
Abstract
‘Indeed, when feedback was given frequently about behavioral progress, researchers found that individuals tended to be more adherent to diet and physical activity goals.’
Introduction
Behavioral weight loss interventions have shown moderate success in helping individuals lose weight, 1 and recently, increased numbers of individuals report attempting to lose weight. 2 Despite positive intervention outcomes, sustained weight loss maintenance continues to be a challenge. Researchers have identified continued high levels of moderate to vigorous physical activity (MVPA) following active weight loss periods as one strategy associated with successful weight regain prevention.3,4 However, effective strategies that promote regular MVPA in order to encourage weight loss maintenance are still needed. Furthermore, regular MVPA following active intervention periods tends to decline over time,5,6 suggesting a need for improved intervention design and monitoring that results in sustained behavioral effects.
Behavioral maintenance work has identified earlier behavior as a strong predictor of future behaviors.7,8 Therefore, if individuals who are not engaging in interventions can be identified sooner, augmentation or additional approaches can be offered to better support the desired behavior change. Using behavior tracking logs to identify these individuals in need of supplemental support is one strategy that may result in increased behavior adoption and maintenance. Tracking dietary intake and MVPA using daily diaries has previously been shown to be an effective weight loss tool. 9 In addition to increasing behavioral awareness for those participating in interventions, this tool presents opportunities for interventionists to monitor participant progress and offer feedback and support. Indeed, when feedback was given frequently about behavioral progress, researchers found that individuals tended to be more adherent to diet and physical activity goals. 9 However, these findings have been limited primarily to 6-month and 12-month studies. 10 Additionally, although behavioral self-monitoring has been identified as a correlate of successful weight loss maintenance, 11 the impact of self-monitoring on weight loss maintenance has been limited to broad and self-reported adherence measures. 10 Work having longer behavioral follow-up and objective self-monitoring characteristics is necessary to better understand what indicators should be monitored to identify disengaged individuals and when intervention augmentation might be most effective.
Recent technological advancements offer easier and more convenient ways for interventionists to survey individuals’ weight loss behavior tracking through websites and mobile applications. These websites and applications designed for tracking physical activity and diet offer convenient and accessible data capture and storage. Individuals can more easily track behaviors using cell-phone applications that they can access most places. These behavioral tracking applications have differing implications for intervention depending on the behavior of interest. For example, with dietary tracking, those who do not track dietary intake are likely not being fully adherent to recommendations; however, they are assumed to be engaging in some sort of dietary intake. 12 Conversely, for MVPA tracking, it is assumed that individuals who are not self-monitoring physical activity are also not engaging in any MVPA at all. 10 Therefore, electronic data capture methods may make it easier for interventionists to identify individuals who are successfully adopting MVPA or not following adoption. This process of identifying individuals through gaps in electronic tracking logs has the potential to better support MVPA initiation or lapse recovery in order to maintain high levels of MVPA over time and improve weight loss maintenance. However, indicators of behavioral engagement and adherence using self-monitoring adherence have yet to be examined.
To begin to evaluate this potential method for identifying individuals who show signs of behavioral disengagement during weight loss interventions, the association of physical activity self-monitoring characteristics with weight loss maintenance and long-term MVPA must first be evaluated. However, few studies have examined physical activity self-monitoring behavior, and to our knowledge, no studies have examined the association of self-monitoring with weight and physical activity out to 24 months. The purpose of this study was to examine the effect of physical activity tracking behavior during a year-long behavioral weight loss intervention on MVPA and weight out to 24 months in order to inform efforts to enhance engagement in the intervention period before significant adherence lapses occur. We hypothesized that later onset of physical activity self-monitoring as well as earlier and more frequent gaps in tracking during intervention would be associated with lower reported physical activity levels and higher measured weight at 24-month follow-up.
Methods
A secondary data analysis was conducted using data from the Tracking Study, a randomized trial comparing the efficacy of 3 different weight-tracking conditions during a nonpharmaceutical lifestyle weight loss program. 13 Participants were randomized to daily, weekly, or no self-weighing for the duration of a 12-month intervention with an additional 12-month measurement-only follow-up. Participants were recruited from the Minneapolis–St Paul metropolitan area in 3 waves beginning in July 2012 and ending in August 2013. Participants were recruited via online advertisements, flyers placed in workplaces and office buildings near the university and in community centers, as well as newspaper and radio ads. Study measurement visits occurred at baseline and at 6-month, 12-month, 18-month, and 24-month time points. This study was approved by the University of Minnesota Internal Review Board.
Intervention activities included in-person group sessions comprising lessons, activities, discussions, worksheets, and handouts delivered by trained nutritionists at the University of Minnesota. Groups met weekly for 6 months, biweekly for 2 months, and monthly for 4 months. Topics of each meeting included behavioral lessons such as goal setting, planning, and problem solving as well as more specific nutrition and physical activity topics. Participants were instructed to set a goal of achieving at least 250 minutes of purposeful MVPA per week. They were instructed to reduce caloric intake, based on their baseline height and weight, but to no less than 1200 kilocalories, in order to lose 1 to 2 lbs per week. Additionally, instructions included reducing fat intake to no more than 30% of daily caloric intake. Specific sessions covered strategies to meet these goals, including topics on including low-fat substitutions, cooking demonstrations, stimulus control, and meal planning. 13 All groups met weekly and had the same lessons and assignments regardless of study arm.
Participants
A full description of the study sample and intervention protocol can be found elsewhere. 13 Briefly, 339 men and women aged 18 to 64 years with body mass index (BMI) 25 to 40 kg/m2 were enrolled in the study. This cohort was 64.9% female and 46.5 (±10.2) years of age, had a BMI of 33.0 kg/m2 (±3.6) on average, and was 86.4% white. Furthermore, 67.9% of participants were married, and 63.7% had at least a college degree. Additionally, participants had to verify that they had home wireless internet for scale connectivity and had no recent weight loss greater than 10 pounds, no history of bariatric surgery, and no significant health concerns. Women could not be pregnant or breastfeeding and could not be planning to become pregnant for the duration of the study. 13 The full study sample was included for this analysis.
