
Abstract
The 5A’s Framework (Assess, Advise, Assist, Agree, and Arrange) has been recommended as a practice guide for obesity counseling. Its integration in research, however, is not well known. This systematic review was to find how the 5A’s Framework was integrated in research on obesity and weight counseling.
Keywords
“A unique contribution of our systematic review is the assessment of the 5A’s Framework intervention details using the TIDieR checklist.”
Nearly 60% of adults are overweight or obese worldwide, which affects 2.5 billion people. 1 Obesity places people at risk for cardiovascular disease, metabolic disease, cancer, clinical depression, and poor health-related quality of life.2,3 Overweight and obesity can be affected by lifestyle behaviors such as eating and physical activity. 4 Adults who engage in healthy lifestyle behaviors are more likely to control their weight and postpone the onset of developing chronic diseases for up to 9 years than those who do not regularly engage in healthy behaviors. 5 To achieve a healthy lifestyle, individuals can initiate action plans and maintain healthy behaviors. However, many people may lack knowledge, skills, and recourses to execute healthy eating and physical activity; subsequently, they need counseling and support from health professionals.
The US Preventive Services Task Force recommends clinicians offer or refer adults with a body mass index (BMI) of 30 or higher to intensive behavioral interventions. 6 The American Academy of Family Physicians’ clinical guidance for obesity and healthy lifestyle suggests that clinicians provide counseling and help patients identify obstacles to healthy eating, set realistic goals for physical activity, and develop behavioral strategies. 7 It is noted that lifestyle behavioral counseling is also beneficial for people whose body weight falls in the overweight category (BMI = 25-29.9) or those who have lost weight and want to prevent weight regain. Given the need for behavioral interventions and recommendations for obesity counseling, it is imperative for clinicians to know how to provide the obesity and weight counseling.
One intervention for addressing obesity and weight counseling is the 5A’s Framework. 8 The 5A’s Framework was developed by the National Cancer Institute to guide clinicians in addressing tobacco smoking cessation. 9 The 5’As Framework was later repurposed for weight counseling.10,11 In 2012, the Canadian Obesity Network supported the delivery of 5A’s weight counseling in family medicine practices. 12 Generally, various iterations of the 5A’s Framework have included five of the following components: (1) Asking (with objective measurement and assessment), (2) Advising (concerning the need for and benefits of achieving a desired outcome), (3) Assessing (patient readiness to change lifestyle behavior), (4) Agreement (between patient and clinician concerning behavior change plan), (5) Assisting (in establishing appropriate intervention or referrals), and (6) Arranging (follow-up on the behavioral change).13-15
Some researchers suggest that high-intensity obesity counseling should include 12 sessions a year, and the counseling can be given in person, by phone, or electronically. 16 Others recommend that interactive behavior change technology for 5A’s based interventions be implemented in the primary care setting to structure health care providers’ clinical interactions and maximize their impact on obesity treatment.17,18 Published systematic reviews that provide intervention details, such as why, how, when, who, and where to implement the 5A’s Framework, is limited. A previous systematic review addressed the 5A’s Framework implemented in clinical setting for individual health behavior change. 13 Another systematic review, based on the findings from 15 studies, concluded that during weight loss counseling, patients would like their physicians to Arrange, followed by Advise, Agree and Assist, but physicians most frequently Advised and Assessed. 14 A third systematic review outlined the definitions of the 5A’s components, the rationale, and sample questions a clinician could ask relevant to each component. 15 These previous systematic reviews did not shed light on implementation details of the 5A’s Framework in obesity and weight counseling. Evidence-based practice is built on consistent findings from multiple studies. But evidence-based implementation procedures are as important as research outcomes. Evaluating intervention details across studies is valuable for researchers to replicate a study and clinicians to adopt an intervention in practice. The purpose of this systematic review was to assess the integration of the 5A’s Framework, including implementation details, in obesity and weight counseling research that addressed lifestyle behaviors (eating, physical activity) in adults with overweight or obesity.
Methods
We adopted the stages of conducting systematic reviews model by Siddaway et al. 19 The stages included scoping (formulate research questions), planning (formulate search terms and preliminary inclusion/exclusion criteria), searching (use multiple databases), screening (export references to a citation manager and assess studies for inclusion/exclusion), and presenting results (extract and synthesize data and offer a new, improved understanding of the phenomena).
