
Abstract
Adolescents from low-income households and minority groups are disproportionately affected by obesity compared with their non-Hispanic white counterparts. Engaging in health promoting behaviors such as routinely eating healthy foods and snacks and engaging in physical activity are ways of preventing and reducing obesity and obesity disparities. The major purposes of the present study are (a) to identify the motivators of and barriers to eating healthy foods and snacks among culturally diverse adolescents and (b) to determine if the strengths of endorsement of these motivators and barriers differ by race, gender, and age. In the present study, a series of factor analyses was used to identify the motivators of and barriers to eating healthy foods and snacks among the culturally diverse adolescent participants (N = 172) in the national study. Specifically, an adolescent motivator of eating healthy foods and snacks scale, adolescent barrier to eating healthy foods and snacks scale, and subscales for each of these 2 scales were identified. The adolescent motivator subscales found were Knowledge and Commitment (α = .86) and Routine (α = .87). The adolescent barrier subscales found were Lack of Exposure (α = .72), Pessimistic Attitude (α = .80), and Temptation (α = .59). MANOVAs were used to determine if the mean scores for these scales and subscales differ by race, age, and gender. Nonsignificant differences were found among the mean scores for these scales and subscales. Results have implications for customizing adolescent health promotion interventions, including those to reduce and prevent obesity.
‘Obesity affects approximately 12.5 million youth in the United States, which roughly equates to 17% of the population of this country’
Evidence is mounting that adolescent obesity is an alarming epidemic in the United States. Consequently, in this country, the promotion of adolescent health has become a major priority.1,2 The national focus on obesity is evident given that First Lady Michelle Obama has spearheaded a health initiative with the ambitious goal of resolving the American youth’s obesity problem within a generation. 3
The statistics concerning adolescent obesity in the United States warrant further research and intervention. Obesity affects approximately 12.5 million youth in the United States, which roughly equates to 17% of the population of this country. 4 Obesity among adolescents in the United States is now recognized as a national epidemic. Furthermore, obesity is also a health disparity disease as indicated by the reality that racial and ethnic minorities are disproportionately affected by this growing obesity epidemic. 4
Over the years, researchers have been uncovering the causes of obesity and the health-related consequences that occur in association with this disease. Data suggest that the contemporary obesity epidemic may be fueled by poor nutrition, 5 lack of physical activity, 6 increased screen time (ie, television watching), 7 and inadequate health literacy. 8 Youth obesity has been associated with adverse health outcomes such as hypertension, high cholesterol, and abnormal glucose tolerance or diabetes.4,9 Along with physical health impairments, adolescent obesity may contribute to victimization through stigmatization. For example, one study 10 concluded that overweight adolescent males and females are more likely to be recipients of bullying than their nonoverweight counterparts and that the amount of bullying increased with weight.
There is much research indicating that engaging in health promoting behaviors such as healthy eating and physical activity is critical to reducing and preventing obesity among adolescents as well as among adults. 11 For example, it has been found that early adolescent dietary intake patterns may help predict obesity in young adulthood in women.12,13 It has also been found that adolescents who participate in physical education 5 days a week may decrease the odds of adult obesity by 28%. 14
Due to the fact that adolescents often eat junk food (ie, food and snacks high in fat, sodium, and/or sugar and thus unhealthy) as part of the adolescent experience, 15 it is particularly important to develop interventions and strategies that foster adolescents’ engagement in eating healthy foods and snacks. Yet, to develop such interventions, it is important to know the motivators of and barriers to eating healthy foods and snacks among adolescents. Currently, there is a dearth of research that identifies such motivators and barriers. The few common adolescent motivators of healthy eating found in the literature include prevention of disease and becoming overweight 16 and attention to the positive benefits of eating healthy. 15
It is only recently that a reliable and valid measure for assessing the motivators of and barriers to engaging in health promoting behaviors including eating healthy foods and snacks was published. This inventory is called the Youth Form of the Motivators of and Barriers to Health-Smart Behaviors Inventory. 17 It is an inventory designed to be completed by adolescents and children. It is novel in that its items were generated by culturally and age diverse children and adolescents. The racial/ethnic composition of this sample was African American (43%), Hispanic/Latino (27%), Asian American (15%), non-Hispanic White American (11%), and “other” (4.2%). The average age of this sample was 12.19 (SD = 2.4). This inventory is particularly useful because the motivators of and barriers to each of its health promoting behaviors domains (ie, Healthy Breakfast, Healthy Foods and Snacks, Healthy Drinks, and Physical Activity) can be assessed separately for each domain. Thus, this inventory can be used to assess adolescents’ motivators of and barriers to eating healthy foods and snacks—the health promoting behavior domain of interest in the present study.
