
Abstract
Low-fat, vegan diets seem to be particularly effective for glycemic control and may significantly lower hemoglobin A1c levels in individuals with type 2 diabetes. However, health care providers report low levels of practice and argue that this diet is hard to follow. This controversy on the acceptability of low-fat vegan diets appears to be a significant barrier to its broader clinical implementation. This review investigated dropout and adherence rates in intervention studies using a low-fat vegan diet in individuals with type 2 diabetes. In contrast to the common belief that this diet is poorly accepted, this review suggests different findings. Dietary adherence appears to be good with approximately 50% of individuals meeting the criteria for high adherence in most studies. Adherence to a low-fat vegan diet was higher than adherence to conventional diets in several studies. Group support and regular supervision improve adherence. Moreover, relatively low dropout rates were found—indirectly indicating good acceptance and high patient interest in this particular dietary modification. Although this review has several important limitations, it appears inappropriate to associate low-fat, vegan diets with poor adherence in individuals with type 2 diabetes. With good and regular support, adherence rates are more than solid and physicians should advocate for this diet more frequently.
‘Several reviews suggested that a low-fat and predominantly plantbased diet may significantly lower hemoglobin A1c levels in individuals with type 2 diabetes.’
Lifestyle and healthy nutrition are the cornerstones of diabetes management.1,2 It is now widely accepted that both a predominantly plant-based diet and a low-fat, vegan diet are particularly effective for glycemic control.3-5 Several reviews suggested that a low-fat and predominantly plant-based diet may significantly lower hemoglobin A1c levels in individuals with type 2 diabetes.1,6,7 Significant improvements have been reported even in severe cases of type 2 diabetes. 8
Nevertheless, many health care providers report low levels of practice, and plant-based diets are not routinely prescribed by physicians.9,10 Some doctors remain skeptical 10 and persistently argue that a low-fat, vegan diet is hard to follow. According to the British Heart Foundation, a plant-based diet is a “serious undertaking” and not suitable for everyone. 11
In the clinical context, low patient interest and difficulties in facilitating patient adoption are often cited reasons for not promoting plant-based diets more frequently. 9 Lee et al argued that low compliance can be expected with vegan diets in clinical trials. 12 The authors emphasized that individuals with a prior omnivorous diet may encounter difficulties in maintaining a vegan diet for a longer period.
Other studies, however, indicated that the acceptability of a low-fat, vegan diet is generally good and similar to other therapeutic diets.13-15 In terms of dietary acceptance, no significant differences were found between a low-fat, vegan diet and a diet following the 2003 American Diabetes Association guidelines. 16 A more recent study reported high acceptability of a low-fat, plant-based diet among participants of a 30-day community-based intervention in Australia and New Zealand. 17 A study from the Czech Republic emphasized that individuals consuming a vegetarian diet felt less constrained than those consuming a conventional diabetes diet. 18 Moreover, it was suggested that perceived benefits of a vegan diet may facilitate adherence. 13
Consequently, there is an ongoing controversy on the acceptability of low-fat, vegan diets in individuals with type 2 diabetes. This controversy appears to be a significant barrier to a broader clinical implementation. Thus, a critical analysis of the available clinical studies in the field seems to be of utmost importance.
The aim of this review was to analyze (1) dropout and (2) patient adherence rates in low-fat, vegan diet intervention studies in persons with type 2 diabetes. Both could possibly serve as indirect indicators for the acceptance and feasibility of a low-fat, vegan diet in this cohort. Factors that influence participant adherence were also examined. Finally, a special focus was put on demographic data of participating individuals to explore who participated in these studies, and to identify possibly existing age and gender clusters.
Literature Search Strategy
The electronic database of PubMed was searched using the search string (“Plant-based” OR “Vegetarian” OR “Vegan”) AND “Diabetes.” Only English language articles were considered for this review. The entire review process was conducted by the author. Both original articles and reviews were screened. Moreover, cross-references and reference lists of the included articles and cited reviews were manually screened for additional articles to ensure that all potentially relevant studies were identified.
