
Abstract
Adopting a plant-rich or plant-based diet is one of the major recommendations for addressing obesity, overweight, and related health conditions in the United States. Currently, research on African Americans’ food choices in the context of plant-based diets is limited. The primary aim of this study was to understand food-related experiences and perceptions of African Americans who were participating in the Nutritious Eating with Soul (NEW Soul) study, a culturally tailored dietary intervention focused on increasing the consumption of plant-based foods. The roles of gender and ethnicity were also examined to identify how eating patterns were chosen or maintained. Twenty-one African American adults in South Carolina, who were randomly assigned to either a vegan diet (n = 11) or a low-fat omnivorous diet (n = 10) in the NEW Soul study, completed one-on-one, qualitative interviews. Emerging themes included awareness, being in control, and identity. The study revealed that access to social support and coping strategies for addressing negative comments about plant-based food choices may be important components to include in future nutrition interventions focused on African Americans.
‘Awareness, being in control, barriers, dietary enablers, and identity emerged as the major themes that depicted participants’ perceptions and daily experiences with food choices irrespective of whether they were assigned to a vegan or omni diet’
African Americans (AAs) have a disproportionately high burden of cardiovascular and metabolic diseases compared with Whites and Hispanics in the United States. 1 AAs also have higher risks for obesity, hypertension, type 2 diabetes, and certain cancers.1-3 In comparison to other chronic conditions, cardiovascular disease (CVD) is a major cause of death among AAs. 4 AAs have a shorter life expectancy compared with Whites, and ethnic health disparities persist despite the availability of CVD-related medications and other pharmaceutical treatments. 5 The disparities are larger in states like South Carolina where CVD risk factors are more prevalent among AAs in comparison to Whites. 6 For example, in 2017, 76% of AAs were obese or overweight in comparison to 65.4% of Whites in South Carolina. 6 One of the goals of Healthy People 2020 is to improve cardiovascular health and well-being 7 ; therefore, research on viable treatment and prevention strategies for CVD, particularly among AAs, remains imperative.
Adopting a healthy diet is a major recommendation for reducing obesity, overweight, and the risks of various health conditions. 8 Guidelines from the American Heart Association indicate that dietary patterns that are rich in vegetables, fruits, whole grains, low-fat or fat-free dairy products, legumes, and nuts, and that limit the use of sweets and highly processed foods can facilitate cardiovascular health and reduce several health risks. 9 Individuals who consume plant-based diets gain significantly less weight and have a lower prevalence of type 2 diabetes compared with individuals who adopt other dietary patterns.10,11 There is increasingly more interest in the health benefits of adopting a vegan or a vegetarian diet, both of which are often rich in whole grains, fruits, vegetables, and legumes. A meta-analysis of 12 short-term randomized controlled trials that compared vegan or vegetarian diets with omnivorous diets showed that participants randomized to vegan or vegetarian diets had significantly greater weight loss than those assigned to nonvegetarian diets. 12 Additional analyses revealed even more significant weight reduction among participants assigned to vegan diets compared with those who were assigned to some vegetarian diets. 12 Studies that included AA participants have found similar outcomes, as AA vegans or vegetarians had significantly lower risks of hypertension, diabetes, and cholesterol as well as lower medication usage.13,14
Studies have examined factors that affect AA food choices.15,16 Research that focuses on AAs’ adoption of plant-based diets or plant-rich diets is sparse, however, particularly in the context of participation in a nutrition behavioral intervention. An in-depth exploration of the adoption process of these diets among AAs may provide an understanding of their food choice decisions and can inform the design of appropriate nutrition interventions. In this article, we report findings from an ancillary study on the experiences of AA adults who were participating in a randomized clinical trial to examine the effects of 2 dietary patterns on CVD risk factors and weight loss: vegan and low-fat omnivorous.
The goal of this ancillary study was to understand AAs’ perceptions and daily experiences with their respective diets and to identify how eating patterns were chosen or maintained. Additionally, links among gender, ethnicity, and dietary patterns were examined to elucidate how or why AAs make certain food choices. Men who follow plant-based diets may be perceived as less masculine.17,18 This perception has the potential to alter how men interpret and adopt diets in comparison to women. The mainstream portrayal of men, meatless diets, and masculinity appears to be changing as plant-based diets gain popularity, 19 but few studies have examined AA men’s perspectives on adopting plant-based diets with respect to the concept of masculinity. Therefore, we were interested in learning about their views and experiences.
