
Abstract
Obesity is notoriously difficult to treat. Effective treatment has been encumbered by traditional assumptions about the cause of the disease. Obesity is typically considered a manifestation of the patient’s dietary misconduct, a simple lack of willpower, or the inability to modify dysfunctional eating habits. Abundant evidence suggests that eating behavior is much more complex than patient choice alone. Eating and the system of regulating eating and body weight are largely controlled by complex signals from multiple organ systems that monitor food intake, gastrointestinal function, and energy storage and send multiple messages to the brain. The brain coordinates the physiological messages and creates additional signals about eating, appetite, hunger, and satiety. Multiple survival, environmental, and genetic factors become part of a biological regulatory system that controls eating and body weight. The system appears to be unstable and often becomes dysfunctional, particularly in an environment of abundant food and calories. Despite the difficulty in modifying the regulatory system, opportunities for management of the disease do exist. Comprehensive lifestyle management can be useful, as can selective pharmacotherapy and bariatric surgery. Public policy changes will likely be helpful in changing community understanding of the disease and its management.
‘How much we weigh becomes a factor in the control of how much and what we eat.’
The Traditional Model
It is generally assumed that the management of obesity depends simply on 2 principle forms of behavior: eat less and exercise more. An abundance of clinical experience suggests that the assumptions are true and that the recommendations are sound. If, in fact, these simple suggestions are implemented, the effort will yield the desired goal. The task of losing weight will be accomplished, and the problem of obesity will be resolved.
Yet, it usually does not work that way. It is exceedingly difficult to do what seems to be so simple, so true, and so certain to achieve the desired goal. Why, and why is it so difficult to lose weight?
The Qualifiers
There are, of course, some qualifiers for these simple rules. The assumptions are true:
if we accept the laws of thermodynamics;
if we assume that eating is merely a matter of choice; and
if we assume that metabolism does not change with changes in eating or with weight loss.
Let us assume that the laws of thermodynamics apply, even to a system as complex as the coordination of the metabolism of trillions of cells in the human body. A calorie is a calorie, whether it is consumed (intake) or it does some kind of biological work (output). If the weight is stable, it means that calories in equals calories out. When the equation is not balanced weight is going up or going down.
It is the second and third qualifiers that require our attention. In these 2 assumptions, we are obliged to consider how much choice humans have about what they eat and whether the metabolic system is the same in all people and in all circumstances?
For the purposes of weight management, it is reasonable to assume that the brain primarily regulates eating. It is easier to see how the brain can regulate the process of eating, however complex, rather than assuming that its role is to regulate the outcome of eating—that is, body weight. As a consequence of this control of eating, we achieve the regulation of body weight. The reverse also seems to be true. How much we weigh becomes a factor in the control of how much and what we eat. The important questions that emerge from this are how much of our eating is a matter of personal choice and how much is set by our underlying physiology.
Weight Stability
One basic issue that obligates our consideration in a discussion of eating is the remarkable puzzle of weight stability. Most people, even those who are obese, are weight stable for significant parts of their lives—often for decades and often within a few pounds. How do they do this? This stability requires some explanation when one considers the precision that is necessary to be weight stable and the amount of food consumed. For example, all the increase in the weight of the American people since 1970 can be explained by an average increase in food consumption of about 10 to 15 calories a day. This is a precision of control that far exceeds the ability of even the most informed and dedicated dieter. The average American adult consumes a bit less than a million calories a year, 50 million calories in an adult lifetime, and about 25 000 lb of food. How can we explain weight stability, which apparently requires a delicate balance of a few calories, in a system that consumes a million calories a year? It seems unlikely that the body is in balance and weight stable by choice or chance alone. It is surely beyond the conscious dietary skills of ordinary people. Some other factors must be making the thousands of small dietary adjustments every day to achieve that degree of weight stability.
The Regulation of Eating
We are obliged then to explore the possibility that eating, and thus body weight, is regulated by some other forces. Conscious choice obviously does exist, but it appears to be only one of many factors involved in the control of body weight.
