
Abstract
A reformed approach to health care tackles health at its roots. Adverse childhood experiences (ACEs) in those exposed to them may contribute significantly to the root causes of many diseases of lifestyle. ACEs are traumatic experiences, such as physical and emotional abuse and exposure to risky family environments. In 1998, a ground-breaking study found that nearly 70% of Americans experience at least 1 ACE in their lifetime, and graded exposure is associated with the presence of mental health disorders, heart disease, cancer, and other chronic diseases. Over the past 20 years, evidence has demonstrated further disease risk, outcomes, and epigenetic underpinnings in children and adults with ACEs. Building resilience—the capacity to adapt in healthy ways to traumatic experiences—through lifestyle modification offers potential to combat the negative health effects associated with ACEs. Emerging research demonstrates resilience is cultivated through individual skills (emotional intelligence, coping, and fostering healthy lifestyle choices), and nurturing supportive relationships. Being mindful of the impact and prevalence of ACEs and diversity of individuals’ experiences in society will help build resilience and combat the root cause of chronic disease. This review aims to cultivate that awareness and will discuss 3 objectives: to discuss the effects and hypothesized pathophysiological underpinnings of traumatic experiences in childhood on health and wellbeing throughout life, to present ways we can promote resilience in our daily lives and patient encounters, and to demonstrate how advocacy for the reduction of ACEs and promotion of resilient, trauma-informed environments are fundamental to health care reform.
‘. . . those who had experienced adversity in childhood were more likely to have heart disease, lung disease, cancer, and numerous other health conditions.’
The Developmental Origins of Disease
As the American Academy of Pediatrics (AAP) identifies in place of their campaign, The Resilience Project, “Pediatrics is a Two Generation Practice.” 1 This is to indicate that our health as adult individuals is not independent of our childhood, and in fact, many diseases of adulthood lay their foundation throughout childhood. There is evidence that coronary artery disease lesions can be found in adolescents associated with modifiable lifestyle factors. 2 Adult chronic disease and pathology, including inflammation and, at least moderately, morbidity of cancer and cardiovascular disease, may have origins in utero and in early childhood.3-6 Additionally, to form healthy behaviors in childhood, research indicates that better success occurs with family-wide interventions. 7
Adverse Childhood Experiences, Lifestyle, and Health
In 1998, the Centers for Disease Control and Kaiser Permanente conducted a study of more than 17 000 adult Americans and found that those who had experienced adversity in childhood were more likely to have heart disease, lung disease, cancer, and numerous other health conditions. 8 The 10 adversities surveyed included physical, emotional, and sexual abuse; physical and emotional neglect; and having household dysfunctions, including a household member with mental illness or a substance use disorder; a mother who had been treated violently; parent separation through divorce, death, or other; or an incarcerated relative. 9 Adults with a history of adverse childhood experiences (ACEs) were found to be at higher risk of developing chronic diseases such as heart disease, lung disease, and cancer. They also have a 2- to 4-fold increased risk of high-risk lifestyle behaviors, including smoking and substance use, having multiple sexual partners, and acquiring sexually transmitted diseases, and a 1.4- to 1.6-fold increased risk of being sedentary and obese. 8
ACE exposure demonstrates a dose-dependent relationship such that a greater number of ACEs is associated with a greater risk of poor health, a relationship only partially attributable to behavioral choices. A recent study found that adults who have been exposed to 6 or more ACEs, for example, were more likely to die before 75 years of age, with a hazard ratio of 1.54, and 2.4 times more likely to die before 65 years of age than those who had fewer ACE exposures. 10 Importantly, this finding was only partially explained by ACE-related health and social problems because the results were adjusted for demographics, including age, gender, race, education, marital status, and financial problems, in addition to health and social problems known to be associated with ACEs independently, such as sedentary lifestyle, smoking, or obesity. 10 A British study corroborated these prior findings of a relationship between ACEs exposure and increased mortality. 11
Since the original ACEs study, a growing body of evidence has replicated and supported the findings of their impact on the field of public health. 12 Importantly, the original 10 ACEs are only some of the factors that can cause trauma for children. Childhood experiences not fully assessed by the ACE score, such as socioeconomic status and social isolation, have been associated with cardiovascular disease, 13 diabetes type II, 14 and risk factors for these and other diseases in adulthood. 15 Smaller studies have shown that the dose-dependent relationship with ACEs may also influence phenotype in particular disease. For example, in a cohort of women with chronic pain from fibromyalgia, those with a history of both physical and emotional abuse in childhood, independent of abuse in adulthood, had greater pain sensitivity and a greater number of locations of bodily pain. 16
The burden of ACEs may not stop with the exposed child and may be intergenerational. 17 In rodent animal studies of maternal separation or maternal food deprivation, offspring saw lasting effects to the stress and fear responses of their offspring. 18 Animal studies throughout the animal kingdom have demonstrated for some time that social isolation and maternal separation lead to poor health, suggesting the same for humans. 19 Human parental exposure to ACEs has been associated with negative outcomes in children, including behavioral health problems, poor health status perceived by the parent, asthma, and developmental delay.17,20-22
The ACE public health crisis is akin to the practice of lifestyle medicine. Felitti 23 came to design to the original ACE study based on observations made in practicing what might be now labeled as lifestyle medicine, in an obesity clinic. Felitti noted that many of his patients who successfully lost weight, but ultimately dropped out of the weight loss program, had a personal history of childhood adversity, which inspired Felitti’s Public Health Paradox: “What are conventionally viewed as Public Health problems are often personal solutions to long-concealed adverse childhood experiences.”23,24 Because the effect of ACEs on disease and mortality is only partially attributed to lifestyle behavioral choices, 10 addressing those choices alone may not get to the root of disease. To address chronic disease and mortality through lifestyle and behavior change, ACEs must first be addressed.