Articles were included if they reported on low-fat, vegan or quasi-vegan dietary interventions (with a minimum duration of 1 month) in individuals with type 2 diabetes. Only studies that reported either a dropout rate or an adherence rate were included in this review. Studies where >25% of calories came from fat were excluded for not meeting the criteria of a low-fat intervention. Studies including non-plant-based diets in the intervention group (eg, low-calorie diets containing technically vegan but industrially processed formula drinks) were excluded. Macrobiotic diets were also excluded from this review since they occasionally allow for small amounts of milk and fish.
Studies were included when the dietary modification was paired with another lifestyle modification, for example, aerobic exercise. Lifestyle modification programs and worksite interventions were included when more than 50% of participants were diagnosed with type 2 diabetes at baseline. Studies were included regardless of their location and setting (eg, clinical study, outpatient setting, corporate setting, medically underserved area, etc).
Results
The initial search using PubMed yielded 817 articles published between 1967 and August 2020. An additional 4 articles we found through manual search. A total of 821 records was screened. A total of 768 records were excluded after assessing the title and abstract. Fifty-three articles remained eligible for full-text review. After full-text review, another 46 articles were excluded for various reasons (see Figure 1).
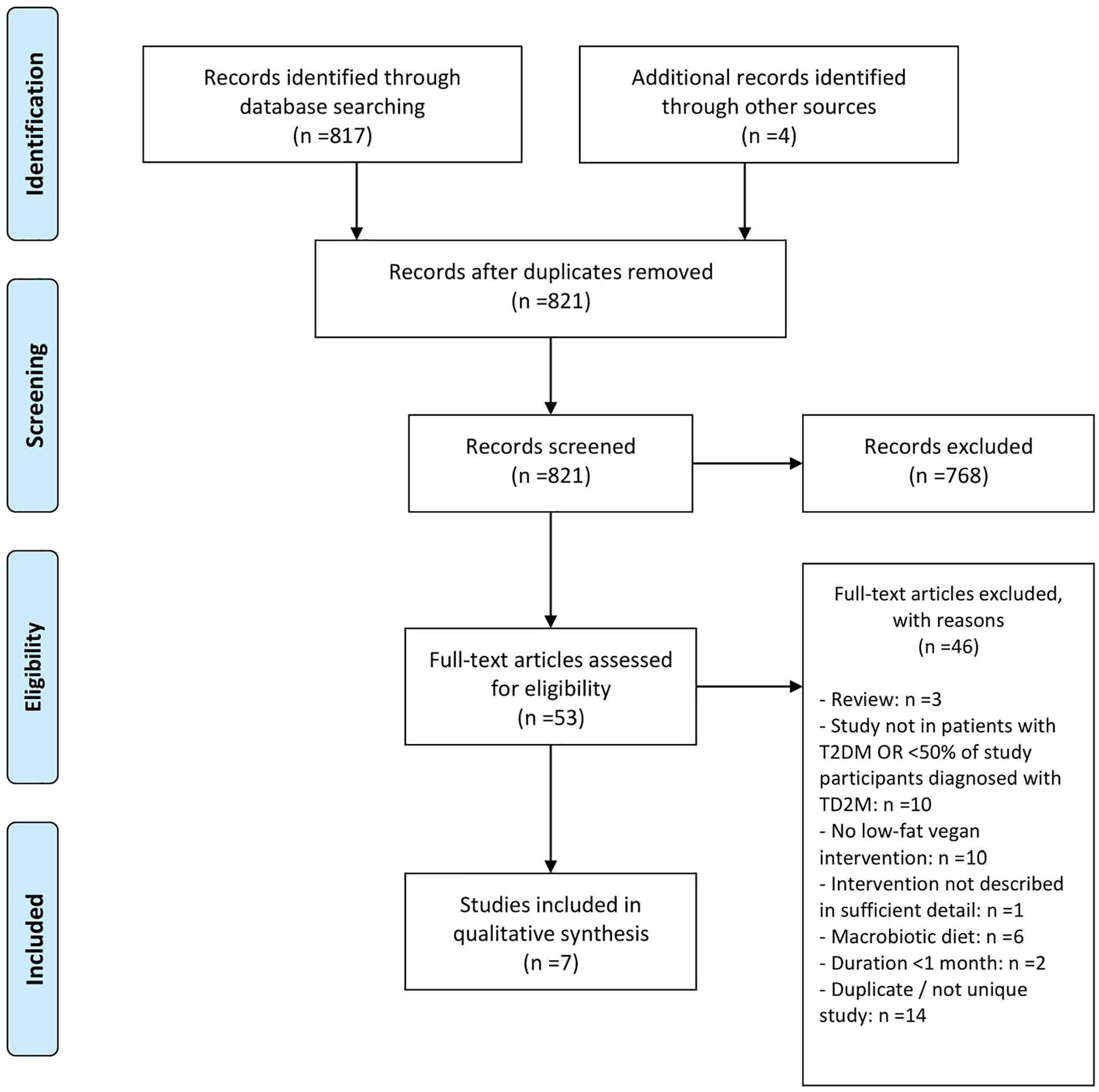
PRISMA 2009 flow diagram.