The task is to explore not whether but how eating is regulated. On one hand, it seems unlikely that individuals make all their food and eating choices. It appears unlikely that they can regulate all their food intake, the timing of eating, starting and stopping, and the selection of food and its quantity, particularly if they have the added obligation to be weight stable. On the other hand, is it controlled by our physiology? Are we hardwired to eat what and when we eat and how much we eat? It is not likely that physiology alone controls eating and body weight because we do, obviously, make choices. Or perhaps there is a third way, a combination of both, much as what seems to happen with other regulated biological systems such as sleeping or breathing.
There are, of course, a number of factors involved in how the brain does all this. It must be balancing all the forces involved in eating: social, evolutionary, genetic, biological, and environmental. It is the brain’s task to have all the diverse instruments in this orchestra playing a finished symphony rather than the dissonance of each instrument playing with no regard for the others. The risk is in judging eating to be a simple task, following some specific dietary mandates, and making a series of uncomplicated food choices. The reality is that the control of eating, so much linked to survival, is at least as complex as other survival systems and at least as important as getting enough air and water.
We should reasonably expect that whatever regulates eating will be a complex system, serving diverse metabolic purposes (eg, ensuring the availability of sufficient metabolic fuel, the storage of nutrients, structural sufficiency, and micronutrient availability) with sufficient redundancy to avoid malnutrition and starvation. All this must be done in the context of the important factors involved in the complex diversity of how humans use food for non-nutritional purposes. Moreover, it should be anticipated that the system should favor food consumption (ie, survival) in preference to mechanisms to eat less, limit food consumption, or lose weight.
Consider what seems likely to be involved in the human use of food and the regulation of eating behavior.
Survival. The eating regulation system is set to favor food consumption. Our prehistoric ancestors were obliged to devote much of their time to food acquisition. The evolutionary advantage, particularly in times of limited food supply, is conferred on those who were skilled at finding food, consuming it, and storing the excess as fat. The advantage is to eat, even to gorge, when food is available. The genetic pool favors food consumption, and humans use this to ensure survival. Every mother nurtures her children with food; not simply for love and comfort, but it is survival. There is little evolutionary advantage in limiting food intake, particularly in the relatively common occurrence of food shortages. An abundant and predictable supply of food coincides, in timing and location, and is a sine qua non for the development of obesity. Survival forces control eating. In the absence of eating signals, life ceases to exist.
Social factors. Anthropologically, all cultures use food for non-nutritional purposes. The organization of groups of people usually depends on the food supply. Food is not typically consumed alone. It is acquired and consumed in a community of people: the village, the tribe, and the family. Complex rules control how food is distributed, to whom, and how it is consumed. Meal patterns, timing, and content stipulate how and what we eat and when. Food is an expression of power, prestige, and social status. Humans fight wars over food. The development of agriculture 10 000 years ago with associated new ways of food production and distribution created the opportunity for new communities to form and facilitated the creation of new rules about how we get our food, how it is distributed, to whom, and by whom. Every religion uses food for non-nutritional purposes. It has become a way of organizing the community. The use of food selection, rituals, festivals, and taboos as part of the community’s way of distinguishing itself is typical. The reward for participation is often an eating event. Social and community patterns control eating.
Environmental factors. Prehistoric humans were probably opportunistic eaters, but modern cultures are more likely to organize food consumption into meals and time of day. Eating depends on the availability of light. Artificial lighting has extended the hours of eating opportunity and has modified sleeping and related eating patterns. 1 Fire (cooking food) has increased the amount of calories available in noncooked, less-digestible food.2,3 Industrial chemicals in our environment affect our body weight.4,5 The world we live in affects our eating.
Biological factors. A number of studies suggest that some viruses are associated with obesity,6,7 and recent research links the otherwise innocuous variability of intestinal bacteria with differences in the processing and absorption of nutrients.8,9 The processing of food and its form—whole, crushed, or liquefied—may affect its digestion and absorption and the calorie content of foods consumed.10,11 We have an abundance of metabolic factors that change as we eat, or change what we eat, or modify the food we consume, or predispose us to create or burn fat. Individual variations in metabolic signals and metabolic rate create variations in how easily individuals gain or lose weight. The natural variations in human biology affect the efficiency of eating and of food.
