
Abstract
Exercise during pregnancy is safe and beneficial; however, most pregnant women do not meet evidence-based exercise recommendations. Further, data on pregnant women’s physical activity are largely limited to women living in urban environments. Purpose. The purpose of this study is to examine beliefs and behaviors regarding exercise during pregnancy in pregnant and postpartum women living in rural communities. Methods. Surveys were distributed in healthcare settings and via social media to pregnant and postpartum (< 3 months) women living in rural communities. Results. Seventy-five women (28.1 ± 5.4 year) participated. Nearly all believed light (96%) and moderate (89%) intensity exercise are safe to perform during pregnancy, while fewer agreed vigorous intensity (52%) or resistance (40%) exercise is safe. Most (88%) believed women can continue their exercise regimen, and 73% believed that previously inactive women can begin training while pregnant. Only one-third of women met recommendations for cardiorespiratory exercise. The majority (66%) never engaged in vigorous exercise, and most (73%) did not participate in resistance exercise. Conclusion. Pregnant women in rural communities participate in light intensity exercise, but are largely not meeting guidelines for aerobic or resistance training. Knowledge related to safe exercises, particularly resistance training, during pregnancy is limited. Targeted education and programmatic planning are needed in this population regarding exercise guidelines.
Exercise Behaviors and Beliefs Among Pregnant Women in Rural Communities Pregnant women in rural communities participate in light intensity exercise, but are largely not meeting guidelines for aerobic or resistance training
Introduction
In the not-so-distant past, women were urged to cut down on or even avoid exercise altogether during pregnancy, as there was concern that maternal exercise could result in adverse health outcomes in the offspring, including malformation, growth restriction, hypoxia, spontaneous abortion, premature labor, and brain damage. 1 The scientific community has since established that for most women, the benefits of exercise during pregnancy far outweigh any potential risks. 2 Accordingly, the American College of Obstetrics and Gynecology (ACOG) recommends that healthy pregnant women exercise at a moderate intensity for ≥ 30 minutes on most, if not all, days of the week. 2 Despite this, evidence suggests that physical activity decreases with pregnancy in both healthy and high-risk women, 3 and only ∼15% of pregnant women exercise at the recommended level.4,5 Pregnancy is a unique life phase during which behavior modification may be quite successful,2,6 but it can also be a time of confusion and conservative practices when it comes to exercise. Furthermore, over 60% of physicians are not familiar with the current ACOG guidelines for exercise during pregnancy, 7 and practitioners rarely discuss physical activity with their pregnant patients. 8 Thus, while women have access to multiple sources of information regarding exercise during pregnancy, it appears that they find the topic to be confusing and lacking specificity.
Accordingly, pregnant women report mixed beliefs regarding the benefits and safety of physical activity during pregnancy. Women living in urban environments report a range of beliefs regarding exercise and physical activity during pregnancy. 9 The majority agree with statements reflecting the ACOG guidelines, the benefits of regular exercise, and the positive effects of physical activity on labor and delivery; however, nearly one-quarter believe women should not continue exercise during pregnancy. There was also a wide range of responses relating to appropriate exercise intensity and body positions during exercise across the trimesters. Differences in race/ethnicity, education, and regular exercise habits appear to explain some of the variances in physical activity beliefs.
Importantly, women living in rural settings may have access to vastly different sources of health information compared to city-dwellers. 10 Furthermore, they likely differ in socioeconomic status, education, and typical activity patterns, which may also impact their beliefs on benefits and risks of physical activity during pregnancy. For example, beliefs regarding the safety of physical activity during pregnancy have been found to be associated with education and income levels, 11 wherein those with lower education and income are more likely to feel that moderate physical activity during pregnancy is unsafe. Indeed, women living in rural areas of the southeastern United States tend to experience greater poverty, have more limited access to health care, and face the highest incidence of infant mortality and adverse maternal outcomes in the nation.12,13 Accordingly, ACOG has specifically noted the need to reduce urban–rural health disparities in pregnancy care. 14 While preliminary studies have indicated that pregnant women in rural communities may have limited knowledge on the risks and benefits of physical activity during pregnancy, 15 research is still largely lacking in this area. Thus, the purpose of this study was to conduct a comprehensive assessment of beliefs and self-reported behaviors regarding physical activity and exercise in pregnant women living in rural North Carolina.