In recognizing that food choices are often a product of social and cultural norms and self-identity, 15 the Unified Model of Vegetarian Identity (UMVI) was selected as the main conceptual model for the study. 20 The UMVI is a multidimensional framework that incorporates constructs of identity with research findings on personal and contextual factors that shape plant-based food choices to provide a more holistic approach for examining what it means to be vegetarian. 20 As nearly half the study participants were following a vegan diet and all participants were asked to either limit or eliminate certain animal products and increase plant-based foods, the UMVI was appropriate for capturing various aspects of their dietary experiences, and it guided the creation of the data collection instrument.
Methods
Study Participants
Study participants were those currently enrolled in a clinical trial known as the Nutritious Eating with Soul (NEW Soul) study. 21 NEW Soul has 2 cohorts of participants, and it focuses on the inclusion of healthy and culturally relevant southern foods in testing whether a vegan diet is more effective than a low-fat, omnivorous (omni) diet for CVD prevention and obesity treatment among AAs in South Carolina. Eligible NEW Soul participants self-identified as AA, were between the ages of 18 and 65 years, had a body mass index that ranged from 25 to 49.9 kg/m2, lived in the midlands area of South Carolina, and were willing to be randomized to either diet. For the current study, those in the first cohort were eligible to participate after enrollment in NEW Soul for at least 6 months. Within this time period, we perceived that participants would have gained some familiarity with their respective diets and would be better positioned to share their experiences.
Dietary Intervention
In partnership with local soul food restaurants and chefs, NEW Soul provided cooking lessons, recipes, and nutritional information on culturally relevant and healthier versions of popular soul food items, such as mac and cheese, fried chicken, and collard greens. For the first 6 months and within their respective groups, study participants attended weekly classes with hands-on cooking and behavioral content that was guided by the Social Cognitive Theory and the Diabetes Prevention Program.22,23 Participants were randomly assigned to follow a vegan diet (consisting of fruits, vegetables, grains, and legumes but no animal products) or an omni diet (consisting of fruits, vegetables, grains, legumes, and fish with limited animal products, such as reduced fat dairy, poultry, and fish, red meat, and eggs). Both diets focused on building nutritional choices around healthy plant foods. 24
Data Collection
Purposeful sampling was used to identify and select NEW Soul participants for in-depth qualitative interviews to examine perceptions and experiences with their respective diets. 25 The first cohort (N = 66) included 7 men and 59 women. About one third of these participants (n = 21) were interviewed with a similar number of individuals chosen for each diet type to enable saturation. Between December 2018 and March 2019, study participants were recruited for one-on-one interviews. They provided informed consent to complete a phone or in-person interview that was audio-recorded and lasted for approximately 35 minutes on average. Demographic information was collected prior to each interview, which included 13 open-ended questions that were designed using the following dimensions from the UMVI: motivation, dietary pattern, salience, and regard. There were also 2 open-ended questions that assessed participants’ perceptions of how their gender and ethnicity were related to their diet. Male participants responded to 5 additional open-ended questions regarding their beliefs and perspectives about what men typically eat and the meaning that they assigned to food. Each study participant who completed the interview received $10. Audio recordings of interviews were professionally transcribed and reviewed by the first author prior to analyses. The study was approved by the Institutional Review Board at the University of South Carolina.
Data Analysis
An open-ended thematic method, which involved line-by-line coding, was used to analyze all data with qualitative software, NVivo 12. 26 After data collection and transcription processes were complete, the first and third authors independently coded 5 transcripts, discussed the preliminary set of codes to resolve differences, and generated emerging themes. On reaching consensus, the first author recoded the initial 5 transcripts and the remaining transcripts using the established codes, which included work environment and accountability partner. Additional codes that were identified during analysis were categorized with similar themes.