Underpinnings of the Relationships Between ACEs and Health
The mechanistic underpinnings of the association between ACE history and poor health are still being elucidated as more research in this field combining studies of psychosocial interactions with neuroscience and epigenetics emerges (Figure 1). Social burdens that put an individual at risk for ACEs also are associated with poor access to health care, high-quality nutrition, and higher education as well as other limited resources. 25 Similarly, these social constructs may predispose exposure to violence or substance use, enabling sedentary lifestyles or addiction. 26 It is hypothesized that the psychosocial stress of trauma exposure may lead to both poor lifestyle choices and burden the body physiologically; however, though these risks overlap, ACEs are not limited to any one socioeconomic demographic. 8 For example, hostile parenting behavior or environment in pregnancy, for a child of any demographic background, may link parental ACE history and the risk of ACEs in offspring.27-30
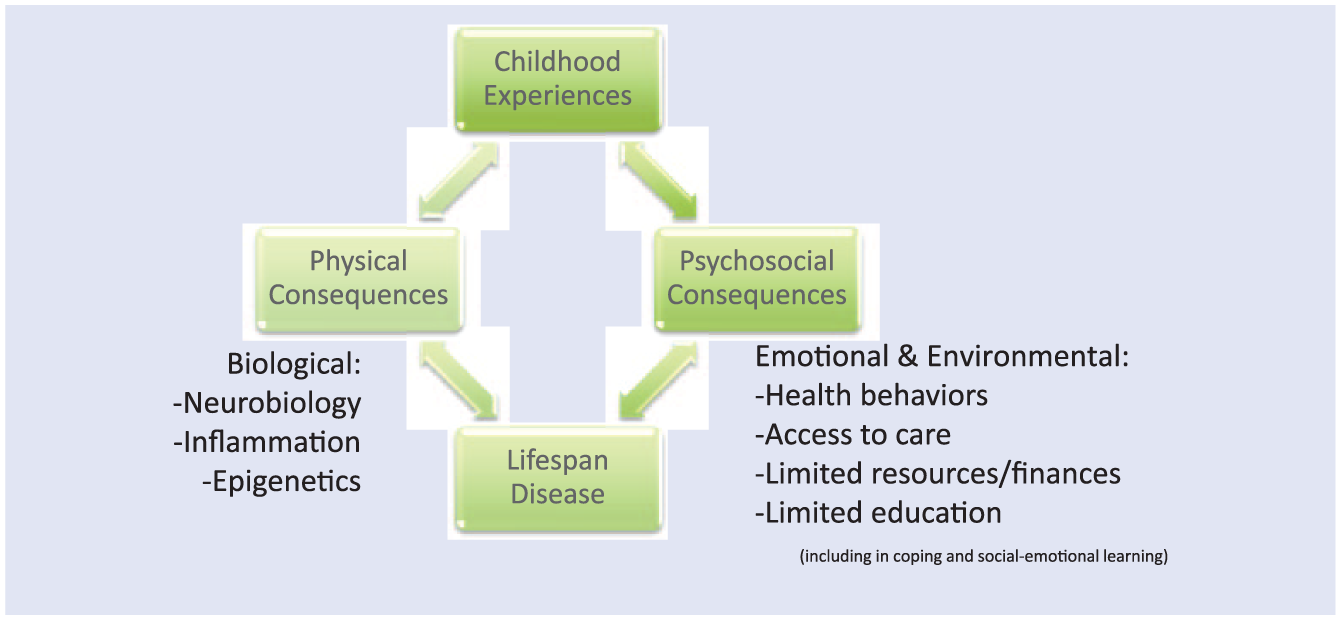
The interplay between ACEs, biology, environment, and disease through the life span: The impact of ACEs on long-term health consequences happens over a lifetime through physical and psychosocial mechanisms. ACEs are associated with increased risk of disease hypothesized to be a result of neurobiological, inflammatory, and epigenetic modifications. Additionally, ACEs have psychosocial impacts often combined with environmental circumstances. Those who experience ACEs are more likely to engage in unhealthy lifestyles, such as substance use and high-risk sexual behavior. Those who are in environments with limited access to care, resources, and education (especially social-emotional learning) are at greater risk of ACEs and also experience barriers to fostering resilience in such environments. The combination of biological, behavioral, and environmental associations with ACEs predisposes to disease across the lifespan.