Methods
Subjects
Pregnant and postpartum (< 3 months) women living in rural counties of Western North Carolina participated in this study. Women were recruited to participate via flyers posted at local healthcare clinics and community gathering places, as well as through social media posts and regional online forums. All subjects provided written (electronic) consent prior to participating, and protocols and procedures used in obtaining these data were approved by the Appalachian State University Institutional Review Board.
Survey Instrument
Participants were asked to complete a survey regarding their health behaviors, beliefs, and barriers, specifically related to physical activity (i.e., any physical movement resulting in energy expenditure) and exercise (i.e., planned, structured, goal-oriented physical activity) during pregnancy. Women were able to complete a hard-copy version of the survey (e.g., at the practitioner’s office/waiting room or home) or an online version via a secure Qualtrics web address. The survey was available in both English and Spanish languages. Data were collected from November 2018 through May 2020. The anonymous survey consisted of 69 questions, including demographics, and took approximately 20 minutes to complete; this also included questions regarding nutritional beliefs and behaviors that are not published in the current article. Survey questions were primarily Likert scale, rank order, and multiple choice/frequency. Physical activity and exercise questions fell into 3 major categories: (1) risks and benefits of exercise during pregnancy, (2) physical activity habits, and (3) barriers. Members and colleagues of the research team reviewed the questionnaire to establish face validity.
Questions on Demographics
Participants reported basic demographic (e.g., age, race, education, and relationship status) and current pregnancy (e.g., seeking prenatal care, planning breastfeeding, and weight change) information. Questions on pregnancy weight change and ideal weight gain were in a multiple choice format.
Questions on Risks and Benefits of Exercise During Pregnancy
These questions were adapted from previous investigations9,11,15 and designed to assess beliefs on risk associated with various types of exercise (e.g., light, moderate, vigorous, and physical contact) and beliefs on potential benefits (e.g., improved energy, labor and delivery, and baby health). Questions were phrased as statements (e.g., “During pregnancy, I believe it is safe to…”) to which respondents chose from 5 options: “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree.”
Questions on Physical Activity Habits
These questions were adapted from the Behavioral Risk Factor Surveillance System 16 and reported elsewhere 11 to assess current physical activity and exercise behaviors. Participants reported average frequencies, durations, and examples of physical activities engaged in within a typical week. Women reporting at least 150 minutes per week of moderate-to-vigorous intensity exercise over three or more days were classified as meeting recommendations for cardiorespiratory exercise, and women reporting engaging in resistance exercise two or more days per week were classified as meeting guidelines for muscle-strengthening exercises.
Questions on Barriers to Activity
This question was designed to assess beliefs on current barriers to being physically active during pregnancy. Participants ranked 5 items from a list of 16 previously reported physical activity barriers, 17 with additional open-ended response options provided.
Data Analysis
Data were analyzed using SPSS (SPSS Statistics for Windows, Version 26, Armonk, NY: IBM Corp 2019). Descriptive statistics were utilized to describe the women and their physical activity beliefs and habits. Pearson chi-square (χ2) correlation coefficients were utilized to determine relationships between categorical demographic parameters and ordinal responses on physical activity behaviors and beliefs questions. Barriers to activity were assessed as weighted rank scores, which were computed as the frequency of respondents multiplied by 5, 4, …, 1 (with 5 indicating the barrier was ranked as the top barrier). Statistical significance was determined when P ≤ .05.
Results
Participants
Subject characteristics.