Many of the past studies that have focused on adolescents’ views of factors that influence their eating habits have not reported race or ethnicity. If race and ethnicity were reported, the samples were primarily composed of non-Hispanic white participants. 18 Identifying race and ethnicity of participants in studies of healthy eating is important because minorities and individuals from low-income households invariably experience some different influences (eg, cultural influences) on their eating behaviors compared with their non-Hispanic white counterparts. For example, the influences on the eating behaviors of adolescents in low-income and minority communities are disproportionately affected by these communities often being located in areas with limited access to fresh food, known colloquially as food deserts. 19
Support for obtaining the views of culturally diverse adolescents regarding the influences on their eating behaviors comes from the fact that much of the past research to identify these influences has involved only experts as research participants. In a systematic review of such research conducted by Shepherdet al, 18 the identified barriers (ie, poor access, cost, and personal taste preference for fast food) and facilitators (ie, familial support, wider availability of healthy food choices, maintaining one’s appearance, and will-power) of healthy eating among youth were identified by professional experts rather than by youth.
In addition to research findings indicating racial differences among adolescents with regard to eating healthy foods and snacks, there are research findings indicating some differences in this health promoting behavior in association with gender (ie, being a female or male adolescent). 20 Bauer et al 20 found that female adolescents tended to regard anxiety about weight as the primary catalyst to eating healthy. It was also found that male adolescents were influenced by maternal and companions’ engagement in eating healthy.
A paucity of research has assessed if there are age and race differences in healthy eating habits among adolescents. Knowing whether such differences (eg, race, gender, and age) exist will shed light on current adolescent health disparities and provide valuable information for creating customized intervention model programs that are readily adaptable for meeting the diverse health promotion challenges of adolescents.
The major purposes of the present study are (a) to identify the motivators of and barriers to eating healthy foods and snacks among culturally diverse adolescents and (b) to determine if the strengths of endorsement of these motivators and barriers differ by race, gender, and age. The following research questions will be examined: (a) What are the motivators of and barriers to eating healthy foods and snacks among the participating sample of culturally diverse adolescents? (b) Are there significant differences in the endorsement of the found motivators of and barriers to eating healthy foods and snacks in association with race, gender, and age?
Methods
Participants
Data from the current study was a part of a larger national sample of youth recruited for a research study to establish the reliability and validity of the Youth Form of the Motivators of and Barriers to Health-Smart Behaviors Inventory. Thus, the sample for the present study consisted of 172 adolescents, ages 11 to 17, who completed the Healthy Foods and Snacks portion of the inventory. The present study defines adolescence as ages 11 to 17 to encompass both younger adolescents (ie, ages 11-14 to denote adolescents in middle school/junior high school) and older adolescents (ie, ages 15-17 to denote adolescents in high school). The average age of these participants was 13.14 (SD = 1.58). Among these participants were 96 (55.8%) females and 71 (41.3%) males. The participants were from 10 states plus the District of Columbia. Specifically, 54.1% were from the South, 1.2% were from the Northeast, 9.3% were from the Midwest, 17.4% were from West, and 18% did not report their home state. With regard to race/ethnicity, there were 39 (22.7%) Asian Americans, 63 (36.6%) African Americans, 36 (20.9%) Hispanics, 18 (10.5%) non-Hispanic Whites, 7 (4.1%) “others,” and 9 (5.2%) participants who did not report their race/ethnicity.
Measures
Demographic Data Questionnaire
The Demographic Data Questionnaire (DDQ) was constructed by the authors to assess the following information for each participant in the present study: race/ethnicity, age, and gender.