Behavior Self-monitoring
Physical activity and dietary tracking logs were kept during the 12-month weight loss intervention. Self-monitoring logs were completed using paper diaries for participants in the no-weighing condition to avoid prompts for self-weighing by the commercial electronic tracking application. Those in the daily and weekly weighing conditions were given a web-based and mobile tracking application Lose It! (FitNow, Inc, Boston, MA). Paper logs were collected at each group meeting and intervention staff recorded the number of days that physical activity and diet was tracked. For those using electronic tracking, the Lose It! accounts were configured to email activity and dietary records directly to the interventionists each week. Interventionists then printed the logs to record the number of days participants had self-monitored their diet and physical activity and give feedback to participants at the in-person group sessions. Participants were instructed to only include intentional exercise in their physical activity tracking logs. Thus, a primary reason for any gaps in physical activity tracking was the absence of engagement in MVPA.
Using the self-monitoring logs, study staff recorded the number of days that MVPA was tracked per week as well as the number of days that diet was tracked. When recording MVPA tracked for data collection, study staff did not count less-exertive, task-focused activities such as gardening or housework as a bout of MVPA. The in-person sessions focused on increasing physical activity above and beyond what participants were already engaging in to produce and support sustained weight loss. Thus, participants were instructed to exclude these activities from their activity logs. Total adherence was defined as the total number of days of recorded self-monitoring during the 12-month intervention period.
Gaps in physical activity tracking were defined as ⩾1 week of no activity logging. Using these gaps, 4 self-monitoring characteristics, including total number of tracking gaps, average length of tracking gaps, late onset of tracking, and week of first gap in behavior tracking, and 4 specific gap lengths were defined. The total number of gaps for each participant was recorded as well as the length of each gap. Average length of the gaps for each participant was then calculated. Late onset of self-monitoring was defined as a binary variable. By the second week of the intervention, individuals who had zero days reported of MVPA self-monitoring based on their weekly logs were categorized as late onset self-reporting; individuals who had at least 1 day of MVPA logged within the second week were categorized as regular onset of self-reported MVPA tracking. Short gaps (1-4 consecutive weeks), medium gaps (5-8 consecutive weeks), long gaps (9-12 consecutive weeks), and extra-long gaps (>12 consecutive weeks) were defined by the number of times participants had gaps of these sizes. These definitions are similar to those in previous literature that examines the effects of long and short gaps of weight control behaviors on weight loss 14 and have been expanded to include more variability in this observational sample.
Dietary self-monitoring was tracked using the same logs as physical activity tracking and was also collected, reviewed, and recorded by intervention staff at each group meeting. Gaps in dietary tracking were defined as zero logged calories for at least 1 week during the active intervention period. Because of similar and contemporaneous tracking of diet and activity, dietary tracking characteristics were defined in the same way as the physical activity self-monitoring characteristics. Separate models to determine the association between dietary tracking behavior characteristics and weight were examined to account for any confounding that may affect weight change resulting from dietary self-monitoring.
Outcomes
Physical Activity
MVPA was measured at each measurement visit by the self-reported Paffenbarger Activity Questionnaire (PAQ). 15 The PAQ comprises both closed and open-form questions that assess activity over the past week. Both closed and open-form questions are used to measure activity caloric expenditure. Two separate questions assessed distance walked and flights of stairs climbed. Weekly kilocalorie (kcal/wk) expenditure from reported moderate to vigorous activities was calculated based on PAQ scoring. 15 This measure performed sufficiently in validation studies compared with VO2 maximal output (r = 0.60; P < .05). 16 A random subset of participants in this sample (n = 174) was randomized to wear Actigraph GT1M accelerometers for 7 days at baseline and 12 months to compare the validity of the self-report measure. Spearman correlations of questionnaire-measured MVPA with accelerometer-measured MVPA based on Freedson cut points 17 showed acceptability at baseline (r = 0.27; P < .01) that improved at 12 months (r = 0.56; P < .01). In this analysis, MVPA was represented by the calculated continuous caloric expenditure variable (kcal/wk).
Weight
Trained staff using Tanita digital scales measured weights at each study visit. Weights at 24 months, accounting for previous weight measurements (at baseline, 6, 12, and 18 months), were compared across self-monitoring variables to capture weight change during the entire study. Weight outcomes were treated continuously.
Covariates
Demographic variables were self-reported at baseline. They included age, gender, race, marital status, and level of education. Race (white or other), marital status (married or not), and education level (college degree or less) were collapsed to binary variables because of the large number of highly educated adults in this sample. Treatment condition (daily, weekly, or no weighing) was also included in adjusted models and treated as a categorical covariate.
Analysis
Analyses were performed in SAS version 9.4 (Cary, NC). Generalized estimating equation (GEE) modeling was used to examine the association between physical activity self-monitoring characteristics and reported MVPA participation measured over the 24-month follow-up. Separate models were used to examine the associations of increases in total number of gaps, average length of gap, late onset, week of first gap, and specified gap sizes with MVPA. The GEE model accounts for correlation of MVPA for each individual measured over time. Furthermore, GEE can handle missing data and uses information from all individuals with some outcome data. An identity link function with a normal distribution was specified for the continuous MVPA outcome. All models adjusted for demographic covariates and used an independence working correlation structure.
GEE models were also used in the analysis of the association of self-monitoring characteristics and weight at 24-month follow-up. Similarly, a normal distribution with the identity link was specified. Because of the correlation between MVPA and dietary tracking measures (r = 0.30-0.91), models assessing the association and self-monitoring of MVPA and diet were analyzed separately. Finally, models examining the interaction of dietary self-monitoring and MVPA self-monitoring characteristics on weight were also evaluated.
Total adherence, measured by total number of self-monitoring days, was also examined as a covariate for the specific gap lengths. However, because of the high correlation between total adherence and gap lengths as well as its strong association with weight, this measure obscures the results and was, thus, left out of the models.
