
Abstract
“Descriptive analysis revealed that over 84% of participants met the World Health Organization’s minimum weekly physical activity recommendation.”
Introduction
The perinatal period is associated with an increased risk of relapse of pre-existing mental disorders and the onset of new psychiatric conditions.1,2 Moreover, mental illness during pregnancy is linked to obstetric and neonatal complications, such as an increased risk of preeclampsia, 3 preterm birth, 4 and negative impacts on fetal life and child development. 5
Despite advancements in the field, it remains concerning that fewer than 25% of women with psychiatric disorders receive adequate mental health care during pregnancy. 6 Several factors contribute to this gap, including the stigma surrounding mental illness in this period, barriers to accessing specialized services, and concerns regarding the use of psychotropic medications—whose risks and benefits must be carefully assessed on an individual basis. 7 Given this context, it is essential to broaden the range of care strategies by incorporating complementary approaches that can support both prevention and treatment, while considering the specific characteristics of the perinatal period.
Engagement in physical activity (PA) has been associated with a reduced risk of developing certain mental disorders such as depression and anxiety, both in the general population and among pregnant women. 8 PA can occur across different domains, including leisure, work (or school), transportation, and domestic tasks. 9 As the motivations for engaging in PA likely differ across these domains, the outcomes in terms of mental health or quality of life may also vary.10,11 According to the most recent meta-analysis on the subject, in the general population, leisure-time PA was associated with positive mental health outcomes, whereas occupational and domestic PA were linked to an increased risk of negative mental health outcomes. 12
However, domain-specific patterns of PA among pregnant women with mental disorders—especially in contexts of social and emotional vulnerability—remain poorly studied. Most research focuses on total weekly PA volume, 8 without considering the context in which it occurs, which may significantly influence its effects. The lack of specific data on this population is partly due to methodological challenges but also reflects a historical neglect in the field of perinatal mental health research.
Therefore, given the scarcity of literature addressing domain-specific PA in pregnant women with psychiatric disorders, this study aimed to identify the most commonly practiced PA domains among these women and to evaluate their possible associations with the severity of psychiatric disorders and with clinical obstetric outcomes.
Methods
Study Design
This is a cross-sectional, descriptive, and analytical study conducted as a subanalysis of a larger project entitled “Outcomes and Biopsychosocial Determinants of Psychiatric Hospitalizations During Pregnancy,” whose research protocol was previously published (Alves et al, 2023). This specific segment represents a focused analysis on physical activity behavior among pregnant women diagnosed with psychiatric disorders.
Sampling
A convenience sampling method was used. Recruitment took place at the Hospital Materno Infantil Presidente Vargas (HMIPV), between June 2022 and December 2024, across three clinical settings: psychiatric inpatient unit, high-risk prenatal care, and maternal-infant ward. HMIPV is a public reference hospital serving pregnant women in clinical and social vulnerability in the state of Rio Grande do Sul, Brazil, with a longstanding history of supporting women experiencing psychological distress. This institutional context directly influenced the profile of participants, most of whom faced multiple layers of vulnerability.
Eligibility Criteria
Inclusion criteria were pregnant or postpartum women aged 18–50 years with a confirmed psychiatric diagnosis during pregnancy. Exclusion criteria included severe psychotic conditions or intellectual disability that compromised the individual’s ability to provide informed and reliable responses during data collection.
Study Logistics and Data Collection
Recruitment
All eligible women were invited to participate by a trained member of the research team, who explained the study objectives and obtained written informed consent. Women admitted to the psychiatric unit were assessed 48 hours after hospitalization. Outpatients were interviewed during scheduled prenatal visits. For postpartum participants, interviews were conducted during the recovery period after delivery.
Interview Process
Participants were interviewed using a standardized questionnaire administered by trained researchers. The assessment tools included.
Sociodemographic Questionnaire
This collected data on sex, age, race, marital status, education level, and average monthly income.
Assessment of Physical Activity and Domains
Physical activity during pregnancy was measured using the Pregnancy Physical Activity Questionnaire (PPAQ), a 36-item self-report instrument widely used in maternal health research across various countries (Chasan-Taber et al, 2004; Silva et al, 2015). It assesses the duration, frequency, and intensity of physical activity across four domains: household, occupational, transportation, and leisure.
