
Abstract
Group settings create a collaborative relationship in which practitioners help patients build confidence, set goals, and remain accountable.
The economic and health burden of type 2 diabetes mellitus (T2D) in the United States continues to grow, and it is well established that lifestyle changes are the key to T2D treatment and reversal. In fact, lifestyle changes should be the first approach to T2D treatment and prevention.1-3 Shared medical appointments (SMAs) are one way to initiate lifestyle-based changes in T2D patients, and the successful use of SMAs in improving clinical outcomes for T2D has been documented, the majority of which included lifestyle-based nutrition and/or physical activity components. 4 SMAs are the use of group settings to treat or manage disease among multiple patients with the same condition, and they often provide an interactive environment with access to a team of providers. 5 Research has shown that benefits of group visits include greater patient and physician satisfaction, improved behaviors, increased self-efficacy, and improved quality of life. Group settings create a collaborative relationship in which practitioners help patients build confidence, set goals, and remain accountable. 6
In February 2020, a 12-week, in-person Diabetes Reversal Program (DRP) enrolling 12 participants was started at Midland Health (MH), in Midland, Texas. However, with the arrival of COVID-19 and executive orders limiting group gatherings in March 2020, the in-person program was put on hold. Eager to explore virtual options for continuing the program amid the pandemic, the program was moved to a virtual platform via Zoom, in line with guidance from the Office for Civil Rights, Department of Health and Human Services, encouraging covered health care providers to utilize telehealth to provide services during the COVID-19 pandemic. 7 The use of telehealth has understandably grown during the pandemic, and telehealth has been used across a variety of medical fields and for various purposes, including clinical care, medical education, rehabilitation, and health communication. 8
While the initial benefit of virtual SMAs was to allow for the program to continue safely during the pandemic, many other benefits quickly emerged. On the administrative end, the virtual programs require less staffing and less overhead cost. The virtual program is less time consuming because it eliminates elements such as travel. It also offers greater flexibility of scheduling, as both providers and patients can join group visits at their convenience from either work or home. An unexpected benefit is that it offers a convenient way for caretakes and spouses to support the patient by easily joining in on classes.
Visit Structure of the DRP Virtual SMA
Before beginning the virtual program, patients attend an in-person clinic visit for biometric measurements (weight and blood pressure) and a blood draw for measurement of HbA1c and fasting lipid panel levels. Patients also given a virtual visit consent that they are asked to review and sign documenting their agreement to receiving services via telehealth. A registered nurse (RN) makes sure a verbal consent has been obtained prior to beginning each first virtual visit and collects a review of systems, which is a list of questions reviewing body systems to identify potential clinical problems, for each patient’s physician visit note.
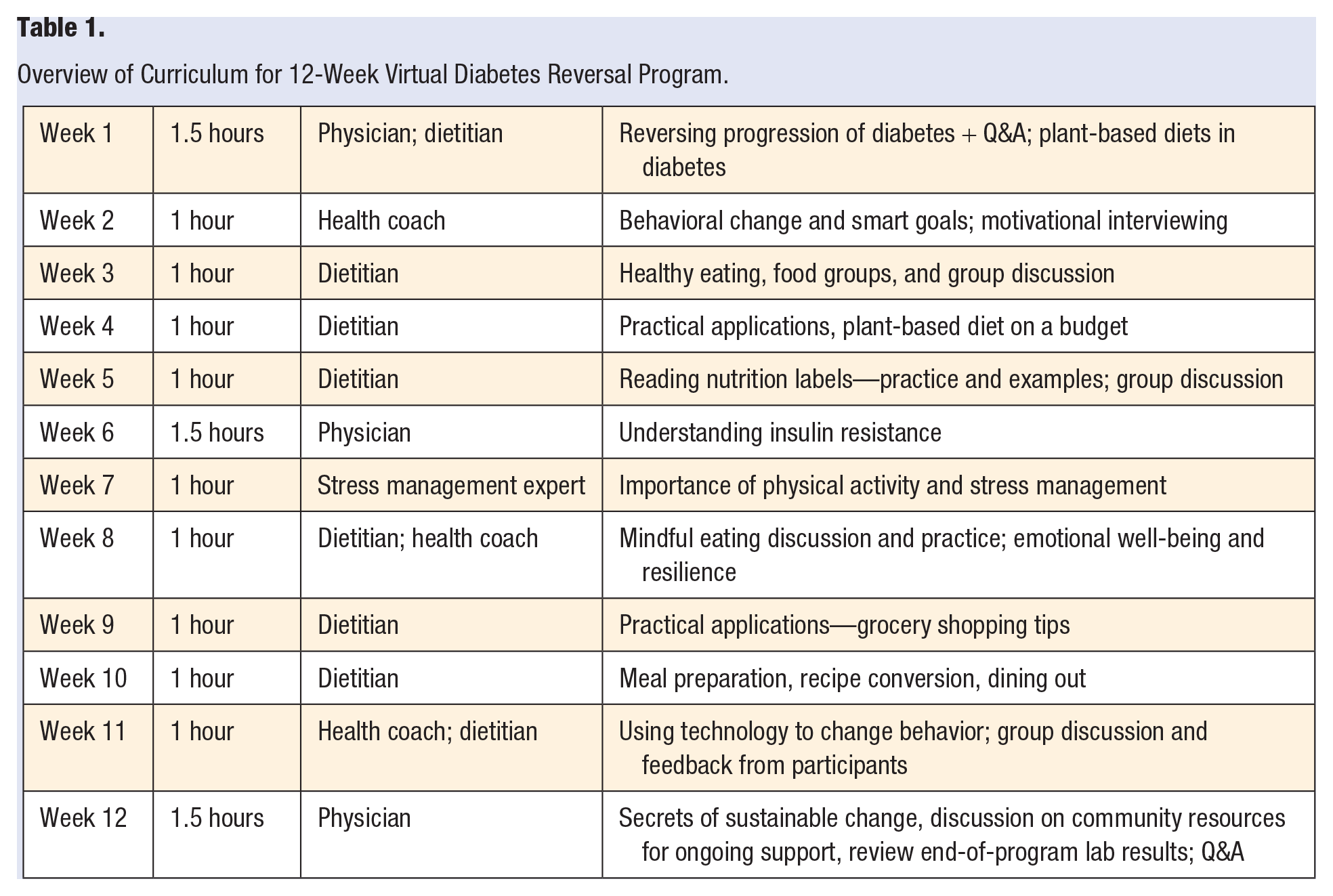
The virtual SMA health care team consists of a physician, registered dietician, health coach (RN), and exercise and stress management expert. Groups are limited to 8 patients. Physician visits last 1.5 hours, while visits with the other team members last 1 hour. Patients check in virtually 10 to 15 minutes prior to the start of the meeting. A brief overview of the curriculum for the 12-week virtual program is illustrated in Table 1.