The literature review revealed 15 studies that used a low-fat, vegan diet in the treatment of persons with type 2 diabetes.3,12,19-31
Several studies reported on lifestyle modification programs that included vegan or plant-based diets a major component. However, some of these studies included only few patients with type 2 diabetes. A study by Campbell et al evaluating the effects of an 8-week whole-food plant-based lifestyle modification program was therefore excluded from this review. 26 While almost 99% of participants completed the 8-week intervention, only 25% (n = 20) of the study participants had type 2 diabetes and 10% (n = 8) had prediabetes. Studies by Shah et al, 28 Wright et al, 29 and Trepanowski et al 30 were excluded for similar reasons: the number of included patients with type 2 diabetes (n = 12 [24%], n = 7 [21%], and n = 2 [5.1%], respectively) was deemed insufficient to be representative of this cohort. The same applies to the GEIKO studies.21,23 Another study evaluating the effects of a physician-supervised 7-day residential program (the McDougall Program), that included a low-fat vegan diet, was excluded due to its short duration (see Figure 1). 27
Table 1 provides an overview of the remaining 7 studies in a chronological order. All but one study investigated the effects of a low-fat, vegan diet. In one study, individuals were allowed to eat one portion of low-fat yoghurt per day. 22 Nevertheless, this study was included in this review—given its almost comparable macronutrient content and the quasi-vegan design.
Dropout and Adherence Rates Among Individuals With Type 2 Diabetes in Low-Fat, Vegan Intervention Studies: An Overview.
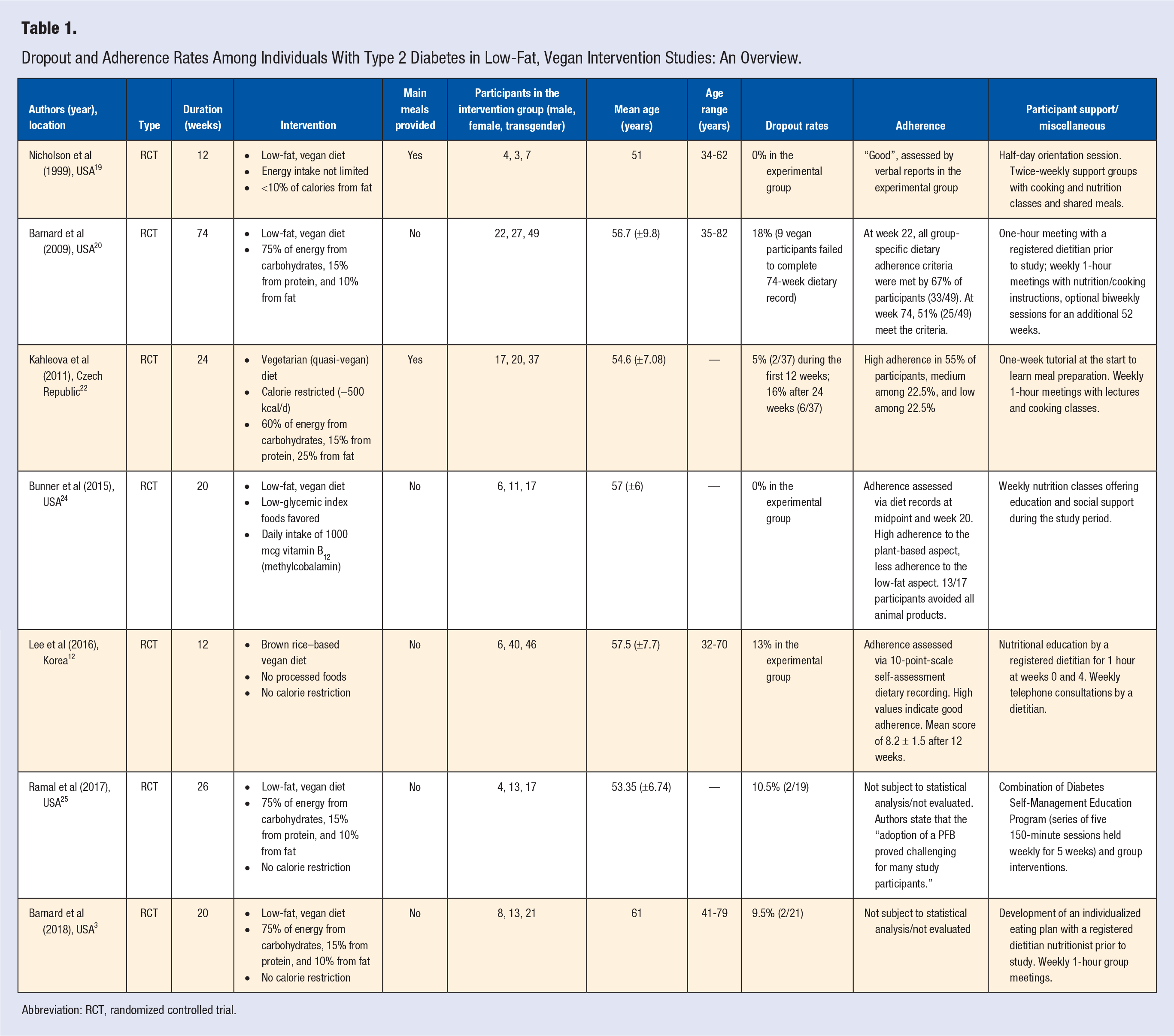
Abbreviation: RCT, randomized controlled trial.
