
Abstract
Purpose: Advantages of fluoridated water, dental insurance, and greater awareness of preventive oral healthcare allow many adults in today’s aging cohort to maintain their teeth into their advanced years. The purpose of this study was to describe attitudes, expectations, knowledge, and intentions related to oral health issues from the experiences of older adults living independently in a largely rural south central state. Methods: A qualitative analysis guided by behavioral constructs of the Reasoned Action Approach was utilized to conduct semi-structured interviews of a purposeful sample of adults age 65 years and older living independently. Results: Participant data (N = 26) revealed 5 themes: difficulties accessing dental care; active coping; taking care of your mouth as part of overall health; interactions affecting oral health–related quality of life; and supporting roles. Overall, the intention to attain dental care was affected by the perceived need to prioritize many health issues over oral care. An overarching expectation to have affordable basic services available pervaded. Conclusion: The perceptions of participants reflect socioeconomic determinants that could be influenced through improved health literacy education focused on establishing a greater understanding of the oral systemic link especially as it relates to diabetes.
“I'm gonna hang on to these as long as I can”: Examining the perspectives and knowledge of oral health issues of older adults living independently attitudes, expectations, knowledge, and intentions related to oral health issues from the experiences of older adults living independently
Introduction
Oral health is vital to the health and quality of life of all adults, particularly older adults. Not only are individuals in this cohort living longer, but they are reaching old age with more of their natural teeth.1-4 The advantages of fluoridated water, dental insurance, greater awareness of preventive oral healthcare, and more restorative dental services make this possible. However, natural changes related to aging result in increased vulnerability to disease.
The demand for oral healthcare services will be greater and more complex than that of previous generations.5-7 Attaining preventive and restorative dental services and improving oral hygiene practices are modifiable behavioral factors allowing for healthier oral tissues, reduced inflammation, and, therefore, improved general health and quality of life. 8
Oral Disease Connected to Overall Health
Oral disease in the older adult is linked to numerous chronic diseases and comorbidities including periodontitis, diabetes, pneumonia, cardiovascular disease, and Alzheimers.9-12 International research using large cross-country databases has found poorer oral health to be predictive of poor general health. 13 Medications have increased life expectancy by improving the management of chronic diseases, yet many of these medications have adverse effects on oral tissues.7,14 Older adults are more likely than other age groups to take a combination of drugs. 15
Unequal Access
Over the past 50 years, complete tooth loss in the United States has decreased by greater than 50% for nonpoor individuals age 65–74 years, while those who are considered poor have experienced little improvements in their dental status over the same time period. 16 Inequalities in access to dental care among lower income older adults in the United States are reported, with cost being the most common reasons for not getting dental care. 17 The barriers most experienced by older adults and reported in the literature are related to lack of finances, transportation, and navigating dental services.18,19 A recent study of adult Medicaid beneficiaries in the state of Michigan 20 reflected perceptions of self-reported improved oral health resulting from the expansion of this optional dental coverage. These results show promise for improving oral health for low income older adults through Medicaid expansion.
Difficult Transitions
Currently, most dental coverage in the United States is obtained through employer benefit plans. When the older adult retires and transitions to Medicare, dental benefits are not included in their health coverage 21 and many older adults cannot afford dental care. 22 Data collected from the 2004–2006 Health Retirement Survey, sponsored by the National Institute on Aging, found the odds of seeing a dentist for those without dental insurance to be less than half when compared to those with dental insurance. 23 The impact of transitioning out of the workforce and maintaining routine dental services is a significant challenge for the older adult, yet trends in the United States indicate that the demand for dental care among seniors is increasing. 24
Health Literacy
Differences exist between oral health literacy and general health literacy. An adaptation of the definition of health literacy, the concept of oral health literacy is described as “the degree to which individuals have the capacity to obtain, process, and understand basic oral and craniofacial health information and services needed to make appropriate health decisions.” 25 A study correlating health literacy and oral health suggested higher levels of health literacy were found to be associated with better self-rated oral health. 26 A study of Canadian baby boomers concluded that the participants had adequate oral health literacy skills but insufficient knowledge of the oral systemic link. 27 Several research projects in the United States and Canada have investigated health literacy or oral health literacy in dental settings,26-29 but none could be found that examined oral health literacy in medical settings. The purpose of this qualitative study was to describe attitudes, expectations, knowledge, and intentions related to oral health issues from the perspective of older adults living in independent settings in the United States.