Scoping
The research question was “how is the 5A’s Framework integrated into research on obesity and weight counseling?”
Planning and Searching
A systematic search of 4 databases was conducted by the health sciences librarian (AJ). We searched PubMed, Embase, CINAHL Complete, and APA PsycINFO combining 2 concepts: “5 A’s Framework” and “obesity-related concepts including: body size/BMI, dieting/eating, exercise, weight loss, etc.” (See Supplement 1 for search strategies). The 5 A’s Framework is referred to counseling techniques/content that include 5 of the following components: ask, advise, assess, agree, assist, and arrange. The inclusion criteria included the publication date range of January 2000 to September 2023. The 5 A’s Framework was recommended by the National Institutes of Health for obesity behavior management in 1998 20 ; subsequently publications on the 5A’s Framework in obesity/weight counseling began to surge. Additional inclusion criteria were that publications must report quantitative results and include the 5A’s Framework within an intervention to influence the outcomes of adult obesity-related behaviors (weighing, healthy eating, and physical activity) or weight outcomes, and/or clinician counseling behaviors. Exclusion criteria included publications examining smoking, substance use, HIV, or cancer. Additionally, animal studies, case studies, qualitative research, systematic reviews and/or meta-analyses, conference abstracts, and protocols were excluded.
Screening
The initial search found 755 records. Duplicate records were removed using a variation of the EndNote de-duplication method.
21