In this study, the PPAQ was administered in person by trained interviewers who provided clarification as needed. For analysis, only moderate-to-vigorous intensity activities were considered, in accordance with World Health Organization recommendations advocating at least 150 minutes per week at this intensity to promote health. This threshold was used to categorize variables and interpret results, aligned with methodologies from previous studies (Yu et al, 2025).
Assessment of Psychiatric Diagnoses
Psychiatric diagnoses were established using the Structured Clinical Interview for DSM-5 Disorders - Clinical Version (SCID-5-CV), applied by a psychiatrist or trained psychiatry resident. Diagnoses included major depressive disorder, bipolar disorder, schizophrenia and other psychotic disorders, substance use disorders, and post-traumatic stress disorder (First et al, 2017).
Assessment of Psychiatric Severity
The Clinical Global Impression (CGI) scale was used to evaluate overall severity of psychiatric conditions, regardless of specific diagnosis. The CGI ranges from 1 (normal, not at all ill) to 7 (among the most extremely ill patients) (Guy, 1976). The scale was previously validated for use in Brazil (Lima et al, 2007).
Assessment of Obstetric Outcomes
Obstetric complications included gestational hypertension, preeclampsia, eclampsia, antepartum hemorrhage, cervical insufficiency, oligohydramnios or polyhydramnios, intrauterine growth restriction, gestational diabetes, and premature rupture of membranes. These outcomes were primarily extracted from medical records. For births occurring outside HMIPV, data were obtained via telephone interviews conducted within 30 days postpartum. For the statistical analyses, these variables were grouped into three categories: hypertensive disorders of pregnancy (including preeclampsia and eclampsia), gestational diabetes, and any obstetric complication (indicating the presence of any of the collected complications other than hypertensive disorders of pregnancy or gestational diabetes).”
