
Abstract
As the number of people living with chronic diseases climbs upward, novel methods to address the root causes of these disease are necessary to transform the state of our nation’s health and our health care system. Interventions directed at making lasting lifestyle changes can have a major impact on the overall health of patients. In this pilot study, 4 obese patients, with unhealthy habits and abnormal blood profiles and biometrics, were able to significantly improve their lifestyles and their lab values with the 3-month intervention of a lifestyle medicine team, including a physician trained in lifestyle medicine, a certified wellness coach, a licensed nutrition specialist, a physical therapist, and a licensed mental health professional. Two patients had type 2 diabetes, and all 4 were hypertensive (blood pressure > 120/80 mm Hg). After the intervention, all improved their nutrition and increased their physical activity. In addition, all experienced improvements in lipid counts, blood pressure, weight loss, and cholesterol. The diabetic patients’ levels of hemoglobin A1C dropped to normal. These successes show the benefits of a lifestyle medicine team approach.
‘Together they can assess readiness to change, find intrinsic motivators, overcome obstacles, cocreate goals, and hold patients accountable for actions and goals.’
Introduction
The United States and many other countries are facing unprecedented unhealthy lifestyle challenges, including myriad fast food choices, sedentary work and leisure habits, serious weight management issues, and overall failure and confusion about developing habits to achieve optimal health and well-being. This adds to the burden of diseases such as diabetes, heart disease, stroke, cancer, metabolic syndrome, and senile dementia, all of which place a significant burden not only on the patients and their families but also on the health care system as a whole.
Lifestyle medicine is a growing area of medicine that focuses on empowering patients to adopt healthy habits. As defined by the American College of Lifestyle Medicine, “Lifestyle Medicine involves the therapeutic use of lifestyle, such as a predominately whole food, plant-based diet, exercise, stress management, tobacco and alcohol cessation, and other non-drug modalities, to prevent, treat, and, more importantly, reverse the lifestyle-related, chronic disease that’s all too prevalent.” 1 Increasing evidence supports that patients may know that they need to exercise more and eat healthy foods, but on their own, they are rarely able to follow through and make lasting change. The combined efforts of a physician experienced in lifestyle medicine plus a health coach utilizing coaching techniques and minimizing the expert approach of advising, telling, threatening, demanding, and cajoling can provide important collaborative support to help patients adopt and maintain change. Together they can assess readiness to change, find intrinsic motivators, overcome obstacles, cocreate goals, and hold patients accountable for actions and goals. 2 A nutrition specialist, physical therapist (PT), and mental health professional add to the lifestyle medicine team’s power by addressing the specific needs of each patient in these areas. This team strategy generates a foundation for success in physical activity, nutrition, eating habits, stress management, and positive mental attitude.
Health and wellness coaching is a burgeoning field in health care. These allied health care providers are trained in facilitating change. Using well-studied and accepted psychological principles, theories, and strategies, such as the transtheoretical model of change, motivational interviewing, goal setting theory, appreciative inquiry, and positive psychology, these trained coaches are skilled in listening to patients, providing them information that they need and want to hear, uncovering powerful motivators, and brainstorming solutions to problems. They do not force change. They enable it. They are negotiators, collaborators, and partners with the patient. Health coaching involves taking a patient-centered approach, where individual patients are directly involved in setting goals, taking personal responsibility for any changes, and focusing on finding techniques that work for him or her. The providers’ roles in this process are effective when they are able to guide individuals through that change process, helping increase the patient’s self efficacy, utilizing the patient’s individual strengths, and building a trusting relationship instead of simply directing behavior or educating through threatening patients with worse-case scenarios. 3
In the United States, nearly 75% of health care costs are related to preventable conditions, yet only 3% of health care dollars are actually spent on prevention. This presents a major problem for the future of health care spending because direct medical costs of cardiovascular disease alone are expected to triple, from $273 billion to $818 billion between 2010 and 2030. 4 Given these statistics, there is a dire need for evidence-based studies that support the role and the value of interventions from a team of health care professionals who not only educate patients about their diseases and risk factors but also empower and inspire patients to collaborate on making sustainable life changes that can affect the health of individuals, families, communities, and our nation.
A patient’s ability to create and commit to behavior change is imperative for lowering the risk for chronic disease, lowering health care costs, and improving the patient’s ability to live a healthy life. Diabetes is one example where appropriate lifestyle changes, through the help of wellness coaching, have been shown to dramatically reduce the risks of the disease. In a randomized trial of 56 type 2 diabetics, Dr Ruth Wolever and her colleagues at Duke evaluated the effect health coaching had on outcomes of glycemic control and behavior change. They concluded that by integrating the individual needs and values of the patients, these diabetic patients were better able to make lifestyle changes that included adherence to medication schedule, diet and exercise, and stress management, which had a positive impact on their control of diabetes as determined by A1C level indicators. 5 In addition, in an integrative review by Olsen and Nesbitt, 6 they and their colleagues compiled a wide range of conditions where coaching interventions have demonstrated a significant improvement for the patient, including diabetes, excessive weight, and high cholesterol. Other individual studies show that coaching interventions have a positive impact on cancer pain, 7 cardiovascular disease, 8 and pediatric asthma management. 9
Another method for obtaining objective measurements of positive lifestyle changes is to look at biometric measurements, a method used in this case series. Over the years, health care, medicine, and insurance companies, have focused on blood profiles and biometric measurements of healthy and unhealthy adults and the relationship of these factors to the patient’s nutritional and physical activity choices. How a physician and a lifestyle medicine team can alter these outcomes has direct relevance to our nation’s overall health as well as its financial health. Lifestyle medicine techniques can address not just lowering risk factors but also how a patient can sustain behavior change and maintain a healthy lifestyle over time.