The Youth Form of the Motivators of and Barriers to Health-Smart Behaviors Inventory (MB-HSBI-Youth)
The MB-HSBI-Youth 17 is an inventory designed to assess motivators and barriers among 4 health-smart behavior domains (ie, Healthy Breakfast, Healthy Drinks, Healthy Foods and Snacks, and Physical Activity). Each domain of the MB-HSBI-Youth consists of 2 scales, a motivators scale and a barriers scale. Each scale consists of specific subscales. This study only used the Healthy Foods and Snacks scales and subscales. The subscales and a sample item for each subscale in parenthesis for the motivators scale of the Healthy Food and Snacks domain include the following: (a) Knowledge and Commitment (“I understand why healthy foods are good for my body”) and (b) Routine (“Eating healthy is a habit for me”). The subscales and a sample item for each subscale in parenthesis for the barriers scale of the Healthy Foods and Snacks domain include the following: (a) Lack of Exposure (“No one ever taught me how to eat healthy”), (b) Pessimistic Attitude (“I do not like the smell of vegetables”), and (c) Temptations (“When someone cooks or gives me unhealthy food, I eat it.”).
Instructions on the MB-HSBI-Youth are to rate level of agreement with each behavior listed on a 4-point Likert-type scale ranging from 1 (strongly disagree) to 4 (strongly agree). The reliability and validity of the Healthy Foods and Snacks domain are reported by the authors of the MB-HSBI-Youth to be acceptable. 17 Specifically for this domain, the authors reported Cronbach’s α to be .89 for the motivator scale and .85 for the barriers scale. Cronbach’s α for the subscales were reported to be as follows: Knowledge and Commitment, α = .85; Routine, α = .82; Lack of Exposure, α = .77; Pessimistic Attitude, α = .79; and Temptation, α = .62.
Procedure
The researchers for the larger national study (from which the data for the present study were obtained) obtained permission to conduct the study from the institutional review board at the University of Florida. The national study (and thus for the present study) occurred at health care sites, faith-based organizations, schools, and YMCAs that were identified with the assistance of health promotion professionals (eg, leaders of YMCAs and directors of state offices of minority health) across the country. The list of potential data collection sites were contacted via letter or telephone and invited to participate in the study, which involved identifying a site contact person who would recruit study participants and have each participant complete a set of study questionnaires (the assessment battery). Contact persons were individuals involved in their community such as members of social clubs, hospital employees, teachers, and church members.
The contact persons were trained by telephone to enlist participants and administer the assessment battery to each participant. Each contact person then executed these research roles after passing a verbal study execution competency questionnaire. The contact person corresponded weekly by telephone with the researchers to provide updates on their progress and to discuss how to address any research-related problems encountered.
Participant recruitment was conducted through a variety of methods, including word-of-mouth, posting flyers, and making announcements at local churches, YMCAs, schools, and other civic organization sites. Interested potential participants were each given a data collection packet by his or her community contact person. This packet contained a cover letter, an informed consent form for the participating youth’s parent’s/caregiver’s signature, an assent form for the participating youth’s signature, the assessment battery, and 2 envelopes—one envelope for the signed consent and assent forms and one for the completed assessment battery. Two envelopes were given to help ensure anonymity of the participants’ answers to the MB-HSBI-Youth and other assessments. Once researchers received the signed consent and assent forms for each youth participant and the completed assessment battery from a contact person, the researchers mailed the parent/primary caregiver for the youth a $10 money order as compensation.
Results
Exploratory Factor Analyses
To address the first research question (What are the motivators of and barriers to eating healthy foods and snacks among the participating sample of culturally diverse adolescents?), 2 exploratory factor analyses (EFA) with promax rotations were conducted employing a weighted least squares mean- and variance-adjusted (WLSMV) χ2 test of model fit in Mplus 7. The first EFA used the original 21 motivator items of the MB-HSBI Youth, and the second EFA used the original 19 barrier items of the MB-HSBI Youth. The EFA using the motivator scale items yielded 2 factors/subscales with eigenvalues over Kaiser’s criterion of 1. Items were retained in each factor/subscale only if that item produced a correlation of above .40 or more with that factor only. The following 2 motivator items did not yield a correlation that met this correlation criterion and thus were dropped from the list of motivator items: “I have the discipline to eat healthy” and “Healthy foods keep my body in shape.”
Employing Kaiser’s criterion for the barrier scale items yielded 3 factors/subscales with eigenvalues above 1. Items were retained in each factor only if that item produced a correlation of above .40 or more with a single factor. 21 The following items did not meet this criterion correlation and thus were dropped: “Healthy foods and snacks cost more than unhealthy foods and snacks” and “Healthy foods are not easy to find at restaurants.”
Two ensuing EFAs were conducted without the dropped items. One of these EFAs was conducted on the motivators scale items, and the other was conducted on the barriers scale items. The EFA using the barrier scale items resulted in one barrier scale item, “I like to eat unhealthy foods when I feel stressed,” having multiple loadings of above .40. Thus, this EFA was repeated without the specified multiple loading item.
