
Abstract
Purpose: This study investigated the impact of a novel group health coaching curriculum on self-efficacy, overall sense of well-being, and self-reported behavior change for people with Parkinson disease (PwP). Methods: This pretest-posttest, mixed-methods study introduced a novel group health coaching curriculum, developed by a Parkinson nurse navigator and certified health coach, to target self-efficacy and well-being in PwP. Data was analyzed via descriptive statistics of survey data and thematic analysis. Findings: With a sample size of 17 participants taking the pre-intervention survey and 12 taking the post-survey, results revealed a 0.27-point average improvement for the Neuro-QoL Positive Affect and Well-Being scale with the highest increase noted in feelings of a sense of purpose with a 0.47-point increase. PROMIS Self-Efficacy scores improved in 8 out of 10 items by an average of 0.22 points. Thematic analysis revealed five domains of participant-perceived benefits including exercise, nutrition, commitment, community building, and goal setting. Conclusion: Preliminary data indicates that this novel group health coaching model and curriculum for Parkinson disease has potential to positively impact well-being, self-efficacy, and self-reported healthy habits. Given results of this pilot initiative, future research to increase sample size and expand objective measurements is warranted.
Keywords
“Certified health coaches are effective communicators trained in evidence-based behavior modification strategies that empower participants.”
Introduction
The prevalence of Parkinson’s disease (PD) has been steadily increasing over the past three decades, leading to a significant global burden of disease. 1 Despite the high prevalence of disease, there is no cure nor are there FDA-approved disease-modifying interventions. This has led to the development of a multitude of programs and tools to improve quality of life (QoL) for people with Parkinson disease (PwP) and their care partners. While these programs can be immensely helpful for PwP, they are often underutilized. 2 With decreased self-efficacy compared to the general population, PwP tend to have diminished belief in their abilities to achieve goals or to engage in various activities that have the potential to improve symptoms and even QoL. 3 The non-motor symptoms of PD, such as depressed mood, apathy, and cognitive decline, can additionally contribute to poor self-efficacy in PwP.3,4
Programs that aim to increase self-efficacy and sense of well-being for PwP have the potential to profoundly impact motivation to actively participate in care, establish healthy habits, and form attainable goals. A cross-sectional study conducted by Estrada-Bellmann et al revealed a significant correlation between decreased self-efficacy and poor performance on the International Parkinson and Movement Disorder Society’s Unified Parkinson Disease Rating Scale, Non-Motor Symptoms Scale for PD, and the Parkinson’s Disease Questionnaire. 5 Improved self-efficacy can increase engagement with activities that help alleviate symptoms, such as exercise. While there are no surgical or pharmacologic therapies to reverse disease, exercise may be effective in slowing disease progression, making participation among PwP especially important.6-8
Many PwP seem to lack the motivation needed to participate in healthy habits. This perceived poor motivation is multifactorial. Fatigue, severity of motor symptoms, apathy, and depressed mood may impact the desire for PwP to engage in exercise.9,10 In one qualitative study from Ahern et al, some PwP expressed a feeling of being “pushed” to exercise by their health care providers and found that they were more likely to exercise when encouraged by family members or friends. 10
Group programming could address the tendency for PwP to withdraw from social settings. Stigma and shame are commonly experienced, with up to 85% of PwP feeling embarrassment related to their disease. 11 Over 22% of PwP feel the need to conceal their diagnosis, further worsening loneliness and a perceived lack of social support. 12 Community-based programs have shown to significantly improve social withdrawal among PwP by introducing an additional opportunity for social engagement and peer support.13,14
Individualized health coaching is shown to broadly improve health behaviors by empowering PwP to acquire agency over their health, and can improve non-motor symptoms such as apathy, mood, and decreased self-efficacy.15-18 Moreover, the benefits of individualized health coaching in PD include significant improvement in QoL and treatment adherence for motor and cognitive function. 19 In those with chronic illness, wellness coaching programs can significantly improve self-efficacy in as little as one and a half months and continue to benefit depressive symptoms for up to one year. 20 Those who participated in health coaching exhibited sustained changes in their overall health habits. 21 Both individualized and group health coaching can improve goal attainment and reduce procrastination. 22
Given these evidenced impacts, individual health coaching and group programming can be offered to PwP in standard treatment plans. However, implementation of individual health coaching may be challenging due to limited capacity of and access to a health coach. Though individualized health coaching has demonstrated great promise in PwP, the potential benefits of group health coaching programs in PD have yet to be described. Further, when health coaching techniques are delivered by a trained, knowledgeable health professional in supportive group settings, these factors may work synergistically to improve social isolation and loneliness, self-efficacy, and motivation for PwP. In this pilot study, we explore the feasibility, acceptability, and potential impact of a group health coaching program in PwP.