This particular case series emphasizes the importance of personalized attention to each patient, meeting them where they are and providing them with the knowledge, tools, and skills they need to successfully modify behaviors and empower them to take care of their own health. Furthermore, in contrast to other larger studies that work to demonstrate positive results of behavioral change on health, this case series strives to provide detailed information about the specific methodology successfully used by the lifestyle medicine team consisting of the physician, health and wellness coach, licensed nutrition specialist, PT, and mental health professional.
A team approach has been reported in the literature with a primary prevention program in low-income minority women diagnosed with metabolic syndrome, called the HAPPY Heart program. In this study, the team included a primary physician, cardiologist, nutrition specialist, PT, and health coach. 10 Over the course of 2 years, this multipronged intervention decreased the rate of metabolic syndrome from 64.7% to 28.2%. This intervention included health coaching by phone or in person 1 to 2 times a week for the first 3 months and once a month thereafter. The health coaching techniques, skills, and strategies used with the patient were not discussed in the article. The PT performed an initial baseline evaluation and designed an individualized exercise program. Free exercise classes were also offered to the participants. The nutrition specialist performed an evaluation and created an individualized nutrition plan. There were free cooking classes offered as well. In addition, at no charge, the participants were offered relaxation, meditation, and tai chi classes as well as smoking cessation and pharmacological support as needed for tobacco use. This was a robust, community-centered intervention with many extra free classes and support systems in place that are not feasible for the average medical practice to offer patients.
In this case series, the lifestyle medicine intervention was centered at one physician’s office, and it focused on the lifestyle medicine team, with the clinic visits as the power of the process. Men and women were studied (predominantly men), and the goal was adopting healthy habits with the aim of lowering biometrics that put the patients at risk for lifestyle-related disease, such as diabetes, cardiovascular disease, stroke, obesity, metabolic syndrome, and cancer. This study looked at more than 1 specific disease. In addition, the team included only 1 physician and that physician was trained in lifestyle medicine. A mental health professional was added to the team of clinicians. It is a similar team model used in the HAPPY Heart study but targets a different population, uses a different composition for the team, and only uses members of the team for the intervention, not free classes or other extra services. The team example and the methods utilized within this brief outpatient pilot intervention can serve as a guide for other practitioners looking to empower both male and female patients at risk for various chronic diseases to change their unhealthy habits and maintain healthy ones. We provide follow-up data at 6 months and 1 year.
This case series is a pilot study that helps fill a gap in the current literature by directly examining how the combination of a lifestyle medicine team, including a lifestyle medicine physician, a certified health and wellness coach, a licensed nutrition specialist, PT, and licensed mental health professional could positively affect behavior, cardiovascular blood profiles, and health biometric measurements. By providing details about the health coaching techniques utilized and the duties of each member of the team, other health care providers can work to replicate these findings using similar strategies.
Methods
The main study question was, “Would patients, who have, or are at greater risk for, chronic diseases benefit from the support of a lifestyle medicine team, including a physician, certified health coach, licensed nutrition specialist, physical therapist, and licensed mental health professional, in making healthier nutritional and physical activity choices?” In this pilot study intervention, benefit was measured by how successful the patients were at increasing healthy behaviors as well as improving their blood profiles and biometrics, thus lowering their risk for chronic diseases or even reversing the process altogether. Four patients consented to our case series (1 female and 3 male patients; all older than 50 years) as a result of their similar health concerns and their intention to undergo a brief outpatient lifestyle medicine intervention lasting a total of 3 months.