Results
Visual plots of MVPA and dietary self-monitoring of participants are shown in Figures 1 and 2. Weeks are colored black to indicate self-monitoring was performed that week. Weeks are colored white to indicate no self-monitoring. Self-monitoring was first recorded and evaluated during the second week to allow participants to receive and become familiar with tracking logs. Descriptive statistics for self-monitoring, reported MVPA calorie expenditure, weight change, and demographic characteristics are presented in Table 1. Throughout the first year of intervention, participants had on average 3.7 (±2.6) gaps in MVPA tracking and 2.7 (±2.2) gaps in tracking of dietary behavior (r = 0.59). Gaps in MVPA self-monitoring (Table 1) lasted an average of 11.6 (±15.4) weeks, whereas gaps in dietary self-monitoring lasted 11.0 (±15.1) weeks on average (r = 0.91).
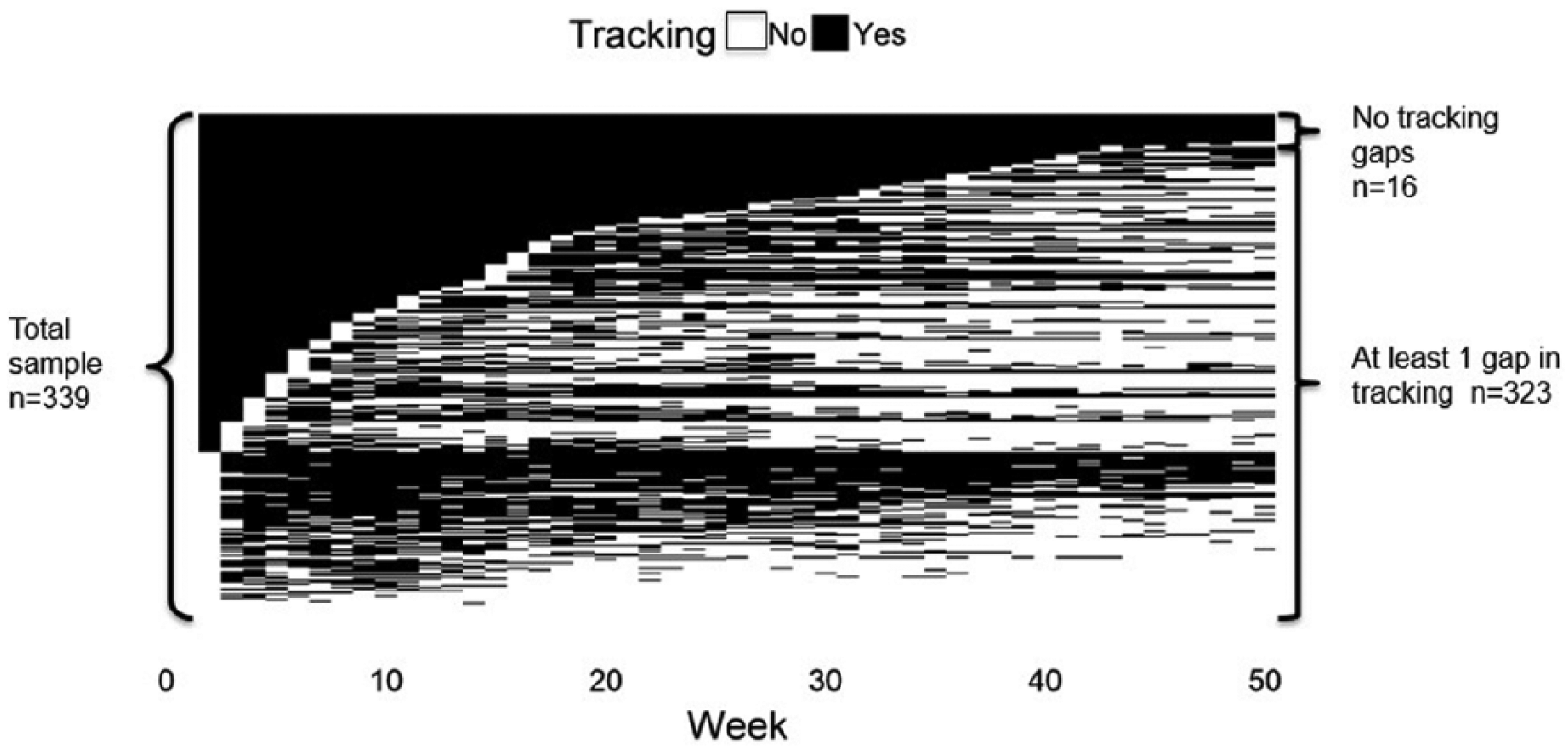
Participant physical activity (PA) self-monitoring during active weight loss intervention. Each row of the image represents 1 participant’s weekly PA tracking data. Participants were sorted by week of first gap in tracking followed by number of weeks tracked. The weeks when PA was tracked are coded in black; the weeks when PA was not tracked are coded in white.