Methods
Participants
Broad inclusion criteria were adopted for the program. Inclusion criteria required participants to be 18 years of age or older, carry an established diagnosis of PD, and be able to connect to a virtual meeting. Strict exclusion criteria were not established regarding disease duration or stage of disease. Participants were recruited from a single academic movement disorders outpatient clinic. While participants may have attended other movement disorders care center programming, our participants did not have pre-existing relationships.
Curriculum Design
The core curriculum was developed by a specialized Parkinson nurse navigator who had certification in health and wellness coaching. The curriculum sought to address the needs of PwP with the primary aim of cultivating healthy lifestyle and behavioral changes and reducing social isolation with a participant-driven approach. In line with the foundational principles of health and wellness coaching, participants were encouraged to approach one another with unconditional positive regard and non-judgmental curiosity. 23 Participants were considered experts in their respective experiences with PD. Participants were encouraged to explore the power of the group’s cumulative experiential knowledge, thus emphasis on group rapport through supportive conversation was a key component of each class.
The curriculum was semi-structured. The longitudinal progression of the participant included initial focus on education and guided self-exploration, shifting toward participant-driven themes in later classes. This transformation demonstrated the group’s growth and autonomy in the coaching process over time. Educational topics addressed in initial classes included an introduction to health coaching through the lens of positive psychology and the effectiveness of lifestyle interventions in managing PD. Guided self-exploration tasks involved envisioning a positive future, identifying and leveraging character strengths, identifying a healthy habit to work toward, and finally, the creation of actionable, individualized weekly goals. Each participant shared their weekly progress toward personal goals. Such participant reports served to create individual accountability from the group and by reflecting on and celebrating successes, allowed participants to implement their learned positive psychology principles. Barriers to success were also collaboratively brainstormed as a group when appropriate. Such brainstorming led to reassessment and determination of goals for the next 7 days. Additional education and resources were provided by the nurse health coach as needed throughout the program. This process was repeated until the 10th and final class wherein participants reflected on their successes and planned for continued growth.
Study Design
This pre-post, mixed-methods, quasi-experimental study funded by a community grant from the Parkinson’s Foundation examined the impact of group health coaching for PwP on participant well-being and self-efficacy via pre- and post-intervention surveys. The study was deemed exempt by the Yale University Institutional Review Board (IRB). A modified informed consent was obtained for each participant, who was made aware that anonymized results would be utilized for research and that their participation was voluntary.
From September 2024 to June 2025, we developed a total of three separate virtual group health coaching program cohorts. Each class accommodated up to 10 participants, and the groups met weekly for 1 hour for 10 consecutive weeks. Topics included exercise education, identifying character strengths, personalized goal setting, finding motivation, and overcoming obstacles. Participants were recruited from movement disorder clinics within the Yale Medicine and Yale New Haven Health systems, and from community outreach events. The primary study aim was to assess the effectiveness of group health coaching for improving self-efficacy and sense of well-being for PwP. Primary outcome measures included a modified Patient Reported Outcomes Measurement Information System (PROMIS) General Self-Efficacy scale and the Quality of Life in Neurological Disorders (Neuro-QOL) Positive Affect and Well-Being scale. Items from both measures are rated on a five-point Likert scale with a five indicating the highest level of confidence in the PROMIS General Self-Efficacy scale and indicating the highest frequency in which the participant relates to each statement for the Neuro-QOL Positive Affect and Well-Being scale.24,25 Qualitative data was also collected via open-ended survey questions. Secondarily, demographic data was collected that allowed for comparison between personal characteristics and response to group health coaching.