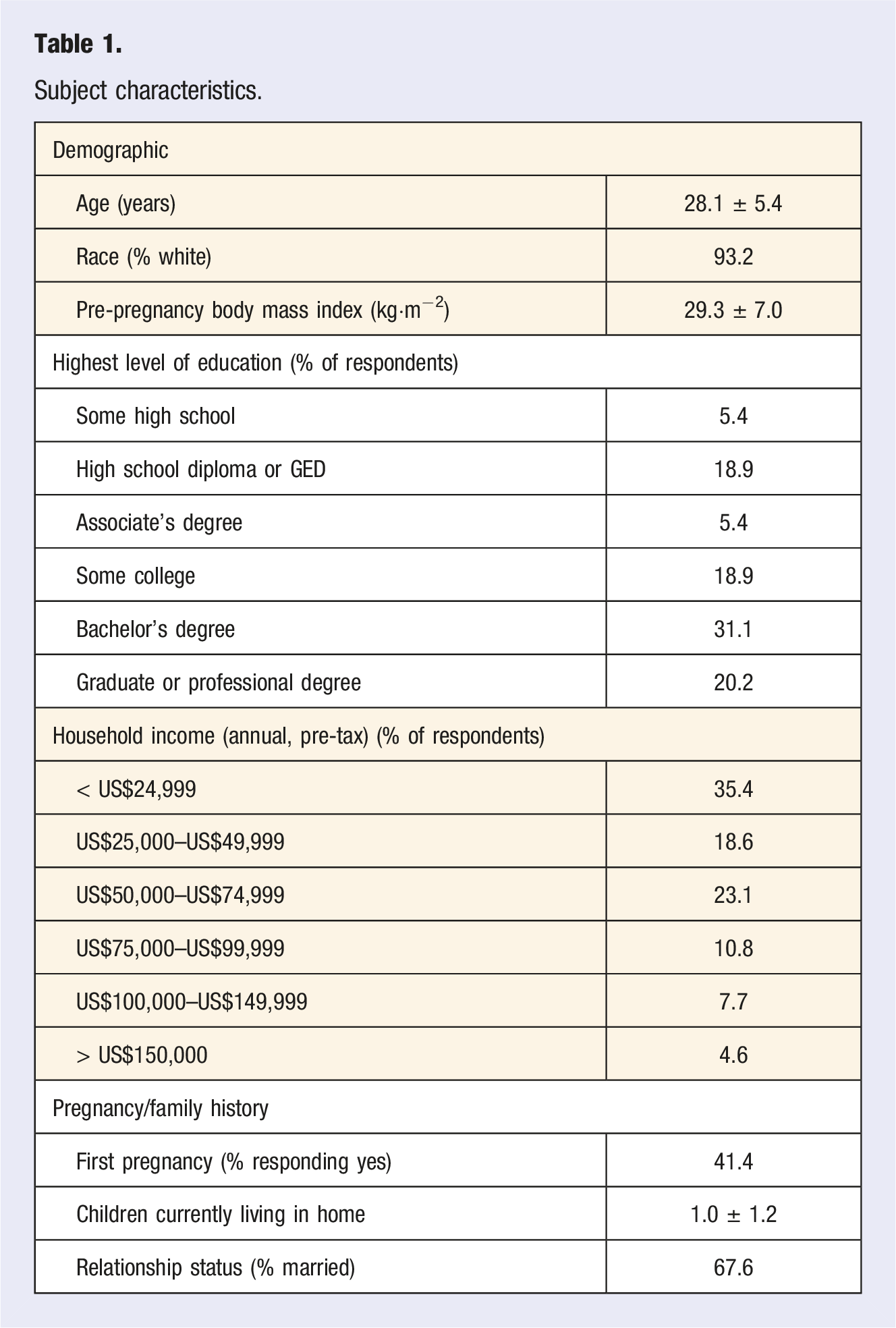
A relatively large proportion of respondents participated in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC; 40%), while 35% had Medicaid/Medicare, and 12% utilized SNAP/Food Stamps. Household income distribution is displayed in Table 1.
Nearly all women (97%) reported seeking prenatal care, and 86% planned to breastfeed.
Weight Gain
The majority of women (72%) felt their weight change during pregnancy was appropriate, while 20% reported gaining too much weight and 8%, too little. Women were knowledgeable on the ideal amount of weight gain during pregnancy (e.g., 15–25 lbs for overweight women, and 25–35 lbs for normal weight women); only 5% reported being unsure regarding optimal weight gain.