Although the behavioral modeling context and psychosocial circumstances in which ACEs occur may influence their health effects, there is also evidence to suggest that there are physiological associations with the burden of ACEs, and although behavior plays a part, underpinning biology may predispose to a lower threshold of acquiring unhealthy behaviors. 31 With further research, disease outcomes may come to be linked with ACEs through nervous, endocrine, and immune system involvement. 32 The comprehensive physiological burden of trauma exposure and its effects on multiple organ systems is known as allostatic load. 33 Some of the hypothesized biological foundations to the impact of ACEs on health and contribution to allostatic load include neuroplastic, hypothalamic-pituitary-adrenal (HPA) axis, inflammatory, and epigenetic modifications.
The Central and Neuroimmune Association With ACEs
The influence of stress on the central nervous system leads to changes of wiring in the brain and central nervous system that goes on to affect the endocrine system through the glucocorticoid and cortisol pathways. In a study by Duncan et al, 34 children who have a history of ACEs show lower resting state activation on functional magnetic resonance imaging (MRI) of the prefrontal cortex, which is associated with attention and concentration, and the motor cortex. Additionally, they have decreased connectedness, using diffusion MRI, of the aversive response network, potentially indicating their inability to adapt to stress and harm compared with children without ACE exposure history. Hart and Rubia 35 reviewed how children with a history of child abuse also have decreased brain volumes, connectedness, and activation in the brain. 35 Specifically, the noted affected regions included the front-limbic brain associated with the processing of emotion and motivation and the fronto-striatal brain involved in executive function, working memory, and attention functions. Research has demonstrated that the effects on brain regions such as decreased gray matter volume in the limbic brain have a functional association with increased risk of relapse when recovering from a substance use disorder, for example. 31
Stress and trauma influence the brain, but this connects to effects on many systems of the body. The brain ignites the stress pathway of the body through the HPA axis. The HPA axis is the “fight or flight” mechanism of response to stress. 32 When a stressful event occurs, this triggers a cascade that releases cortisol, the stress hormone, to cause changes in the body to arm the body to face danger, including raising blood pressure, suppressing inflammation while activating natural killer cells, and elevating blood sugar levels for energy. 32 However, when the stress, or effects of stress are prolonged, or chronic, these physiological modifications can manifest as hyperactivity or hypoactivity of the HPA axis, autoimmune diseases or suppressed immune surveillance of neoplastic cells, hypertension and atherosclerosis, and diabetes and metabolic diseases. 33 In adolescents, those with a history of childhood maltreatment had a poorer multisystem profile, including 18 measures, some of which are as follows: cardiac (blood pressure, cholesterol), metabolic (glucose, insulin, waist circumference), and inflammatory biomarkers. 36 Some of the underpinnings may be because maltreated children in childhood, often into adulthood, had elevated inflammation and dysfunctional diurnal cortisol curves. 32 Specifically, social isolation, was identified by one study as contributing to inflammation independent of risk factors of adversity and other adversity types. 37
Evidence of HPA axis dysfunction manifesting as a result of ACEs stems from animal studies. One review summarized findings that demonstrated inverse function of the stress and fear responses of the HPA axis in mothers and offspring stressed by maternal child separation or maternal food deprivation. 18 Others have shown that parental bonding can be protective against activating stress responses such as reduced corticoid stimulating hormone and glucocorticoid feedback into adulthood. 38 In animals, bonding behaviors, including maternal grooming and nursing of offspring, are hypothesized to protect against intergenerational dysfunction of the HPA axis, possibly through the neural effects of the hormone.