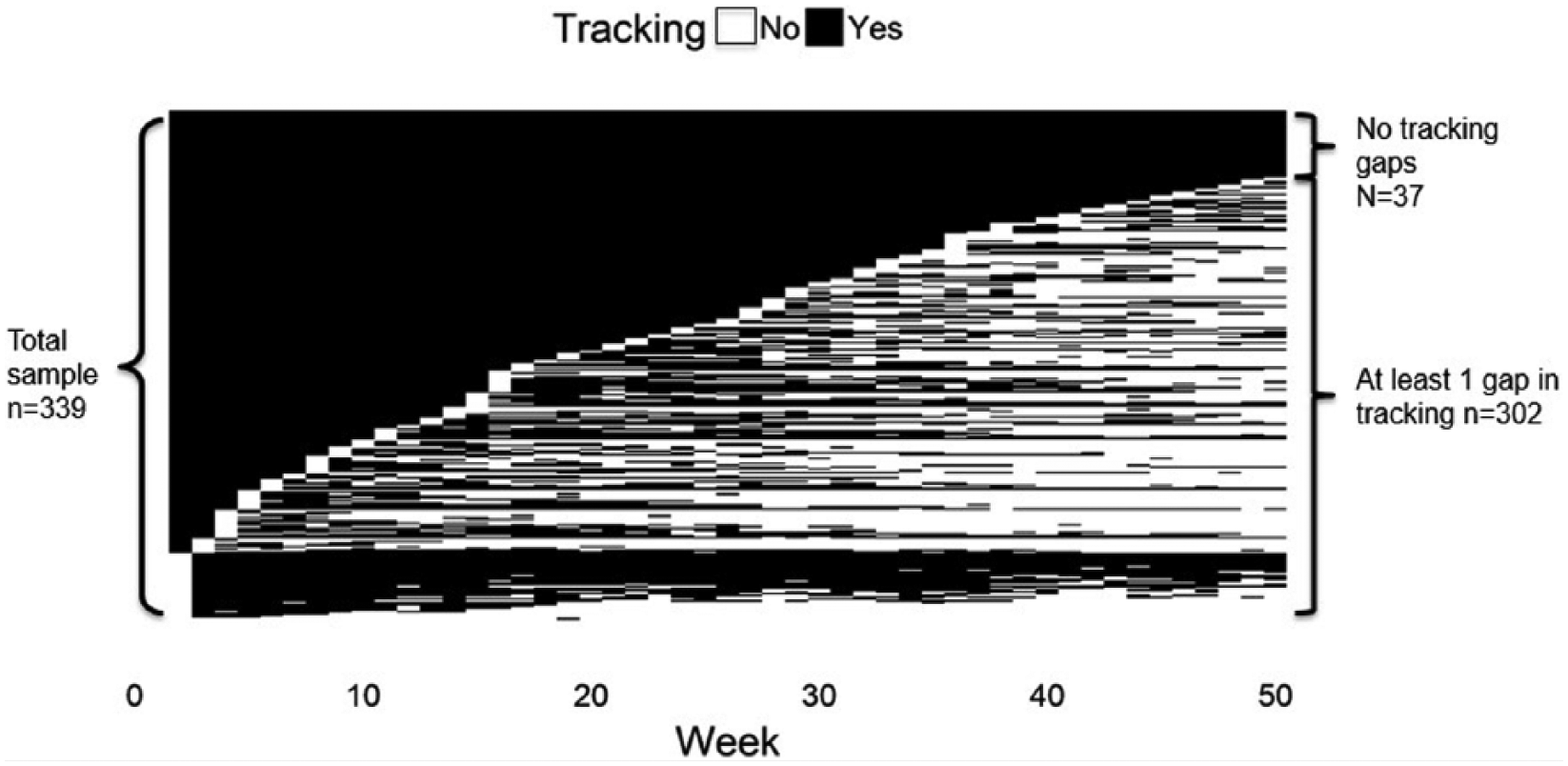
Participant dietary self-monitoring during active weight loss intervention. Each row of the image represents 1 participant’s weekly physical activity tracking data. Participants were sorted by week of first gap in tracking followed by number of weeks diet was tracked. The weeks when diet was tracked are coded in black; the weeks when diet was not tracked are coded in white.
Weight Change, Physical Activity, and Self-monitoring Characteristics of Participants.
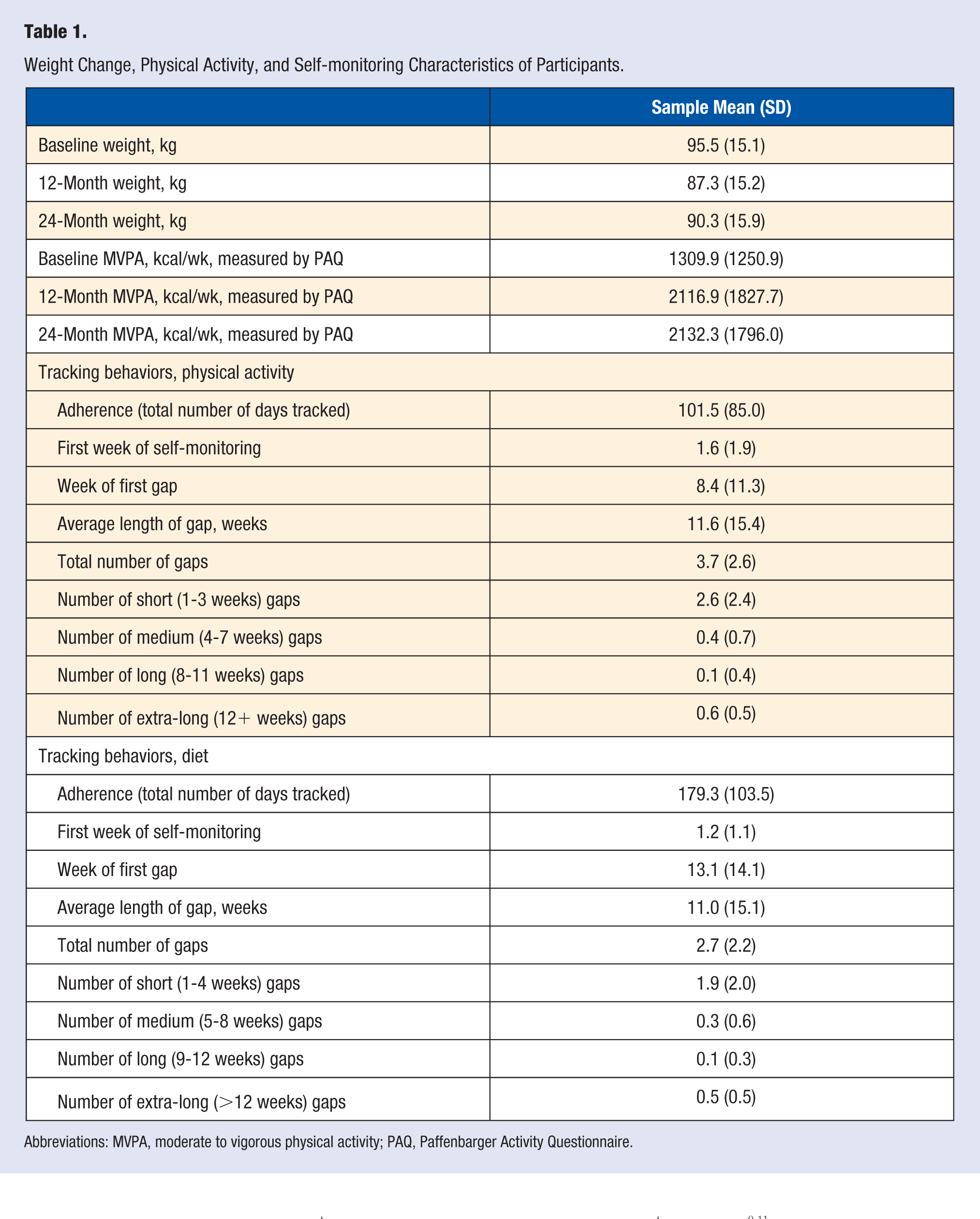
Abbreviations: MVPA, moderate to vigorous physical activity; PAQ, Paffenbarger Activity Questionnaire.
