
Abstract
There is increased recognition that lifestyle factors, including nutrition, physical activity, emotional well-being and stress management, tobacco use, alcohol consumption, and sleep habits, are major determinants of health. There is a need to teach practicing physicians, medical trainees, and other health care providers how to perform a “lifestyle history.” This article proposes 13 screening questions physicians should consider exploring with patients. It provides the rationale and scientific evidence supporting each question and includes key lifestyle counseling points for clinicians to consider.
‘However, it is important to recognize that simply asking the questions conveys to the patient that the physician values and recognizes the role of lifestyle modification in reducing risk for chronic disease.’
Introduction
Medical education has traditionally focused on the management of acute and chronic disease rather than on disease prevention and health promotion through lifestyle changes. However, there has been increased recognition in recent years that lifestyle factors, including nutrition, physical activity, tobacco use, alcohol consumption, emotional well-being and stress management, and sleep habits, are major determinants of health. 1 A robust body of research has implicated modifiable lifestyle factors in the causes of many of the major chronic diseases, including cardiovascular disease, hypertension, cancer, and type 2 diabetes. 1 In one study, adhering to 4 healthy lifestyle factors (never smoking, having a body mass index less than 30 kg/m2, performing 3.5 h/wk or more of physical activity, and adhering to healthy dietary principles of high intake of fruits, vegetables, and whole-grain bread and low meat consumption) was shown to lower the risk of developing chronic disease by 78%. 2 This knowledge is important because the World Health Organization has predicted that by 2020, two-thirds of all diseases worldwide will be the result of lifestyle choices. 3
Although physicians would benefit from the help of allied health professionals with lifestyle counseling, access to these services is often limited. A national survey of 11 170 Canadian physicians working in an office or community clinic revealed that only 17% of them had access to a registered dietitian in their practice. 4 Availability of exercise physiologists and kinesiologists is even more scarce. 5 In light of this, there is a critical need for physicians to become knowledgeable in lifestyle medicine. 6 This has been defined as the “evidence-based practice of assisting individuals and their families to adopt and sustain behaviors that can improve health and quality of life.”7 (p202)
In a survey of 9 Canadian medical schools, most medical students reported a lack of comfort in discussing the role of nutrition in the treatment of disease. 8 More than 87% reported that undergraduate medical education should dedicate more time to teaching on nutrition. 8 In a recent study, primary care physicians identified time constraints and a lack of familiarity with lifestyle counseling as the main barriers to discussions around the primary and secondary prevention of childhood obesity. 9 A review of the websites of medical schools in the United States identified that more than half of the physicians trained in 2013 received no formal education in physical activity. 10
This article proposes 13 screening questions physicians can explore with their patients as part of the standard medical history (Table 1). It also outlines the rationale and scientific evidence behind each question. Key lifestyle counseling points are also included because the asking of the questions can serve as powerful stimulus for lifestyle medical patient education. However, it is important to recognize that simply asking the questions conveys to the patient that the physician values and recognizes the role of lifestyle modification in reducing risk for chronic disease.
Queen’s Lifestyle History.