Results
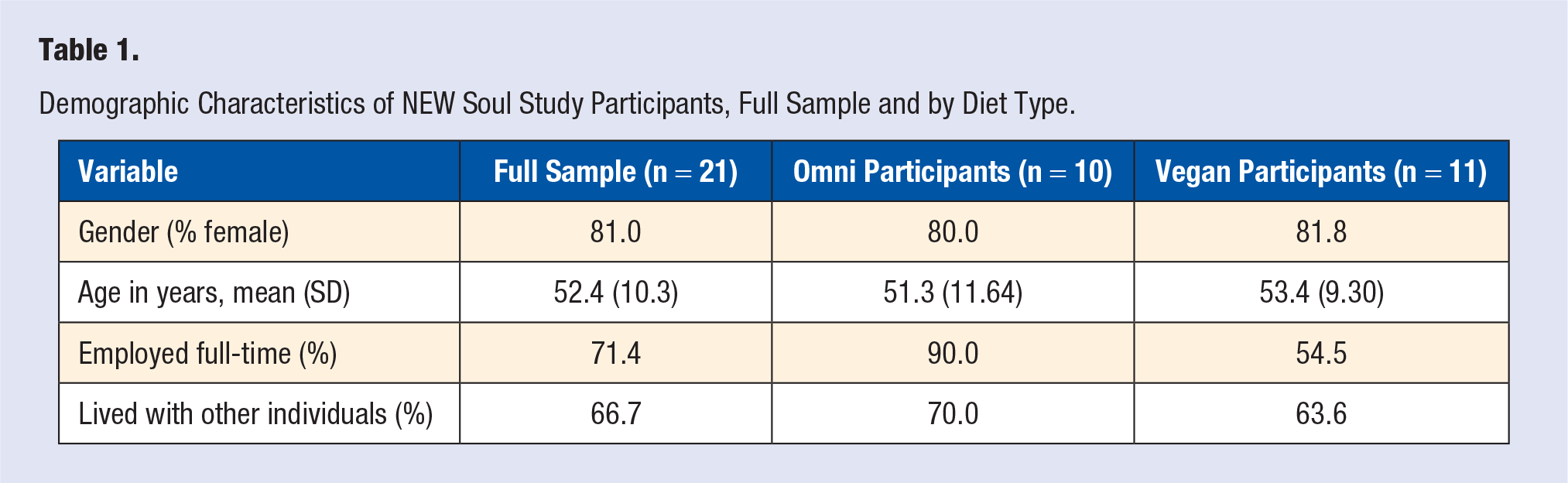
Participants were about four fifths female and 50 years (Table 1). Almost three quarters were employed full-time and two thirds lived with other individuals. Most participants indicated that they were inspired to make dietary changes because of personal motivation. Specifically, struggles with high blood pressure, prediabetes, weight loss, the desire to have more energy, and a family history of chronic conditions were major factors that prompted them to adopt plant-based diets.
Demographic Characteristics of NEW Soul Study Participants, Full Sample and by Diet Type.
Awareness, being in control, barriers, dietary enablers, and identity emerged as the major themes that depicted participants’ perceptions and daily experiences with food choices irrespective of whether they were assigned to a vegan or omni diet. The following sections include quotes that illustrate the themes and highlight individual, societal, and contextual factors that shaped AAs’ food choices.
Awareness
Study participants described how they were making more conscious food choices because they were more aware of healthier options and had gained knowledge and exposure from the larger study. Consequently, how they shopped for food and what and how they ate was changing in comparison to choices they made prior to the study. A vegan, female participant (VF14) explained: If I’m gonna do something sweet, I’m even now learning, okay, let’s pick up a piece of fruit instead of the Oreo cookie. Even though the Oreo cookie is vegan, let’s do fruit versus the cookie.
This quote from an omni, male participant (OM18) captured sentiments that many participants shared about incorporating more plant-based foods into meals: I think more about what I put in my mouth. I’m eating more beans and whole grains than I ever have. I used to think that grains were a no-no but I’ve been eating them and it’s been working out well.
A vegan, male participant (VM16) described how he was paying attention to labels: I’m conscious now of the grocery store visit that we went on. Now it makes you conscious about looking at labels, uh, seeing what the saturated fats is, what the, you know, the cholesterol, how much sugar is in it, the dietary products, and so it’s just made me more aware of eating healthier and—and ways of buying healthy items.
Several participants expressed how they were trying different food options because of increased knowledge. An omni participant (OF12) shared this about herself and her household: I’m more focused on eating healthier, making wiser choices in terms of making sure I eat three meals a day. I haven’t always done that. And making sure that there’s lots of vegetables, at my meals, which that wasn’t always the case. . . . We no longer have cookies and that kind of stuff. We now have healthy crackers like the Triscuits. We have carrot sticks, yogurt, that kind of stuff, which we didn’t always keep that on hand.
Additionally, some participants indicated that their food preparation methods changed because of increased dietary knowledge and awareness. One omni participant (OM10) described changes at home: I’m more mindful of what I eat and how I prepare foods. Rather than a lot of fried foods I bake more . . . baking more often now. . . . I don’t snack as much.
Other participants admitted that although they were more knowledgeable about healthier options, they were still struggling to become fully compliant with their respective diets. A participant (VF11) reflected: Well I eat less than—I do fall off the wagon sometimes. . . . I will not eat any red meat. I still do chicken every once in a while and salad. And so mostly it’s chicken and salad.