Records were then imported from the reference manager into Covidence for screening, review, and extraction. After removing 227 duplicate records, 40 records were randomly selected (AJ) and used for training the research team (CS, HH, MD). During the training, each record was reviewed by 2 team members against inclusion and exclusion criteria, which resulted in an interrater agreement rate of 80% (2 members had the same screen results). Meetings were held throughout the screening process (training and abstract/full-text reviews) to discuss the records with conflicting review results until a resolution was made either by 2 reviewers achieving an agreement or by the first author making a final decision. The team reviewed abstracts of the remaining 528 records and retained 65 records for full-text review with an agreement rate of 93.75%. Additional records were removed during full-text review, resulting in 22 articles for the final analysis (PRISMA
22
flow diagram in Figure 1). PRISMA diagram for literature search and article selection.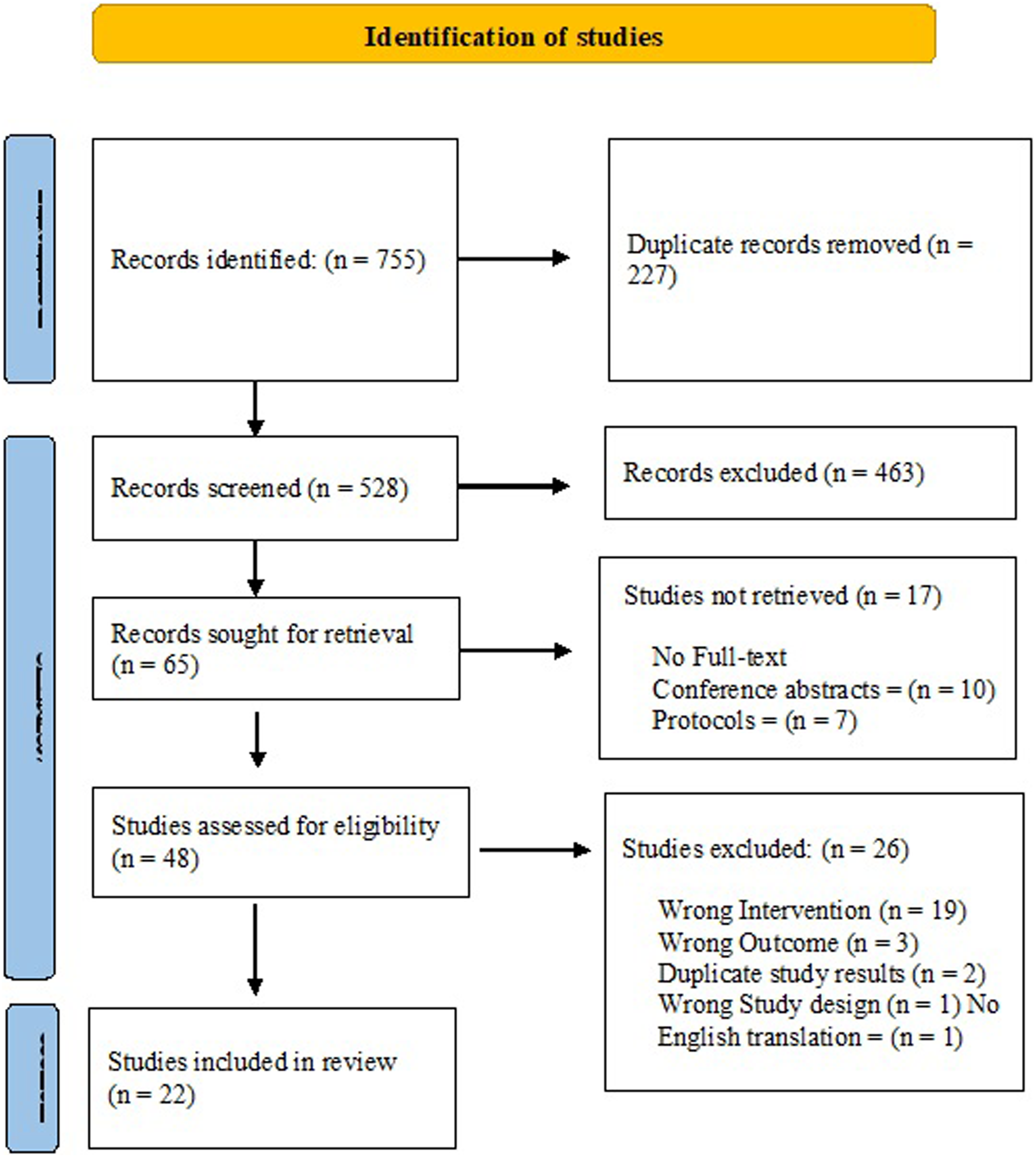
Literature Analysis
The TIDieR (Template for Intervention Description and Replication) checklist was used to facilitate analysis and report. 23 TIDieR includes 12 questions about intervention details, such as brief name of the intervention (study purpose), why (theory/model), what (activity, material), who (intervention provider), how (mode of delivery), where (location of the intervention), when and how much (frequency, length), tailoring (personalized, titrated, adapted), modification (change), and how well (attrition, adherence). Excel files were created, and the first author (CS) and a research assistant independently extracted information from each article to capture TIDieR required information.