Methods
Design and Participant Selection
A qualitative analysis was used to learn about the specific insights of participants and how their experiences affect their likelihood of performing the behavior of seeking dental care and what it feels like to face oral care issues as they transition into greater levels of dependency. Approval from a university-based IRB was obtained. A purposive sample of older adults age 65 years and older (n = 26) was recruited, primarily through flyers and snowball techniques, at congregate meal sites (senior centers) and a federally funded senior housing facility in a largely rural south central state. Individuals from senior centers or their own homes were selected in order to reach a more independent target group at a time when oral health behaviors may be more modifiable. Initial recruitment was through 2 senior centers and resulted in 17 participants with an average age of 75 years. Attendance rates at community centers appear to have dropped nationwide especially among “younger” older adults, a phenomenon identified by a study of senior centers in Connecticut
30
and reflected in this interview process. In addition, approximately 50% of the initial interview participants of this study either had dental insurance or reported the ability pay out of pocket for dental care. To satisfy the goal of diversity in range of age and socioeconomic status, a targeted recruitment effort was subsequently extended to ages 65–70 years and a subsidized housing facility. A brief demographic questionnaire and in-person, one-on-one interviews were conducted on August 2018–January 2019. Saturation, the point at which no new information was being revealed, determined the final sample size.
31
A qualitative thematic analysis of semi-structured interviews was used for data analysis. Three questions guided the interviews: What do older adults/seniors age 65 years and older at senior centers know about the links between oral health and other health issues? What do older adults/seniors age 65 years and older at senior centers believe to be their future oral health concerns and needs as they age? How do older adults/seniors age 65 years and older at senior centers intend to manage their oral healthcare now and in the future?
Theory and the Interview Process
The constructs of the behavioral theory known as the Reasoned Action Approach (RAA) guided the creation of interview questions. This value expectancy theory integrates constructs of the Theory of Reasoned Action and the Theory of Planned Behavior by attempting to understand behavior from the unique perspective of the target population. 32 The RAA focuses on intention to perform recommended health practices. Theory constructs within the RAA connect self-efficacy to intention. Oral health–related quality of life and health literacy were also considered in the conceptual framework. A focus group (6 individuals from a senior center) was convened to pilot test interview questions. Feedback was used to revise the questions for clarity and to elicit free response more effectively. Individual in-person interviews were recorded and transcribed, verbatim, and averaged 31 minutes with a range of 19–60 minutes. Neither focus group participants nor interviewees received incentives for participation. Transcribed data were read and reread by the first author and compared to the audiotaped recordings, to ensure accuracy.
Analysis of Data
Thematic analysis as described by Braun and Clark 33 was used to review data for patterns of meaningful content related to the research questions. The first author completed the early phase of coding in which data were organized in an Excel document and interesting features highlighted and coded. Codes were collated into potential themes. Themes were examined to identify subthemes. The second and third authors examined the initial coding and thematic analysis to refine the specific features of each theme and subtheme. A second phase conducted by all 3 authors involved a selective process in which the specifics of each theme and subtheme were reviewed to generate definitions and names for each theme. Themes were refined, and discussion continued until consensus was achieved, to best capture the essence of the overall data set. Each segment of data was given an abbreviated code as a means of naming the data. The second and third author examined the initial coding adjusting until a consensus was agreed upon. A second phase conducted by all 3 authors involved a selective process in which the most significant, or frequent codes were sorted, integrated, and organized into categories, subthemes, and themes. Themes were refined and defined to best capture the essence of the data results.