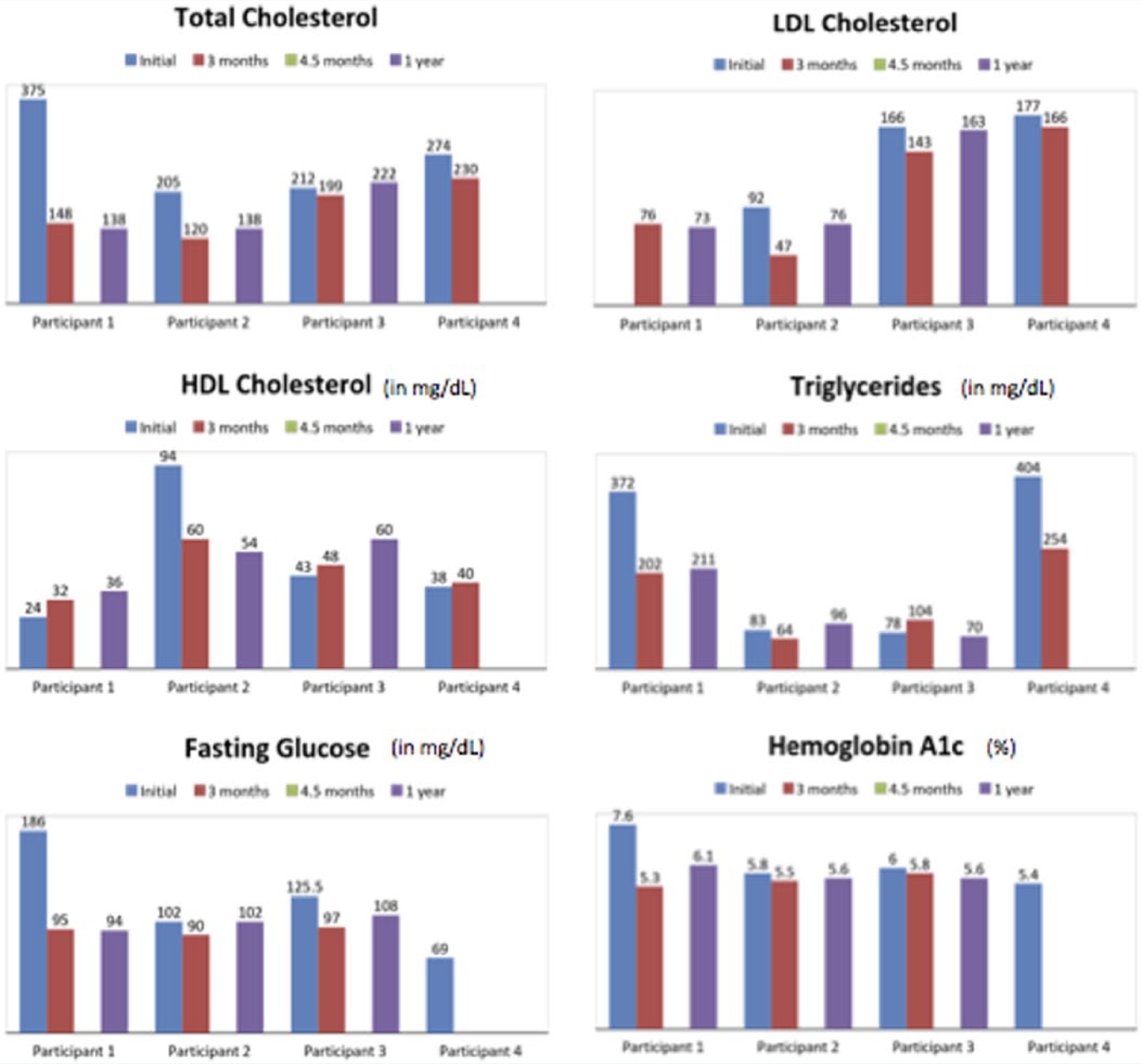
All 4 patients had blood drawn to establish a baseline blood profile targeting total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, fasting glucose, and hemoglobin A1C numbers (Figure 4). They also had biometric readings taken for blood pressure, waist circumference, weight, body mass index (BMI), and percentage body fat for baseline measurements. Three months later, in March 2013, all 4 patients agreed to have a second round of blood drawing and biometric measurements. Both blood profile numbers and biometrics were compared. The complete set of biometric tests completed include blood pressure and waist circumference; bioimpedance, including weight, BMI, percentage body fat, body fat mass, and skeletal muscle mass; a modified Mediterranean diet score and health habits score; and a health risk assessment developed from a questionnaire and database from the University of Michigan. Finally, additional lab tests were performed to include advanced lipid profiles (currently used HDL labs), advanced metabolic profiles (currently used HDL labs), advanced micronutrient testing (determination of levels of 37 vitamins and micronutrients currently used by SpectraCell labs), specified cardiovascular genetic risk factors (currently used HDL labs), and screening tests for thyroid, liver, and renal labs.
Change in Blood Profile Numbers.
The lifestyle medicine physician was trained in lifestyle medicine at Loma Linda’s School of Public Health, gaining a MPH in Lifestyle Medicine; completed externships with Institute of Lifestyle Medicine at Harvard Medical School and St Helena Center for Health; attended CME courses on the topic of lifestyle medicine through the Active Lives: Transforming Ourselves and Our Patients at Harvard Medical School; and completed Healthy Kitchens, Healthy Lives at the Harvard Medical School and Culinary Institute of America. The physician was knowledgeable and skilled in behavior change, including the transtheoretical model of change, motivational interviewing, social cognitive theory, and theory of reasoned action.
Patients met with the physician for an initial 60-minute meeting; a 60-minute, 1-month follow-up meeting; a 30-minute follow-up meeting each month thereafter; and a 60-minute visit at the end of the intervention. During the first visit, the physician completed an initial, focused, preventive medicine–type evaluation; ordered basic labs and some advanced cardiovascular, metabolic, and nutritional testing; introduced the idea of behavioral change; listened to the patient’s history and concerns; and introduced patients to the health coach. Follow-up visits involved a combination of listening, supporting, and educating. The physician and patient shared discussions about the importance of lifestyle changes for health, overall health check-ins, quarterly standard biometric tests, and specific labs as needed, per the physician’s discretion.
The patients were guided in terms of physical activity and diet. The Full Plate Diet was used as an example of healthy eating. Following this whole foods, plant-based diet, participants were encouraged to increase their intake of whole grains, fruits, vegetables, and beans/legumes. For exercise, the patients were encouraged to reach the national physical activity guidelines of accumulating 150 minutes each week of moderate-intensity physical activity, strength training twice a week, and flexibility training weekly.
The Wellness Coach was a certified and trained coach who had completed a Master’s of Science in Fitness and Sports Management and obtained certification from the American College of Sports Medicine, Wellcoaches Wellness Coach-Core Competencies certification, Wellcoaches Professional Wellness Coach Certification, Institute of Lifestyle Medicine Scholar, and Immunity to Change Coaching certification.
Each patient had a 60-minute initial visit with the health coach followed by 10 weekly or biweekly 30- to 60-minute meetings. At the initial visit, the health coach interviewed the patient to identify individual goals and to gain an understanding of specific challenges, barriers to change, character strengths, and support networks. With this information, the health coach was able to tailor future sessions to meet the needs of each patient.