Genetic factors. Human variation, substantially imbedded in our genes creates variations in individuals and in groups of people. People who have what has come to be called the “thrifty” gene need fewer calories than others lacking this genetic profile.12,13 Those with family obesity are significantly more vulnerable than others. Epigenetic factors,14,15 biological or environmental, affect how genes are expressed and which ones affect metabolism. The offspring of mothers who survived a famine 16 weigh more than those whose mothers had ordinary food. Genetic factors make individuals more or less vulnerable.
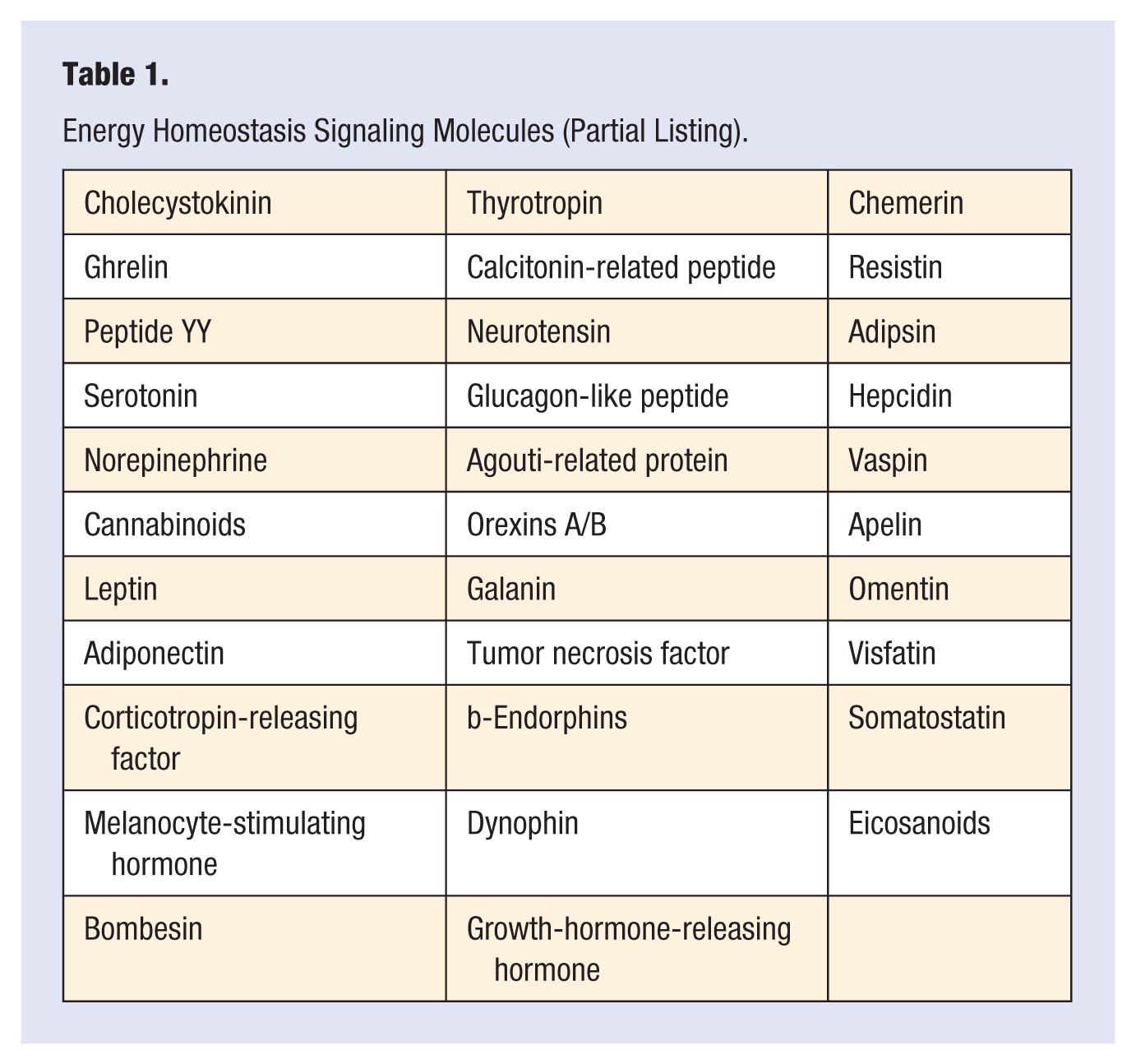
Regulatory factors. The body has complex communication mechanisms that send information from one system to another. The brain gets information from a variety of messengers telling it what is in your stomach and gastrointestinal tract, what you have eaten and how much, what is being processed by the liver and by muscle, and how much fat is being processed and stored. The brain sends information, including food consumption information, to create hunger, appetite, and satiety. There are dozens of these messengers (Table 1), hormones, signaling and regulatory substances, peptides and adipokines, and neurochemicals that regulate individual patterns of eating events. Their biological setting, profoundly affected by all the other factors, controls eating and body weight.