The majority of the included studies was conducted in the United States.3,19,20,24,25 One of the included trials came from the Czech Republic and one from the Republic of Korea.12,22 One study had a special background and was conducted in a medically underserved area (San Bernardino County, California, United States of America), where residents face economic disadvantages and where the mortality from diabetes-related complications is particularly high. 25
Sample size was rather small and ranged from 7 to 49 in the intervention groups.19,20 Participants’ age ranged from 32 to 82 years.12,20 The mean age was 55.8 years across studies. In all but one small study, 19 more women than men were enrolled. In a Korean study from 2017, the proportion of women was 87%. 12 The highest proportion of men (57%) was found in a small pilot study by Nicholson and colleagues, which included only 7 participants in the intervention group. 19
Race and ethnicity were reported in detail in only 4 of the included studies.3,20,24,25 Apart from a 2019 study that specifically investigated the impact of a plant-based diet (coupled with group support and specific follow-up strategies) in Latinos, 25 people of Hispanic origin were underrepresented in most trials.3,20,24 The study samples in the trials by Barnard et al were predominantly White or Black.3,16,20 Their earlier study included an almost even number of White (21/49) and Black people (22/49) in the intervention group. Their 2018 study included more White (13/21) than Black people (6/21) in the intervention group. Study participants in the intervention group in the trial by Bunner and colleagues were predominantly White (11/17). 24
Study duration varied significantly and ranged from 12 to 74 weeks (Table 1). The average study duration was 26.85 weeks.
Dropout rates also varied significantly across studies. Both a smaller pilot study from 1999 and a trial by Bunner et al reported a dropout rate of 0% in the intervention group.19,24 Dropout rates were constantly below 20% across studies.