Self-monitoring and MVPA
The results of the GEE analyses of physical activity self-monitoring characteristics on self-reported MVPA are presented in Table 2. Late onset of MVPA tracking was associated with lower physical activity. Participants who were not tracking by the second week of the intervention reported 323.7 kcal/wk (standard error [SE] = 153.6; P = .04) less MVPA at 24 months compared with those who began tracking earlier. Furthermore, ongoing consistent tracking in the study (ie, later appearance of the first gap in MVPA self-monitoring) was significantly associated with increased reported MVPA; with every additional week of consistent tracking, reported MVPA increased by 25.0 kcal/wk (SE = 7.8; P < .01) at 24 months. Additionally, increases in short (1-4 weeks), medium (5-8 weeks), and long (9-12 weeks) length gaps were not significantly associated with MVPA achievement. However, extra-long (>12 weeks) length gaps were significantly associated with decreased reporting of weekly MVPA by 544.3 kcal (SE = 124.5; P < .01) at 24 months.
Association of PA Tracking Behaviors and Reported MVPA (kcal/wk) at 24 Months. a
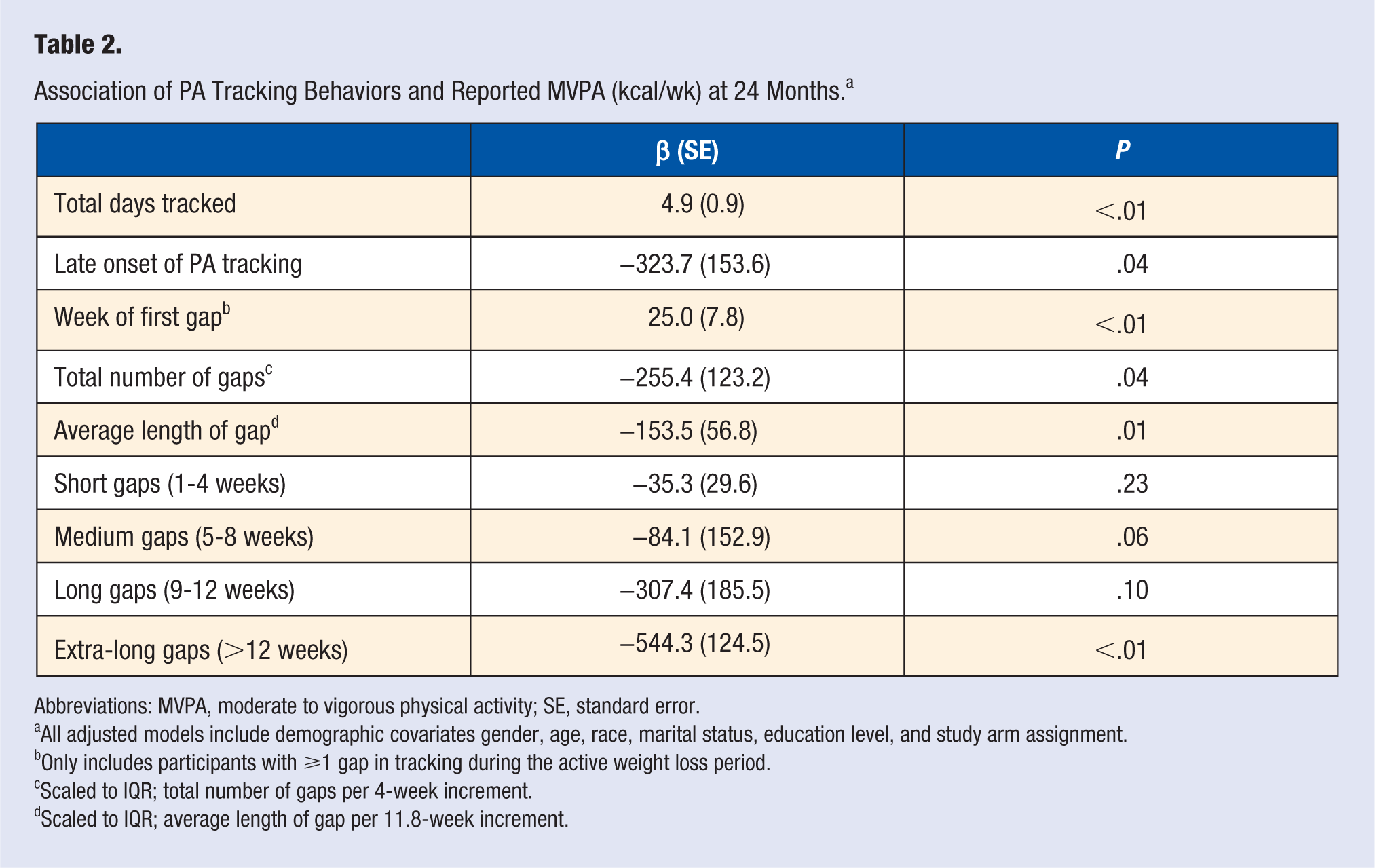
Abbreviations: MVPA, moderate to vigorous physical activity; SE, standard error.