In recent human research, a study by Hantsoo et al,39 that followed 48 women throughout pregnancy demonstrated an association with particular gut microbiota, specifically Prevotella species, and a history of ACEs. Additionally, particular microbiome diversity had associations with increased cortisol and inflammatory markers in response to stress, but in women with a high intake of dietary omega-3 fatty acids, high levels of inflammatory cytokine IL-6 in response to stress was mitigated. Therefore, ACE history, in addition to stress response and nutrition are hypothesized to impact the microbiome and inflammatory load in pregnancy, which then influence offspring health outcomes. 39
Epigenetics and ACEs
Epigenetics, or the study of modification of genes and chromatin without changes to DNA itself, has been associated with ACEs. An example of an epigenetic modification may be the addition of a chemical methyl group to nucleic acids, specifically cysteines, within the DNA that may affect the ability of those genes to be transcribed. 40 Many of the associations with ACEs and stress have been in genes of the HPA axis. In 2012, Tyrka et al 41 found that hypermethylation of the promoter region of the glucocorticoid receptor gene, NR3C1, was associated with lack of nurturing in childhood measured by parental loss, childhood maltreatment, and parental care. The epigenetic modifications were associated with functional HPA response to stimulation testing. In 2016, Yehuda et al 42 demonstrated that hypermethylation of the FKBP5 gene, a chaperone to the glucocorticoid receptor, was present in holocaust survivors. Importantly, this study was one of the first to demonstrate that correlated inverse changes in the methylation of FKBP5 were seen in their offspring. 42 Tyrka et al 43 since reviewed this and others’ works and concluded that these epigenetic modifications could be the link between psychosocial dysfunction in childhood and adult psychiatric disease. This work has prompted others to hypothesize the connection between maternal and early childhood health and disease with later life comorbidity through epigenetics and need for further research. 44
With the association between ACEs and cardiovascular disease, a recent study demonstrated that hypermethylation of FKBP5 is associated with increased risk of cardiovascular disease, such as elevated body mass index (BMI), waist circumference, hemoglobin A1C, and low-density lipoprotein (LDL) cholesterol. 45 Additionally, it was found that a subset of individuals had associations between FKBP5 methylation and number of cardiovascular procedures while having an inverse association with physical activity, independent of LDL cholesterol and BMI, respectively. This work demonstrates that there is more to be discovered in the connection between epigenetics associated with ACEs and the underpinnings of adult chronic disease.
Taken together, it is clear that the interplay of neuroscience, epigenetics, and life course social and behavioral factors lays the foundation for the development of maladaptive physiology that may predispose to psychiatric and chronic disease if not inhibited. 46
Resilience: Individual to Community
Resilience is the ability to recover from or adapt to change or adversity. 47 The Centers for Disease Control and Prevention state that the greatest protective factor against the sequelae of ACEs on health are safe, stable, and nurturing relationships and environments.9,48 Resilience in individuals can be fostered through their self, surrounding environments and relationships, and communities that support building internal and external characteristics (Figure 2).