Furthermore, some participants described how their perspectives about food choices and sources had changed since study enrolment. They were more aware of their own behaviors and attitudes toward what and when they ate.
Being in Control
Most study participants indicated how they maintained control of their diets by becoming disciplined about their food choices. They were often determined to find appropriate meals and indicated how a change in mindset affected the selection and consumption of healthier options that aligned with their diets. One participant (OF18) noted: I don’t let what my husband or anybody else, ah, what they may be eating affect me because if I, you know, want to continue, on a course that I’m on, I mean it takes a while for you to lose weight, but you have to really want it, you know, to see results.
Many participants indicated that they remained in control of their diets because of coping strategies they adopted, especially when eating outside of their homes. For work, parties, or family events, some study participants prepared or bought items that were congruent with their diets and took those along to have options in that social setting. Planning was an important strategy that made it easier for some participants to remain compliant with their diets and stay in control of their choices.
For other participants, having a plan for social settings was equally important. One participant (VF18) explained: I’ve brought my own dishes before or a dish that I will eat . . . when we’re having a family gathering if I get a chance to put my two cents in we’ve got to have a salad bar. And so that’s the way it was thanksgiving, that’s the way it was Christmas and I think one of the good things I did was just to build my stuff up with salad and some toppings.
Some participants indicated that they were cautious about discussing their diets outside their households because they perceived that others were not comfortable, particularly with having to accommodate their new choices. One participant (VF44) described: So, what, what we learned to cope is we just don’t talk about it. [Laughs] You know, we just don’t warn anybody. And when we go there, we either bring something that we can eat with us and just say, “Hey, we brought a dish and this is pretty good,” and that works really well. Or we don’t say anything and we kind of pick around what’s available that is the path of least resistance for us.
In describing their interactions with others who did not share the same dietary restrictions or who questioned or criticized their choices, many participants expressed that they remained in control because they were unfazed by what others said. They described a firm commitment to being healthy and cited knowledge about better food choices as some of the reasons why they were not bothered by comments. A participant (VF14) said: It’s a decision and a choice that I made for me and my family and that’s—that’s just what it is. They eat what they eat, I eat what I eat.
Another participant (OF13) shared a similar opinion: Everybody has their opinion, but I don’t have to listen to them. . . . Because at the end of the day, I make the final decision about my body and my health.
Barriers
Although nearly all participants had positive experiences with their diets, they also described barriers to making plant-based choices. Some participants indicated that their work environments hindered their ability to select certain foods. One person (VF58) explained: ’Cause I’m usually, like, you know, waking up in the morning and on my way to work. And by the time I get home at night, it’s 8:00, 9:00 o’clock—8:00, 9:00 o’clock at night. So I’m going straight to bed. So it’s those wake hours and when I’m at work. The only time I ever have a chance to break is for lunch. . . . And then, sometimes at lunch if I hadn’t had a chance to make a Wal-Mart run or to make a kale salad, you know, I might grab, like, some pinto beans from Bojangles. . . . But it’s hard to find good, healthy food options if I’m not preparing it at home based on where I live.
A participant (VF15) who worked in the food industry said: Because I do work in a restaurant, there’s so many choices. It makes it hard, because I enjoyed meat in the past, that makes it hard, and just the whole complete change makes it hard.
Additionally, some participants, who lived alone, expressed a lack of interest in cooking for just one person, and this affected their food choices. One participant (OF19) shared this: I just have to spend some more time preparing. Probably on weekends because of my work schedule, and the time that I get home from work, I’m usually like just too tired to try to put anything together . . . and the effort of doing all that for one person.
For most participants, the biggest challenge was how their respective diets conflicted with food traditions in their homes or families. Some family or household members did not understand these new dietary changes, were not willing to provide support by changing what they ate, or lacked the knowledge and capacity for change. One participant (OF12) lamented about contrasts between family traditions and her diet: My husband bakes. He loves to bake. He only bakes at Christmas time, so he bakes a smorgasbord of tasty Christmas holiday treats. And he’ll make five different types of holiday Christmas cookies that we only have at Christmas time, but how do we navigate away from that because that’s been tradition for 22 years?
Additionally, another participant (VF11) described a typical meal at a family gathering: I mean, you probably could eat collard greens. But then, it’s gonna be cooked in fat. You might have a salad. Don’t always have a salad. So everything is—is cooked the traditional, southern way with butter and fat and, you know . . . the candy yams have a lot of butter in it. . . . So your typical holiday meal wouldn’t be fixed the vegan way.