Data Analysis
Data were summarized using absolute and relative frequencies. Descriptive variables were presented as medians, minimums, maximums, and interquartile ranges due to nonnormal distribution verified by the Shapiro-Wilk test. Differences in PA time across domains were assessed using the Friedman test. Associations between PA domains and obstetric complications were examined using the Mann–Whitney U test (for continuous data) and chi-square test (for categorical data). Spearman’s correlation was used to assess the relationship between CGI severity scores and PA time in each domain. Analyses were conducted using SPSS version 25, with statistical significance set at P < 0.05.
Ethical Considerations
This study complied with the principles of the Declaration of Helsinki and was approved by the Ethics Committees of HMIPV and UNISINOS (approval number 5.205.194). Written informed consent was obtained from all participants whenever possible. In cases where psychiatric symptoms temporarily impaired the participant’s ability to provide consent, a legal representative was asked to sign the consent form on their behalf.
During data collection, researchers had access to personally identifiable information. However, each participant was assigned a unique identification number when completing the research form, ensuring that only the lead investigators could match participants to their data. The final dataset contained no identifying information beyond these codes.
Results
Sociodemographic and Psychosocial Characteristics of the Sample (n = 64).
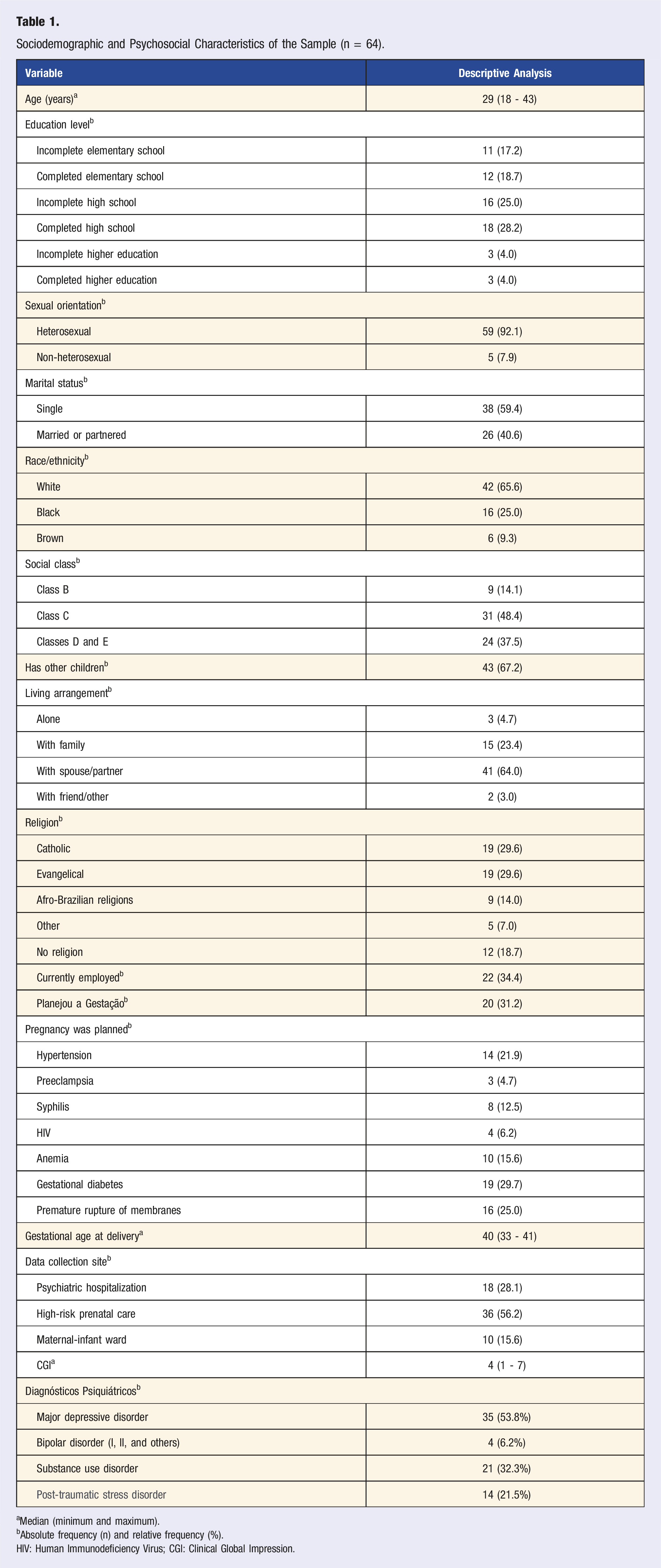
aMedian (minimum and maximum).
bAbsolute frequency (n) and relative frequency (%).
HIV: Human Immunodeficiency Virus; CGI: Clinical Global Impression.
Weekly Time Spent in Moderate-to-Vigorous Physical Activity by Domain.
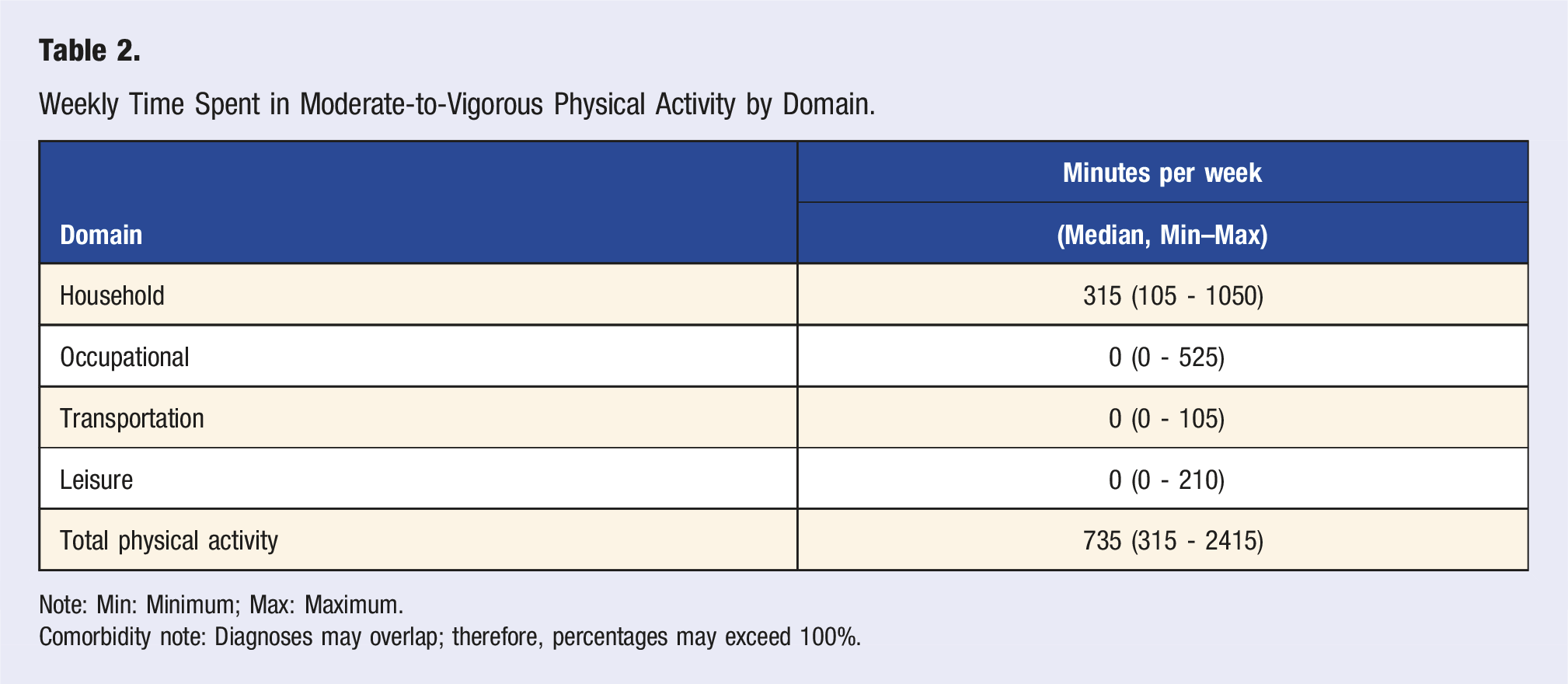
Note: Min: Minimum; Max: Maximum.