Physical Activity Safety and Benefits
Beliefs on the safety of various exercises are shown in Figure 1. Women believe that mild or light intensity exercise (96%) and moderate intensity exercise (89%) are safe to do during pregnancy. Fewer respondents reported feeling that vigorous intensity exercise (52%) and resistance exercise (40%) are safe during pregnancy. These responses reflect the reported beliefs that pregnant women will gain some benefit from mild (96%), moderate (64%), and vigorous (15%) exercise. Most women agreed that abdominal twisting or bending exercises (67%) and exercise with the potential for falling (91%) are not safe during pregnancy. However, approximately one in five reported being unsure about the safety of vigorous, resistance, and abdominal exercises. Beliefs on safety were not related to any demographic parameters. Reported beliefs of respondents (n = 56) on the safety of 9 various types of exercise. Subjects chose Likert scale options from Strongly Disagree to Strongly Agree when presented with a question phrased similarly to “(Blank) exercise is safe for pregnant women to perform.” Percentage of respondents reporting each answer option is displayed.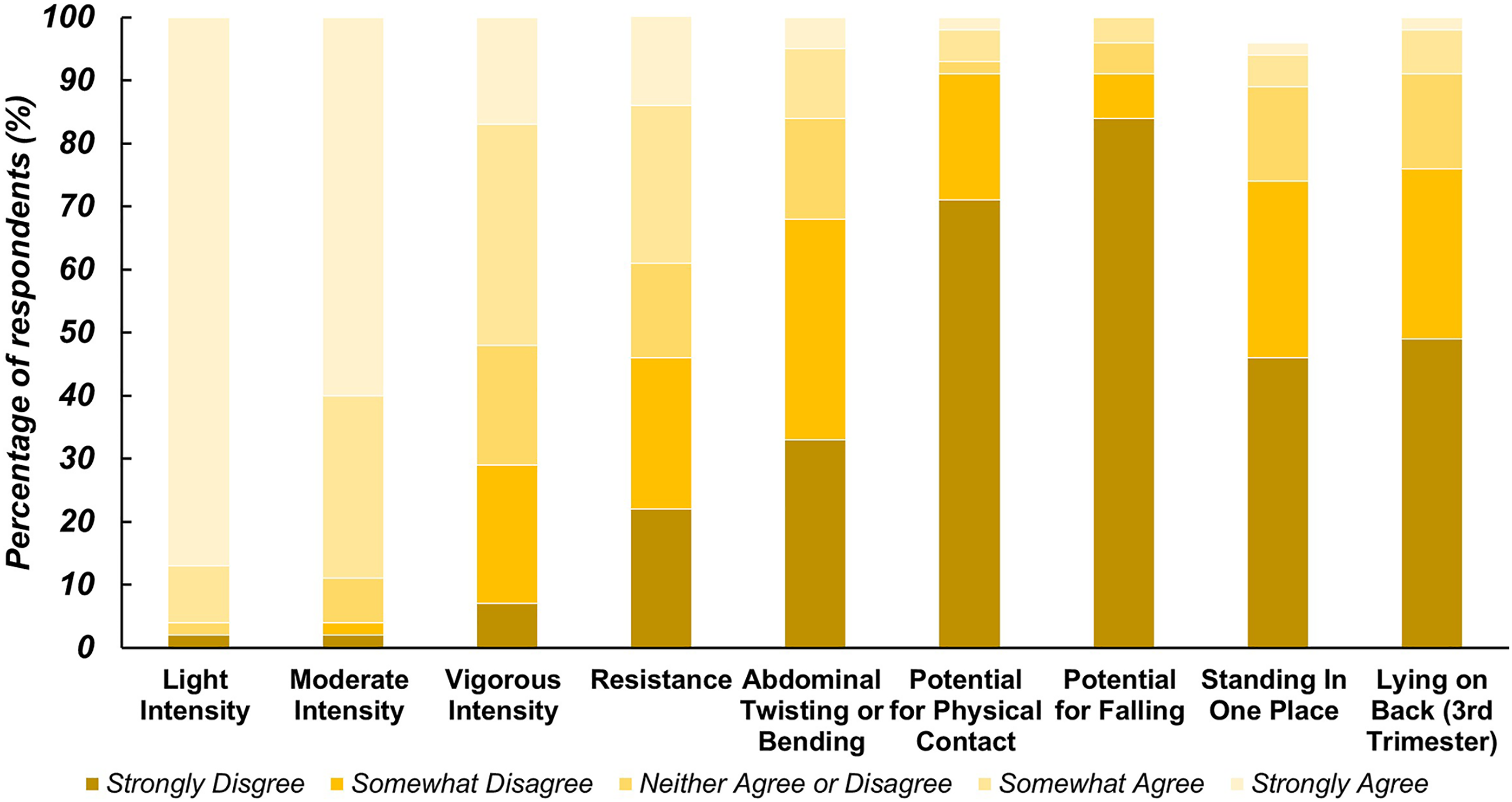
Most (88%) agree that women can continue their regular exercise during pregnancy, and 73% believe women who were not physically active before pregnancy can begin an exercise program during pregnancy. In contrast, only 30% agree with the statement that a pregnant woman can exercise even if she becomes tired/exhausted. Many women recognize the need to avoid exercise while lying on their back during the second (58%) and third (68%) trimesters, though 15% also think these exercises should be avoided during the first trimester.