A third participant (VM16) shared this: I don’t want them to feel uncomfortable because, you know, I’m a vegan that they feel like they can’t eat this in front of, “Oh, he doesn’t eat that or he doesn’t—”I don’t want that to be the topic of discussion. . . . I used to make pound cakes, so they ask now, “Are you still making pound cakes? Can—are you allowed [laughs]—to have pound cake?” and all this stuff. . . . So it’s like, you know, I don’t make them anymore, so they’re kind of, “Where is it?” you know, or so it—it kind of conflicts with the stuff that I used to prepare and I used to, you know, do most of the cooking, so now they’re having to resource—bring their own resources, and their own meals, and yeah.
Furthermore, some participants struggled with cooking and meeting the expectations of others, particularly when those participants were the ones who often prepared meals at home. This affected opportunities to fellowship with others over food items, including meat, that were previously a staple part of their diets.
Dietary Enablers
Having family support facilitated participants’ ability to make healthy choices. When partners, parents, or children accepted foods that aligned with either diet, study participants felt encouraged to make daily changes. One participant (OF12) described her partner’s role: My husband shops and he knows not to bring in things that are tempting . . . he pretty much does not buy the stuff that I’m like, “Please don’t bring this in the house.” So that’s very supportive.
For some participants, having a family member who attended at least one nutrition class influenced how food choices were perceived at home. Inviting these guests to engage in study activities was strongly encouraged as it was an important strategy for facilitating sustained support outside of the study. One participant (VF44) reflected: I was really amazed that when I was accepted in the study and, and pulled vegan, I didn’t know that my husband was going to share the same diet plan. I feel really fortunate . . . and he’s really compliant and, you know, I think, I feel fortunate. He’s really made it easier for me to not have to struggle with that at home.
Another participant (OM10) indicated that his partner’s response to food choices changed over time: Before it was like if you made fish, you know, it had to be fried fish. And I was like, well, I’m going to have to eat baked fish, you know, so, you know that was one of the biggest changes, like the preparation of the food from fried to baked . . . she’s been enjoying the different baked dishes, so she’s come around.
Sometimes family members supported study participants by cooking for them. In describing her family’s efforts, one participant (VF15) said: . . . My parents. They will prepare something that doesn’t have meat, just because they know. Or if I go out to eat, people in my family will already say they’ve got these vegetables or you can eat this.
Attending study-related nutrition classes, having accountability partners, and supportive work colleagues also enabled positive dietary choices among participants. Many participants mentioned the classes as an example of an instrumental resource for making dietary changes. One participant (VF19) shared this: I found the information presented in class helpful. Sometimes, I might challenge something about it, but I find it helpful that it pushes me to learn more, think more. You know, I’ve become acquainted with other spices in food groups that I don’t typically eat. You know, combinations of things, you know, that I wouldn’t have put together. . . . I’m certain I would not have done this independent of this study.
Participants also described recipes and other aspects of the classes that they found useful. One participant (VF18) said: The class itself I mean even the cooking demonstrations and so many recipes that I’ve been given. Of course if I was more diligent you would think especially if I’m not working full time I have more time to do these things but the resources have been great that we’ve been getting in class.
Furthermore, participants often referred to accountability partners they received through the study as a facilitator; however, a handful described others outside of the study who encouraged them to make, select, or cook appropriate food options. One participant (OF15) shared: I have my one accountability partner who’s been my best friend for 20-plus years and she’s a vegetarian, so I usually talk with her about if I’m having a struggle . . . about how to cook something different or try something different. She knows what my normal food tastes are, so she’s a big encourager for me.
Another participant (VF8) discussed ways in which her work colleagues facilitated her awareness of appropriate meal options: They see something, or a restaurant, or something at the store that indicates that it’s a vegan . . . you know, grabbing it and saying, “Hey, I thought you might want to try this,” or, “This is what I saw. They were advertising this.” . . . You know, trying to keep me abreast with things that are on the can do list.
In addition to using class materials, some participants conducted independent research to identify recipes and food items that they could incorporate into their meals.
Identity
In describing how they perceived themselves and their feelings about their respective diet, study participants shared 3 components of identity: feeling good about the diet, disassociation from the term vegan, and a lack of conflict between being AA and dietary choices. Additionally, male participants shared perspectives on masculinity and dietary choices.
First, some study participants expressed that they felt good about their food choices. For example, one participant (VM16) indicated that the diet change was empowering: I feel good about being a vegan and the direction that my life is going now, that the more I’m getting educated on meal preparation and just the support, it’s, you know, it’s a good direction, I think.