Data Collection
Surveys were completed via an online Qualtrics link. Anonymized results were collected prior to and at the completion of each group health coaching program to reduce recall bias. To evaluate the impact of the programming on participant well-being and self-efficacy, the Neuro-QOL Positive Affect and Well-Being scale and PROMIS General Self-Efficacy scales were utilized. Demographic information was also gathered, and participants had the opportunity to provide qualitative feedback to questions relating to individual goals and goal attainment as well as perceived pros and cons about the program.
Statistical Analysis
Raw scores were calculated for the Self-Efficacy and Well-Being scales. Raw scores were averaged for each item to allow for direct comparison before and after group health coaching sessions. As the survey data was not paired prior to and after the group health coaching intervention, and Gaussian distribution could not be assumed, a two-tailed, Mann–Whitney U test with a significance level of 0.05 was utilized to determine statistical significance. Descriptive analyses were also obtained to assess the demographics of the sample population. In addition to quantitative measurements, open-ended questions were included to capture participants’ subjective experiences and perceptions regarding the group health coaching sessions. Thematic analysis was used to analyze responses with initial responses being manually coded and assigned to broader themes.
Results
Sample Characteristics
There were a total of 29 group health coaching participants, including 28 people with PD and one care partner. Of these 29 participants, 12 identified as female and 17 identified as male. Seventeen participants completed the pre-group health coaching survey with 12 completing the post-group health coaching survey. All participants who completed the surveys indicated that they have had a diagnosis of PD with disease duration ranging from 3 months to 16 years. All participants were recruited from the academic movement disorders clinic. Of the initial survey participants, 82.35% had a bachelor’s degree or higher with all participants having completed at least some college. Approximately 88.24% of those participants identified as white with the remaining 11.76% identifying as Asian.
Positive Affect and Well-Being
Neuro-QoL Positive Affect and Well-Being averages before and after group health coaching for Parkinson disease.
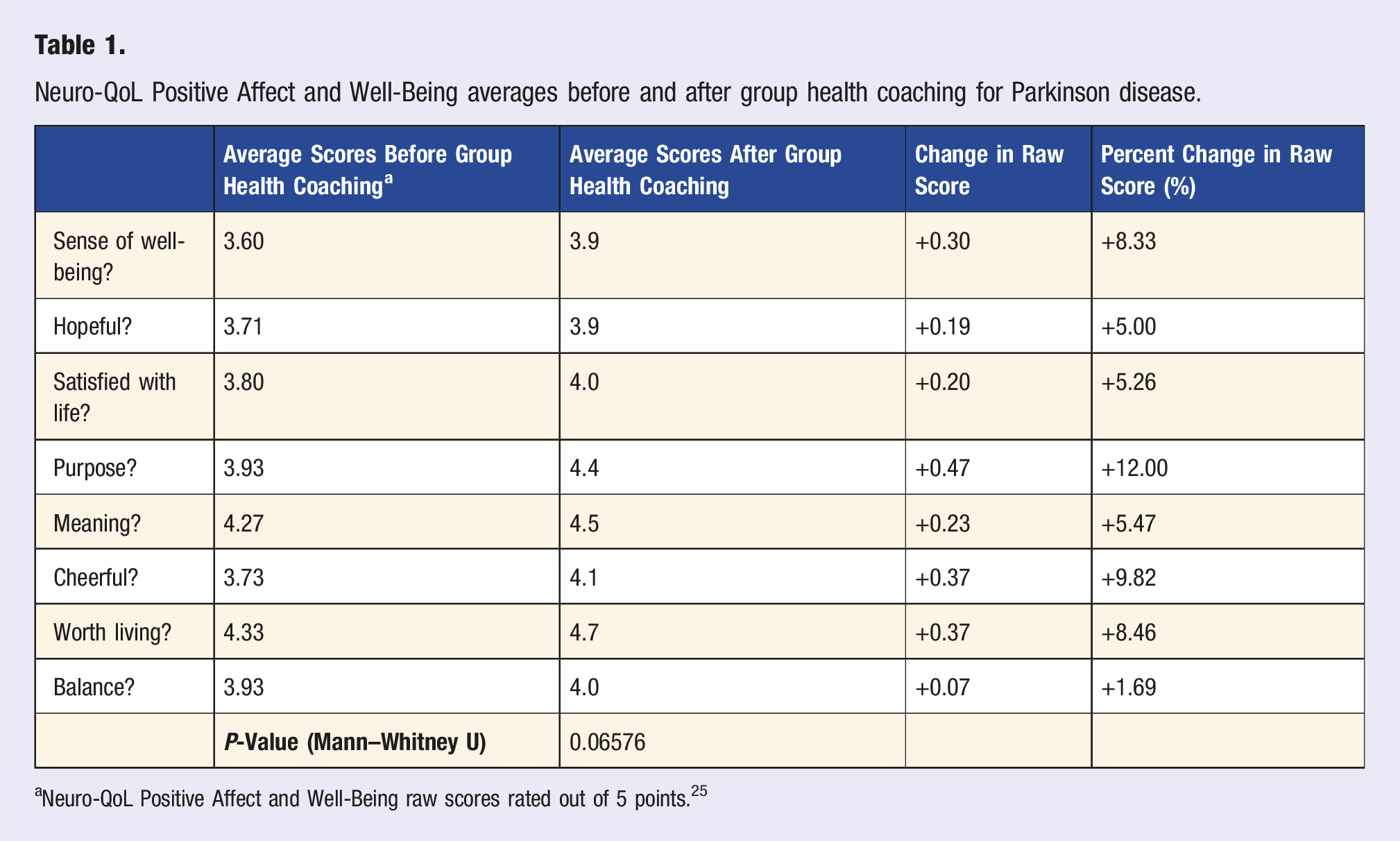
aNeuro-QoL Positive Affect and Well-Being raw scores rated out of 5 points. 25
Self-Efficacy
Modified PROMIS General Self-Efficacy averages before and after group health coaching for Parkinson disease.
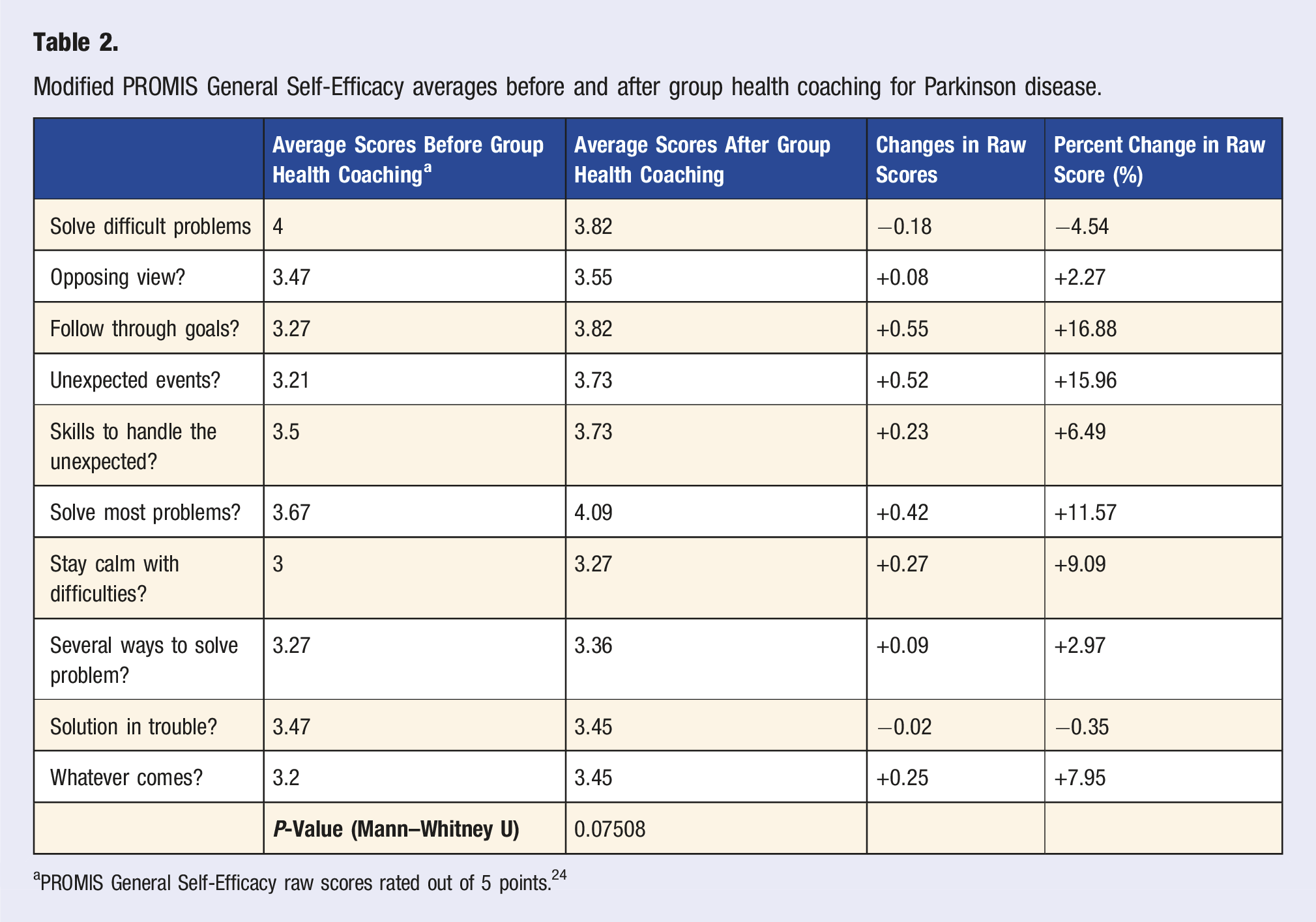
aPROMIS General Self-Efficacy raw scores rated out of 5 points. 24