Final results of the 2 EFAs with items appropriately dropped are presented in Tables 1 and 2. The 2 factors/subscales in the motivators scale for the adolescent participants were “Knowledge and Commitment” and “Routine.” Knowledge and Commitment (M = 3.19, SD = 0.55) was the most strongly endorsed motivator subscale. Of the items composing the Knowledge and Commitment subscale, the most strongly endorsed item was “I understand why healthy foods are good for my body”(M = 3.5, SD = 0.7), and the least strongly endorsed item was “There are healthy options at most restaurants I go to” (M = 2.87, SD = 0.91). The motivators subscale Routine (M = 2.74, SD = 0.73) was endorsed with less strength than Knowledge and Commitment. Of the items composing the motivator subscale Routine, the most strongly endorsed item was “I am used to eating healthy foods and snacks every day” (M = 2.84, SD = 0.98), and the least strongly endorsed item was “Eating healthy is a habit for me” (M = 2.60, SD = 0.95).
Factor Loadings for the Subscales of the Motivator Scale a .
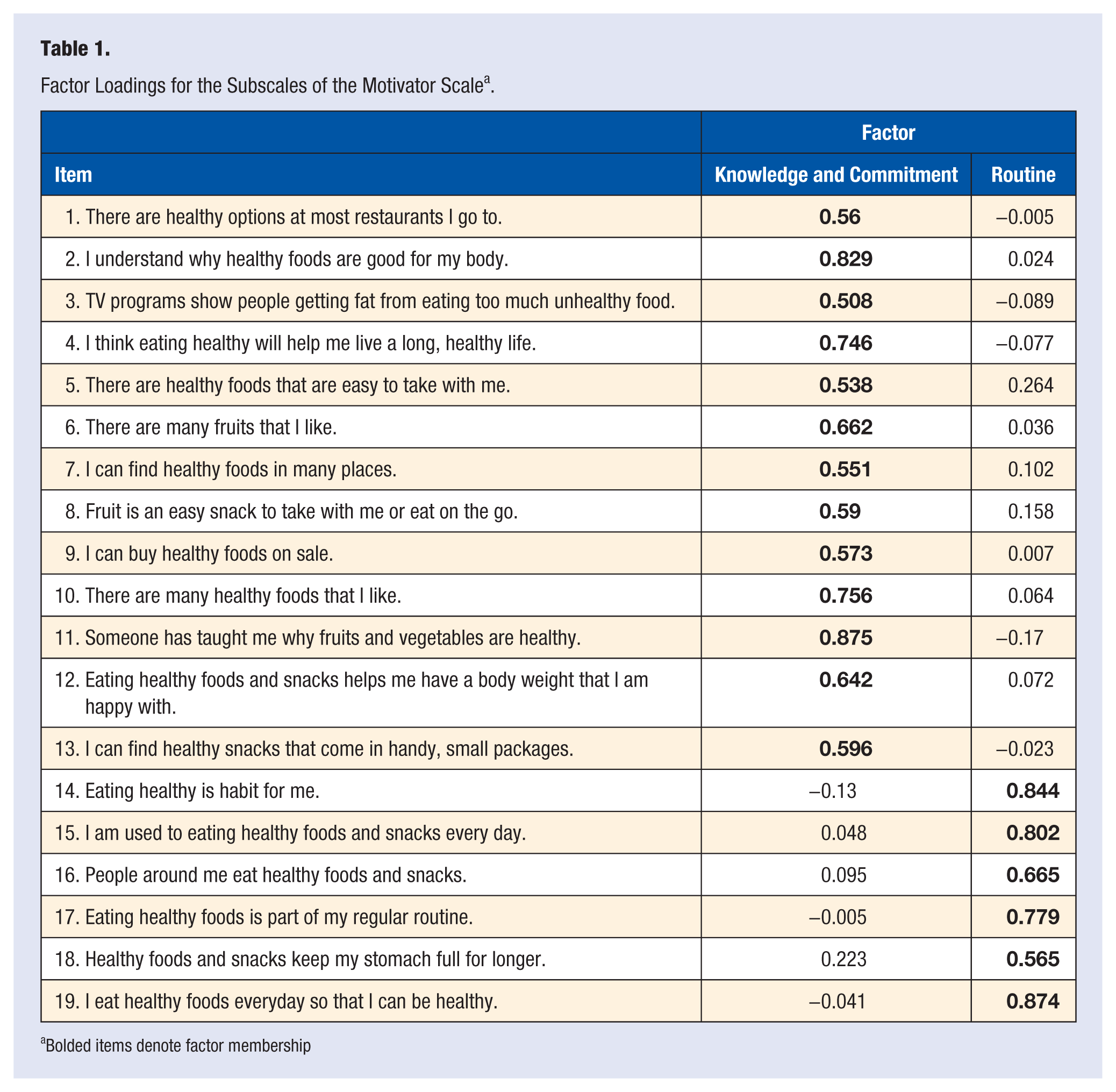
Bolded items denote factor membership
Factor Loadings for the Subscales of the Barrier Scale a .