Others talked about how the diet change reminded them of the responsibility they had for their personal health and well-being. One participant (OF19) said: Well, it’s helped me to remember that my health is important, and that I bear responsibility in improving my lifestyle, and hopefully elongating my life in a healthy way, than to live a long time and still not be healthy.
Second, some participants abstained from using the term vegan when discussing their food choices in social settings. For example: I will say plant-based versus vegan because like I still own leather shoes and I know some people, you know, when you say vegan, it’s like you don’t do this, you don’t do that, you don’t do—you know, and I’m not that—it’s like this is what I eat or what I don’t eat. It’s not what I wear or don’t wear. (VF14)
Another participant (VF19) provided insight about the term: The word plant-based diet makes people more comfortable than saying vegan. You know, it’s because how can you be opposed to people wanting to eat plants? . . . I don’t usually say I am vegan . . . it doesn’t usually come up in that kinda way that I’ll answer questions by saying I’m vegan but mostly it comes up about choices that I’m eating and I’ll say that I’m eating a vegan diet. . . . If I’m standing up in a room introducing myself and they say tell us something about yourself, I probably would not say that I’m vegan as that being an important part of who I am defining myself as.
Third, reflecting on food and ethnicity, nearly all participants indicated that their dietary choices did not conflict with their AA identity. Some participants mentioned that many food items could be prepared in healthy ways. Others discussed stereotypes about AA foods, indicating that these did not depict who they were or how they conceptualized healthy eating.
One participant (OF19) said: I don’t see a conflict. It’s not like I sit and I think, “Oh my God, now I’m eating this and now I’m less of an African American because of choices I’m making.”
Another participant (VM15) succinctly described his perception of AA identity and food choices: I’m black. Eating differently don’t change that.
Participants generally indicated that the focus was on being healthier and finding alternative options to food items they enjoyed.
Finally, male participants, whose ages ranged between 39 and 60 years, reflected on the meaning of food, societal beliefs about men’s food choices, masculinity, and their diets. All 4 men indicated that they prepared meals at home. Two of them were primarily responsible for cooking for others in the home. Some men referred to food as a source of comfort or sustenance, but they also indicated that men’s food choices and values had changed over time. For example: Food is a comforter, you know. Food is delicious. Certain things, now, uh, my taste for that I used to not like, like beets and that type of thing, I find myself liking some things that I didn’t like as a child, you know. (VM16)
All men agreed that there were widely accepted beliefs that meat was a central part of men’s food choices and an important source of protein, but some men indicated that these societal perceptions were changing. For example, a participant (VM15) said: I think society changed. I think more and more people are vegan.
There were mixed opinions about whether adopting a plant-based diet conflicted with societal beliefs about what men eat. Two men expressed that the conflict occurred because men were often expected to eat meat instead of other items. In describing media portrayals, one (VM16) said: You get these commercials on TV all day long that just show men eating meat. You don’t see anybody sitting around talking about getting hummus.
The other male participants did not perceive any conflicts. One participant (OM10) indicated that societal perceptions of men’s food choices were changing because of the knowledge he had gained through the study as well as his recent dietary experiences: I see lots of guys that are super in shape and everything like that where they don’t eat a lot of meat. They eat lots of vegetables and stuff like that. They still have a physique like wow.
Additionally, none of the male participants saw a conflict between masculinity and choosing plant-based diets. All of them explained that making healthy dietary choices did not define a man or determine masculinity. One participant (OM18) said: It doesn’t conflict because to me your masculinity can be tied to how healthy you are. . . . At one time I might have thought it [masculinity] was tied to what I ate but I just don’t see it now.
Generally, gaining knowledge and media portrayal influenced men’s views of masculinity with respect to food choices.
Discussion
This study examined the perceptions and lived experiences of 21 AA adults who were enrolled in a nutrition behavioral intervention to identify how they adopted plant-based diets. Interviews revealed that awareness, being in control, barriers, dietary enablers, and identity affected their adoption of a vegan or omni diet. Findings about awareness, knowledge of food options, and enablers, such as social support, are not unusual as it is well-documented that these are determinants of food choice and dietary adherence.27-30 Study participants described how knowledge and exposure to healthy plant-based options and alternative meal preparation methods transformed their skills and perspectives on food choices. As documented elsewhere,27,30 however, awareness or knowledge alone was insufficient for behavior change. Some participants struggled in consistently making plant-based food choices. Support from a spouse, siblings, and others within participants’ social networks was crucial for transitioning toward those food choices. Participants also indicated that the provision of structured support and the assignment of an accountability partner through the NEW Soul intervention were instrumental in normalizing regular consumption of recommended foods for either the vegan or omni diets. Previous studies have indicated that a supportive network, which includes others who understand or have adopted plant-based diets, is critical for diet adherence.19,31,32 Future nutritional interventions for AA communities may benefit from incorporating these strategies to bolster dietary adherence.