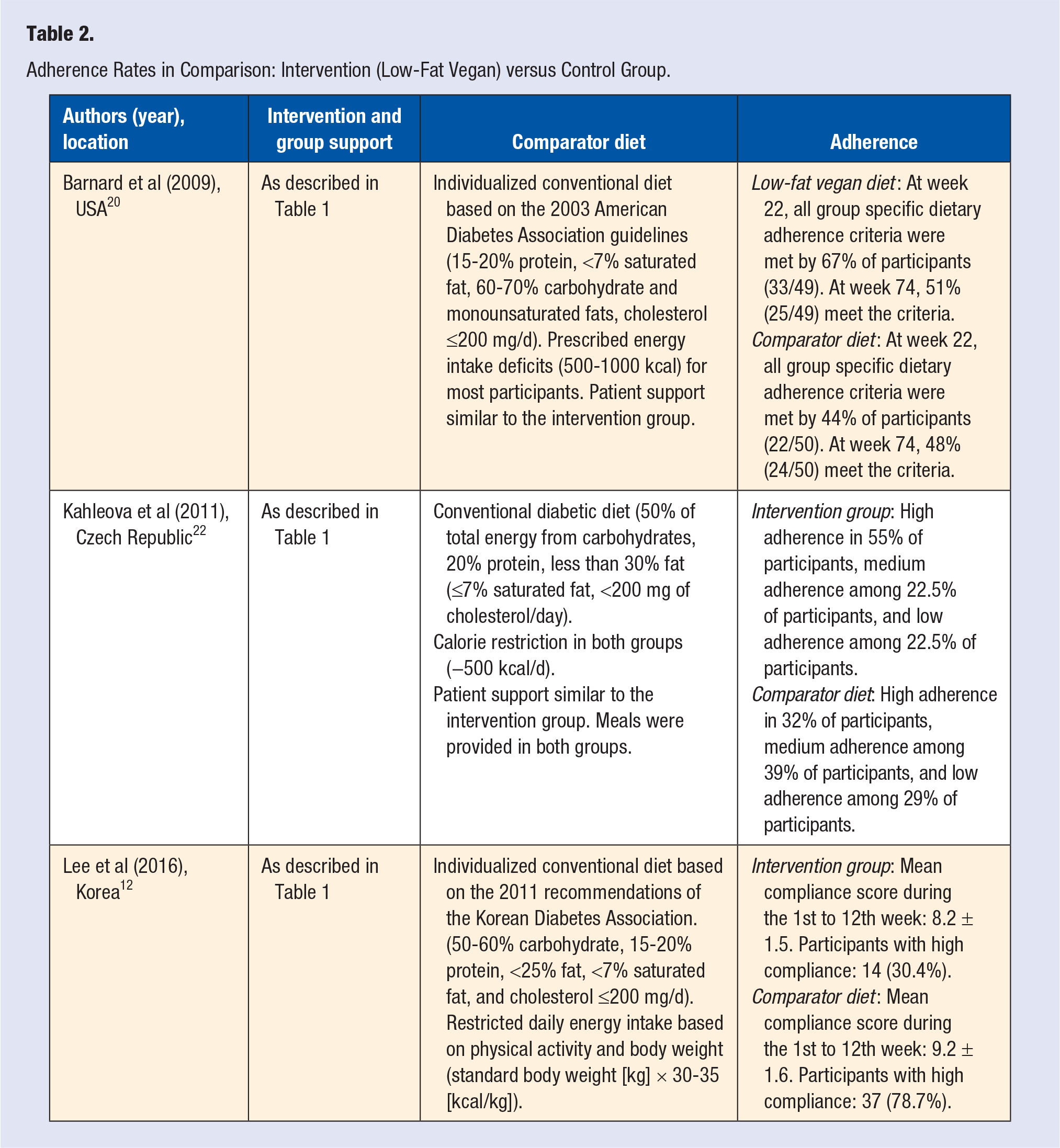
Adherence to the low-fat, vegan diet also varied significantly across the included studies (see Table 1). In most studies, adherence was either “good” or “high” according to the authors. A study by Barnard and colleagues revealed a particularly high adherence rate: 67% of participants in the intervention group met all group-specific adherence criteria. 20 Kahleova et al reported high adherence in 55% of participants and medium adherence among 22.5% of participants. 22 Some studies did not report adherence rates.3,25 Table 2 compares adherence to the low-fat vegan diet with adherence to the comparator diet in the control group of the respective studies. Only studies that reported adherence rates in both groups (intervention and control, respectively) were considered for this analysis. In 2 studies, adherence to the low-fat, vegan diet was higher than adherence to the comparator diet, and in one study it was significantly lower.
Adherence Rates in Comparison: Intervention (Low-Fat Vegan) versus Control Group.