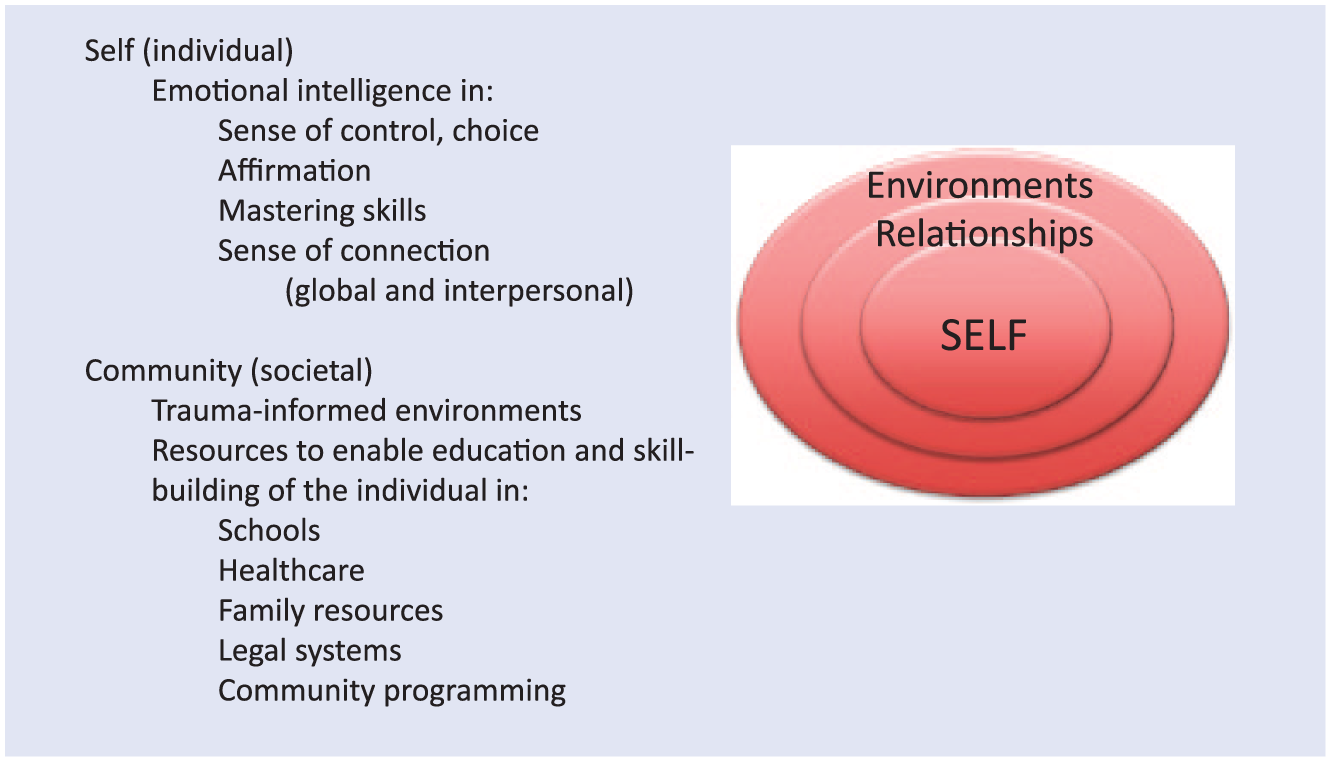
The layers of resilience: self and community. Resilience, or the ability to adapt to change, can occur at individual, interpersonal, and community levels. Individual (or self) resilience occurs when one embodies a sense of control, affirmation, master of skills, sense of connection with others, and a purpose. These characteristics stem from emotional intelligence and social support that can be created in safe and supportive relationships. Community (or societal) resilience occurs when a larger environment is created that is trauma informed and provides resources to enable education and skill building in individuals through schools, health care organizations, law enforcement and policy makers, and family programming.
Individual Resilience and Interventions
Individual resilience can be built through enhancing skills of emotional intelligence and coping with stress. Such self-characteristics may include self-esteem, hope, and a sense of control.49,50 When an event occurs, individuals may experience it very differently, allowing it to result in different effects. An event that is experienced as traumatic may have poor longitudinal effects. 51 If an event is mildly stressful, though, there is some space for an individual to mitigate the effect using resilience. For example, when one builds skills of emotional intelligence in themselves and others, it may enable an emotional space to be formed around the experience and a sense of control over the moment and, possibly, with a calm response, rather than reactivity. This allows for a potentially stressful event to be mitigated and not necessarily exert a potential negative effect (Figure 3). However, not all stressful or traumatic effects can be avoided. Therefore, the ability to adapt to change, or resilience, is also a cumulative process after the experience of many events. This long-term resilience can also be fostered. Traub and Boynton-Jarrett 47 reviewed the literature to synthesize the factors that may modify individual resilience in early development into five as follows: 1— directly building individuals’ cognitive traits (positive appraisal style, or having optimisim and confidence in the face of adversity, and executive skills), and supporting individuals’ growth through 2— coaching responsive parenting, 3— supporting maternal mental health, 4— teaching parents the importance of good self-care skills and consistent household routines, and specifically for clinicians, 5— offering anticipatory guidance about the impact of trauma on children.” 47
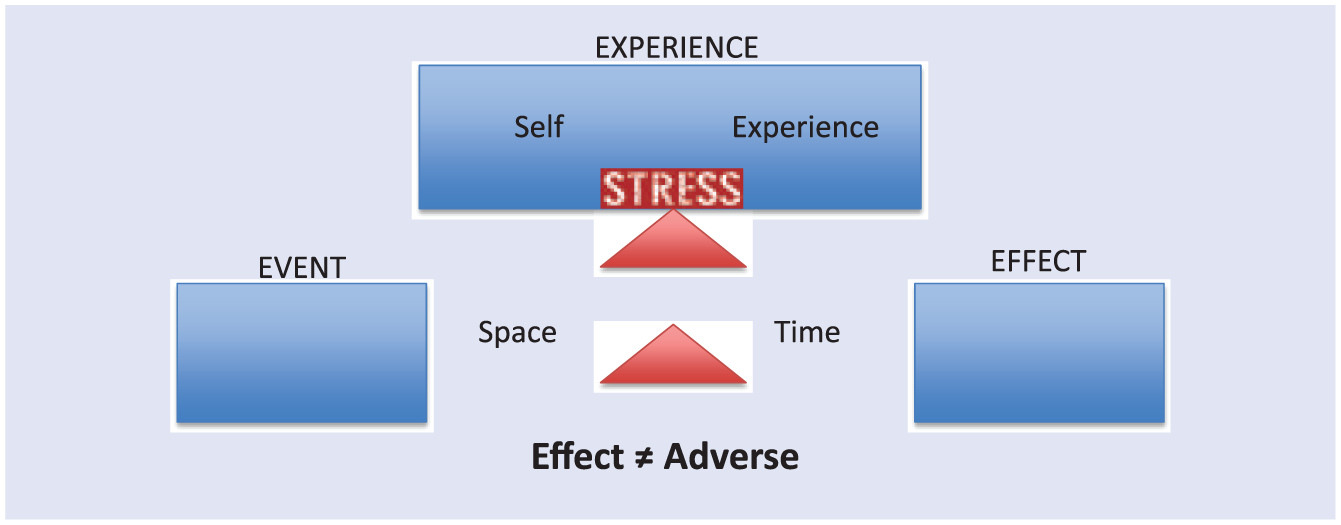
Building resilience: An individual’s experience of an event may lead to an effect that is adverse or resilient. If one has skills such as emotional intelligence, coping, or mindfulness, they may build a biopsychosocial space (emotionally calm and physiologically nonactivating of the neurobiological stress response) that fosters a moment of control over outcome of the event. This may allow a less adverse experience and effect to result despite the occurrences of a potentially stressful or traumatic event.