Study participants mentioned two techniques that helped them remain in control of their diets. First, individuals reported adopting a mindset to be self-disciplined about what they consumed. Previous research indicates that self-discipline is important for making healthy eating choices. 33 Therefore, it is plausible that individuals who were already self-disciplined in other aspects of life may have applied this same value toward eating habits. Additionally, the desire to be self-disciplined with a diet may be linked to food value choices centered on health and well-being. 28 Prioritizing health above other food-related values, such as cost and taste, may alter an individual’s food-choice trajectory and increase self-discipline for diet adherence, particularly when illness occurs.28,34 In the present study, having a chronic condition or a family history with disease was often cited as impetus for a diet change; therefore, participants were potentially more conscious about altering their food choices for health reasons.
Second, some AAs in this study used meal planning to facilitate the selection of plant-based choices, particularly outside of their homes. Specifically, meal planning referred to preparing meals at home, taking lunch to work, and buying or packing food items for social occasions. Study participants who used any of these steps were more likely to have alternative food options in settings where healthy, plant-based items may have been limited. This may not be surprising as meal planning can enhance diet quality, and food variety and dietary adherence in diverse settings.35-38 Incorporating meal planning strategies that are appropriate for different household types into nutritional interventions, particularly within AA communities, may enable self-discipline for adopting plant-based diets.
Participants reported critical comments and negative occurrences when they made plant-based food choices, especially in social settings. Relatedly, the conflict between plant-based diets and existing food traditions with their homes and families was a major challenge for many AAs. In certain instances, household members or immediate family members were willing to accommodate plant-based meals and snacks, but extended family gatherings and other social occasions were more difficult to navigate when deciding what and how to eat. Additionally, some family members and friends put pressure on participants to consume meat or eat larger portions of food. Most participants said they dealt with this challenge by being unfazed by reactions and comments from others because they learned about healthy options from the study and were beginning to observe personal health benefits. In a study on food consumption identities among vegan and vegetarian men, participants also reported that they ignored negative comments that were made about their diets. 19 Among those who may adopt plant-based diets, experiences that involve negative behavior or comments about healthy food choices from others have previously been documented and may result in stigma.20,39 Concerns about being stigmatized or ostracized because of a choice to adopt plant-based meals and eschew meat may derail the desire to permanently adopt a plant-based diet. 40 In the present study, however, most participants did not modify their food choices to accommodate others whom they encountered when eating. As observed in a previous study, 32 some of our vegan participants expressed being cautious during conversations with non-vegans to minimize conflict and potentially critical remarks. Among predominantly AA communities in the US South, preparing and eating plant-based foods may still be novel, and many individuals may perceive such food items as nontraditional or foreign. 41 Therefore, it is important for AAs, who may be among the first to adopt such diets within their social networks, to receive education about how to cope with potential resistance from family, friends, and other acquaintances who may not be familiar with these food choices or their benefits. Additionally, the portrayal of AAs who have adopted plant-based diets through traditional and social media may reduce some of the associated stigma and resistance to these food choices within the AA community.
Study participants held various viewpoints when reflecting on their identity with respect to their assigned diets. First, most participants did not see any links between their AA identity and adopting a plant-based diet. They generally perceived that this lifestyle was important for their health and quality of life, but it did not conflict with their identity. A previous qualitative study that focused on vegans of color identified mixed findings on links between ethnicity and veganism with some participants suggesting that ethnicity was central to the notion of veganism while others held contradictory opinions about those ties. 39 Results from both studies underscore the intricate connections that link food to ethnicity and identity which may differ when considering food choice values, life transitions, geography, and other factors. 20 Additional research will be important for identifying nuances in cultural and ethnic identity with respect to adoption of plant-based diets, particularly in regions of the United States where such diets are less prevalent.