Different approaches to assess adherence rates were chosen. Some authors defined adherence by specific criteria, such as “absence of meat, poultry, fish, dairy or eggs.” 20 Others employed a 10-point scale from which 1 point was deducted whenever an individual reported consumption of meats, poultry, fish, daily goods, or eggs in his daily dietary record. 12 In most studies, adherence was evaluated based on a self-assessed dietary records. Several trials included unannounced telephone calls to each participant with the aim to administer a 24-hour food-recall. However, these calls were not subject to statistical analysis.3,20,22
The literature search also revealed that the structure of the dietary interventions varied significantly across studies. In some studies, meals were provided on a daily basis (see Table 1).19,22 In other studies, it was the participant’s responsibility to eat in accordance with the study guidelines.3,12,20,24,25
Study targets for macronutrient distribution were comparable among studies. Diets were designed to contain 75% of energy from carbohydrates, 15% of energy from protein, and 10% of energy from fat (see Table 1). In one trial, the diet had a slightly higher fat content, partly because participants were allowed to eat one portion of low-fat yoghurt per day. 22
It is noteworthy that the degree of individual support and supervision also varied substantially across studies. For example, a Korean study from 2017 included personal nutritional education by a registered dietitian for 1 hour at the beginning of the study and after 4 weeks. 12 In addition to that, the study design included weekly telephone consultations by a dietitian. Compared to this study, the support for participants in other trials was more intense. In addition to a 1-hour meeting with a registered dietitian prior to the study, a trial by Barnard and colleagues included weekly 1-hour meetings with nutrition and cooking instruction for 22 weeks. 20 After the first 22 weeks, participants had the opportunity to attend (optional) biweekly sessions for an additional 52 weeks. A study from Kahleova et al and a 2018 study from Barnard and colleagues included a comparable intervention.3,22 The most intense interventions were found in studies by Nicholson et al 19 and Ramal et al. 25 It is also important that some studies paired the dietary modification with additional exercise. 22 Finally, to allow for a comprehensive discussion of the results, it is crucial to note that the vast majority of studies did not limit daily energy intake (see Table 1). Only one trial included a calorie restriction (−500 kcal/d). 22
Discussion
Limited adherence to conventional diets is well-documented among patients with type 2 diabetes in the literature.32,33 This review analyzed participant demographics, adherence rates, and dropout rates in low-fat, vegan dietary interventions in patients with type 2 diabetes. Moreover, this review explored how a low-fat, vegan diet compared to other diets in terms of adherence in this cohort.
The majority of study participants were women between the ages of 50 and 60. The proportion of men was comparably low. Dropout rates ranged from 0% 19 to 18%. 20 Dietary adherence to the low-fat, vegan diet appeared to be generally good. With one exception, adherence to a low-fat vegan diet was higher than adherence to conventional diets (see Table 2). Hereafter, findings from this review are discussed in detail.
Dropout rates ranged from 0% 19 to 18%. 20 Most studies had a dropout rate below 15% (see Table 1). This could be interpreted as an indirect indicator of good dietary acceptance and adequate feasibility. Dropout rates of 20% are common for nutrition intervention studies, 34 and the aforementioned rates are comparable with other nutrition trials in individuals with type 2 diabetes. Dropout rates in non-vegan, dietary interventions in individuals with diabetes were, for example, 18% in 12 weeks, 35 18% in 26 weeks, 36 50% in 52 weeks, 37 23% in 16 weeks, 34 and 30% in 16 weeks. 38 In regard to this aspect, low-fat, vegan dietary interventions do not seem to be associated with increased dropout rates in clinical trials.
Although dietary adherence was not assessed in every single study, it appears to be generally good (Table 1). Considering all aforementioned studies, approximately 50% of participants across studies met their group-specific dietary adherence criteria, indicating high adherence.21,22 This rate is remarkable, compared to the unsatisfactory adherence rates to dietary recommendations in other studies and populations.39-43 In one landmark trial, all group-specific dietary adherence criteria were met by 67% of participants (33/49) after 22 weeks. Fifty-two weeks later, more than half of participants (25/49) still met all criteria. 20 It is also important to note that adherence to a low-fat, vegan diet was slightly higher than adherence to conventional diets in all but one study (see Table 2).