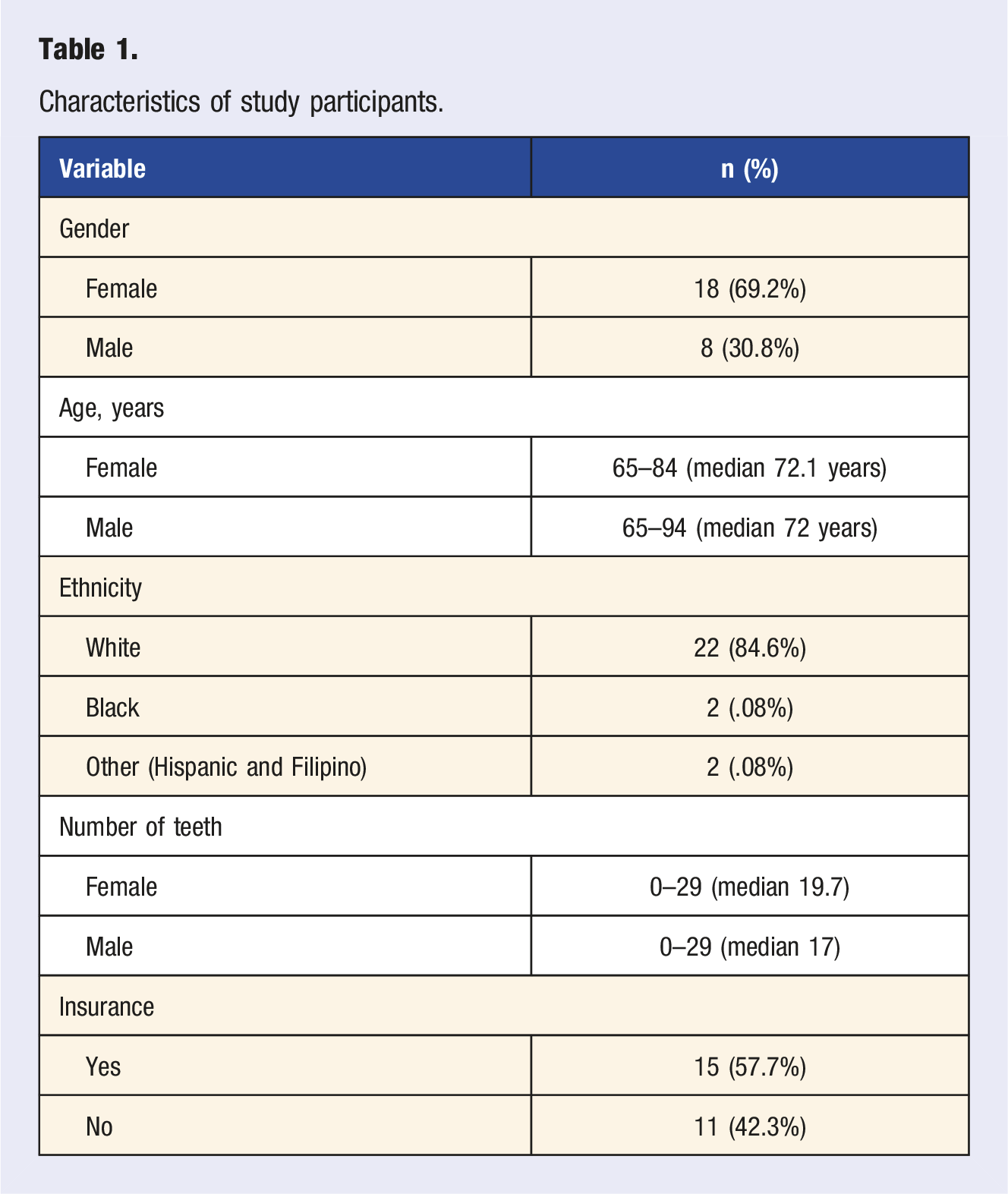
Characteristics of study participants.