Respondents believe that physical activity and exercise during pregnancy will increase energy levels (81%), improve labor and delivery (78%), and improve the health of the baby (70%). They do not believe that physical activity and exercise will result in lower weight babies (only 6% agree with this statement).
Current Physical Activity
Current physical activity levels are displayed in Figure 2. Approximately two-thirds of women (47 respondents) reported being physically active. Of those who were physically active, most reported beginning physical activity as early as the first trimester of pregnancy, with 6 women beginning in the second trimester, and one in the third. Half of the women reported participating in moderate intensity exercise ≥ 3 days per week. However, the majority (66%) of pregnant women do not ever engage in vigorous exercise, and most (73%) do not participate in resistance exercise. Based on reported minutes per week of various activities, 33% of women met the ACSM recommendations for cardiorespiratory exercise, while 12% met the ACSM recommendations for muscular fitness training. There was a significant relationship between education level and meeting cardiorespiratory exercise guidelines (X2 = 22.026, P = .001), largely driven by the finding that 10/13 (77%) of women with a graduate or professional degree did meet the recommendations. There was also a significant relationship between achieving recommended aerobic activity levels and children in the home (X2 = 8.411, P = .038), with women caring for 1 child more likely to meet guidelines than those with 0, 2, or 3 (64% vs. 23%, 18%, and 33%, respectively). Reported beliefs of respondents (n = 55) on the benefits of physical activity during pregnancy. Subjects chose Likert scale options from Strongly Disagree to Strongly Agree when presented with these statements. Percentage of respondents reporting each answer option is displayed.
Barriers to Physical Activity
The primary reported barrier to physical activity during pregnancy was a lack of time (weighted rank = 166), followed by being too tired (117), lack of motivation (88), and bad weather (76). Women also reported barriers toward meeting their overall healthcare needs, and approximately one-quarter of respondents listed lack of child care and demanding work hours as major obstacles. The ranking of barriers was largely not related to any sociodemographic parameters (e.g., age, income, and children) or exercise levels (i.e., meeting guidelines); however, ranking lack of time as a top-tier barrier (i.e., ranked #1 or 2) was associated with education level (X 2 = 11.638, P = .040). Women with some high school (0% rated as top-tier barrier), some college (43%), or a bachelor’s degree (30%) tended to be less likely to rate lack of time as a top barrier compared with women with a high school diploma or GED (57%), associate’s degree (75%), or graduate or professional degree (60%). Ranking bad weather as a top-tier barrier was also associated with education level (X 2 = 18.633, P = .002). Most women with a graduate or professional degree (78%) rated bad weather as a top-tier barrier, whereas very few women with some high school (0%), a high school diploma or GED (25%), an associate’s degree (33%), some college (0%), or a bachelor’s degree (8%) ranked it as such.
Discussion
The primary findings of the current study are that pregnant women in rural Appalachian (United States) communities are (1) relatively knowledgeable on optimal weight gain and general benefits of physical activity during pregnancy, (2) not well-informed regarding benefits of vigorous aerobic and strengthening exercises during pregnancy, (3) unsure and/or unaware about the safety of certain activities, (4) moderately physically active, and (5) experiencing common barriers to physical activity.