In contrast to the Lifestyle Medicine Physician, the health coach’s work focused on understanding not just what needs to change for the individual’s success but how to help that person make those changes. This was accomplished through a variety of techniques, many that overlap and reinforce those of the physician and some that take more time and require specialized training. For example, the health coach used motivational interviewing, the transtheoretical model of change, and active listening, as did the physician. However, in addition to these skills, the health coach also used appreciative inquiry with curiosity, constructive developmental theory, language of ongoing regard, visualization, mindfulness, strengths-based approach, immunity to change techniques, SMART—specific, measurable, action oriented, realistic and time sensitive—goal setting, and positive psychology. Each coaching session was structured around the basic format of outlining the purpose of that specific meeting, addressing successes and challenges of the past week, creating a deeper learning experience for the present sessions, and cocreating new goals for the following week. At the end of each coaching session, the patient identified a single takeaway from the meeting that helped set a focus for the patient.
Whereas the majority of the interactions between medical professionals and patients occurred with the physician and health coach, many other health professionals were involved, depending on the needs of the patients, including the licensed nutrition specialist, PT, and licensed mental health professional.
The licensed nutrition specialist’s role was to provide an initial nutritional evaluation with ongoing recommendations tailored to each individual. The Full Plate Diet, introduced by the lifestyle medicine physician in the initial meeting, was used to reinforce the principles of a whole food, plant-based eating pattern and served as the overarching guide for nutrition. Each patient, then, had at least 3 follow-up visits with the nutrition specialist. These visits were specific to the needs of each patient, both nutritional and lifestyle related. Some learned meal planning and home food preparation. Others, who primarily ate out, needed help planning and ordering healthy options from a restaurant menu. Most needed and desired grocery shopping support. The nutritionist met the patients where they were and worked to provide the support that each one needed by personalizing the recommendations and plans.
The licensed mental health professional provided an initial lifestyle and behavior evaluation, an evaluation of each patient’s readiness to change, an evaluation of resilience, and screening for anxiety, depression, and other mental health disorders. Each patient was then provided with recommendations. None of the patients had any significant mental health disorders warranting a diagnosis or medication. However, most of them had significant health behavior issues and social issues, which made behavior change more difficult. Ultimately, future visits with the licensed mental health professional were used to provide more intensive support of behavioral changes, with a focus on mood and stress management.
The initial physical therapy evaluation included grading balance, flexibility, muscular strength, muscular endurance, aerobic capacity, posture, and gait. The focus was on function and fitness. A complete exercise history was also gathered. From this evaluation, PTs generated a report with specific exercise recommendations. Each patient then had at least 3 follow-up visits with the PT to work on identified issues and create home-based programs that guided the patient to continue to work on strength and function.
The use of a team model that includes a licensed nutrition specialist, PT, and mental health professional is essential. Though lifestyle medicine physicians can provide basic nutrition, exercise/physical activity, and health behavior information and an experienced health coach can provide support in health behavior, facilitating change, identifying internal motivators, and strategizing around obstacles, often, patients have extremely poor nutritional habits, inadequate exercise habits with or without joint issues, decreased functional capacity, and emotional pain as well as instability. In these instances, patients require greater expertise in these specific areas to succeed.
Insurance covered most of the cost of lab tests in the study. However, insurance did not cover the fees for the physician, the licensed nutrition specialist, the PT, the licensed mental health professional, or the health coach. Thus, the reimbursement for all these professionals was bundled into a flat fee, which the patient paid out of pocket. The long-term health benefits of a healthy lifestyle and the evidence-based reviews on the benefit of health coaching in making these changes emphasizes the need for there to be some payment within the health care system for these incredibly beneficial services that both reverse and prevent poor health conditions and habits. However, at this time, it is necessary for the patients to invest in their health until the health care payer system catches up. The outcomes of this study will help prove the benefit of this type of individualized care, which would actually save the third party payers large sums of money in the future.
Results
In this study, initially, patients were assessed in the following areas: nutrition, physical fitness, health behavior, and preventive medicine. From the diagnostic labs drawn, it was noted that all patients had total cholesterol levels >200 mg/dL and LDL cholesterol >130 mg/dL. All 4 patients also had elevated blood pressures (>120/80 mm Hg, prehypertensive/hypertensive). More than half of the patients also had triglycerides >150 mg/dL, low HDL cholesterol <40 mg/dL, elevated blood glucose levels >100 mg/dL, and elevated hemoglobin A1C levels >5.7%. Each patient was in the obese category, with a BMI >30 kg/m2. Waist circumferences were >35 inches for the women and >40 inches for the men, which put them in a high-risk category for several chronic diseases. Weight and percentage body fat were elevated for each patient. Also, 2 patients had type 2 diabetes, and 2 patients had gout.
Results for labs and biometrics at baseline, 3 months, 4.5 month, and 12 months are summarized in Figure 1. The results overall at the 3-month mark show clear improvement in all markers. Notably, 2 patients with diabetes experienced normalization of their fasting blood glucose as well as normalization of their hemoglobin A1C levels. In addition, there were marked reductions in total cholesterol and LDL cholesterol values, including total cholesterol reductions of 85 points and 225 points in 2 different patients.