Comorbidity note: Diagnoses may overlap; therefore, percentages may exceed 100%.
Associations Between Physical Activity Domains and Clinical Outcomes During Pregnancy.
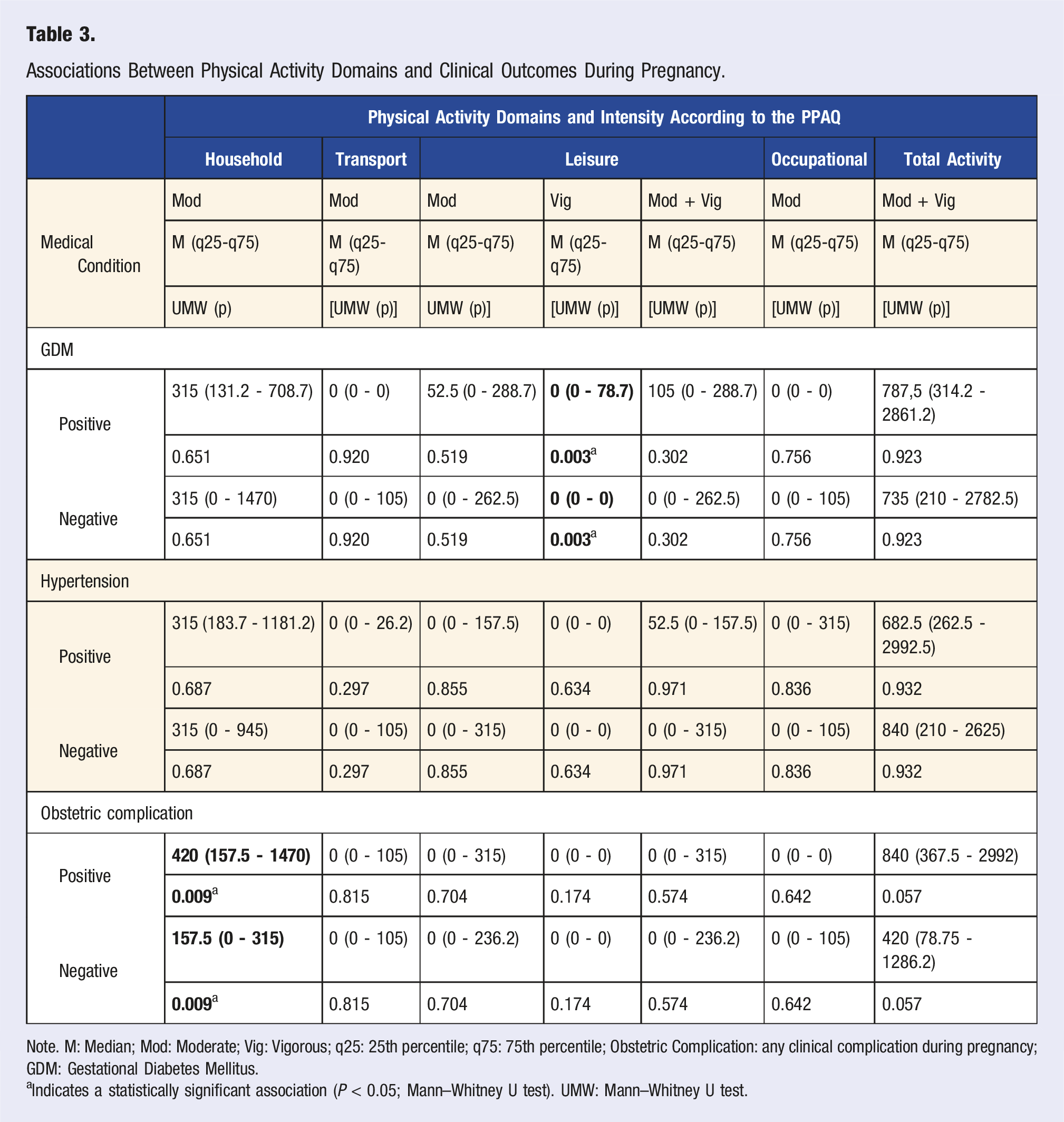
Note. M: Median; Mod: Moderate; Vig: Vigorous; q25: 25th percentile; q75: 75th percentile; Obstetric Complication: any clinical complication during pregnancy; GDM: Gestational Diabetes Mellitus.
a Indicates a statistically significant association (P < 0.05; Mann–Whitney U test). UMW: Mann–Whitney U test.
In the leisure domain, a statistically significant association was found between vigorous physical activity and the diagnosis of gestational diabetes mellitus (P = 0.003). However, it is important to note that the median number of minutes in this domain remained zero for both those with and without the diagnosis, suggesting that the association was driven by the presence or absence of any physical activity rather than the volume performed. Among the women diagnosed with gestational diabetes mellitus, four engaged in vigorous physical activity. Of these, three reported an estimated 105 minutes per week of vigorous activity, and one reported 315 minutes per week of vigorous activity. In contrast, none of the women without gestational diabetes mellitus reported engaging in vigorous physical activity.
Correlation Between CGI and Moderate-to-Vigorous Physical Activity Domains.
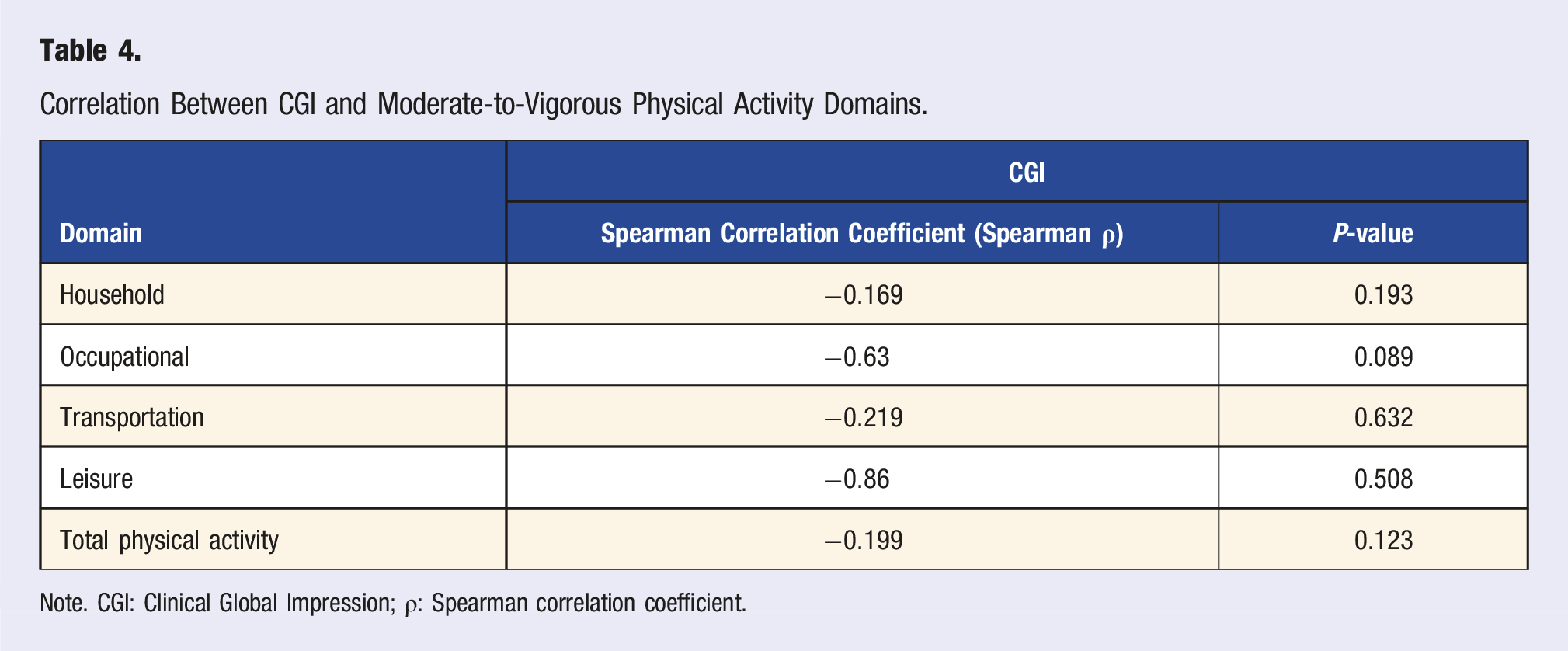
Note. CGI: Clinical Global Impression; ρ: Spearman correlation coefficient.
Discussion
Descriptive analysis revealed that over 84% of participants met the World Health Organization’s minimum weekly physical activity recommendation. However, this activity was highly concentrated in the household domain (median of 315 minutes per week), while leisure, transportation, and occupational domains showed median values of zero. This pattern suggests that physical activity occurred predominantly in functionally obligatory contexts