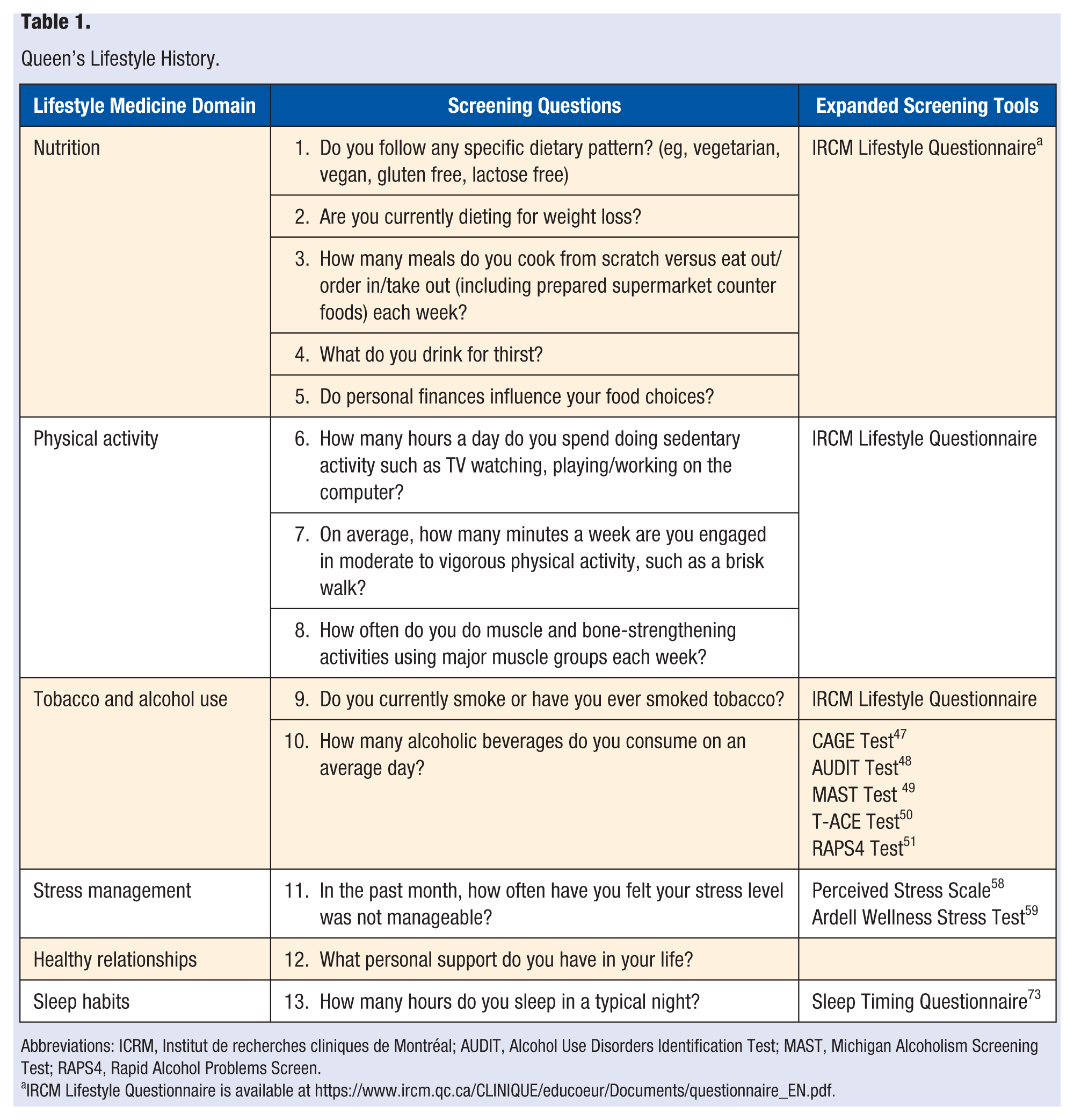
Abbreviations: ICRM, Institut de recherches cliniques de Montréal; AUDIT, Alcohol Use Disorders Identification Test; MAST, Michigan Alcoholism Screening Test; RAPS4, Rapid Alcohol Problems Screen.
IRCM Lifestyle Questionnaire is available at https://www.ircm.qc.ca/CLINIQUE/educoeur/Documents/questionnaire_EN.pdf.
The Lifestyle History represents an expansion of the traditional “Social History” and “Habits” of the clinical history to reflect the larger spheres of lifestyle medicine. The 13 screening questions are meant to quickly identify problem areas in lifestyle that can be later explored in more detail similar to other questions taught to medical students as part of the standard medical history. The authors recognize that it may be difficult to ask all 13 screening questions in a clinical encounter given time constraints, particularly because many of the questions are open-ended to invite reflection, discussion, and goal setting. Strategies to overcome this could include targeting lifestyle medicine questions to patients perceived to be at high risk for unhealthy lifestyle issues, asking a few lifestyle questions at ongoing clinical encounters with a patient, and/or scheduling a separate lifestyle medicine visit, potentially as a shared appointment with other members of the interdisciplinary lifestyle medicine team. Suggestions for expanded screening tools are also provided. An example of a lifestyle medicine note is provided in Figure 1.