The first official guidelines on exercise during pregnancy were published by ACOG in 1985; early recommendations were based on little scientific evidence and included such suggestions as keeping heart rate below 140 bpm and limiting strenuous activity to < 15 minutes. 18 Subsequently, research has indicated that exercise during pregnancy is not only safe but can reduce common complaints of pregnancy (e.g., low back pain, leg pain, and urinary incontinence) 19 and incidence of excessive gestational weight gain, 20 diabetes and preeclampsia, 21 while improving labor and delivery 22 and, potentially, long-term offspring health. 23 Like pregnant women living in urban and suburban areas of the US South, participants in the current study largely recognize many of the benefits of being physically active during pregnancy, though to a slightly lower degree for some statements (e.g., agreement that exercise improves labor and delivery—94%9,24 vs. 78%). Women cited primary care physicians and obstetricians as their primary sources of information when making choices about nutrition (unpublished data), and it is likely that they similarly rely on healthcare providers for information about exercise during pregnancy. Previous research indicates that physicians encourage pregnant women to be physically active, but that they are less apt to know the latest ACOG guidelines and/or provide any assistance in developing an exercise program. 24 Nearly all women in the current study were seeking prenatal care. While in some countries there is a substantial difference in rates of prenatal care among women living in rural and urban locations25,26, in the United States, research indicates that residence category is not necessarily associated with late initiation of prenatal care or views on the importance of prenatal care,27-29 though other studies have found that US women in rural locations have higher rates of inadequate prenatal care.30,31 It is likely that proximity to a large university, despite its rural location, impacted our participants’ attributes (e.g., socioeconomic status and education) and healthcare access.
Physical Activity Safety and Benefits
Compared with beliefs on light-to-moderate intensity exercise, women were less likely to consider vigorous aerobic exercise and strength training as either safe or beneficial. Vigorous exercise is not associated with adverse maternal or fetal outcomes32-34 and, in fact, may lower rates of gestational weight gain in women who develop gestational diabetes 35 and improve physical fitness. 36 However, as the impact of vigorous exercise in women who were previously inactive is not fully elucidated, sedentary women are not advised to begin vigorous exercise during pregnancy out of an abundance of caution. 37 Regardless, a recent meta-analysis of 10 cohort studies and 5 randomized control trials indicated that vigorous aerobic exercise in the third trimester appears to be safe for most healthy pregnancies. 38 Only half of our respondents agreed that vigorous exercise was safe to perform during pregnancy, and just 15% believed vigorous exercise during pregnancy provided benefits. These findings are again quite similar to a comparable survey provided to pregnant women living in more urban areas, in which 13% believed vigorous exercise during pregnancy provided benefits. 9 Exercise guidelines for pregnant women, while extremely clear on the safety, efficacy, and benefits of moderate intensity exercise, are less clear when it comes to vigorous exercise. This lack of clarity in the scientific literature is reflected in the varying beliefs of pregnant women.
Similarly, light- and moderate‐to‐vigorous intensity resistance exercise does not result in adverse maternal or fetal health outcomes39-41 and is particularly beneficial in women with gestational diabetes, reducing their need for exogenous insulin. 42 Furthermore, resistance training acutely reduces feelings of mental and physical fatigue in pregnant women while increasing energy. 43 Results of a review of 61 randomized control trials provide strong evidence for the effect of a combined aerobic and resistance training regimen for improving maternal cardiorespiratory fitness and preventing urinary incontinence. 44 Despite clear evidence of benefits from muscle-strengthening exercise and no adverse effects, only 12% of women in the current study met guidelines, and just 40% agreed that resistance exercise was safe. Many activities that are not recommended during pregnancy (e.g., standing for long periods, lying on the back, and holding breath) are characteristic of typical muscle-strengthening exercises. Further, while abdominal strengthening exercises are distinctly recommended in physical activity guidelines for pregnancy, the majority of women (67%) believe these activities are unsafe. It is possible that women conflate known (and anecdotal) activities that are discouraged during pregnancy with strength training. On the other hand, research consistently indicates that a smaller proportion of the population (10–30%) meet muscle-strengthening exercise guidelines 45 than cardiorespiratory exercise, and thus, the low percentage of our pregnant population meeting these recommendations may simply reflect general population trends. Healthcare providers are uniquely positioned to provide information on the specific benefits and safety considerations of resistance training during pregnancy; however, many practitioners lack the necessary knowledge and training, themselves, to provide specific exercise advice. 8 Encouraging physicians to consider referring pregnant patients to certified exercise professionals for supervised exercise training programs may help to overcome this challenge.