Some vegan participants in the current study did not identify as such within social settings because the term vegan may have negative connotations or made people uncomfortable. Instead, they used the term plant-based in describing their food choices when eating with others. This decision may have been a strategy to minimize vegan-related stigma and is reminiscent of low public regard among AA vegans in the current study. Study participants had adopted vegan or omni diets for only a few months prior to the qualitative interviews; therefore, it may have been hard to wholeheartedly embrace a vegan or omni identity because of the short period over which these diets had been adopted. Rosenfeld and Burrow 20 have indicated that such an identity may stabilize and gain prominence over time. Future studies on plant-based diets among AAs should consider how age, diet duration, and ongoing life events may concurrently shape food identity, health, and quality of life. Additionally, a vegan participant, who used clothes and shoes made from animal skin/hair, indicated that veganism exclusively referred to consumption of plant-based items. This distinction between food choices and other vegan-related issues may reflect the personal motivations for adopting a plant-based diet. Participants did not describe prosocial or moral motivations for adopting plant-based diets, as outlined in the UMVI model. 20 These motivations may be more common among people who adopt plant-based diets on their own when compared to individuals, such as our study participants, who were randomly assigned to plant-based diets for health-related reasons. An in-depth examination of personal, prosocial, and moral motivations and their ties to dietary adherence among AAs may be relevant for developing future nutritional interventions.
Another highlight of this study was the examination of AA men’s perceptions of masculinity with respect to plant-based diets. While there were only 4 male participants, their experiences and perspectives were important for expanding evidence on the intersectionality of plant-based diets and masculinity within a Western context. They believed that following a plant-based diet did not detract from masculinity, and one participant expressed that the way in which one treated other people was a more distinguishing characteristic of masculinity. Similar findings on the coexistence of masculinity and plant-based diets have been documented in at least one study in which predominantly White, male participants preserved their masculine identities because their decisions to become vegan or vegetarian were rational and evidence-based. 19
Perceptions of masculinity are often entrenched in cultural and societal norms and may influence health behaviors.19,42 Black masculinity is synonymous with physical and mental strength, provision, pride, and control.43,44 Other characteristics of Black masculinity, such as spirituality, family connectedness, and responsibility, have also been identified.42,45 All AA men in this study endorsed some of these characteristics of Black masculinity, especially when they talked about taking responsibility for their health and some positive interactions with family members in purchasing and preparing items that aligned with their diets. There appears to be an increasingly positive portrayal of male vegans and meatless diets in mainstream media.18,19 While AA men in this study did not explicitly raise this issue, it is possible that such media portrayals may have eased concerns about the perception of plant-based diets as ultra-feminine. In general, men are less likely to participate in studies, health promotion, or prevention programs,46,47 and this pattern was observed in our study in spite of the extensive recruitment of both men and women in and around Columbia, South Carolina. Additional research with a larger and more diverse sample of AA men can elucidate the intersectionality between masculinity and food choice identity.
This research broadens the current knowledge on the experiences of AAs who adopt plant-based diets, but there are a few limitations, including the use of a convenience sample and the low sample size. First, study participants were mostly female and middle-aged or older. Younger AAs may have different nutritional experiences. Second, participants had only been following their assigned diet for a few months, so their experiences and perspectives may be limited in comparison with AAs who have embraced a dietary change for many months or years. Third, NEW Soul participants who stopped attending classes were not available, so the sample for the ancillary study may be reflective of those who were more committed to maintaining their diets. Finally, both vegan and omni participants identified similar struggles with dietary adherence, but individuals on entirely plant-based diets and those on low-fat animal product diets may experience different issues with adherence.
In conclusion, this study provided important insights regarding AA’s perceptions and experiences with plant-based diets with implications for future nutrition interventions. For instance, continuously evaluating and enabling social support for making healthy food choices may facilitate successful outcomes. Additionally, using behavioral strategies, like role play, to empower AAs with skills to face criticism about plant-based food choices may be an essential intervention component. Further research on links between stigma and plant-based diets, particularly among AAs, may be useful in identifying appropriate strategies for adopting these food choices. As others have suggested, 41 expanding this work by including various ethnic groups will provide more insight about challenges and successes related to plant-based nutritional choices.
Footnotes
Acknowledgements
We are thankful to NEW Soul participants who completed the qualitative interviews.
Author Contributions
GMTM, EAF, SW, and MB designed the research. MB, AC, MD, MJW, and GMTM conducted the research. MB and AC analyzed the data and provided input for interpreting the results. MB wrote the paper. GMTM had primary responsibility for final content. All authors read the manuscript, provided edits, and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this article was supported by the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health under Award Number R01HL135220. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Approval
The study was approved by the institutional review board at the University of South Carolina.
Informed Consent
Written, informed consent was obtained from all study participants.
Trial Registration
The primary study from which participants were drawn for this research is a registered trial. The ID Number: NCT03354377.