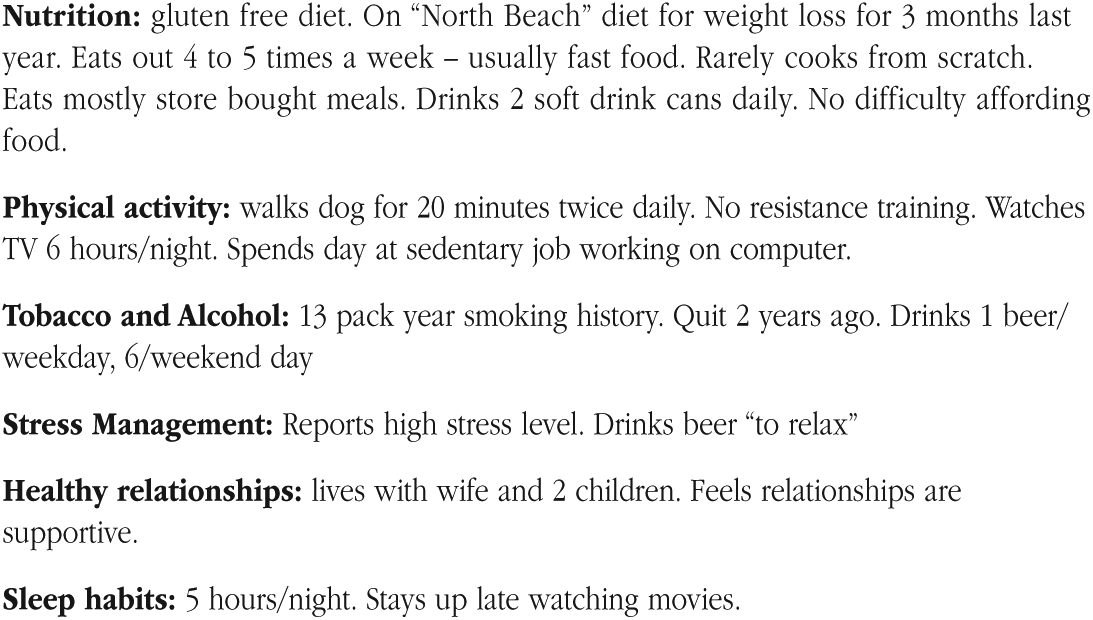
Sample lifestyle medicine history note.
Lifestyle History Questions
Do You Follow Any Specific Dietary Pattern? (eg, Vegetarian, Vegan, Gluten Free, Lactose Free)
Rationale
Nutrition science has recognized that there is no single dietary pattern that is optimal for everyone. 11 Moreover, the dietary pattern that is more appropriate for someone may change throughout their life. There has been a movement away from a “good food/bad food” approach toward a focus on overall dietary patterns. Recent research suggests that optimal dietary patterns are characterized by (1) high intake of fruits, vegetables, whole grains, and water as a preferred beverage; (2) moderate intakes of dairy products, plant-based proteins, poultry, fish, and fats; and (3) limited intakes of red meat, alcohol, refined grains, and sweets. 12
Canada’s Food Guide provides a pattern of healthy eating appropriate for most adults 13 ; however, many Canadians do not follow the recommendations, with the majority eating fewer than the recommended minimum of 5 daily servings of vegetables and fruits. 14 In recent years, it has become increasingly common for people to omit or limit foods from one or more food groups. Examples include omitting milk and alternatives as a result of perceived lactose intolerance and limiting grains for perceived gluten intolerance or to follow a low-carbohydrate diet. Most people should be encouraged to eat a balanced diet and not eliminate entire food groups. Consider referring patients avoiding one or more food groups to a registered dietitian to ensure that missing nutrients are obtained through other foods and/or supplements. A more comprehensive screening tool prepared by Institut de recherches cliniques de Montreal (IRCM) to assess eating, physical activity, and smoking habits is available at https://www.ircm.qc.ca/CLINIQUE/educoeur/Documents/questionnaire_EN.pdf.