Adherence criteria, however, varied significantly from study to study, which makes direct comparison a complex matter. Barnard et al defined dietary adherence to a vegan diet by 3 criteria, including (1) absence of animal products in any 24-hour recall, 3-day dietary record, or incidentally at any point; (2) saturated fat ≤5% and total fat ≤25% of energy on 3-day dietary record at weeks 22 and 74; and (3) mean daily cholesterol ≤50 mg on 3-day dietary record at weeks 22 and 74. 20 Although these criteria appear to be quite strict, two thirds of participants (33/49) in the vegan group met these group-specific criteria at week 22. 20
Kahleova et al assessed dietary adherence via daily calorie and cholesterol intake. 22 The authors defined high adherence as a daily energy intake being no more than 100 kcal in excess of the intake prescribed. Medium adherence was defined as less than 200 kcal in excess. Participants were included in the low-adherence group if none of the above-mentioned criteria were met. High adherence also required an average daily cholesterol intake ≤50 mg and medium adherence ≤100 mg, respectively. Based on these criteria, 55% of study subjects had a high dietary adherence and 22.5% had a medium adherence (Table 2).
While the proportion of subjects with high adherence appears to be satisfactory, it is lower compared to the study by Barnard and colleagues. 20 One potential reason for this could be that Kahleova and colleagues used a calorie-restricted diet. 22 This is usually not the case for low-fat, vegan diets, which elicit weight loss in the absence of prescribed energy limits. This is conceivable because reduced dietary fat intake reduces total dietary energy density. 3 The lack of energy limits or caloric restriction, which is a hallmark of the classical low-fat, vegan diet, seems to increase dietary adherence. The fact that both studies included a comparable amount of support for participating individuals further strengthens this argument.
The authors of a Korean study assessed dietary adherence rate in a completely different manner. 12 A 10-point scale was used and one point was deducted for the consumption of meats, poultry, fish, daily goods, or egg. During the first month, a mean compliance of 8.6 (±1.3) points was observed. Again, subjectively, this appears to be a good value indicating good adherence. The Korean kitchen is traditionally meat-based and a mean value of 8.6 points suggests that participants allowed themselves “only” between 1 and 2 exceptions per day. It is crucial to note that mean compliance scores decreased during the trial (see Table 2). Mean compliance score during the 1st to 12th weeks was 8.2 (±1.5) points. One potential reason for this could be the fact that personal support was rather limited in this specific trial. Apart from a single hour of nutritional education at the beginning of the study, the trial included “only” weekly telephone consultations. The personal- and the group-support aspect from other trials is missing. This is by far not an indicator for a low study quality, but rather a sign that the dietary intervention was initially well-received even without intensive support.
While it is difficult to compare the different dietary adherence assessments, the study by Lee et al suggests that increased individual support (including frequent group sessions) increases adherence. This is consistent with prior studies emphasizing the benefits of group-based diabetes self-management education over individual consultations.44,45 Moreover, regular dietary monitoring was found to be another key component in improving dietary compliance in patients put on a low-fat diet. 46
Identification of factors that might increase or decrease adherence is difficult because none of the studies was designed to assess adherence in the first place. A 2017 survey revealed that American health vegans and vegetarians were more likely aged 30 to 65 years, female, physically active, at least high school educated, and chronically ill. 47 Some of these attributes match well with the participants included in the studies discussed in this review (more female participants, mean age of 55.8 years, chronically ill). Nevertheless, it seems inappropriate to draw valid conclusions from this—simply because the studies are inhomogeneous and served other purposes in the first place.
A 2017 review by Burgess et al investigated determinants of adherence to lifestyle intervention programs in adults with obesity. 48 Hereby, (early) weight loss success was shown to be one of the most prominent predictors of adherence. Obesity and overweight are highly prevalent among individuals with type 2 diabetes.49,50 Importantly, low-fat vegan diets have been frequently associated with (sustainable) weight loss51,52 and this could be a potential explanation for the good adherence in the above-mentioned trials. Participants allocated to the vegan group lost significant weight after modifying their diet.12,19,20,22,24,25
Identification of factors that might increase adherence to a low-fat, vegan diet will be of great importance in the future. For the Mediterranean diet, for example, some predictive factors were already identified.53-55 This may be useful in designing effective lifestyle intervention programs. Similar work has yet to be done with low-fat vegan diets to spread their popularity.