All adjusted models include demographic covariates gender, age, race, marital status, education level, and study arm assignment.
Only includes participants with ⩾1 gap in tracking during the active weight loss period.
Scaled to IQR; total number of gaps per 4-week increment.
Scaled to IQR; average length of gap per 11.8-week increment.
Self-monitoring and Weight
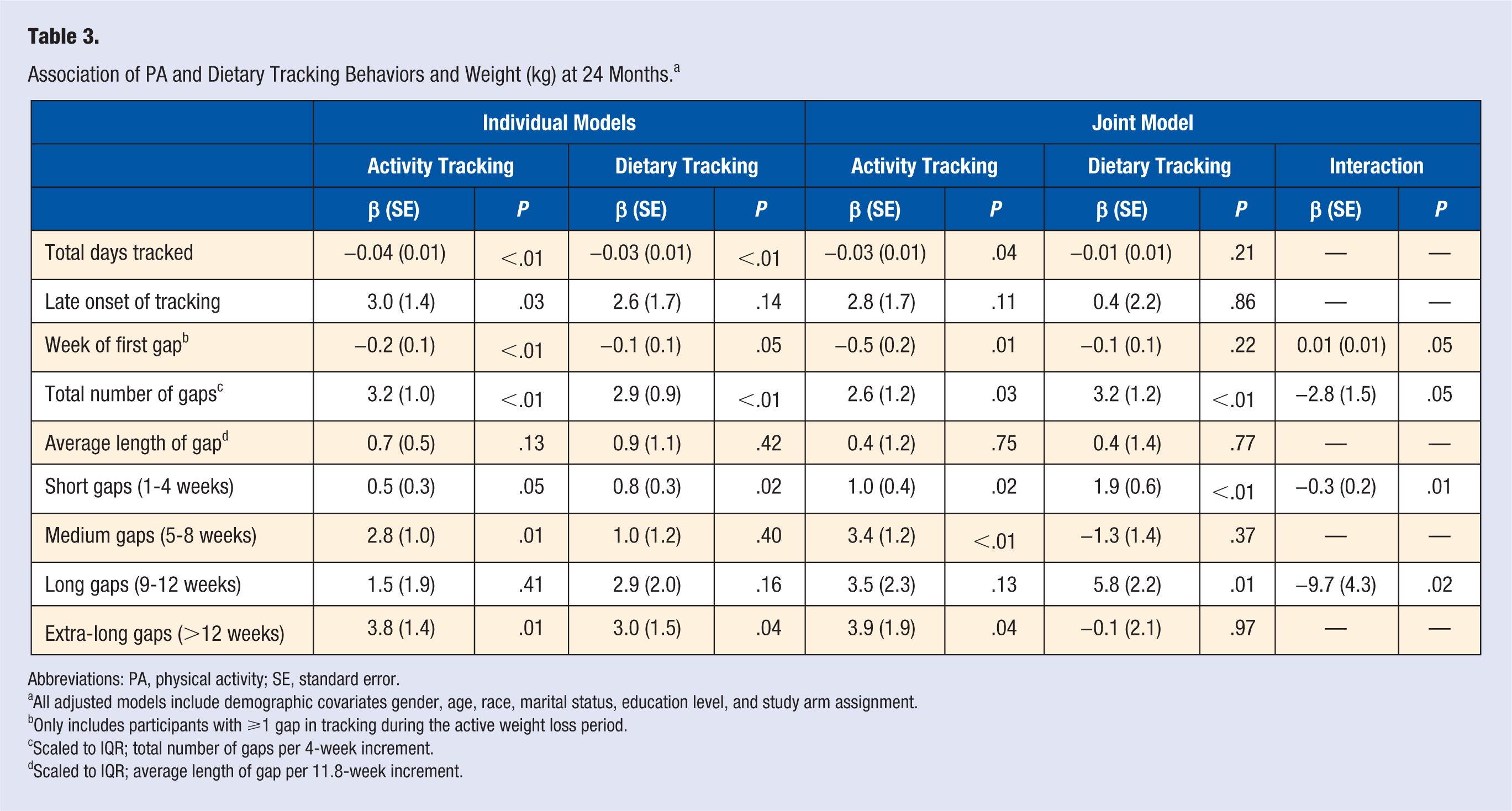
Independent models examining associations of physical activity and dietary tracking separately with 24-month weight are reported as well as a joint model (Table 3). Effect measure modification was reported when present in the joint models. In the individual models, late onset of physical activity tracking was associated with higher weight (Risk Difference (RD) = 3.0 kg; SE = 1.4; P = .03). Results of the joint model suggest that after controlling for late onset of dietary tracking, late onset of physical activity tracking was still statistically significantly associated with increased weight.
Association of PA and Dietary Tracking Behaviors and Weight (kg) at 24 Months. a
Abbreviations: PA, physical activity; SE, standard error.
All adjusted models include demographic covariates gender, age, race, marital status, education level, and study arm assignment.
Only includes participants with ⩾1 gap in tracking during the active weight loss period.
Scaled to IQR; total number of gaps per 4-week increment.
Scaled to IQR; average length of gap per 11.8-week increment.
Week of first gap for physical activity tracking evaluated independently was significantly associated with weight, suggesting that as the week of the first gap in tracking increased, weight decreased by 0.2 kg (SE = 0.1; P < .01). Results of the joint model show the effect modification between week of first gap in physical activity and dietary tracking to be statistically significant.