Presenting Results
Extracted information was synthesized and presented in tables. We synthesized our results into 4 categories of interventions for: (1) medical students and residents, (2) physicians, (3) non-physician health care providers, and (4) patients. In the results section, we first summarize study purpose, how the 5A’s Framework was used, and the components of the 5A’s Framework across studies. We then report intervention details based the TIDieR checklist.
Study Quality Assessment
We used the National Heart, Lung, and Blood Institute tools for multiple types of studies to appraise study quality because our analysis included studies of various designs.
24
Among the 15 studies with an experimental design and a comparison group, 4 had a quality rating
Results
Study Characteristics
Study Characteristics (N = 22 Studies).
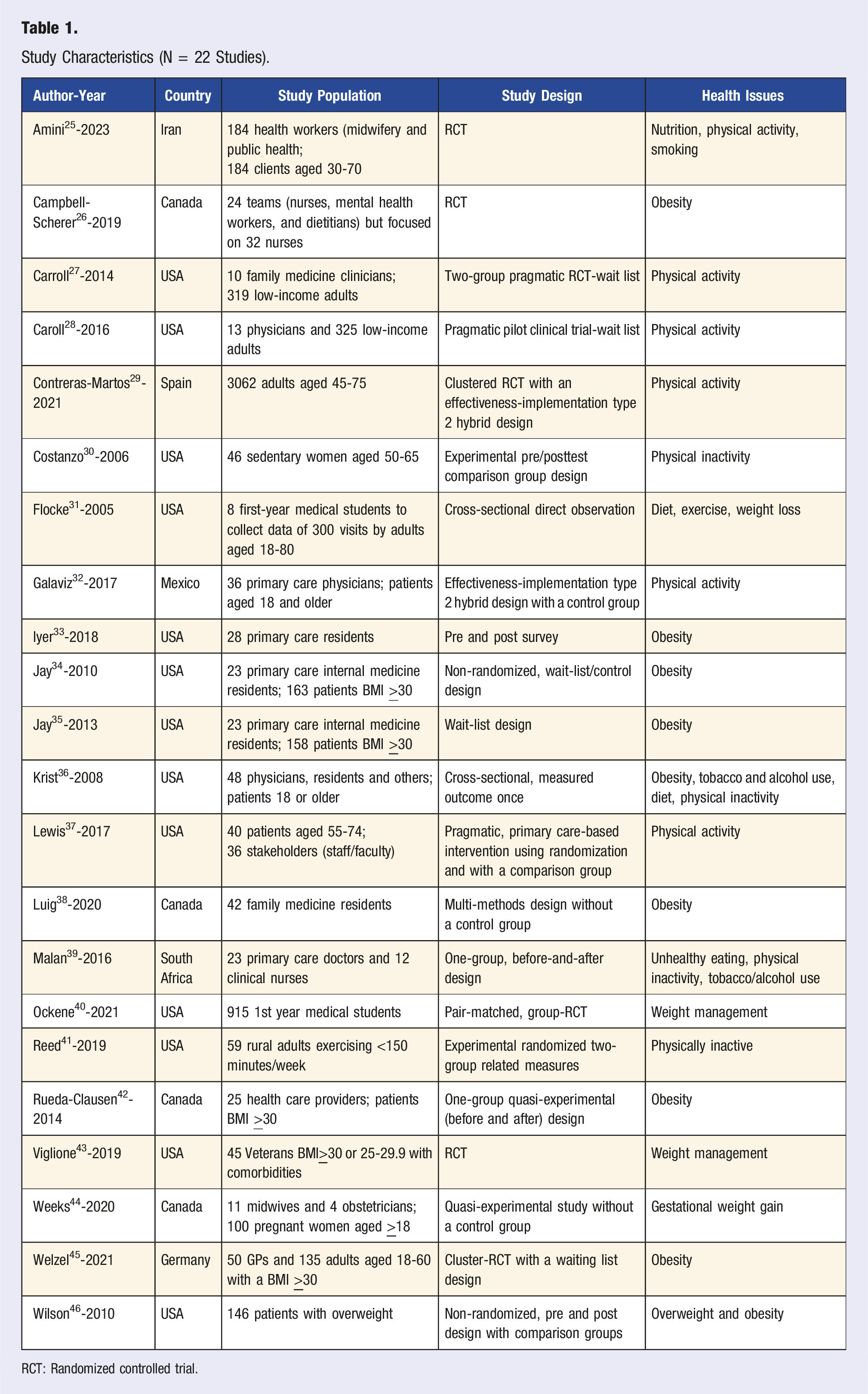
RCT: Randomized controlled trial.
5A’s Interventions Focused on Medical Students and Medical Residents
Study Purpose and 5A’s Based Studies (n = 22).

Intervention Details in 22 Studies (Why, What, How, and When).

Intervention Details in 22 Studies (Where, Who, Tailoring, Modification, and How Well).
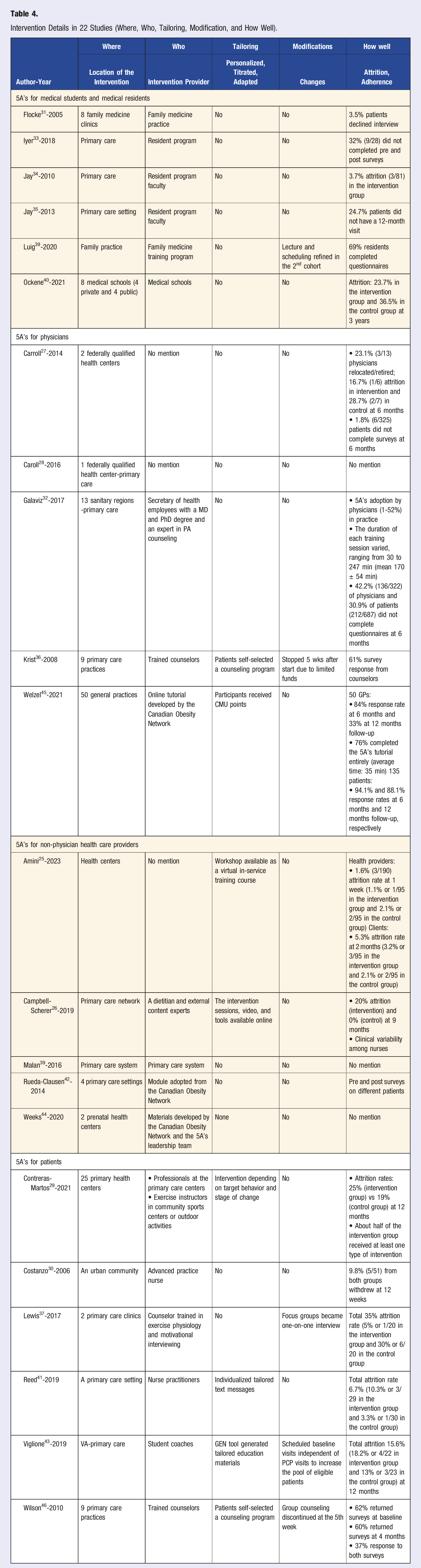
Five of the 6 medical student/resident studies were conducted in the primary care setting, and one was implemented in 8 medical schools (Table 4). No major modifications were reported except one study that refined lecture and scheduling for the 2nd cohort of family medicine residents. 38 Adherence data were not commonly reported. Attrition rates varied from 3.7% to 36.5% between pre and post intervention surveys.