Difficulties Accessing Dental Care
Participants reported lack of financial resources limited their ability to go to the dentist and receive preventive, restorative, or emergency dental care. Several described difficulties acquiring insurance when transitioning out of the workplace. “I’ve checked out a few that I’ve gotten in the mail… But a lot of them have limitations where they won’t do anything for two, three, up to five years if you’ve got an existing condition. And this would be considered an existing condition [pointing to broken/missing front teeth].” (Participant 24) “Well, as long as I was working, I would generally go every year. I stopped working 4 years ago, and I’ve only been once since.” (Participant 4)
Others described reaching a point in which such extensive work was needed that they could not afford to have necessary treatment, ultimately resulting in having all their teeth removed, or being forced to endure badly deteriorating dental conditions. “One day I woke up, probably not quite a year ago. I woke up and these 3 teeth they were in my mouth. Just broke [asked if she got them checked]. No, it cost a hundred dollars just to walk in a door, it really does. A lot of people have no idea of the things that are not available.” (Participant 25)
Transportation challenges were described by several participants. One participant described being charged for a missed dental appointment due to unreliable transportation issues. Others expressed frustration with having to depend upon friends, family, or public transportation. “I could call a friend, I can try, but that is not something I would say that I can count on.” (Participant 25)
Confusion and frustration with the healthcare system was evident. Some participants assumed that Medicare would pay for their dental care, while others were not sure if they had Medicare, or Medicaid, or both. Others described difficulties in understanding the terms of the policy or deciding what would be best for their individual circumstances. “I don’t think there’s a dental plan like all of us really need to be honest with you. It doesn’t cover—you’re limited on this, and this, and this. And you might need more of this. So, it’s going to be costly. It saves you some but you’re paying a monthly premium.” (Participant 8) “It’s so hard, everybody wants to do everything over the phone, and I’m a one-on-one person. When I’m on the phone, I can’t think of certain things I want to say, and then of course they want a lot of personal information that I don’t like giving over the phone.” (Participant 11)
When asked how they would manage a dental emergency a common response was “I don’t know.” Several participants indicated that dental care was given a low priority as financial concerns, family situations, or other health issues were given precedence. “Those decisions will very likely be money driven. … If I am 80 years old and broke—then I am not going to do much. If I am 80 years old and everything is going well then, I may have them [dentist] do everything.” (Participant 23) “Glasses, and dentistry, you know you don’t get that. And that’s really hard. Now I got my glasses every other year. I paid for ‘em. But the dentist I didn’t, I didn’t even go.… I would rather get my glasses than get my teeth fixed.” (Participant 26)
Active Coping
Many comments described coping strategies that reflected a degree of independence and resilience. “In other words, I don’t just get out there and call and asked someone to come here and help me do this or do that. I just never—I wasn’t raised up that way and I still don’t do that. I just kind of do what I can for myself.” (Participant 15) “I can eat softer foods. I can cook things a little bit longer.” (Participant 21) “I would probably go to Walmart and get me some Orajel and I would take some aspirin, or Tylenol, and heating pad and just tough it out until I could get over it.” (Participant 24)
Taking Care of Your Mouth as Part of Overall Health
When asked about the connection between oral health and the health of the body, heart disease was most frequently mentioned, with comments about poisons and infections spreading though the body. The negative effects of smoking and concerns related to proper nutrition were recognized. Approximately one-third of participants made remarks that indicated general lack of awareness. Several, who reported having diabetes, did not connect the disease with oral health issues. Others, in obvious need of dental care, as observed by broken or missing front teeth or self-reporting tooth problems, did not know of any connection. Some described a history of infections and extractions but could not explain why they lost teeth. “I’m a diabetic…I’ve had it six or seven years…so I don’t know if that has anything to do if your teeth or not.” (Participant 7) “I had some kind of infection around two teeth that was there for quite a while, and the dentist decided the teeth needed to come out…but I don’t know what the infection was about.” (Participant 10)
The importance of oral health education at an early age was recognized. The question of whether it is normal to lose teeth as you age resulted in a variety of responses. “yeah, I guess you’re gonna lose some teeth. That’s part of the deal. I’m gonna hang onto these as long as I can, but we’ll see how it happens. It’s happened to me, so it is normal.” (Participant 13) “I don’t think that’s normal; I think I may not be normal. I think of my wife as normal because she still has all her teeth.” (Participant 21)
Interactions Affecting Oral Health–Related Quality of Life
Related subthemes described how the interrelationship between several factors negatively impacted quality of life. For some, aesthetics was an important factor, both in terms of the state of natural teeth or regarding the wearing of dentures. “I was very ashamed when they (natural teeth) were broken and stuff--didn’t smile in pictures or anything like that.” (Participant 22) “All my friends know I have dentures so that doesn’t bother me, but people that don’t know, I’d rather they didn’t know, cause I always had a really good smile, that was the thing that I was proud of.” (Participant 6)