Energy Homeostasis Signaling Molecules (Partial Listing).
All these bits of information about survival, evolution, culture, rules and customs, genetics, and biology are gathered by the brain. The brain coordinates the eating signals. The signals vary from one person to another. The way humans eat is a complex form of behavior affected by scores of information inputs. It is affected by simple things such as time of day, other people, other eating events, and of course, our deliberate efforts to manage eating for health and weight concerns. There is no particular reason to assume that the signals are the same for all people and no reason to assume that the information transmitted will be fixed, permanent, or set at an ideal, optimum, or healthy level.
It follows that eating is a particularly complicated system of positive and negative signals controlled by scores of factors that regulate eating behavior. The system seems difficult to balance in humans and appears often to be set at an uncomfortable or unhealthy level. The choice to eat means ignoring or overriding these biological, cultural signals. When we ask people to eat less, we are asking them to superimpose their willful determination on the biological signals that are telling them to do otherwise. It is possible to eat less but very difficult to do this in a sustaining way. Our reality, however, is the sad recognition that if we want to manage obesity, we must use this limited ability, choosing what to eat in order to override the metabolically dysfunctional system.
It is difficult to create behavior change and modify eating patterns, particularly when the change conflicts with biologically set eating signals. It is not, however, necessary or reasonable to assume a fatalistic model of futility in weight management. Is it difficult? Yes. Is it impossible? No.
What resources do we have available? What can be done, and what might be done, and what do we need to be careful about?
Short-term interventions are useless. This is the nature of almost all diet books, dietary miracle cures, and secret and ancient oriental remedies. The personal intensity of these dietary fads does not cure the disease and does not reset the regulating systems. Their impact is usually brief because the characteristics of the intervention are in conflict with well-established, intensely imbedded, preexisting eating habits. These interventions are sustainable only as long as the individual patient can tolerate and sustain the necessary changes.
When individuals lose weight, they change not only their size and the complicating metabolic illnesses, but they also change the associated social, situational, and emotional state. The person who uses food and eating as a way of coping with the stresses of life (a food-dependent personality) needs, with weight loss, to develop alternate ways of coping with stress or to modify the pattern of using food for stress management. Similarly, the patient who uses excess weight or the state of being obese (a fat-dependent personality) as a way of managing, coping with, or avoiding tasks, responsibilities, aspirations, or personal relationships, now, having lost the excess weight, must deal with these responsibilities or shift to an alternate way of coping. Complex compensating emotional patterns that are stable in the obese patient often fall apart when the patient loses a substantial amount of weight.
These factors and other issues linked to eating reinforce the importance of psychological and emotional awareness in patients and in health care personnel who participate in weight management programs. This is in part because these issues make it difficult to change patterns to enable patients to lose weight and also because they contribute so substantially to the complexity of the task of the maintenance of weight loss.