5A’s Interventions Focused on Physicians
Five articles reported 5A’s interventions conducted with family medicine and primary care physicians.27,28,32,36,45 These 5 studies aimed to improve physician-patient communication and physicians’ counseling skills related to physical activity (n = 3), body weight (n = 1), and other unhealthy behavior (n = 1) (Table 2). The 5 A’s Framework was integrated into observation checklists, weight counseling training programs, weight counseling document guide, or electronic medical records. Advise, Assist, and Agree were included in all 5 studies, Ask and Agree in 4 studies, and Assess in 2 studies. Krist et al. added “Address” when testing an electronic linkage system to help clinicians perform behavioral counseling. 36
Table 3 (intervention details based on TIDieR) shows that the Research, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework was included in one study. 32 Physician counseling training programs varied from 40 minutes to 4 hours in length and were delivered via individual, group, and online formats. The training also included problem-solving, standardized patient practice, practice guidelines, and knowledge quizzes. One study used prompts built in electronic medical records to help clinicians perform the 5A’s counseling and refer patients to different counseling modalities (group, telephone or computer care, and physician). 36 Three studies used a wait-list design, where the control group received the training 6-8 months after the intervention.27,28,45
All 5 studies were conducted in primary care settings (Table 4, TIDieR information). Most articles did not clearly address who delivered the training to physicians. In one study, an officer from the Secretary of Health (Mexico) provided the training. 32 Trainees in one study received continued medical education points. 45 Recruitment in another study was discontinued after 5 weeks due to limited funds. 36 Carroll et al. reported attrition rates of 16.7% and 28.7% at 6 months for the intervention group and the control group, respectively. 27 Galaviz et al. provided adherence data which included the duration of each training session from 30 to 247 minutes. 32
5A’s Interventions Focused on Non-physician Health Care Providers
Five studies involved non-physician health care providers (midwives, nurses, public health workers, mental health workers, and dietitians).25,26,39,42,44 The 5A’s Framework was adopted to develop (1) an education program or a checklist to facilitate provider–patient communication or (2) a questionnaire to collect data about provider counseling behavior (Table 2). Ask, Assess, and Assist were included in 4 studies, Advise in 3 studies, and Agree and Arrange in 2 studies. One study added an “Alert” to their intervention, which was to provide tailored information to the patient and elicit understanding. 39 Clinicians in this study provided behavioral counseling to standardized patients immediately before and after training and again 6 weeks later for skill assessment.
Tables 3 and 4 capture TIDieR related information. Researchers adopted the WHO-Healthy Lifestyle module, Theoretical Domains Framework, Motivational Interviewing, and Health Belief Model in 5A’s interventions conducted with non-physician health care workers (Table 3). Five A’s Framework integrated training workshops ranged from 60 minutes to 24 hours over 12 education sessions. Workshops included group discussions, video watching on the Internet or via application, and printed handouts and checklists. Two of the 5 studies included a control group.