rather than for leisure or health promotion. According to Self-Determination Theory by Deci and Ryan, 13 behaviors driven by external pressures tend to be associated with lower satisfaction and fewer psychological benefits, potentially limiting the positive effects of physical activity on mental health, 14 and in some cases, even contributing to negative outcomes when perceived as burdensome or stressful. 12
Current literature consistently shows that women of lower socioeconomic status tend to engage in physical activity primarily within the domestic domain, whereas those with higher income and education levels have greater access to leisure-related activity.15,16 Our findings align with this pattern, highlighting the unequal distribution of physical activity domains among pregnant women. Previous studies have shown that even when pregnant women meet recommended levels of physical activity, their engagement tends to be limited to low-intensity or caregiving-related activities, with limited participation in leisure or transportation contexts.17,18 One such Brazilian study, 18 found that increases in leisure-time physical activity during pregnancy were restricted to women with higher education and income. In our sample, the predominance of the household domain and limited activity in other domains reflect a context of social inequality and constrained choice, where physical activity is often linked more to functional burden than to health promotion. 19
Regarding associations, one key finding was the link between higher levels of household physical activity and the presence of obstetric complications. Women with such complications reported a median of 420 minutes per week in this domain, compared to 157.5 minutes among those without complications. This finding raises a relevant hypothesis: in contexts with limited support networks, the burden of domestic labor may pose an additional risk for adverse pregnancy outcomes—either through physical strain