Resilience promoting skills can be fostered through early healthy relationships and modeling, as can be done with positive parenting approaches, which may offset developmental and emotional health effects or impacts of stressors such as economic hardship.52,53 Resilience can also be fostered through educational interventions that help an individual maintain balance targeting “the resilience zone.” In this zone, individuals act with adaptability, social awareness, high executive functioning, and responsiveness rather than reactivity. 54 Therefore, any intervention aimed at reinforcing these skills may build resilience. Some examples include mindfulness or social-emotional learning (SEL).
Mindfulness, or the practice of awareness without judgment or attachment, taught directly to children or through parenting skills, may foster resilience. 55 Mindfulness can allow for mitigation of a stressful experience (Figure 3), but its practice over time (weeks) has been shown to increase attention, social skills, conflict avoidance, and coping in children, resulting in improved classroom behavior, decreased anxiety and depression, and even a reduction in child abuse potential by parents. 55 Similarly, SEL allows children to identify emotions and respond skillfully, perhaps limiting the manifestation of emotions such as frustration or sadness as negative behaviors or aggression. The core competencies of SEL include social skills, identifying feelings of others and self, and behavioral coping and relaxation. 56 Such educational programs also improve children’s academic performance, as demonstrated in a study that compared SEL with a control curriculum. 57 SEL can be classroom based or delivered at home such as with the Mind Yeti58,59 app developed with the Committee for Children, which is an application for mindfulness activities with children and caregivers. Importantly, this study did not assess for ACEs, nor do the interventions for school-based mindfulness programs reviewed by Ortiz and Sibinga, 55 yet the characteristics of resilience can be fostered early in life even without identifying if a history of ACEs is present. 57
Trauma-Informed Care
Just as resilience can be built without identifying a history of trauma, many children and families who are likely to have experienced unknown violence or other trauma present to medical care. 60 Therefore, social interactions including those in health care should be cognizant of trauma exposure in all individuals. 60 The Substance Abuse and Mental Health Services Administration (SAMHSA) defines that a trauma-informed approach follows the “4 Rs” and “realizes the widespread impact of trauma and understands potential paths for recovery; recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system; and responds by fully integrating knowledge about trauma into policies, procedures, and practices, and seeks to actively resist re-traumatization.”51(p9)
Although SAMHSA suggests that this can inform approaches that organizations and communities can take, the AAP suggests that a trauma-informed care approach can be started by individual providers with a simple frame of mind. The AAP states that ACEs should influence practitioners to consider asking, “What happened to you?” instead of “What’s wrong with you?” with their patients. 61 Lifestyle medicine and behavior modification can be informed by the concept of, “What happened to you?” For example, when approaching smoking cessation counseling, one might look to identify environmental or stressful triggers for smoking. In stressing the importance of adherence to a healthy diet, one may identify what emotions unhealthy foods might be masking. In attempting to suggest increasing exercise and physical activity, one might identify barriers in safety or social support in the environment.