When specifying gap lengths, increased frequency of short gaps in activity tracking (β = 0.5; SE = 0.3; P = .05) and dietary tracking (β = 0.8; SE = 0.3; P = .02) were individually significantly associated with higher weight. Additionally, the joint model indicated the presence of effect modification (β = −0.3; SE = 0.2; P = .01). Increases in the number of extra-long gaps in activity self-monitoring (β = 3.8; SE = 1.4; P = .01) and in dietary self-monitoring (β = 3.0; SE = 1.5; P = .04) were associated with higher weight. The joint model results suggest that associations of physical activity tracking and weight remained. Finally, effect measure modification by gender was tested for each self-monitoring variable and was not statistically significant.
Discussion
This work is innovative in the examination of physical activity tracking behaviors and their association with 24-month weight and reported physical activity. Consistent with previous work linking adherence to behavioral outcomes,9-11 a strong association between self-monitoring adherence and physical activity and weight outcomes were observed in this sample. However, the variation in self-monitoring, illustrated in Figures 1 and 2, suggests that measures that offer more information about which patterns in self-monitoring may be problematic is necessary. Specifically, to improve weight loss intervention outcomes, it is critical to seek out earlier indicators that provide information about when to intervene. Previous work has suggested that more variability in weight during weight loss interventions is associated with worse weight loss and maintenance. 18 The present analysis expands on this work by examining self-monitoring measures beyond broad adherence and early in the intervention to offer timely support for individuals who show signs of behavioral disengagement. The results supported our hypothesis because late onset of physical activity tracking, total number of self-monitoring gaps, and increases in the average length of the gap were associated with less MVPA. Additionally, because the first gap in self-monitoring occurred later in time, reported MVPA also increased. This work complements previous work10,19,20 examining the effects of MVPA self-monitoring on participation by using more objective self-monitoring measures as well as extending follow-up time. Furthermore, these results suggest that observing gaps in self-monitoring via electronic data collection during active weight loss interventions may be an important tool for practitioners to identify participants who may be susceptible to behavioral relapse or disengagement.
Increases in short, medium, and long length gaps were not significantly associated with MVPA. However, this may be indicative of low power to detect a significant effect because of the low frequency of gaps. Table 1 shows that during the first year of intervention, participants had on average 2.6 (±2.4) small gaps and less than one each of medium, large, and extra-large gaps during the first year of intervention. Nevertheless, a dose-response relationship at 24 months is indicated by the effect sizes. Increases in short gaps are associated with the smallest difference in MVPA, whereas extra-long gaps appear to have the largest difference in MVPA. Future investigations using larger samples with a variety of self-monitoring gap sizes is needed to clarify this relationship.
The strong statistical association between extra-long-gaps in behavior tracking and MVPA suggests that individuals who have gone more than 12 weeks, or approximately 3 months, without tracking during a behavioral weight loss intervention could likely benefit from intervention augmentation or modification. Strategies that seek to reengage individuals showing little self-monitoring activity within a 3-month time frame during a longer intervention period, such as the 1-year duration that is typical of behavioral interventions, may be one way to improve and optimize interventions for successful physical activity outcomes. Strategies to consider include personalized barrier assessments, 21 reframing of regulatory focus, 22 and introducing groups or partners to promote accountability. 23
Results also somewhat supported the second hypothesis because late onset of physical activity self-monitoring and increases in total gaps were associated with higher weight. Furthermore, among individuals who had self-monitoring gaps, weight was inversely associated with the timing of the initial gap in tracking. Models examining dietary tracking characteristics resulted in similar findings. However, late onset of dietary tracking was not significantly associated with weight. This may be a result of the large number of participants who began tracking diet within the second week of intervention (n = 269).
The joint models incorporating the association of both diet and activity tracking behaviors with weight resulted in a variety of outcomes. Because of the correlation between the 2 tracking behaviors, late onset of tracking (r = 0.64), average length of gap (r = 0.91), and extra-long gaps (r = 0.76), very large SEs resulted in each of the models. Therefore, the independent models give more information about the associations between self-monitoring characteristics and weight outcomes. Effect measure modification appeared to be bordering significance in the joint models examining week of first gap and total number of gaps. Results for both suggest an antagonistic interaction, such that increases in the total number of gaps for diet and physical activity independently were associated with increased weight; however, the joint association of tracking gaps for both diet and physical activity was subadditive. This may be a result of an “engagement-effect.” That is, individuals who were not tracking either behavior may be disengaged, and long gaps in tracking both behaviors do not result in more disengagement. Further research that examines specific patterns of self-monitoring or incorporates qualitative data will help better elucidate this finding. When considering gap length, the presence of effect measure modification of short dietary and activity self-monitoring gaps suggests that increased frequency of gaps lasting 1 to 4 weeks should raise concerns and indicate a need for intervention adjustment. Because of the low number of medium, long, and extra-long gaps in this sample, results for these models should be interpreted cautiously. The lack of statistical significance in MVPA across these gap lengths could also suggest that there were no differences between those who did and did not self-monitor activity. For purposes of clinical recommendations and intervention development, these results support intervening after a lapse that has lasted up to 4 weeks to reengage participants in support of their health behavior change. However, gap lengths smaller than this may not be the best way to monitor overall behavioral adherence. Total number of gaps or monitoring the week of the first gap may better indicate individuals struggling to maintain physical activity.
Our findings are consistent with previous work identifying dietary tracking as an integral feature for successful weight loss. 10 However, focusing on MVPA tracking and examining the association with weight maintenance by using a longer follow-up time, the present study offers unique insight into an understudied behavioral relationship. By exploring the association of self-monitoring gaps on MVPA and weight out to 24 months, this analysis highlights specific and measurable criteria for intervention practitioners working in lifestyle behavioral weight loss. Future investigations should examine quality of self-monitoring as well as more specific timing of gaps in tracking to provide earlier and more precise measures of self-monitoring adherence.