Useful Counseling Points
Eat a variety of nutrient-rich foods, including whole grains, lean protein (eg, plant-based proteins), fruits and vegetables, and low-fat or fat-free dairy. Eat less food high in solid fats, added sugars, and sodium (salt). 14
Make as much of your grain products whole grain as possible each day. Eat a variety of whole grains, such as barley, oats, quinoa, and wild rice. Enjoy whole grain breads, oatmeal, or whole wheat pasta. 15
Try to eat 6 to 8 servings of fruits and vegetables in a variety of colors each day. Choose fresh, frozen, low-sodium canned, or dried options. 13
Choose lean sources of protein: have meat alternatives such as beans and peas (kidney, pinto, black or white beans; split peas; chickpeas; hummus), soy products (tofu, tempeh, veggie burgers), and unsalted nuts and seeds. When choosing animal proteins, use low-fat cuts of beef or pork and skinless chicken or poultry. Eat at least 2 servings of fish each week. Use cooking methods such as roasting, baking, or poaching that require little or no added fat, and when using oils, choose olive, vegetable, or canola oils. 15
Use the Harvard Healthy Plate to learn more about portion sizes and how to eat a balanced diet (available at http://www.health.harvard.edu/healthy-eating-plate), but generally at least half of every meal should be vegetables, and the remainder should be divided evenly between grains and a protein source.
A registered dietitian can assist patient how to eat well with a specific dietary pattern.
Are You Currently Dieting for Weight Loss?
Rationale
In 2014, 40% of Canadian men and 27.5% of women reported height and weight that classified them as overweight; 20.2% of Canadians aged 18 years and older reported figures that would classify them as obese. 16 As a result, excess energy intake is a common nutritional concern. Although many adults consume too many calories, they may not be consuming sufficient macronutrients or micronutrients, particularly if they are making nutrient-poor calorie-dense choices or omitting entire food groups as part of a fad diet. As the use of fad diets is common, physicians need to be familiar with the popular ones.
Useful Counseling Points
How Many Meals Do You Cook From Scratch Versus Eat Out/Order In/Take Out (Including Prepared Supermarket Counter Foods) Each Week?
Rationale
Nutrient density is a useful concept to evaluate how healthy a food is. Nutrient-dense foods are defined as foods that provide substantial amounts of vitamins and minerals and have relatively few calories. 19 Energy-dense foods provide more energy in a given quantity of food. Patients should be encouraged to get more nutrients from their calories by minimizing intake of energy-dense, nutrient-poor foods because consumption of these foods is known to be associated with increased risk of obesity and chronic disease risk. 20 Fast and prepared foods are typically energy dense and associated with excessive portion size, and their consumption is contributing to the escalating rates of overweight and obesity in North America.17,21
Useful Counseling Points
What Do You Drink for Thirst?
Rationale
Sugar-sweetened beverages, such as soft drinks, fruit drinks, sports drinks, energy drinks, iced tea, and lemonade are common fluid sources. These beverages provide calories but few or no nutrients; also, calories from fluids have been proposed to be less satiating and may lead to calorie overconsumption. 22 Their intake has been linked to obesity. 23
Useful Counseling Points
Do Personal Finances Influence Your Food Choices?
Rationale
Food insecurity exists within a household when one or more members do not have access to the variety or quantity of food that they need because of financial strain. 24 About 8% of adults and 5% of children experienced food insecurity in Canada in 2012. 25 Physicians need to be aware of the importance of food insecurity as a determinant of health. The most common strategy to address food insecurity in Western countries relies on food distribution primarily in the form of food banks 26 ; however, physicians need to be advocates for more comprehensive strategies, including government commitments to living wages and welfare, taxation reforms, and new approaches to agricultural food and nutritional policies. 27
Useful Counseling Points
Become knowledgeable of food distribution resources in your community (eg, food banks, soup kitchens, community gardens, good food baskets, school breakfast/lunch programs). 26
How Many Hours a Day Do You Spend Doing Sedentary Activity Such as TV Watching, Playing/Working on the Computer?
Rationale
The World Health Organization has identified physical inactivity as the fourth leading contributor to global mortality, with an estimated 3.2 million annual attributable deaths globally. 28 In addition, physical inactivity is estimated to be the main driver for approximately 21% to 25% of breast and colon cancers, 27% of diabetes, and approximately 30% of ischemic heart disease burden. 28 Common sedentary activities include television watching, playing video/computer games, car travel, and reading. Many modern occupations involve prolonged sitting. A recent 12-year study of 17 000 Canadians found that people spending 50% or more of their time sitting had higher mortality rates, even after controlling for age, smoking, and physical activity levels. 29
The Canadian Sedentary Behavior Guidelines advice limiting how much time children spend being sedentary in front of screens or in vehicles. 30 They recommend that children <2 years have no screen time and children 2 to 4 years old should limit screen time to less than 1 h/d. Although there are no sedentary time guidelines for adults, they should be encouraged to limit sedentary behavior and include physical activity breaks during sedentary time.