The Biology of Resilience
When resilience skills or interventions are trialed, they have biological consequences from childhood to adulthood that oppose the biological impacts of ACEs. For example, early attachment promotes increased temporal gyrus—a brain area involved in language and social cognition—volume in later childhood. 62 Systemically, parental warmth is associated with decreased allostatic load, including measures of blood pressure, cortisol levels, cholesterol levels, glucose and insulin levels, waist circumference, and inflammatory markers. 36 In adults with a mean age of 35 years, experiencing attachment through a supportive relationship demonstrated increased attention through a reactive time analysis task and associated increased activation of the prefrontal cortex (the brain region involved in attention). 63 Mindfulness practiced in a cohort of adults, mean age of 25 years, demonstrated increased attention with increased prefrontal cortex and decreased amygdala (brain region associated with fear) activation. 64 Although social isolation can raise the odds of inflammatory and biological markers comparable to individuals living a sedentary lifestyle, those with the highest amounts of social support had lower levels of inflammatory C-reactive protein levels as well as lower waist circumference, BMI, and systolic blood pressure. 65
Although some biological outcomes have proven to be reversible with resilience, the science of epigenetic and behavior modification is still in its infancy. Scientists hypothesize that epigenetics is a promising field in the underpinnings of disease because of its reversibility, at least pharmacologically. 40 However, some of the original science in epigenetics done by senior investigator Andrew Feinberg and colleagues demonstrated that methylation of DNA occurs with behavioral change in honeybees that take on different roles in their community, changes that can be reversed when going back to their original roles. 66 This work implicates epigenetics as an exciting field for the possibility of reversal of the imprints of psychosocial and behavioral adversity in humans, but such research would require longitudinal data that have not yet been completed.
Action and Advocacy Toward Resilience
Many organizations and resources are available to those interested in fostering environments of resilience at home, in schools, or in communities. Although most have not undergone randomized controlled trials for efficacy, they are built on the evidence of SEL, relationship building, and mindfulness. Table 1 offers a nonexhaustive list of tools for caregivers, educators, and families of young children to help build skills or create supportive environments. For example, the Robert Wood Johnson Foundation and the Joan Ganz Cooney Fund for Vulnerable Children partnered with Sesame Street to create the Sesame Street Communities online platform with videos, short games, and exercises that can be used as tools to help lay foundations for communication and education in families around topics of adversity and stress.67,68 Some topics include incarceration, divorce, and mindfulness.
Examples of Resilience Building Tools and Organizations.