Current Physical Activity and Barriers to Exercise
Based on our findings, pregnant women in southern Appalachia are participating in light intensity exercise, but are largely not meeting ACSM guidelines for cardiorespiratory or muscular fitness exercise. Only 33% of our respondents meet the frequency, intensity, time, and type guidelines for cardiorespiratory exercise, while just 12% met guidelines for strengthening exercises (only 8% met both cardiorespiratory and strength recommendations). The prevalence of women in the current study achieving the recommended level of cardiorespiratory exercise does appear to be greater than previously reported values in pregnant women (i.e., ∼13% to 45%, depending on operationalization5,46), but similar to or slightly lower than estimates in the general population of women.47-49 Approximately one in five (19%) women in North Carolina meet both aerobic and muscle-strengthening federal guidelines according to a recent report by the centers for disease control and prevention; this percentage is similar to the reported average for all women nationwide (18.7%) 49 ; the 8% of our pregnant participants meeting both these guidelines is substantially lower than the general population of North Carolinian women.
Engagement in physical activity depends on a number of determinants, including personal attributes (e.g., knowledge, attitudes, health, and demographics) and environmental factors (e.g., access), 50 as well as the relationship between perceived benefits and barriers. 51 Indeed, rural women’s physical activity behavior is positively associated with physical activity knowledge, yet physical activity behavior remains significantly lower than knowledge. 52 While recent work indicates that inactive and active (non-pregnant) women in rural Midwestern US communities report the same top barriers to physical activity (i.e., motivation, fatigue, and weather), inactive women find these barriers to be more problematic; whether this is due to objective and/or perceptual differences in the magnitude of the barrier is unclear. 53 Interestingly, lack of time—the fourth-highest–-rated barrier in the aforementioned study—was one of only four (out of 22) barriers not impacted by physical activity status. Our pregnant participants’ top perceived barriers were similar to those recently reported by rural Midwestern women—lack of time, followed by fatigue, low motivation, and bad weather. This is consistent with earlier qualitative research in rural pregnant women indicating symptoms of pregnancy (e.g., fatigue), time constraints (e.g., other family/work responsibilities), and personal motivation are common barriers to physical activity. 17 While education level may play a role in the determination of some barriers to exercise in rural pregnant women—namely, time constraints and perception of weather as a barrier—certainly, more targeted research in this area is warranted.
Research indicates that motivation/intent, more so than other perceived barriers, most strongly influences pregnant women’s participation in exercise. 54 Motivation may be driven, at least in part, by knowledge of the subsequent benefits for mother and baby; perhaps consistent with this idea, we found a significant relationship between education and meeting guidelines among pregnant women in our study. However, educational achievement in the current study was not specifically related to lack of motivation as a barrier to activity. Pregnancy is a unique time period in a woman’s life in which frequent visits with a physician occur, and thus, encouragement and assistance by healthcare professionals to develop an exercise program (or referral to an exercise professional), in conjunction with providing information about major benefits, will likely have a positive influence on women’s exercise intention and adherence during pregnancy.
Of note, the current study is limited by a relatively small sample size and a largely homogenous (e.g., Caucasian, educated, and married) sample that may not be reflective of rural communities throughout the United States. Thus, caution should be applied in generalizing these results to the larger population of rural pregnant women.
Conclusion
Pregnant women in rural southeastern American communities self-report being physically active and are participating in light intensity exercise, but are largely not meeting ACOG recommendations for aerobic or resistance training. These women are generally knowledgeable on optimal weight gain, the safety of light and moderate intensity aerobic exercise during pregnancy, and benefits of physical activity during pregnancy, but knowledge related to safe exercises, particularly resistance training, during pregnancy is limited. Targeted education and programmatic planning are needed in this population regarding exercise guidelines for pregnant women, including examples of safe aerobic and resistance exercises.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the Appalachian State University Office of Student Research.
Ethical Approval
Reference to approval by the Institutional Review Board is in the methods section.
Data Availability Statement
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data are not available.