or the inability to secure adequate rest. This aligns with recent literature suggesting that household activity may be a risk factor for poor perinatal outcomes. A longitudinal study conducted among pregnant women in China, 20 found that those who maintained high levels of household activity throughout pregnancy exhibited greater physical and mental fatigue, even after adjusting for confounders. Fatigue, in turn, has been associated with increased risk of pregnancy complications, cesarean delivery, and postpartum depression, 21 highlighting the role of household burden as a vulnerability factor. Similarly, a study conducted in Spain, 22 showed that excessive occupational activity—often overlapping with domestic tasks in low-income settings—was associated with worse perinatal outcomes and poorer mental health indicators. These findings reinforce that the type, intensity, and—above all—the context in which physical activity occurs are critical to its effects. When physical movement is driven by necessity, without room for rest or autonomy, its benefits may be diminished or even transformed into a source of strain. This is supported by a meta-analysis showing that leisure-time physical activity significantly reduces the risk of preterm birth, while no such protective effect was observed for household or transportation activity. 23
Another important aspect concerns the barriers faced by pregnant women with psychiatric disorders in engaging in leisure-time physical activity. The literature highlights difficulties related to motivation, fear of judgment, low body image self-esteem, stigma, and social isolation.24,25 These subjective obstacles are compounded by structural barriers—such as lack of safe public spaces, limited time and financial resources, lack of childcare support, and restricted access to qualified professionals. As a result, leisure-time physical activity becomes a distant privilege, obstructed by multiple layers of inaccessibility.