Some felt a deep sense of regret associated with the loss of teeth or having to live with deteriorating conditions. “I think it is ugly, I think it exhibits to other people that, perhaps, I am not a clean person, or I’m not careful, or concerned about my look, or something. I hate it! I don’t even like to look in the mirror.” (Participant 25)
Others reported feeling helpless or hopeless. At the intersection of this myriad of oral health factors was a sense of compromised quality of life. “There is a lot of people that have given up wearing their dentures…they got the cheap dentures, and they don’t fit anymore. And they’re painful, so, it’s easier just to change their diet.” (Participant 8)
Theme 5: Supporting Roles
Throughout the interviews, comments reflected varying degrees of social and practical support from family, friends, and professional resources. Most described not wanting to burden family members with their healthcare needs. “I don’t have any family here, but I really don’t think I anticipate family helping me because I’m not wanting to burden my family.” (Participant 3)
Friends were an important, but limited, source of support related to getting dental care. “I think the choice of friends would narrow about going to something like a dental appointment, which may take a long time. Instead of dropping me off at Walmart and coming back in 30 minutes and pick me up. It’s a little more of a commitment.” (Participant 25)
Those that had a regular dentist expressed appreciation and reliance on their care. “I actually called him on a Saturday one time. I woke up with a bad toothache and he had me come right into the office.” (Participant 11)
When asked to explain how the community should help, responses were conflicted. Most comments reflected the desire and expectation to have basic dental services available. “I think the insurance industry and Medicare and all these things need to catch up. It’s not like the old days, when people didn’t need their teeth after they were 45 or 50. A lot of them would die before they were 60.” (Participant 2)
Discussion
This study examined the attitudes, expectations, and knowledge of oral health issues of older adults living independently. Most previous studies looked at barriers and challenges to dental care in more dependent settings such as long-term care facilities. The experiences related through the interviews provide insight into the struggles these individuals face. Comments from study participants revealed access to care, active coping, taking care of your mouth as part of overall health, interactions affecting oral health–related quality of life, and supporting roles to affect their ability to manage the transition into greater levels of dependency.
Barriers to access to care are commonly known to be related to lack of finances. Study participants described health insurance to be crucial to accessing dental care. Not having dental insurance equated with not getting dental care for most. Transportation issues are a well-documented access to care concern.18,19 In this study, participants related that having transportation available was not enough. It was important to understand the challenges of having a dependable source of transportation that would ensure that they did not miss an appointment, and one flexible enough to allow for uncertain appointment lengths. One participant described using a paid transportation service but prioritized its use for medical appointments.
Actively coping strategies included subthemes related to stoic independence, resilience, and self-care remedies. A degree of proactive behavior was evident for those who had dental insurance and planned to keep it.
Taking care of your mouth as part of overall health provides insight into the importance of health literacy. Many participants lacked knowledge of the connection between oral diseases and common chronic diseases. This finding is consistent with a study of Canadian baby boomers which concluded that the participants had adequate oral health literacy skills but insufficient knowledge of the oral systemic link. 27 Few individuals in the current study conveyed knowledge of periodontal disease and oral cancer similar to findings of McQuistan et al in their study of patients 65 years or older, who were aware of basic dental disease and prevention but were unfamiliar with concepts related to these serious oral conditions. 34 Participants also revealed a lack of understanding of the pathological processes that occur within the oral cavity. Increased oral health literacy is associated with reducing cancellations and missed dental appointments, 35 making the value of the dentist patient relationship vital. The natural aging processes that transpire inside the tooth can reduce sensitivity, while the insidious nature of the caries process can lead to extensive deterioration before symptoms or obvious damage are apparent. The consequence of this pattern of deterioration as referenced in a Kentucky study of older adults was termed the “Dental Death Spiral” in which a cycle of disadvantage leads to cost prohibitive extensive dental restorative needs. 36
The greatest knowledge deficit among participants of this study was related to lack of understanding about the well-established bidirectional link between periodontal disease and diabetes. Only one participant, who indicated they had diabetes, reported an understanding of the importance of good home care and more frequent professional preventive care. This more frequent protocol is considered the standard of care among dentists and periodontists but is not routinely practiced. Supporting this finding is a study comparing the dental care practices of individuals with diabetes in which they were found to be less likely to have had preventive dental care compared to individuals without diabetes. 37 The results of the current study, combined with scientific evidence indicating the systemic connection of diabetes to oral health, and increasing prevalence of diabetes and prediabetes 38 further supports the need to include oral health education as part of diabetes prevention programs.