Thematic analysis of qualitative feedback before and after group health coaching intervention.
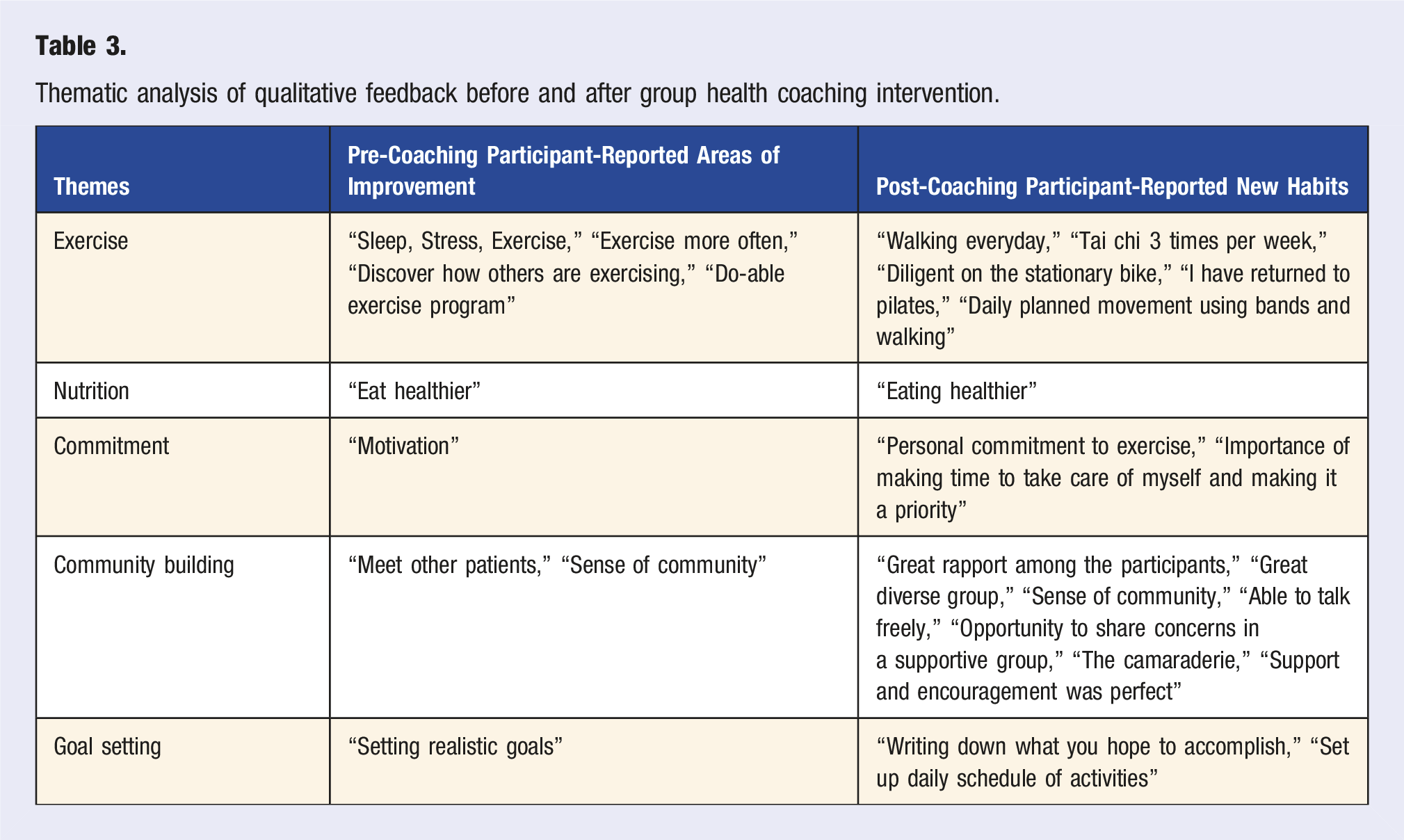
Thematic Analysis on Perceived Improvements After Group Health Coaching
After thorough thematic analysis, five categories were identified when participants were asked what they would like to accomplish and their perceived improvements, including “Exercise,” “Nutrition,” “Commitment,” “Community Building,” and “Goal Setting.” As depicted in Table 3, seven survey respondents indicated that their goals prior to group health coaching included exercising more and finding more effective ways to exercise. An additional three responses included goals of increasing motivation and setting realistic, attainable goals. Engaging with others and building a sense of community was also a prevalent goal with three responses focused on meeting and learning from others in the pre-group health coaching survey. In the post-group health coaching survey, eight respondents indicated that they had become more consistent with exercising and found modes of exercise that best fit their needs. When asked what participants enjoyed most about the group health coaching sessions, nine participants listed the supportive environment and the ability to learn from other people with PD. This benefit was observed even after the conclusion of group health coaching classes with one group opting to continue virtual meet-ups monthly.
Discussion
At the conclusion of this group health coaching course, average scores improved for both modified PROMIS General Self-Efficacy and Neuro-QoL Positive Affect and Well-Being. Using these five-point Likert scales, self-efficacy and well-being scores increased by a total average of 0.22 and 0.27 points, which translates to a 4.4% and 5.4% average point increase across all items, respectively.24,25 The results of this small study suggest the subjective effect of a semi-structured group health coaching curriculum for PD across multiple domains, including sense of well-being, self-efficacy, behavioral change, and social engagement. Moreover, these findings also indicate that a group health coaching program for PwP is both feasible and well-accepted as demonstrated by high participant engagement and the positive qualitative report. Thematic analysis underscored the potential benefits to commitments to exercise, sense of community, and development of healthier habits and goal setting. Both qualitative and quantitative data indicated that survey respondents found the sessions to be effective in aiding motivation and ability to troubleshoot challenges comfortably with the instructor and fellow participants. Beyond these data points, health coaching groups decided to continue with virtual, monthly group sessions independently, further signifying the advantages of the group setting.