Overview of Curriculum for 12-Week Virtual Diabetes Reversal Program.
In addition to the virtual 12-week DRP program, patients are provided with a variety of resources for ongoing support. These include an online wellness portal for hospital employees; access to a guide by the Plantrician project focusing on adopting whole food, plant-based diets to promote wellness; access to LighterPro, a software that generates personalized nutrition plans based on allergies, cooking skills, and other preferences; exercise and stress management classes, and health coach support. Patients are also directed to ourhealthycity.com, a local nonprofit that promotes wellness through plant-based nutrition and offers tools such as videos on how to better navigate grocery stores and local restaurant guides. Finally, patients are provided with opportunities for one-on-one contact with staff to ensure that questions and concerns have been addressed.
Lessons Learned
It is important to conduct a virtual visit demo appointment on zoom with each patient prior to them beginning the virtual program. This helps the program run smoothly by minimizing technical glitches. Second, in-person SMAs are conducted every other week, but the virtual program was changed to meet on a weekly basis to ensure patients remained engaged. The health coach’s role is to provide additional support by helping to motivate patients with strategies to enable positive lifestyle changes.
Although the virtual SMA program was originally put in place in response to COVID-19, we have found that it is equally, if not more successful, than the in-person SMA. The key factor driving the virtual program’s success is ensuring that the group feels connected, remains engaged, and feels the presence of a strong support network. In our program, this was achieved by consistent, weekly group appointments, ongoing health coach support and additional opportunities for one-on-one contact with staff as needed, as well as opportunities for small breakout sessions to further facilitate discussion and engage patients. Finally, “presentation” segments of the program were recorded so that participants could access the information again if needed.
Success Stories
Since March 2020, four virtual groups have been completed, and now we permanently offer both in-person and virtual versions. To highlight the program’s success, I would like to briefly share the stories of two patients who completed the program.
The first patient is a 49-year-old male, who began the program in person but was then admitted to the hospital for an abscess related to his T2D and developed sepsis, a severe infection spread in the blood that can result in vital tissue and organ damage. He was told it would take 6 months for his wound to heal and was unable to work. On then joining our virtual SMA program, his wound was completely healed in 2 months; he lost 40 lbs, improved his HbA1c from 7.9 to 6.1, returned to work.
The second patient was a 60-year-old male who felt that his health had been declining over the past several years. In addition, he was experiencing diabetic neuropathy and weight gain. He began the DRP and mentions that he, in particular, liked how the classes shared the scientific basis behind the concepts being presented, and he mentions frequently emailing back and forth with the dietician when he had questions about cooking and food preparation. He describes his weekly meetings with the health coach as “stripping away problems and being left with progress.” After the program, his HbA1c dropped from 6.9 to 6.2, systolic and diastolic blood pressure dropped by nearly 20 points, he lost 20 lbs, and his heart rate dropped by 10 bpm. Neuropathy in his ankle and feet was nearly gone, and he noticed his sleep greatly improved, which he attributes to improved breathing.
Conclusion
It is well established that promoting lifestyle changes benefits health, and lifestyle changes have the potential to dramatically improve outcomes in patients with T2D. At MH, we developed a successful 12-week SMA program for diabetes reversal. This program benefits patients by providing increased access to lifestyle-based wellness resources, and it financially benefits the health network by reducing staffing and overhead costs, and providing physicians, nurse practitioners, physician assistants, clinical nurse specialists, registered dietitians, and clinical social workers with an opportunity to bill insurances under the 12-week intervention. While the benefits to patients and staff are of utmost importance, it is also important to appreciate these financial benefits to the network, as billing and reimbursement for group medical appointments are often perceived as barriers for implementing SMAs. 9 As Lacagnina et al 5 mention, optimizing reimbursement helps to ensure viability, and it is important that SMA providers, from dietitians to nurses to educators, bill for services using existing Current Procedural Terminology (CPT) codes as well as their own National Provider Identifier to maximize reimbursement. 9
At MH, we demonstrated that our 12-week program could be moved to a virtual platform with success equal to or potentially greater than the in-person program. In addition to the benefits of in-person SMAs, virtual SMAs offer convenience and flexibility in scheduling, as well as opportunities to involve patient’s family members. 5 Zulman and Verghese 10 further note how virtual care has led to “the unexpected consequence of offering clinicians humbling insights into the lives of patients” with respect to factors that inevitably influence health, including living conditions, food security, and available support systems. With a continued focus on connecting and engaging virtually with patients, providing ongoing support, and providing patients with one-on-one opportunities to virtually connect with staff outside of the group setting, we will continue to offer both in-person and virtual SMAs as valuable options for patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.