional mobility, balance, and lower extremity strength. This study adds to previous literature showing that this intervention is safe, feasible, and effective for improving motor symptoms of PD. Future studies should continue to evaluate these motor-based outcome measures while including additional measures of PD progression.
Supplemental Material
sj-xlsx-1-ajl-10.1177_15598276211028144 – Supplemental Material for A Retrospective Analysis of Group-Based Boxing Exercise on Measures of Physical Mobility in Patients With Parkinson Disease
Supplemental Material, sj-xlsx-1-ajl-10.1177_15598276211028144 for A Retrospective Analysis of Group-Based Boxing Exercise on Measures of Physical Mobility in Patients With Parkinson Disease by James W. H. Sonne, Kyle Joslyn, Katherine Reus, Michelle Angulo, Sarah Guettler and Morris C. Beato in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Due to its retrospective nature, the Institutional Review Board of University of Central Florida deemed this study “Exempt”.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.