Perhaps part of the lack of oral health literacy is related to dentistry being set apart from medicine, resulting in decreased attention to oral health literacy. Facilitating better understanding of oral health and disease may lead to a greater understanding of overall health literacy and improvement of health outcomes. In a study correlating health literacy and oral health, higher levels of health literacy were found to be associated with better self-rated oral health and higher quality communication between patient and dentist. 26 This improved communication had a positive influence on health literacy. Every effort should be made to blend the practice of dentistry with the practice of medicine in educating and increasing overall health literacy, including oral health, particularly as people approach their senior years.
Interactions affecting oral health–related quality of life culminated from subthemes related to wearing dentures. Acceptable aesthetics and function reflected a sense of well-being. An underlying sense of ambivalence related to dentures being a solution to having tolerated years of pain, difficulty chewing, and embarrassment before resorting to complete tooth loss and replacement. A sense of helplessness was expressed by those who had extensive dental care needs.
A reliance on social networks as a means of support varied. A sense of isolation was expressed by many of the study participants. When asked who they could rely upon to get help with the care of their mouth, several stated that they might reach out to a family member if they had to. Many stated a reluctance to be a burden to friends or family.
While participants expected more from the current healthcare system, they did expect to share in the cost of dental care. A desire to have community resources that would provide a basic exam pervaded. One participant stated that it did not have to be a “Cadillac plan.” Those that had an established dentist expressed loyalty and confidence in their care. Those without dental insurance described difficulties finding a dentist that would work with them. Several said if an emergency came up, they would have to call around until they found a dentist that would allow for a payment plan or go to the emergency room.