All 5 studies were implemented in the primary care setting, including 2 prenatal health centers 44 (Table 4). Dietitians and nurse practitioners delivered the intervention training to non-physician clinicians. Tailoring activities included making the training online and providing individualized text messages. Attrition and adherence data were not reported in 3 of the 5 studies. Attrition was low (1.6% vs 2.1% for intervention and control) at 1 week in one study 25 and high (20% vs 0% in intervention and control) at 9 months in another study. 26
5A’s Intervention Focused on Patients
The 5A’s Framework was used in 6 studies to improve patient outcomes. These studies intended to improve patient’s physical activity (n = 4),30,37,41,43 weight (n = 1), 46 and weight, diet, and physical activity (n = 1) 43 (Table 2). The 5 A’s Framework was included in behavioral counseling or electronic medical records in the patient-focused studies. All 6 patient-focused studies adopted Assess, Advise, Agree, Assist, and Arrange, and none included Ask.
Several additional theories/models were included in these studies, including Transtheoretical Model of Behavior Change, Health Promotion Model, Social Cognitive Theory, and RE-AIM Framework (Table 3). The 5A’s Framework was used by study interveners to provide counseling for patients, deliver group sessions, coach patients, and refer patients to community resources. Often, patients received additional instructions, such as how to use wearable devices to track, monitor, and record diet, physical activity, and sleep. Patients also received coaching calls and participated in group sessions. Training for counselors and study interveners lasted 15-20 minutes to 20-25 hours. Each coaching call was 25 minutes, and each group session was 90-120 minutes long. The length of patient-focused interventions was 12 weeks to 9 months. One intervention used an electronic system to encourage patients to choose one of the three intensive counseling methods: Weight Watchers Program, individual telephone counseling, or computer-based counseling. 46 All 6 patient-focused studies included a comparison group.
Table 4 shows that 5 of the 6 patient-focused studies recruited study participants from primary care settings. Exercise instructors, advanced practice nurses, trained counselors, and health coaches delivered the interventions. One study conducted via the U.S. Veterans’ Administration health system involved undergraduate, graduate, and pre-medical students as health coaches. 43 Tailoring and modifications of the 5A’s Framework intervention were reported in several studies. Interventions were tailored to provide information and counseling based on a person’s stage of change and allowing the patient to self-select a counseling program. Some study modifications included: changing focus groups to one-on-one meetings, scheduling baseline visits independent of primary care provider visits, and discontinuing free Weight Watcher’s program referrals at week 5 of the study. One study had a high attrition rate of 35%, 37 while others reported a rate of less than 20%.41,43
Discussion
This systematic review, including 22 quantitative articles, aimed to assess how the 5A’s Framework was integrated, including implementation details, in research on obesity and weight counseling. We found that the 5A’s Framework was adopted in studies conducted primarily in the primary care setting across the U.S. and other countries. The finding agrees with the recommendations addressed in previous publications about primary care being an ideal practice setting to implement 5A’s based obesity and weight counseling.7,13-15,17,18
Most of the studies in our analysis integrated the 5A’s Framework in obesity and weight counseling trainings as formal medical curricula and continuing education programs for physicians in training, current physicians, and non-physician health care workers to influence (1) their obesity and weight counseling behaviors and communication with clients and (2) patients’ obesity and weight loss behaviors. Some researchers also used the 5A’s Framework as a validation tool to assess obesity/weight counseling behaviors/skills of health care providers, and the validation tools could be translated into a skills observation checklist and/or self-assessment questionnaire.
A minority of the studies in our review was patient-focused to improve the patients’ obesity-related behaviors and weight outcomes. Those patient-focused studies not only integrated the 5A’s Framework in training the people who provided a proposed intervention but also combined additional behavior change strategies in the intervention, such as self-monitoring of diet and physical activities or offering outside primary care support programs. These studies all included a comparison group but did not include the component of Ask.
Various combinations of the 6 components (Ask, Assess, Advise, Advise, Agree, and Arrange) were selected by researchers to conduct their studies. Across the 4 categories of 5 A’s interventions in our analysis, Advise and Assist were most frequently included than the other components. Additionally, the 6 patient-focused studies in our review all adopted Assess, Advise, Agree, Assist, and Arrange, and none included Ask. In a previous systematic review, Assist and Arrange were reported most desired by patients, but Advise and Assess were most frequently practiced by physicians. 14 Whitlock et al. viewed the 5A’s as a unifying construct: each A is unique and together the 5A’s components become an organizational construct for clinical weight counseling. 13 More research is needed to assess whether or not each component leads to different patient outcomes and which combination of the components results in more weight loss or better weight maintenance. The Multiphase Optimization Strategy (MOST) could be a useful framework in trial design to determine the relationship between 5A’s components and study outcomes relevant to patient weight or provider counseling behaviors. 47 Before such research data are available, it may be important to regard the 5A’s as a unifying construct for obesity and weight counseling, rather than emphasize individual components in the 5 A’s Framework.