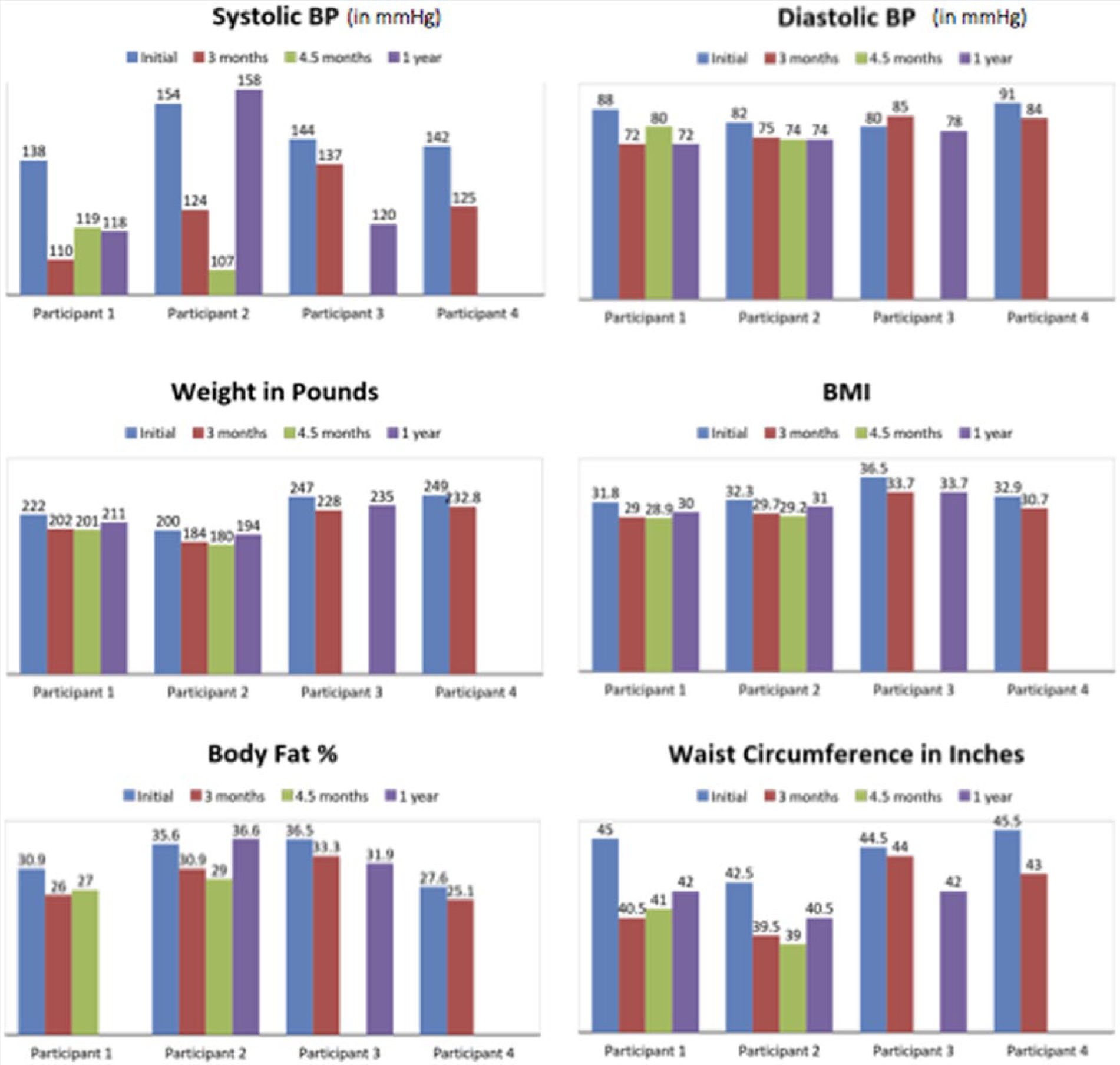
Biometric Changes Over Time.
Data from a 1-year follow-up were able to be obtained in 3 of the 4 patients. None of the patients actually gained weight when comparing their initial weight with their final weight. Patients 1, 2, and 3 all saw decreases in body weight both at the 3-month and 12-month marks. Patients 1 and 2 additionally saw improvements in total cholesterol. Whereas participant 3 only saw improvements at the 3-month mark, his LDL was lower and HDL overall higher by the end of the year. His waist circumference was 2.5 inches less at the end of the year.
This patient is a corporate accountant and workaholic who frequently skips breakfast, eats very little for lunch, and eats “whatever my wife prepares” for dinner. His wife was not on board with significant diet change. In addition, this patient started working out with a personal trainer during the first 3 months. However, when tax season arrived, he went back to working 12-hour days and paying very little attention to his lifestyle habits. His only exercise would be his monthly walk with the lifestyle medicine physician. Finally, participant 4 had a great start—that is, 16 pound weight loss and 44 point drop in total cholesterol. Unfortunately, he then decided to exit the program and “do it on his own.” The lifestyle medicine physician was not able to get him to return for testing.
The behavior changes that were fueling these biometric changes are noted in Figures 2 and 3. There was a trend in all 4patients toward increased intake of fruits and vegetables, whole grains, and beans/legumes when comparing the data at baseline with those at 6 months. Also, all 4 patients increased their strength training and cardio activity after 6 months, with 3 patients initiating strength training and cardio programs as a result of the intervention. None of the 4 patients was involved with a regular cardio program at baseline.