The Treatment Options
Can we do anything to change the signaling systems or simplify the necessary behavior change? Substantial effort is required to make deliberate changes in human eating behavior, and the complexity and overlapping redundancy make it difficult to modify or reset the biological/physiological settings of the eating control regulating systems. There are 4 options:
using intensive and comprehensive multidisciplinary lifestyle modification programs;
using pharmacotherapy to change the settings on the signaling neurochemical and biochemical control mechanisms;
surgical changes in the anatomy of the intestinal tract; and
making changes in the price of food, modifications in its availability and distribution, or comparable changes in public policy that can have a population, rather than an individual effect.
Individually formulated lifestyle interventions can be sustained and effective for long-term management. These interventions, using behavioral and cognitive, nutritional, exercise and activity, and situational guidance and counseling have been shown to be effective in a continuing way.17,18 They enable patients to lose weight, to sustain their weight loss, and to complement and reinforce weight loss achieved with very-low-calorie and a variety of other diets, pharmacotherapy, and surgical interventions. These techniques involve the skills of counselors, coaches, and therapists from a variety of backgrounds. These therapists, with a variety of skills, can help patients analyze their eating issues, understand the social and emotional factors related to their excess weight, and make changes that are consistent with their life patterns and their previously existing characteristics. As with all other interventions, lifestyle modification will not cure the disease or reset the regulators. Continuing counseling and supportive reinforcement is usually required to achieve long-term control.
If we recognize that substantial effort is required to make deliberate changes in our willful eating behavior, we will also pose the question of how difficult it is to modify or reset the biological/physiological settings of the eating control regulating systems. There are currently 3 options.
We have no good ways of changing the regulating system without the use of some kind of pharmacotherapy or the use of some other interventional procedure. Even if we had effective ways of modifying one or another molecule in the regulating system, we would still have a series of obstacles to continuing control. We have identified scores of molecular participants in the eating regulatory system, and it does seem likely that many of the major participants in the controls are identified. Part of the problem is that many of the signaling molecules are involved in multiple other neurochemical information and signal transmitting systems. Thus, it will be difficult to change the level of serotonin, an important participant in the regulation of eating, without simultaneously changing its impact on mood and sleep. We will need to develop ways of targeting our pharmacotherapy to specific anatomical or functionally critical sites to avoid the unwanted side effects. It will be difficult to create medications that affect one part of the brain without expecting that unwanted side effects will be created. It will not be realistic to expect to modify one brain chemical without some other kinds of central nervous system side effects.
We should also recognize that the complexity of the brain’s regulatory system serves the additional purpose of redundancy of controls. The system appears to defend its control by creating duplication in the signals. If the action of molecule X is suppressed with a pharmacological agent, it is likely that molecule Y will duplicate its mechanism of action. Eating and survival seem so important that it does not depend on a single molecular mechanism.
This redundancy is a major reason that effective pharmacotherapy will probably require the simultaneous use of multiple medications. Many medical problems such as cancer, infectious diseases, and diabetes are effectively treated using multiple drugs. Obesity will probably need the same approach.
Surgical procedures often provide a significant amount of weight loss and improvement in metabolic abnormalities. The changes are often not permanent. New techniques include the use of a variety of electrical stimulating devices and the placement of mechanical devices in the stomach and small intestines to send artificial gastric and small-intestinal signals. These procedures diminish the surgical risk associated with the currently available bariatric procedures. All surgical procedures should be considered as an aggressive alternate way of managing the problem; but none resolves the problem, nor do any offer permanent control. Surgical patients and professional service providers should be prepared to sustain long-term management efforts.
None of these intervention techniques, pharmacotherapy, or surgery will resolve the problem. The brain eventually develops ways of compensating for any intervention—medical or surgical.