Useful Counseling Points
Try to limit sedentary behaviors that involve very little physical movement while awake, such as sitting or reclining while watching television or playing with nonactive electronic devices such as video games, tablets, computers, or phones.
If your work is sedentary in nature, organize physical activity breaks throughout your day.
On Average, How Many Minutes Per Week Are You Engaged in Moderate to Vigorous Physical Activity, Such as a Brisk Walk?
Rationale
Physical activity is movement that increases heart rate and breathing. It requires energy expenditure by skeletal muscle. Like appropriate nutrition, physical activity enhances health and well-being and decreases risk factors for chronic diseases.31,32 Recent research indicates that for the primary prevention of diabetes and secondary prevention of coronary heart disease, stroke, and heart failure, physical activity is as effective as, or more effective, than many drug interventions. 31
On a scale relative to an individual’s personal capacity, moderate-intensity physical activity is usually a 5 or 6 on a scale of 10. As a rule of thumb, persons doing moderate-intensity activity can talk, but not sing their favorite song, during the activity. Heart rate should be 50% to 70% of maximum heart rate. 33 On a scale relative to an individual’s personal capacity, vigorous-intensity physical activity is usually a 7 or 8 on a scale of 10. If a patient is doing vigorous-intensity activity, he or she will not be able to say more than a few words without pausing for a breath. Heart rate will have increased to 70% to 85% of maximum heart rate. 33
Canadian guidelines for physical activity have been developed by the Canadian Society for Exercise Physiology (CSEP) and provide advice on the minimum physical activity that Canadians need to engage daily for maintaining health and well-being. 30 Before starting a new exercise program, participants may use a self-guided questionnaire such as the Physical Activity Readiness Questionnaire to alert those with elevated risk to consult a health care provider before participation. 34
Useful Counseling Points
Explore barriers and problem solve solutions to participation in physical activity. Commonly perceived barriers include lack of time; lack of energy or fatigue; lack of interest or motivation; long-term illness, injury, or disability; cost; feeling ill at ease or uncomfortable; fear of injury; and lack of physical skill. 30
Encourage patients to do at least 150 minutes of moderate- to vigorous-intensity aerobic physical activity per week, in bouts of 10 minutes or more. 30
Brisk walking is an easy activity to incorporate for most people. 30
How Often Do You Do Muscle and Bone-Strengthening Activities Using Major Muscle Groups Each Week?
Rationale
Resistance training has been shown to increase lean muscle mass and muscle strength,35,36 and bone mineral density reducing risk of osteoporosis.37-39 In individuals with diabetes, it has been shown to improve glycemic control. 40 The CSEP guidelines provide advice on frequency of muscle and bone-strengthening activities. They also provide advice on including physical activities to enhance balance and prevent falls in individuals older than 65 years. 30
Useful Counseling Point
Try to add muscle and bone-strengthening activities using major muscle groups at least 2 d/wk. 30
Do You Currently or Have You Ever Smoked Tobacco?
Rationale
Cigarette smoking is the leading preventable cause of mortality. 41 The major causes of tobacco-related mortality are atherosclerotic cardiovascular disease, lung cancer, and chronic obstructive pulmonary disease. 42 Screening patients for tobacco use and providing smokers with behavioral counseling and pharmacotherapy to stop smoking has been identified as one of the most valuable preventive services in health care. 43
Useful Counseling Points
How Many Alcoholic Beverages Do You Consume on an Average Day?
Rationale
Excessive alcohol intake is associated with increased mortality as well as a number of adverse health and social consequences. 45 Unhealthy alcohol use has been identified as the fourth leading cause of preventable death in the United States. 46 A variety of validated screening tests for problem drinking exist, including the CAGE Test, 47 AUDIT Alcohol Consumption Questions, 48 Michigan Alcoholism Screening Test (MAST), 49 T-ACE, 50 and the Rapid Alcohol Problems Screen (RAPS4). 51
Useful Counseling Points
According to the Dietary Guidelines for Americans 2015-2020, the US Department of Health and Human Services, and US Department of Agriculture, moderate drinking is defined as up to 1 drink per day for women and up to 2 drinks per day for men. 52
According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA), for men up to age 65 years, drinking at low risk for developing an alcohol use disorder is defined as no more than 4 drinks on any single day and no more than 14 drinks per week. 53 For women, who tend to have lower volumes of distribution, and men older than 65 years, lower-risk alcohol use is no more than 3 drinks on any single day and no more than 7 drinks per week. 53
In the Past Month, How Often Have You Felt That Your Stress Level Was Not Manageable?