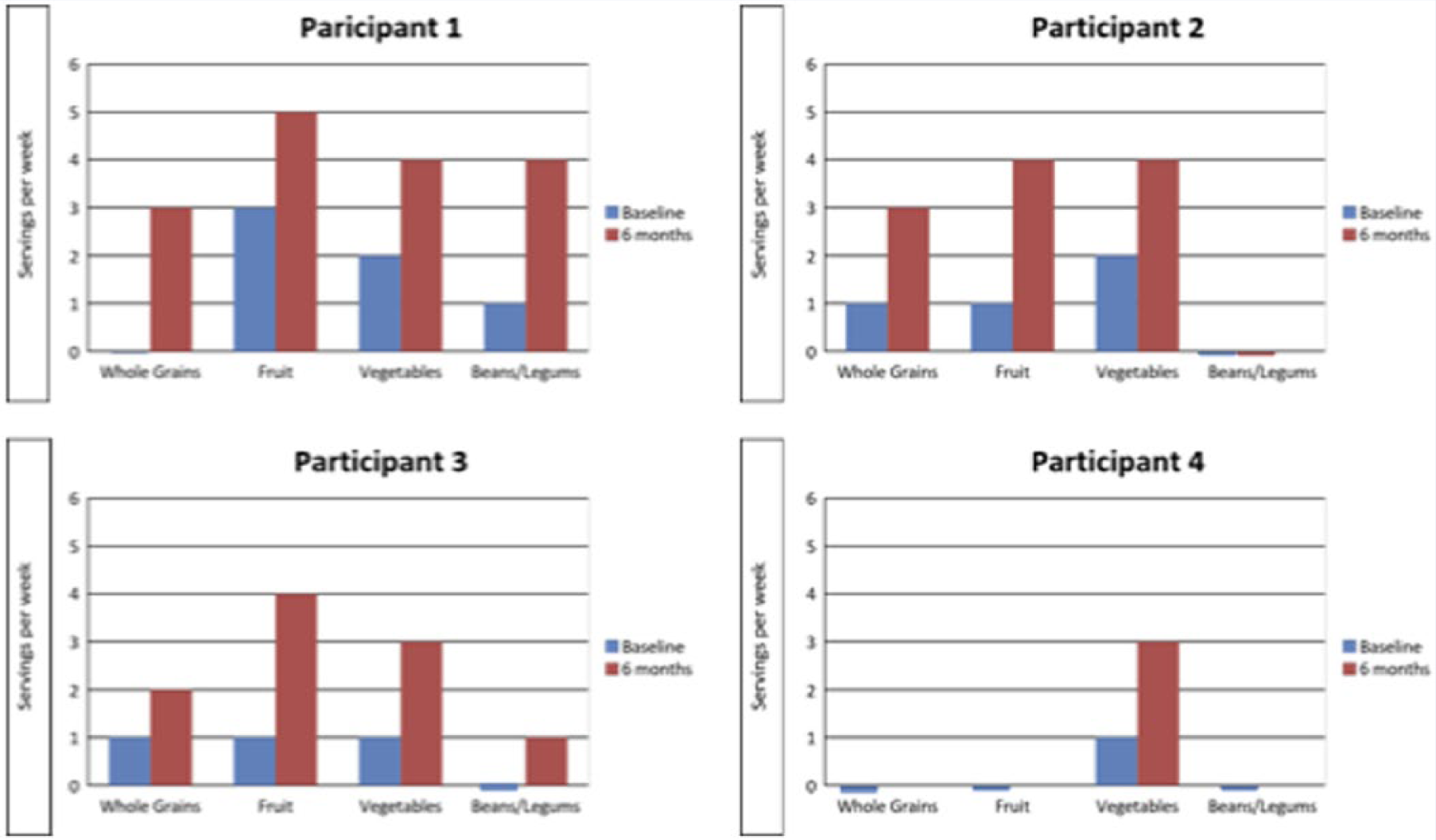
Change in Diet Behaviors in Servings Per Week.
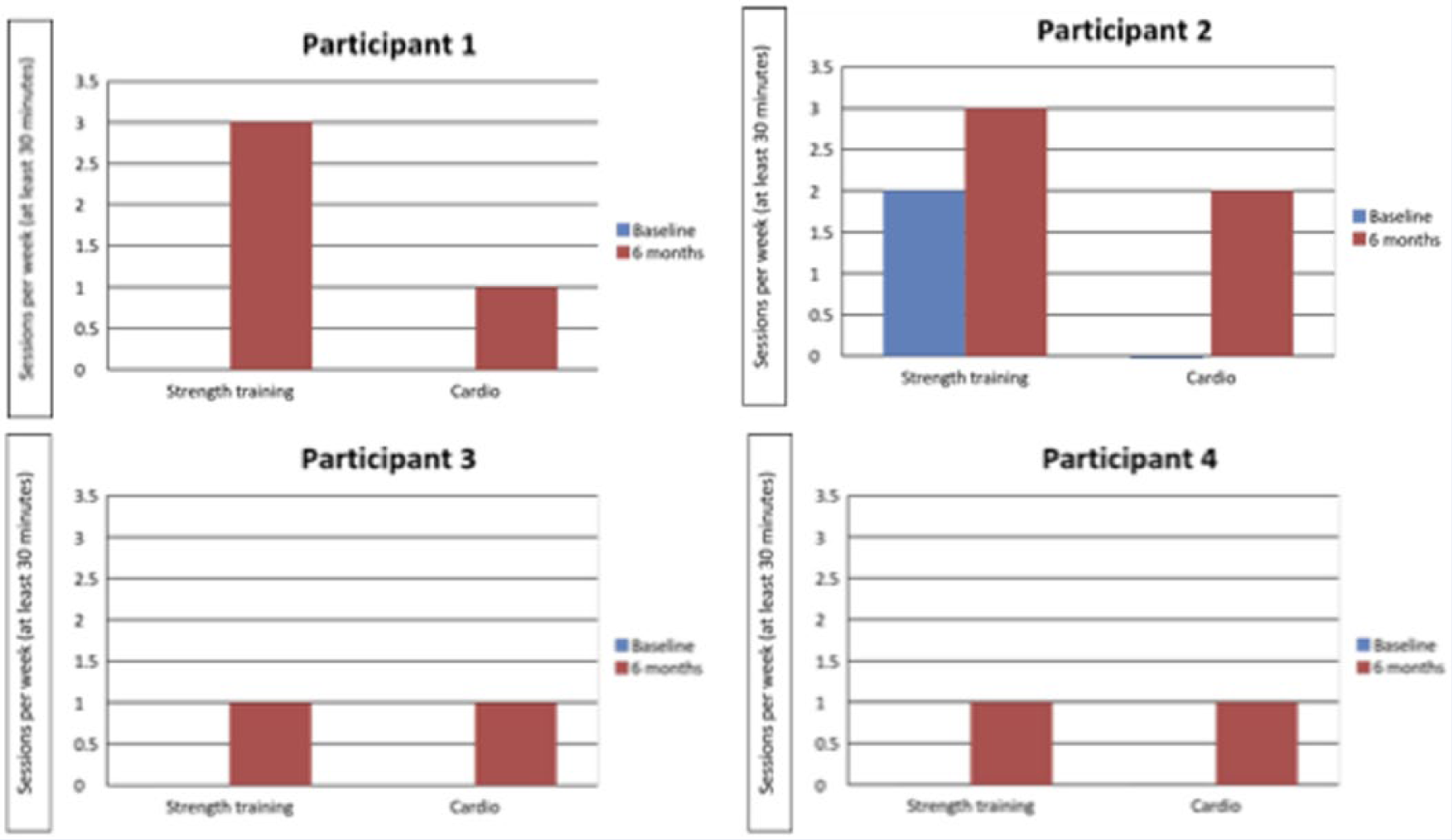
Change in Exercise Behaviors in Session Per Week.