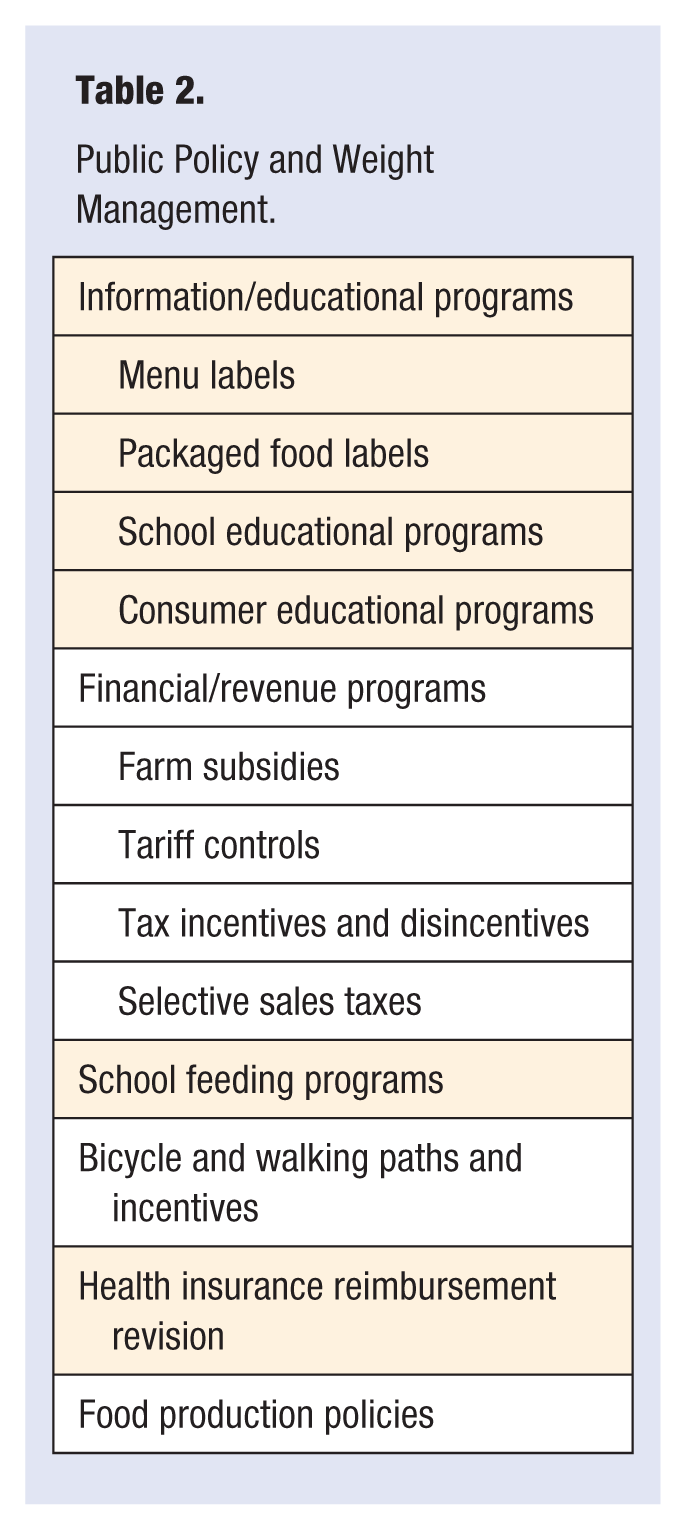
Another part of the management of obesity is focused on how aspects of the modification of public policy (Table 2) can be used to mitigate the dangerous environment that contributes to overeating and obesity. Can we achieve value by creating a different environment for the population generally in addition to what we can do for each individual patient? The value of any intervention will not be that it will cure the disease or resolve the problem but rather that it will help patients make useful lifestyle changes. Most changes will involve government intervention. Some will involve voluntary agencies or resources.
Public Policy and Weight Management.
The Futility of the Misconduct Model
Obesity is a difficult disease to manage. Part of the problem is ineffective choices and personal difficulty in modifying eating patterns. Much of the problem is caused by a series of dysfunctional signals from an extraordinarily complex neurochemical system that controls eating behavior in a complicated world that favors food consumption.
Obesity is not caused simply by the indifference or the willful misconduct of the patient. The traditional mandate to “eat less and exercise more” is the nutritional equivalent of telling a depressed patient “just pull yourself together” or an asthmatic patient “just breathe easy.”
Footnotes
Acknowledgements
I am indebted to my colleague, William Picon, PhD, for his thoughtful formulation of the concept and therapy of food and fat dependence.