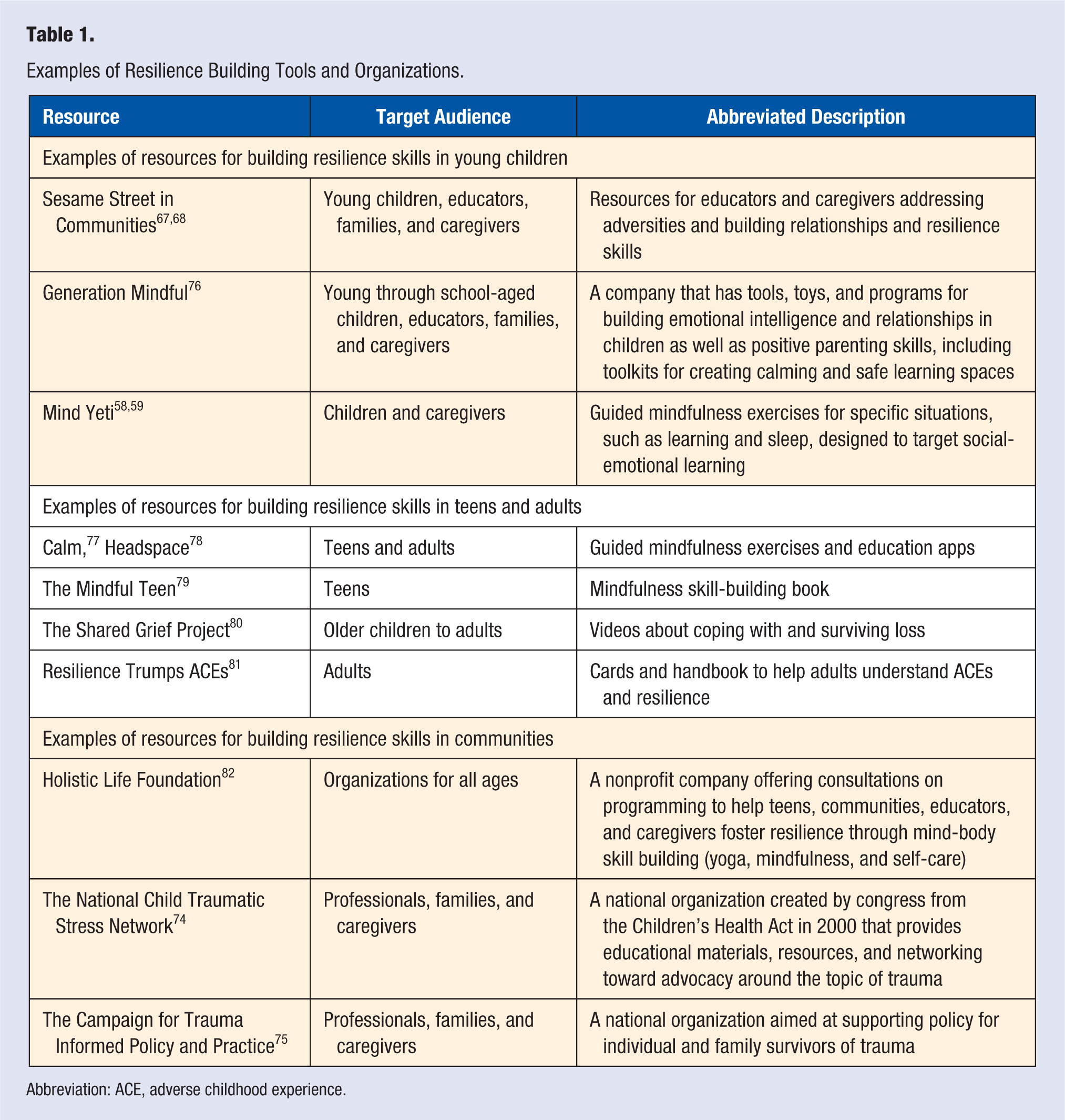
Abbreviation: ACE, adverse childhood experience.
Health Care Reform for Resilient Communities
Resilience needs to be manifested in communities as a whole. 51 To do this, funding to support such programing is needed through policy. Research has demonstrated that there may be a return of investment of up to 11 dollars for every 1 dollar spent on SEL, when including lifetime potential education and earnings, health, and a reduction in juvenile crime, and an 11% increase in academic achievement in students.69-71
In addition to education reform, the National Scientific Council on the Developing Child called for policy surrounding child welfare and care, maternal employment linked with public assistance, prenatal and newborn health care, and support for new parents. 72 Examples have been made from the early 1990s through the presence of policies that support such agendas, including a property tax allocation to children’s services in Vermont and a perinatal nurse-family program to prevent abuse that is connected with Medicaid plans in New York. However, more is needed, because SAMSHA suggests community resilience must infiltrate safety of communities; trustworthiness among community members and organizations, including law enforcement and the judicial system; opportunities for all; collaboration, peer, and family support; and embracing historical, gender, and cultural diversity. 73
Some organizations are allowing clinicians, educators, parents, and community members alike to join the advocacy toward combating ACEs and building resilient communities. The National Child Traumatic Stress Network, funded by SAMHSA and the Center for Mental Health Services, and the US Department of Health and Human Services and coordinated through UCLA and Duke University, 74 and the Campaign for Trauma Informed Policy and Practice 75 are two examples (Table 1).
Conclusion
ACEs have lasting effects on health through intergenerational behavioral and biological mechanisms. Resilience against the sequelae of ACEs can be fostered in children throughout life with healthy relationships. To influence chronic disease with lifestyle medicine, ACEs need to be addressed from bedside to communities. Clinicians can start with a trauma-informed care approach while pursuing advocacy and policy change at local and national levels.
Footnotes
Acknowledgements
This material was presented at the 2018 American College of Lifestyle Medicine conference. The author would like to acknowledge the work of Jessica Ratner and Marguerite (Cooper) Lloyd.
Author’s Note
Robin Ortiz has no financial disclosures. She has conducted research in ACEs and epigenetics and is a volunteer member of the executive board for Generation Mindful but holds no financial relationships. This manuscript is based on a speech given at the Annual Meeting of the American College of Lifestyle Medicine 2018 in Indiana, IN.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author has no financial disclosures. She has conducted research in ACEs and epigenetics and is a volunteer member of the executive board for Generation Mindful, but holds no financial relationships.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.