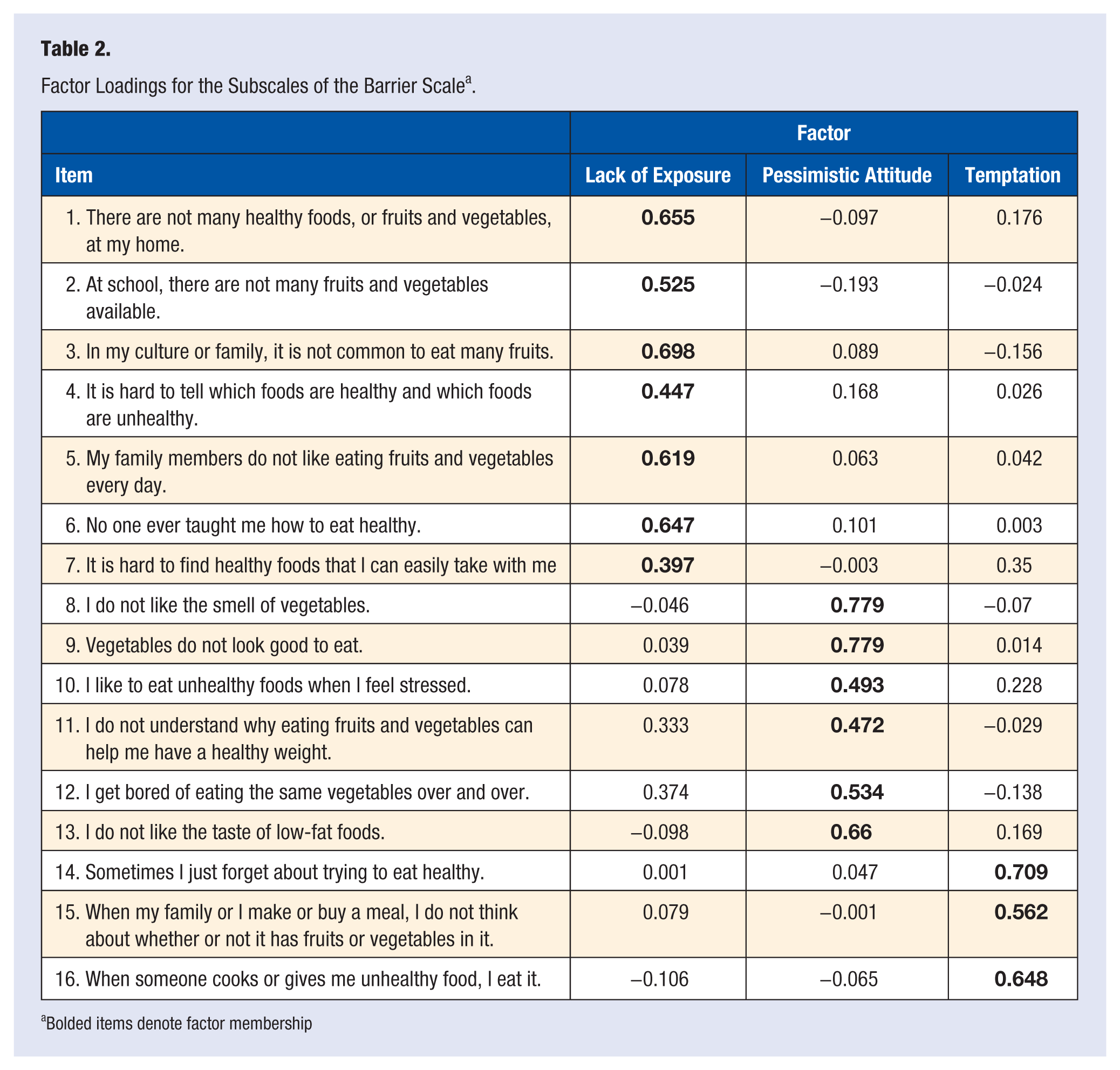
Bolded items denote factor membership
The 3 factors/subscales in the barriers scale were Lack of Exposure, Pessimistic Attitude, and Temptation. Temptation(M = 2.66, SD = 0.76) was the most strongly endorsed barrier subscale. Of the items composing this subscale, the most strongly endorsed item was “When my family or I make or buy a meal, I do not think about whether or not it has fruits or vegetables in it” (M = 2.76, SD = 1.03), and the least strongly endorsed item was “When someone cooks or gives me unhealthy food, I eat it” (M = 2.51, SD = 1.04). The most strongly endorsed item in the Lack of Exposure (M = 2.07, SD = 0.67) barrier subscale was “At school, there are not many fruits and vegetables available” (M = 2.32,SD = 1.09), and the least strongly endorsed item was “No one has ever taught me how to eat healthy” (M = 1.64, SD = 0.92). The most strongly endorsed item in the barrier subscale Pessimistic Attitude (M = 1.87, SD = 0.61) was “I do not like the taste of low-fat foods” (M = 2.22, SD = 1.05), and the least strongly endorsed item was “I do not understand why eating fruits and vegetables can help me have a healthy weight” (M = 1.83, SD = 0.94).
Cronbach’s α was calculated for each new adolescent subscale. The Knowledge and Commitment (α = .86) and the Routine (α = .87) subscales within the motivator scale yielded good measures of internal consistency. The Lack of Exposure (α = .72), Pessimistic Attitude (α = .80), and Temptation (α = .59) subscales within the barrier scale yielded adequate measures of internal consistency.
Multivariate Analyses of Variance
To address the second research question (Are there significant differences in the strengths of the found adolescent motivators of and barriers to eating healthy foods and snacks in association with race, gender, and age?), 2 multivariate analyses of variance (MANOVAs) were used given the conceptual inverse associations of motivator scales and barrier scales and of the subscales within each scale. Prior to conducting these MANOVAs, age was dichotomized to reflect the ages of adolescents in middle school (ie, ages 11-14) and the ages of adolescents in high school (ie, ages 15-17). Additionally, assumptions necessitated by a MANOVA were examined. This examination revealed outliers (greater than 3 standard deviations above the mean) in the Knowledge and Commitment and Pessimistic Attitude subscales. These outliers were trimmed. No transformations were necessary.