Although no statistically significant associations were found between physical activity levels and psychiatric disorder severity—as measured by the Clinical Global Impression (CGI)—Table 5 points to relevant exploratory trends, such as negative correlations in the leisure (r = −0.86) and occupational (r = −0.63) domains. These trends suggest that women with lower symptom severity may be more able to engage in pleasurable and structured activities, while those experiencing greater psychological distress remain limited to functional activities such as domestic tasks. The small sample size may have limited the statistical power to detect more subtle associations. Additionally, it is important to consider the limitations of the CGI as a severity measure: while useful in clinical settings due to its simplicity, it is a global and subjective assessment that does not capture diagnostic complexity or functional variability. In the perinatal context especially, symptoms such as fatigue, anxiety, and social withdrawal may have multiple underlying causes, complicating the interpretation of overall severity and reducing the CGI’s sensitivity to detect nuanced relationships between physical activity and mental health.
Several limitations must be considered in interpreting our findings. The cross-sectional design precludes causal inference, meaning that observed associations are limited to correlational insights. This is particularly relevant in findings where reverse causality may be suspected, such as the case of gestational diabetes. Additionally, the study employed a non-probabilistic sample of women under mental health care, which limits the generalizability of the results.
Further limitations include the use of the PPAQ, a self-report instrument susceptible to recall bias and social desirability,26,27 especially in populations with lower educational levels. 28 Future studies employing objective measures such as accelerometers could provide more accurate assessments.
Taken together, the findings point to a pattern of physical activity shaped more by social, structural, and gender-based determinants than by autonomous motivation. The concentration of movement within the domestic sphere, the limited engagement in domains such as leisure, and the multiple vulnerabilities—psychiatric, economic, and gender-related—faced by this population underscore the urgent need for public policies that integrate physical activity promotion and perinatal mental health care as interdependent priorities.
Conclusion
The findings of this study underscore the need to rethink how physical activity is assessed, particularly in vulnerable populations. Rather than merely summing weekly minutes or estimating energy expenditure, it is essential to understand the context and motivation behind physical movement. Although most pregnant women with psychiatric disorders met the minimum weekly physical activity recommendations, the majority of this activity occurred in the household domain—characterized by functional demands rather than autonomous choice. The literature shows that the physical and mental health benefits of physical activity are more strongly associated with leisure-based practices, whereas household activity under pressure may reflect overload and a lack of self-care.
This population experiences a condition of triple invisibility—by being pregnant, by facing psychological suffering, and by living in socioeconomically vulnerable circumstances—which further exacerbates barriers to self-care. This study also highlights the importance of descriptive approaches to understanding underexplored realities, offering valuable insights for future research and the development of public policies that are more attuned to the lived experiences of these women.
Footnotes
Author Contribution
All authors contributed substantially to the development of this manuscript and meet the criteria for authorship. The specific contributions of each author are detailed below according to the CRediT (Contributor Roles Taxonomy) system: Oliveira, R. L. A.: Conceptualization (lead); methodology (supporting); writing—original draft (lead). Ferrão, Y.: Conceptualization (supporting); methodology (supporting); supervision (lead). Primo de Carvalho Alves, L.: Methodology (equal); formal analysis (equal); supervision (equal); project administration (equal). Scherer, J. N.: Methodology (equal); formal analysis (equal); supervision (equal); project administration (equal). Mattos, L. K.: Investigation (equal); writing—original draft (supporting). Mellati, M. E.: Investigation (equal); writing—original draft (supporting). Althoff, B. F.: Data curation (equal); writing—review and editing (equal). Oliveira, V. G.: Data curation (equal); writing—review and editing (equal). Santos, F. S.: Data curation (equal); writing—review and editing (equal). All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study will be funded by FAPERGS (Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul, (22/2551-0000532-2)).