Finally, it must be emphasized that meals were provided in some of the studies presented in this review (see Table 1). This could be a significant confounder, since it makes the dietary modification easier in terms of meal preparation, time management, personal efforts, and financial savings. One may not exclude that provided meals may increase adherence—simply because the dietary modification appears to be more convenient. On the other hand, veganism has many ethical and social aspects, including self-efficacy and social identification with the diet. 56 Provided meals could also decrease interest in those individuals who pay close attention to self-preparation of meals or for those who dislike eating out.
This review has several limitations that warrant further investigation. First, none of the included studies was designed to assess dietary adherence in the first place. Thus, adherence rates were usually not subject to statistical analysis. Some studies did not include an adherence evaluation.3,25 The use of different dietary adherence assessments is another crucial limitation. Subjectively, some methods appear stricter than others. One study did not categorize adherence, 12 which makes comparison between studies even more difficult.
Moreover, the amount of supervision and support varied significantly across studies (see Table 1). This leaves a lot of space for different interpretations of the available data. One study added aerobic exercise to the dietary modification after 12 weeks. 22 One may not exclude that persons who disliked the exercise part dropped out from the study for reasons unrelated to the dietary intervention. Furthermore, individuals whom were willing to accept assignment to a low-fat, vegan diet as part of a study protocol may have been generally more motivated than other individuals with diabetes.
The duration of the trials included in this review is another key limitation that warrants further consideration. Study duration ranged from 12 to 74 weeks, which results in a mean duration of 26.85 weeks. This is particularly important because only one trial had a duration longer than 1 year. 20 While short studies do not allow for reliable statements regarding long-term dietary adherence, it is also noteworthy that the trial with the longest duration reported the best adherence rate. 20 Barnard et al emphasized that at week 74, more than half of participants fully met their group specific dietary adherence criteria.
It is important to note that members of same study group (Barnard et al) were involved in 4 of the 8 included studies.3,19,20,24 It is plausible to assume that this study group gathered significant experience in the course of the years. This must be taken into account when discussing adherence and dropout rates. It is reasonable to assume that patients will significantly benefit from this experience and that an established team, with well-designed and proven methods, might be more efficient in empowering and motivating patients to modify their diet. This, in turn, might result in higher adherence and lower dropout rates.
Finally, there are methodological limitations of this review to consider. Given this review is a single author contribution, only one person screened and extracted the included literature. Only the electronic database of PubMed was searched (with an English language restriction); therefore, it is possible that relevant studies from other sources were missed.
Conclusion
There are many barriers to a systematic assessment of dietary adherence in low-fat, vegan intervention studies in individuals with type 2 diabetes. Comparison between studies is particularly difficult for several reasons, including different dietary adherence assessments and varying amounts of individual support. In contrast to the common belief that low-fat, vegan diets are poorly accepted among individuals with type-2-diabetes, this review suggests different findings.
Dietary adherence seems to be good across studies with approximately 50% of individuals meeting the criteria for high adherence in most studies. With one exception, adherence to a low-fat, vegan diet was higher than adherence to conventional diets (see Table 2). This serves as a clear indicator that the acceptance of low-fat, vegan diets is underestimated. Furthermore, group support and regular supervision seem to increase adherence rates.
The relatively low dropout rates also serve as an indirect indicator for good acceptance and high patient interest in this particular dietary modification. Compared with other nutrition intervention studies, dropout rates were not increased.
The analysis of demographic data of participating individuals revealed that younger men are underrepresented in low-fat, vegan dietary intervention trials. Findings are mostly derived from women in their 50s and 60s. Additional research is therefore necessary in this particular field. Race and ethnicity were reported in detail in only 50% of the included studies. It appears inappropriate to draw valid conclusions from these data. Future work in this field is therefore necessary to identify populations that are especially susceptible to such a dietary modification. Finally, future studies should identify factors that may increase or decrease adherence to a low-fat, vegan diet. This is of particular importance to design successful dietary interventions programs for those patients that are less susceptible to dietary modifications.
Although this review has several important limitations, such as the number and duration of the included studies, it appears inappropriate to associate low-fat, vegan diets with poor adherence in individuals with type 2 diabetes. This review indicates that the acceptance is much higher than often perceived by physicians. Summarizing this review and translating its findings into clinical practice, physicians should advocate for low-fat, vegan diets more frequently. With good and regular support, adherence rates to a low-fat, vegan diets are more than solid.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.