There are several limitations to this exploration not previously mentioned. This analysis relies on several assumptions regarding confounding. Although several demographic variables were examined and adjusted for in the models, it is likely that not all possible confounders were measured. Although this sample has a larger proportion of men (35%) than typical weight loss samples, this was still a fairly homogeneous sample. Most individuals were white (86.4%), college educated (63.7%), and married (67.9%). 13 These characteristics suggest that external validity is an issue and similar investigations using more diverse populations should be conducted. It should be noted that participants in the Tracking Study had additional weight loss support, including frequent group meetings, beyond self-monitoring. Therefore, these findings are limited to a supportive weight loss intervention setting and cannot be extrapolated to the larger population using dietary and MVPA self-monitoring for self-guided weight loss.
Measurement error from self-reported MVPA limits this study further. The PAQ assesses individuals’ MVPA participation in the previous week via self-report. Thus, individuals may overestimate MVPA. Additionally, individuals may participate in higher levels of MVPA the week prior to being weighed. Differential overreporting of MVPA could potentially bias the results away from the null. However, it is plausible that this overestimation would occur in both groups of participants regardless of self-monitoring status because of social desirability of being in a weight loss intervention. Future work should use objective MVPA measurement such as accelerometry.
Defining a gap as a weeklong period in which the behavior of interest is not tracked is a broad measurement and may not adequately capture tracking adherence. Participants who did not track MVPA because they did not participate in MVPA and those who did not turn in a log regardless of MVPA participation were both counted as having a gap in tracking. Some individuals may also differ in self-monitoring because of personality differences, such as feeling more pressure to be adherent. Personality traits were not explored in this study, and differences in tracking across different personality types should be considered in the future.
As part of the study, participants had the choice of using their own smart phone or were given iPod touch devices in order to access the Lose It! mobile application. Individuals assigned to paper logging may have experienced more frustration or barriers because of the relative difficulty of completing a paper log versus using an automated, database-linked mobile app and may have been less adherent as a result. Conversely, adults who were not as comfortable with technology may have preferred paper logs. However, the mean age of this sample was 46.5 years, and individuals were required to have an at-home Wi-Fi network in order to connect study devices (ie, Wi-Fi–enabled scales, iPods) to their home network as part of the inclusion criteria. Interestingly, although there were no differences in age across conditions, post hoc comparisons showed that the older group (ages at or above the mean of 46.5 years) tracked both physical activity (28.5 [95% CI = 26.2, 30.8] weeks vs 21.0 [95% CI = 18.4, 23.7] weeks; P < .01) and diet (33.0 [95% CI = 30.8, 35.2] weeks vs 27.0 [95% CI = 24.4, 29.6] weeks; P < .01) more often than those whose ages were below the sample mean age. This suggests that age may not be as important when considering the mode of self-monitoring (paper vs electronic) in any adult with a baseline level of technology access.
As noted above, it is plausible that the paper logging may have been more burdensome than the digital option. Indeed, the average number of weeks tracked differed across conditions for physical activity (no weighing = 18.7 weeks, 95% CI = [15.8, 21.6]; weekly weighing = 30.5 weeks, 95% CI = [27.5, 33.5]; daily weighing = 27.1 weeks, 95% CI = [24.2, 30.0]; P < .01) as well as diet (no weighing = 21.3 weeks, 95% CI = [18.7, 24.0]; weekly weighing = 35.7 weeks, 95% CI = [33.0, 38.5]; daily weighing = 34.6 weeks, 95% CI = [31.9, 37.3]; P < .01). Participants in the no-weighing group that was not assigned to use Lose It! were encouraged not to use other electronic tracking tools to avoid potential contamination with weight tracking features in those apps and were provided with paper diaries for study tracking. Approximately one-third of this group chose to use an electronic tracking website or mobile application; these logs were printed for interventionist assessment. Although treatment assignment was included as a covariate, residual confounding may remain. However, it is important to note that individuals in all categories achieved clinically significant weight loss. Future work should consider differences in preferred self-monitoring tools across demographic characteristics, specifically with populations that may be less familiar with technology. Similarly, with the growth of consumer-based electronic physical activity monitors, research comparing the effectiveness of self-monitoring with these devices to logs in which activity is manually entered is another important next step.
Additionally, because diet requires substantially more frequent logging than MVPA to capture the full behavior, conclusions concerning dietary tracking and how often or how detailed logs should be for successful outcomes is limited. Further work should focus on the optimal detail of tracking logs and duration of behavior tracking needed to produce and sustain healthy dietary and physical activity behavior changes. Differences in tracking behaviors across demographic and psychosocial characteristics are additionally important. Nevertheless, the insight provided by this analysis captures self-monitoring for a fairly large sample over a substantial period of time.
Finally, although this article addresses MVPA maintenance in a sample of individuals actively trying to lose weight, there is little that can be said about specific strategies that may be effective in ensuring high rates of 250 weekly minutes of MVPA achievement and continuation. Little is known about the mechanisms of behavioral maintenance and habit formation and how to intervene for improved behavioral and health outcomes. Self-monitoring may be a sufficient indicator of MVPA at 24 months simply because it indicates MVPA participation at 12 months. Future work should test intervention augmentation strategies, so that once behavioral disengagement is detected, individuals are offered effective options to enhance behavioral maintenance and improve weight loss success.
Conclusion
This study defined different characteristics of physical activity and dietary self-monitoring and examined their associations with MVPA achievement and weight following a behavioral weight loss intervention. Findings suggest that tracking tools offer important information about behavioral engagement early in interventions that may be useful for identifying individuals who may need additional support or augmentations. As electronic tools for self-monitoring become more ubiquitous and precise, monitoring physical activity and dietary tracking should be considered to identify individuals who show signs of behavioral disengagement early to improve behavior change and weight maintenance.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the Tracking Study was provided by NIH Grant R01DK093586-05 (Jennifer A. Linde, PI). Dr. Gavin is additionally supported by NCI training grant [T32 CA139139, PIs: Penedo and Spring].
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.