In terms of qualitative data, patients reported learning the importance of a high-fiber diet as well as the importance of encouragement from family and friends. One patient noted better sleep, feeling better overall, and that “a new way to eat, is a new way to live life.” One patient reported not knowing how to resolve health problems naturally before the intervention; she could now eat complex carbohydrates and her blood sugar levels kept improving. Other comments on noted benefits included, “My old diets were sapping my energy, and now by changing to a more high fiber diet, my energy is up, my cardio training has increased, as well as endurance, and I have the desire to sustain it.” One patient said, “People better understand their blood profile numbers and from this understanding comes an improved recognition of how and why to lose weight. Making a commitment is even better.”
It should be noted that no negative outcomes were experienced, other than some patients having to buy new clothes and belts because the old ones were too big.
Discussion
The findings of this Lifestyle Medicine Team pilot intervention case series are consistent with research demonstrating that changing lifestyle behaviors helps patients manage disease and the recent research that states that health and wellness coaching interventions help patients adopt healthy habits. These lifestyle changes have a direct positive effect on the patient’s management of chronic diseases and their comorbidities. The initial results include dramatic improvements in blood lipids, blood glucose levels, blood pressure, weight, BMI, body fat percentage, and waist circumference. The biometric and blood work changes at 1 year, though not as dramatic as the 3-month results, are still powerful demonstrations of reducing the risks of morbidity and poor health outcomes. The fact that all 4 patients adopted a healthier diet and increased their physical activity with this pilot intervention is important because most people know that they should eat better and exercise more, but they do not know how to accomplish these broad, overarching goals. The team was successful in empowering the patients to adopt healthy habits.
The partnering of a lifestyle medicine team with physician, health and wellness coach, licensed nutrition specialist, PT, and licensed mental health professional, in a safe, supportive environment, can significantly improve the ability of patients to identify motivators, enhance self-efficacy, and develop the critical and creative thinking skills to plan, assess, alter, and follow through with action plans for behavior change. Using the expertise of all these individual health care providers and having each one adopt a consistent coach approach communication style is an important part of a lifestyle program. When communication is open, greater trust is built. Likewise, it ultimately helps motivate and inspire patients to take responsibility for their health decisions. It is through the challenges and opportunities for taking responsibility for one’s health that patients grow and learn.
There is a coaching cycle that has been examined and previously documented as an effective communication strategy. 11 In this cycle, there are 5 steps that the coach follows, including (1) expressing empathy, (2) aligning motivation, (3) building confidence, (4) setting SMART goals, and (5) holding patients accountable to change. The first step in the cycle—empathy—allows the provider to truly connect with the patient and their needs. This is a necessary aspect of the lifestyle medicine intervention that hinges on understanding the patient’s life circumstances, fears, stressors, 10-year vision, and any previous failed attempts at behavior change for the individual. These historical facts play an important role in the change process. This provider empathy alone has been shown to correlate with patients’ improved control over risk factors such as hemoglobin A1C and LDL levels. 12 So listening and reflecting back to the patient are ways in which the coach or any provider can demonstrate empathy to the patient.
Identifying a powerful motivator is critical. External motivators can work for a short time, but it is internal motivators that allow for lasting behavior change. Thus, it is important for the provider to understand those intrinsic motivations, such as feeling energized after a workout or feeling calmer throughout the day when eating 3 meals and 2 small snacks each day. Identifying a patient’s strengths and calling on them to help the patient adopt healthy habits can increase confidence. Creating small manageable goals that the patient can most certainly achieve brings about the feeling of success, and success breeds success.
By setting SMART goals, the provider is helping set the patient up for success. SMART goals outline what the patient needs to do, breaks it into manageable steps, provides a reasonable time frame, and displays measurable outcomes to provide specific feedback on progress. This helps sustain motivation and provides measurable data for the provider and patient to troubleshoot as well as make changes to ensure success. Finally, none of the goals set are of any use if the patient does not follow through. Providing a structure of accountability not only reinforces the provider-patient relationship but allows open communication and dialogue to make sure that intermediate goals are met and problems or barriers are overcome. 11
Each individual success and achievement (increased physical activity, improved blood profile and biometrics) provides patients new motivation, insight, and confidence for setting and attaining healthy goals, going forward. This in turn can create a new desire to improve both their health and well-being. Recent systematic reviews conducted by a number of researchers indicate the potential benefit effective wellness coaching programs can have on patient health. Olsen and Nesbitt 6 discuss multiple and significant benefits for patients participating in such programs. Wolever et al 3 and Kivela et al 13 also affirm the lasting benefits and effectiveness of wellness coaching programs and stress the positive role that providers can play in facilitating these behavior changes. All stress the need for more research to be conducted to establish best practices and methodologies for programs to maximize their benefit to patients.