While group motivational interviewing and health coaching demonstrates well-documented successes in other chronic diseases, this study evaluates the benefits of a group health coaching program for PwP as a novel and easy to implement strategy to improve well-being in PD.26,27 One scoping review highlighted the impact of group health coaching on adherence to exercise, reducing embarrassment, and improving physical symptoms, self-efficacy, and feeling of control over health and well-being in cancer survivorship.27,28 Furthermore, a qualitative study conducted in Norway explored the potential benefits of group-based exercise classes and impacts on motivation, finding encouragement and praise from fellow participants to be central to their success. 29
Similar to previous findings, our participants commented on their positive takeaways from the group experience, citing benefits such as encouragement, support, camaraderie, and the opportunity for candid conversation. Moreover, our participants adopted new healthy habits and engaged in behavioral change. Due to high rates of apathy, such changes can be challenging in the Parkinson’s disease population, often presenting a barrier to adhering to new lifestyle modifications. It is therefore noteworthy that our group health coaching participants were motivated to participate in and enact behavioral changes, such as an improved diet and regular exercise. Such an effect certainly warrants further study and speaks to the utility of a group health coaching intervention for this population.
Building on the Group Health and Wellness Coaching competencies, our group health coaching sessions emphasized the instructor–participant relationship, aided in the creation of actionable goals, and encouraged positive group dynamics. 30 In individual health coaching, having shared characteristics, earning trust, being available, providing personal support, and support in decision-making have been found to be central to the coach–patient relationship. 31 In this study, group health coaching participants highlighted how group dynamics contributed to these aspects. Participants expressed feelings of support and trust with their group members as well as their instructor with bonds further strengthened through having a shared diagnosis.
Careful consideration of the instructor role is an essential component in designing a group health coaching program. We strongly believe the positive outcomes cited by our participants were directly related to the informed guidance of the instructor. Certified health coaches are effective communicators trained in evidence-based behavior modification strategies that empower participants. 32 In addition, having experienced nursing knowledge of the disease profile of the group is crucial to the success of the instructor in providing evidence-based information and forming trustworthy connections with participants. Our instructor—a Parkinson nurse navigator and certified health and wellness coach—was therefore uniquely qualified to lead this group. This dual training presents another potential avenue of training to enhance longitudinal neurodegenerative care.
Limitations
While preliminary results suggest potential efficacy of group health coaching as a beneficial intervention for PwP, the sample size was not large enough to reach statistical significance. For this reason, non-parametric statistical analyses were used to determine significance. Due to this limited sample size, there was also a lack of diversity in demographic data, making the research less generalizable to certain groups, such as those with lower educational attainment. Participants were recruited from a single movement disorders center on a volunteer basis, and thus may represent a selection bias. Despite this, participants were able to find meaningful new therapeutic relationships in one another. We think this offers opportunity to explore if similar impact could be achieved on a larger scale broadening recruitment outside of a single center with a focus on community outreach.
Furthermore, survey data was not paired prior to and after the group health coaching intervention, making direct comparison more challenging. In addition, all data was survey-based without objective measurements. Based on these findings, further investigation is warranted to better define the impacts of this novel intervention. Future research with larger sample populations could introduce additional outcome measurements, potentially elucidating its clinical utility and significance.
Conclusions
Our novel group health coaching program was designed to meet the unique needs of PwP and empower them to take control of disease through thoughtful lifestyle modifications. As in individual health programs, coaching was initiated by a trained coach, however in this program was reinforced through a supportive group of peers. This preliminary data suggests that a group health coaching curriculum for PwP has potential to increase motivation, build a sense of community, and champion positive behavioral and lifestyle changes. After the group health coaching intervention, self-efficacy and sense of well-being improved across nearly all measures with qualitative data underscoring the positive impact of the group setting in enhancing motivation and providing support in enacting lifestyle modifications. Further research is needed to fully appreciate the potential clinical applicability of group health coaching as an intervention for lifestyle modifications in those with PD.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Parkinson’s Foundation; PF-CG-1281262.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.