One MANOVA was conducted to examine race, gender, and age differences in scores on the 2 found subscales of the motivator scale of the eating healthy foods and snacks domain. These subscales were Knowledge and Commitment and Routine. The multivariate tests indicated a statistically nonsignificant difference for race, Pillai’s Trace = .041, F(8, 284) = .746, P = .651, for sex, Pillai’s Trace = .015, F(2, 141) = 1.060, P = .349, and for age, Pillai’s Trace = .036, F(2, 141) = 2.622, P = .076. The second MANOVA was conducted to examine race, gender, and age differences in scores on the 3 found subscales of the barrier scale of the eating healthy foods and snacks domain. These subscales were Pessimistic Attitude, Lack of Exposure, and Temptation. The multivariate tests indicated a statistically nonsignificant difference for race, Pillai’s Trace = .087, F(12, 417) = 1.039, P = .412, for sex, Pillai’s Trace = .015, F(3, 137) = .677, P = .568, and for age, Pillai’s Trace = .028, F(3, 137) = 1.317, P = .271. Thus, no follow-up univariate analyses were conducted to address the second research question.
Discussion
The MB-HSBI-Youth was developed to measure the motivators and barriers associated with engaging in health promoting behaviors among culturally diverse youth (children and adolescents combined), including youth who are racial/ethnic minorities and/or have a low household income. The purposes of the present study were (a) to identify the motivators scale and its associated subscales and the barriers scale and associated subscales of the Healthy Foods and Snacks domain of the MB-HSBI-Youth for adolescent participants in the national study used to develop this inventory and (b) to determine if scores on the identified subscales differ in association with race/ethnicity, gender, or age. To identify these scales and subscales EFAs were used.