When viewed through the lens of RAA theory, intention to control oral health status was strongly influenced by dental insurance availability (self-efficacy and policy), knowledge of the oral health-chronic disease link (lack of health literacy), and availability of external social support. Self-efficacy was most strongly linked to finances, which limited access to care due to lack of insurance or cost of care. Figure 1 serves as a visual reference of the conceptual constructs and influencing behaviors. Dental diseases are preventable and existing dental diseases treatable, especially in the early stages. The healthcare cost savings would benefit the older adult and the healthcare system. Reaching out to the independent living older adult population at a time when the risk factors of dental diseases are more modifiable is an important public health issue. The perceptions of the individuals interviewed reflected socioeconomic disparities that could be decreased through health literacy education. Public health efforts to improve the oral health of older adults should seek to increase access to care by increasing the availability of basic dental care services. All stakeholders should advocate for an evaluation of policies that would expand Medicare coverage for older adults and increase access to care. Theoretical construct pathways influencing intention and potential barriers to proactive oral health behaviors.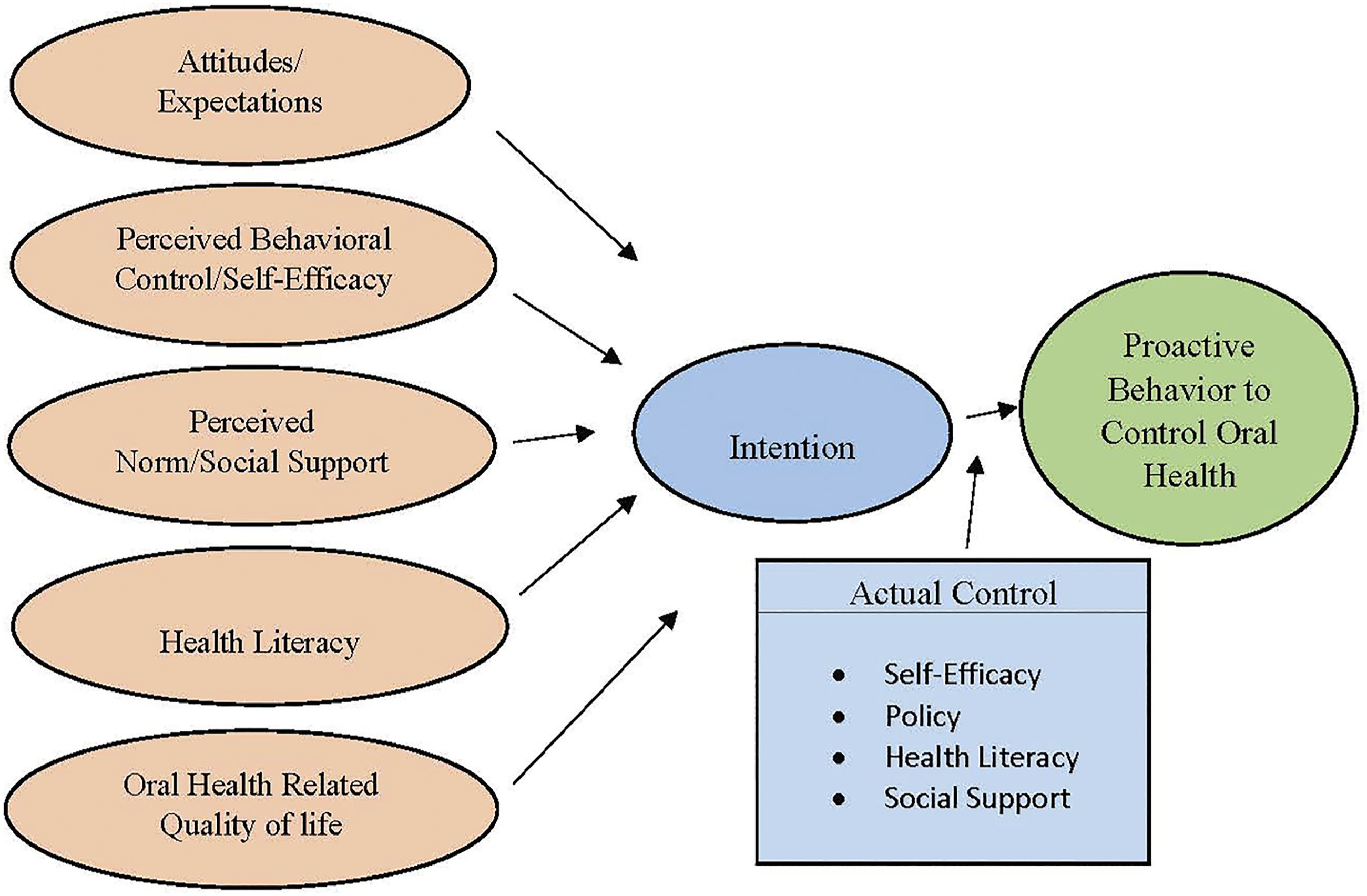
Limitations
The findings of this study are limited due to the purposeful and small sample size. The sample represents a small section of a largely rural South Central state; thus, findings may not be generalizable to the rest of the state or to the nation
Future Directions
Future research related to understanding the attitudes, expectations, and intentions of adults in middle age regarding oral care needs is recommended as a means of informing oral health promotion and emphasizing proactive behaviors at a younger age. Pilot studies with a focus on oral health literacy and providing support that would guide individuals through the complexities of the oral healthcare system are warranted.
Conclusion
Older adults present with different oral health needs and challenges than previous generations. Healthcare educators and professionals can benefit from understanding the perceptions of these senior members of society to best help them transition with dignity and greater quality of life as they age. This study revealed the need to increase oral health literacy as a way of improving overall health outcomes. Public health program planning can use the information learned in this study as a guide to help these individuals become more proactive and better prepared for the transitions that come with healthy aging.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.