A unique contribution of our systematic review is the assessment of the 5A’s Framework intervention details using the TIDieR checklist. TIDieR is thought to improve replicability of intervention and comparability between studies. 23 Ideally, similar results, such as effect sizes and confidence intervals, generated from multiple studies or replications are likely to support a theory or hypothesis or to estimate the evidence.19,48 Some researchers recommend conceptual replication as an attempt to test the same fundamental idea using different dependent variables, designs, and participant population. 49 We are not able to provide, based on our systematic review, standard intervention procedures for 5A’s based interventions. However, our analysis findings offered similarities and differences in intervention details across studies with various designs and study participants that tested the fundamental idea of the 5A’s Framework. Some similarities included integration of the 5A’s Framework in counseling trainings, intervention conducted in the primary care setting, and involvement of a comparison group in 5A’s based studies that were focused on patients. Many differences and variations were also noticed across studies in the mode of intervention delivery, duration of intervention, modification and tailoring during intervention, and whether to use triangulation of additional theories and frameworks, such as health promotion, behavior change, and motivation interviewing theories, in a 5A’s based intervention. Certainly, more research is needed, especially well-designed studies that pay attention to intervention details. As health care is becoming more complex due to advanced technologies and obesity treatment modalities, more studies for multilevel interventions, such as integrating the 5A’s Framework in electronic medical records to enhance obesity/weight counseling, referral, and follow-up among interdisciplinary care teams or combining the 5A’s Framework behavioral counseling with pharmacological and surgical treatment modalities for obesity, are also recommended.
Practice Implications
Our review findings imply that health care providers working in the primary care setting have the privilege to begin and continue the conversation about weight with their clients and the providers will need to have the knowledge and skills to use the 5A’s Framework in weight counseling. Five A’s or other weight and obesity counseling continuing education could be provided for newly hired providers and re-enforced with annual continuing education workshops. Care system modification in the primary care setting, including software and additional personnel, will need to be modified to facilitate providers’ assessment, documentation, follow-up, and billing and reimbursement. Nevertheless, potential challenges could occur when implementing a 5A’s based weight and obesity counseling program, and challenges may include obtaining the buy-in from the administration (e.g., developing education programs), the provider team (e.g., time constraints), and supporting staff (e.g., change patient flow), and mobilizing resources to offset costs from the implementation.
As the 5A’s Framework is largely applied to the development of obesity and weight counseling skills and the validation of competencies of current and future care providers, another practice implication is to include the 5A’s Framework in education programs and licensure, board, and clinical certification exams to reinforce the importance of obesity and weight counseling and help improve the obesity epidemic.
Limitations
Limitations in this systematic review are related to the quality of the available evidence, including a lack of information concerning intervention adherence and dose, limited study attrition data, and a limited number of fully powered randomized controlled trials (RCTS). Future research should provide intervention adherence and dose intended, delivered, and received. 50 Our systematic review was focused on intervention details. We did not perform meta-analysis because studies included in our analysis were not all RCTs. Our analysis could not address whether the 5A’s based research is efficacious in changing care provider’s counseling behaviors or the patient’s weight outcomes.
Conclusion
This systematic review examined how the 5A’s Framework was integrated in research on obesity and weight counseling. Findings indicated that the 5A’s Framework has been integrated in interventions with the intent to impact counseling competencies/skills of the health care provider and the patient’s weight management behaviors and outcomes. The 5A’s Framework can be used in training programs for medical students and physician and non-physician health care providers. It can also be utilized to develop assessment tools to evaluate counseling behaviors of health care providers.
Supplemental Material
Supplemental Material - Integration of the 5A’s Framework in Research on Obesity and Weight Counseling: Systematic Review of Literature
Supplemental Material for Integration of the 5A’s Framework in Research on Obesity and Weight Counseling: Systematic Review of Literature by Carol Shieh, Heather K. Hardin, Mandelle Dreu Doerstler, and Anna Liss Jacobsen in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.