The number of motivator subscales/factors and barrier subscales/factors and the names of each subscale/factor were consistent with the results for the youth (children and adolescents combined) in the national study used to develop the MB-HSBI-Youth. The 2 motivators subscales were (a) Knowledge and Commitment and (b) Routine. The 3 barrier subscales were (a) Lack of Exposure, (b) Pessimistic Attitude, and (c) Temptation.
It is noteworthy, however, that 4 items in the subscales that emerged from the EFAs applied to the youth (children and adolescents combined) motivator and barrier item scores in the study to develop the MB-HSBI-Youth were dropped from the subscales that emerged from the EFAs applied to the adolescent only motivator and barrier item scores used in the present study. The dropped items may be items that are uniquely associated with children versus adolescents.
One of the dropped items was dropped from the Routine motivator subscale that emerged from the EFA applied to the adolescent only data used in the present study. Specifically, this item is “I have the discipline to eat healthy.” This item may have been dropped because the adolescents whose data were used in the present study do not view discipline as a key motivator to engage in healthy eating given that as adolescents they have more control over their eating than when they were children. Therefore, this may suggest that having discipline may be less relevant in light of the increased freedom that comes with their movement from childhood to adolescence.
The second dropped item was dropped from the Knowledge and Commitment subscale of the motivators scale. Specifically, this dropped item was “Healthy foods keep my body in shape.” One possible explanation for this item being dropped is that adolescents may perceive exercise rather than healthy foods as necessary for body shaping. This explanation is informed by the fact that intentional exercising to shape one’s body tends to occur more in adolescence. 22
It is also the case that one item was dropped from the Pessimistic Attitude barriers subscale. This dropped item was “Healthy foods and snacks cost more than unhealthy foods and snacks.” This item may have been dropped because adolescents (compared with children) experience peer pressure to eat unhealthy foods and snacks and thus the relative cost of healthy versus unhealthy food and snacks may be irrelevant for adolescents. 10 By contrast, children may not experience such peer pressure, and thus knowing that healthy foods and snacks cost more than unhealthy foods and snacks may in fact be a barrier to them eating healthy foods and snacks.
The finding that the item “Healthy foods are not easy to find at restaurants” was dropped from the Lack of Exposure barrier subscale that emerged in the present study may have to do with the fact that adolescents very often eat at fast food restaurants where the few available healthy foods are easily typically known (eg, salads). 23 Because of their higher education level, adolescents may have the knowledge necessary to find healthy foods in any restaurants.
It is also noteworthy that the item “I do not understand why eating fruits and vegetables can help me have a healthy weight,” which was in the Lack of Exposure barrier subscale in the study using youth (children and adolescents combined) to develop the MB-HSBI-Youth, switched to the Pessimistic Attitude barrier subscale in the present study involving the adolescent data only. This switch suggests that adolescents may no longer view lack of exposure to fruits and vegetables as a significant concern given their age; instead, they may simply have a distaste for fruits and vegetables (ie, a negative attitude toward them), which is a typical reaction during the adolescent stage of development. 24 Adolescents are more likely to enjoy eating fast foods with their friends rather than eating cooked vegetables at home given the influence of peer socialization needs.
Knowledge and Commitment was the most strongly endorsed motivator subscale. Of the items composing the Knowledge and Commitment subscale, the most strongly endorsed item was “I understand why healthy foods are good for my body.” The motivators subscale Routine was endorsed with less strength than Knowledge and Commitment. Of the items composing the motivator subscale Routine, the most strongly endorsed item was “I am used to eating healthy foods and snacks every day.”
The most strongly endorsed items in each motivator subscale mentioned above suggests that adolescents may be confident in their abilities to understand the importance of eating healthy foods and snacks and to follow through with that understanding if eating healthy foods and snacks is part of their daily routine. Additionally, these most strongly endorsed items suggest that interventions to foster eating healthy foods and snacks among adolescents should include an emphasis on promoting an understanding of the nutritional importance of eating healthy and on creating an eating routine that includes eating healthy foods.
Temptation was the most strongly endorsed barrier subscale. Of the items composing this subscale, the most strongly endorsed item was “When my family or I make or buy a meal, I do not think about whether or not it has fruits or vegetables in it.” The most strongly endorsed item in the Lack of Exposure barrier subscale was “At school, there are not many fruits and vegetables available.” The most strongly endorsed item in the barrier subscale Pessimistic Attitude was “I do not like the taste of low-fat foods.”