Collaboration and treating the patient as the expert in his or her own life experiences, dreams, and desires are key elements of the lifestyle medicine collaboration. This coach approach, with an emphasis on connection and teamwork, is one factor that sets the lifestyle medicine intervention apart from traditional medical services.
This case series report proposes and tests a new model of medical practice, which includes a lifestyle medicine team made up of a physician, a health and wellness coach, licensed nutritional specialist, PT, and mental health professional. This is a pilot study. The team model used in this 3-month lifestyle medicine intervention is one that uses a collaborative approach among providers and, importantly, a collaborative approach with the patient. A focus on both a healthy diet and physical activity, along with setting goals and keeping patients accountable while personalizing the intervention to address specific obstacles and call on powerful, individual motivators, is a model that can be replicated in a number of medical practices. In addition, this case series is an example of how to include lifestyle medicine in clinical practice without waiting for insurance to cover the costs and provides a payment strategy that can work for some patients who are able to pay an additional fee. This pilot study of 4 cases provides a template for team lifestyle medicine interventions that can fill the need for this type of patient care that is not currently covered by the United States health care system.
In our study, analysis of the patient’s behaviors, blood profiles, and biometrics suggests that having frequent collaboration and support from the lifestyle medicine physician and health and wellness coach during the first 3 months of the intervention positively affected the patient’s motivation and decision making, and improvements continued to be significant 9 months after the intervention, which was 1 year after the start of the pilot study.
In addition, this case series provides a collection of blood profile measurements and biometric indicators that may be useful in the future for yearly visits with a patient’s primary care provider. During a time when chronic diseases are being diagnosed in unprecedented numbers, enhancing the ability of patients to be able to make decisions affecting their health is a key competency for lowering health care costs and also improving personal responsibility.
This pilot study is limited by the number of participants and the follow-up time of 1 year. There is a need for further research on the efficacy of using lifestyle medicine teams in the doctor’s office, similar to this one. Future research should include longer follow-up periods to test for sustainability beyond 1 year. A larger number of participants and randomized controlled trials will add value and power to the results of future studies.
There is a growing interest in lifestyle medicine and lifestyle health promotion. In a recent study in Sweden, a multicenter effort to utilize lifestyle medicine teams in primary care centers to promote healthy habits was developed to help physicians and their practices address the growing need for behavior modification in the realms of healthy eating, regular physical activity, consuming alcohol only in moderation, and smoking cessation. 14 Traditional medical practice did not adequately address lifestyle because of time constraints, negative attitudes toward lifestyle promotion among providers, and lack of a clear lifestyle promotion program for patients. This intervention, which was designed to enable physicians and their practices to adopt a successful lifestyle promotion program, revealed that the intervention did change the attitudes of physicians about lifestyle promotion, making them more positive and feeling more competent. However, the intervention fell short in its ability to reach patients because of the difficulty the centers had with in-house referrals for healthy lifestyle promotion. Teamwork and coordination of the lifestyle promotion pieces were not fully realized in this Swedish study. Their conclusion was that “more research is needed on lifestyle promotion referral structures in primary care regarding their configuration and implementation (p. 1).” This pilot study with 4 cases serves to help answer the call for more research into a comprehensive program with in-house referrals.
Conclusion
Our pilot study adds to the current scientific body of evidence demonstrating that improved health outcomes can be obtained through a lifestyle intervention centered at one physician’s office with a focus on weight loss, increased physical activity, and fostering healthy nutrition habits. Each of these can be significantly improved when the intervention includes an integrated team of health professionals.
Because evidence in support of the benefits of health coaching to prevent and treat chronic disease is mounting, coaching skills delivered by a lifestyle medicine practitioner and or a health coach need to be incorporated into yearly annual visits as well as follow-up visits in which behavior change is addressed. This study serves to support this approach.
This case series highlights the role physicians and health coaches can play in creating sustained behavior changes that improve individual health outcomes. By playing an active role in identifying areas where patients need education and support and helping them understand how to access resources necessary to make those changes, medical professionals can help them take the required steps to make lasting health improvements without extreme medical interventions. Working with a team of allied health care providers, including licensed nutrition specialists, PTs, and licensed mental health professionals, is a valuable way to meet the needs of the patients regardless of their complexity.
By providing a working model of in-house health promotion services using a physician, nurse, certified health coach, licensed nutrition specialist, PT, and licensed mental health promotion, all working together as a team, this case series serves as a pilot study and an example for further research into a team approach to lifestyle medicine. To our knowledge, this is the first case series describing the specific roles of each team member while clearly demonstrating the skills, techniques, and support offered by the health coach. In addition, this case report also demonstrates the successful use of a lifestyle medicine team to effect behavior change in both men and women with chronic disease with results after a 3-month intervention and follow-up in 1 year. Further research should expand this method through large group sizes, control groups, and randomization.
A lifestyle medicine team approach is an intervention that can be incorporated in most physician practices, especially if they are connected to a hospital where there are licensed nutrition specialists, PTs, and mental health professionals. Each member of the team helps in assisting the patient in a specific way, related to their area of expertise, but all members embody a similar counseling style, with a supportive, compassionate, collaborative tone. They are unified in their overall goals and work with the patient, treating the patient as the expert in their own behavior and experiences. This pilot study can serve as a model for future medical practices, so that lifestyle medicine teams can successfully foster lasting change in their patients and, thus, helping their patients confidently and effectively tackle unhealthy habits.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Frates is on the board at Curves.