Rationale
Stress is a common patient complaint; 60% to 80% of primary care visits may have a stress-related component. 54 Meta-analyses have indicated that chronic stress is associated with reduced quality of life 55 and increased cardiovascular risk. 56 However, one study of more than 33 000 primary care office visits found that only 3% included stress management counseling. 57 It was the least common type of counseling, compared with counseling about nutrition (16.8%), physical activity (12.3%), weight reduction (6.3%), and tobacco cessation (3.7%) The Perceived Stress Scale (10 questions) 58 and the Ardell Wellness Stress test (25 questions) 59 are 2 tools that can be used to screen for stress in more depth.
Useful Counseling Points
What Personal Support Do You Have in Your Life?
Rationale
Several studies have shown that people who have satisfying relationships with family, friends, and their community are happier, have fewer health problems, and live longer.63-65 Conversely, a relative lack of social ties is associated with depression and later-life cognitive decline as well as increased mortality.66,67 One meta-analysis, which examined data from more than 309 000 people, found that lack of strong relationships increased the risk of premature death from all causes by 50%. 67 In view of this, the patient’s personal support system should be explored.
Useful Counseling Points
How Many Hours Do You Sleep in a Typical Night?
Rationale
A sufficient amount of sleep is essential for optimal physical health. The American Academy of Sleep Medicine and Sleep Research Society recommends that those aged 18 to 60 years should sleep 7 or more hours per night on a regular basis for optimal sleep health. 68 Similarly, the National Sleep Foundation consensus report specifies that 7 to 9 hours is recommended for adults aged 18 to 64 years and 7 to 8 hours is recommended for those 65 years of age and older. 69 Infants, children, and teenagers require substantially more sleep than adults. 69 Insufficient sleep is a common problem. According to data from the National Health Interview Survey, nearly 30% of US adults reported sleeping 6 or fewer hours per day, and rates are even higher among younger adults, racial and ethnic minorities, and patients with low socioeconomic status. 70 Short sleep duration has been associated with increased risk of cardiovascular disease, obesity, and all-cause mortality.71,72
The Sleep Timing Questionnaire is a tool that can be used to explore sleep habits in more depth. It includes questions about habitual wake times and bedtimes on weekdays and weekends, similar to those obtained from a sleep diary. 73
Useful Counseling Points
Stick to the same sleep schedule, even on the weekends. 68
Exercise daily. 68
Maintain a sleep environment conducive to sleep (eg, comfortably cool temperature, reduction of environmental light and noise). 68
Wind down with quiet activities that may promote sleep, such as reading with a dim light. 68
If you cannot sleep, do not look at a clock. Go into another room and do something relaxing until you feel drowsy enough to fall asleep again. 68
Conclusion
Given the global pandemics of chronic disease and the role of modifiable health behaviors in their prevention, lifestyle history needs to become an essential part of the standard medical history. Instruction on appropriate screening questions and counseling points should become a standard component of the curriculum of undergraduate clinical skills training and clinical encounters. A total of 13 lifestyle history standard screening questions have been proposed in this article to help identify unhealthy behaviors and replace them with ones that promote health. The number has been kept small to ensure their adoption, recognizing the reality of common time constraints in medical history taking. However, the authors hope that as medical students, physicians, and other health care providers become more comfortable and competent in taking a lifestyle history and with continuity of care, the breadth and depth of questioning and counseling can steadily expand.
Finally, the recommendations outlined above for lifestyle and dietary modifications would best be approached with motivational interviewing techniques with the goal of developing specific, measurable, achievable, realistic, and trackable (SMART) goals with evolving targets and appropriately timed follow-up to produce sustainable and effective lifestyle behavior change. 74
It can also act as an important gateway to involve other members of the interdisciplinary lifestyle medicine team, including registered dietitians, exercise physiologists/exercise coaches/personal trainers/kinesiologists, psychologist/licensed therapists/health coaches, nurses, pharmacists, and lifestyle medicine physician specialists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.