The most strongly endorsed barrier subscale items suggest that adolescents tend to not place much emphasis on the presence of fruits and vegetables in their meals, which may be a product of their distaste for low-fat foods. 24 These ratings may suggest that adolescents regard their school cafeteria, a main source of weekly meals, as lacking in fruits and vegetables. If such healthy food options are indeed lacking at the school cafeteria of the adolescents whose data were used in the present study, these adolescents may have few opportunities to become accustomed to the taste of diverse fruits and vegetables.
The least strongly endorsed item in the Temptation barrier subscale was “When someone cooks or gives me unhealthy food, I eat it.” The least strongly endorsed item in Lack of Exposure barrier subscale was “No one has ever taught me how to eat healthy,” and the least strongly endorsed item in the Pessimistic Attitude barrier subscale was “I do not understand why eating fruits and vegetables can help me have a healthy weight.”
Two of the 3 least strongly endorsed barrier subscale items focus on lack of knowledge of healthy foods (ie, “No one has ever taught me how to eat healthy” and “I do not understand why eating fruits and vegetables can help me have a healthy weight”). The comparative lower endorsement of these items as barriers to eating healthy foods and snacks suggest that some adolescents may be comfortable with their capabilities of identifying healthy foods and snacks and have learned at least to some degree why eating healthy foods and snacks is important.
The MANOVAs applied to determine if scores on the identified subscales in the present study differed in association with race/ethnicity, gender, or age revealed nonsignificant differences among these demographic variables. This finding was surprising given that previous studies by other researchers have found that girls’ eating habits were better than boys, 25 that being an adolescent male was positively associated with high fat and sugar intake pattern, 26 and that fruit and salad intake was negatively associated with age. 26 The differences in results between this study and other studies may be attributed to the fact that the adolescents whose data were used in the present study included large percentages of African Americans (36.6%) and Hispanics/Latinos (20.9%). Additionally, this study intentionally targeted areas/organizations with high percentages of low-income adolescents, which is not the case in most of the studies that have reported age and gender differences in eating behaviors.
One limitation of the present study is that although the investigators of the study went to great lengths in order to collect an ethnically/racially diverse sample that would accurately represent the youth of the United States, a large proportion of study participants came from the Southern United States. This geographic imbalance limits the generalizability of the findings in present study.
The size of the adolescent sample used in the present study poses certain limitations with regard to the analytic tools employed in this study. Ideally, an exploratory factor analysis would be performed on a larger number of participants than those available in the present study. However, there were a large enough number of cases to have a variable ratio of 4:1 to 5:1, which is deemed satisfactory. 27 Additionally, the sample size is just below the 200 participants characterized as a large sample. 28
Given the limitations of the present study, future studies that seek to replicate and validate the findings from this study may benefit from having a larger and randomly selected sample of adolescents. Such a sample may result in the exclusion and inclusion of different motivators and barriers subscale items for the eating healthy foods and snacks domain of the MB-HSBI-Youth and different strengths of ratings of these items and of their overall subscales. Additionally, a larger number of adolescent participants would enable use of a confirmatory factor analysis.
Future studies may seek to identify adolescent specific scales and subscales for all domains of the MB-HSBI-Youth (ie, Healthy Breakfast, Healthy Drinks, and Physical Activity). Such studies may lead to an adolescent-specific version of this inventory. The future development of an adolescent-specific version of this inventory may be instrumental in identifying population-specific motivators and barriers. Such an inventory may inform the development of culturally specific health promotion programs that target adolescents and help teach them, especially adolescent females, the difference between maintaining a healthy lifestyle versus disordered eating (eg, dieting, calorie counting, and extreme exercising).
The present study has important implications for psychologists, particularly those interested in counseling and health psychology. Given the training of the psychologists in multicultural counseling and research as well as in mental and physical health promotion to prevent disease, these professionals are perfectly suited to conduct culturally sensitive health promotion assessment research similar to the present study. Psychologists are also trained to use a developmental approach to understanding human behavior—an approach that appears needed in the present study given the finding in this study that some of the motivators of and barriers to eating healthy foods and snacks might be different for adolescents compared to children. Additionally, psychologists are well trained in culturally sensitive inventory development. Thus, these professionals can assume leadership in conducing the next step in research needed to develop an adolescent-specific version of the MB-HSBI-Youth that can be used with multicultural adolescent populations.
Footnotes
Acknowledgements
Thank you to PepsiCo for providing the grant funding to support the research reported in this article. The research funder had no involvement in the study design; in the collection, analysis, and interpretation of data; or in the writing of the article.