
Abstract
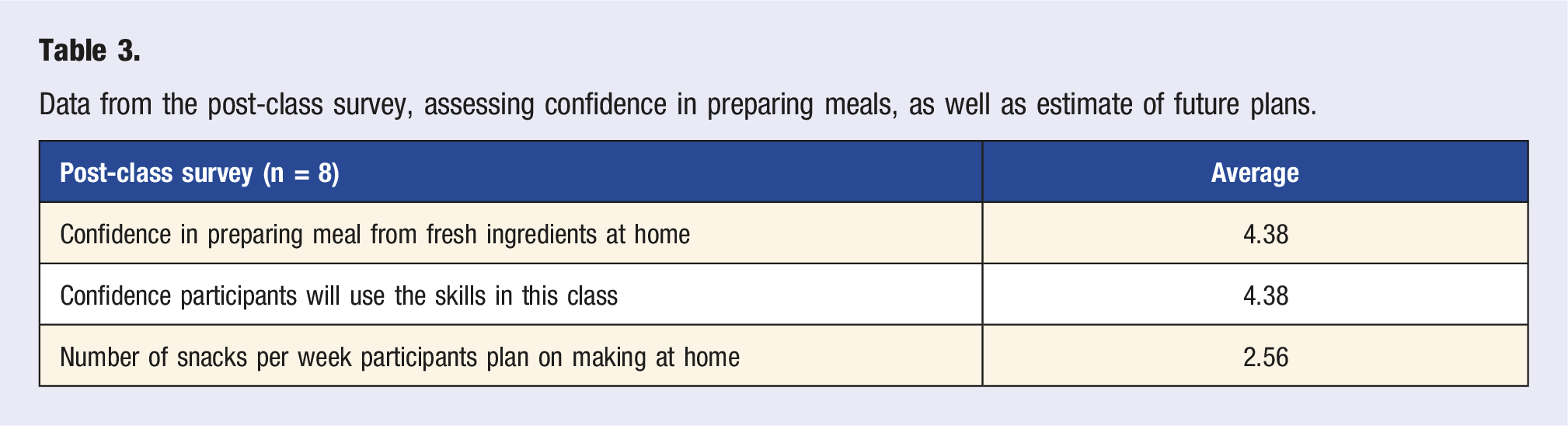
Cooking meals at home is associated with more healthful eating and even other healthy behaviors, such as increased physical activity, but for many there are numerous barriers to making this a reality. Healthy teaching kitchen interventions aim to help patients overcome these barriers. Our pilot program worked to address this issue by demonstrating the feasibility and acceptability of a virtual culinary medicine session designed for outpatient clinic patients. Participants were recruited from a single community primary care clinic for a virtual culinary medicine session. Of the 29 subjects who attended the class, 13 (45%) filled out the pre-course survey, and 8 (26%) filled out the post-course survey. Average participant confidence in preparing snacks at home from fresh ingredients increased from 3.62 to 4.38 out of 5 after attending this session, though the results were not statistically (OR .47; P = .172; 95% CI .16 to 1.3). Post-participation comments were overwhelmingly positive. This study showed that a virtual cooking class is feasible in a community clinic setting and is positively received. In addition, a culinary class teaching healthy cooking techniques paired with nutrition training may improve patient’s confidence in the kitchen.
Keywords
“This intervention demonstrates the feasibility of a virtual culinary instruction intervention to teach home-based snack preparation.”
Background
Cooking meals at home is associated with more healthful eating and even other healthy behaviors, such as increased physical activity. 1 Meals prepared at home are generally healthier than meals purchased outside the home for various reasons. Many purchased foods, especially snacks, are convenience foods, designed to be shelf stable, portable, and hyper-palatable, which often requires additional processing and additives such as salt, sugar, fat, and artificial preservatives.2,3,4 Conversely, with full control of ingredients and cooking methods at home, individuals may make more intentional choices about ingredients and include more whole foods. Yet, for many Americans, there are numerous barriers to preparing meals at home including inadequate time, limited access to fresh ingredients, financial constraints, and lack of culinary training.5,6
It is not trivial that cooking foods at home requires prerequisites to be successful. One must first have the money and a convenient place to purchase fresh ingredients. This is a prevalent barrier, with more than 53.6 million Americans having poor access to healthful food.7,8,9 Second, the individual must have a place and the necessary tools to prepare food, as well as possess basic food preparation skills. It has been demonstrated that culinary skills can be improved through technical instruction, increasing the likelihood of cooking meals at home and enhancing the health of individuals, families, and communities. 1 Culinary skills instruction can be performed virtually through online courses, producing similar success and outcomes as in-person teaching. 10
Culinary Medicine, an emerging field in healthcare, attempts to address these barriers. It is characterized by training medical professionals to blend the art and science of food preparation and medicine. Health professionals trained in culinary medicine coach patients to help them prepare and eat enjoyable foods which will prevent and even treat their medical conditions. 11 Data is emerging regarding the role of healthy teaching kitchens in combatting chronic illness globally. In a systematic review of the impact on food preparation interventions, Reicks, et al. found that often these interventions were associated with increased intake of fruits, vegetables, and plant sources of protein. 1 Some studies showed reduction in Body Mass Index (BMI) at 3 months. However, nearly half of the studies reviewed lacked a control group, and many studies were small. 12
Another small, uncontrolled study showed that patients involved in healthy teaching kitchen visits improved their A1c and blood pressure—the more participation, the greater the improvement. 13 Another larger, randomized controlled trial showed improvements in healthful eating and significant cost savings. 14 And 1 RCT, done at a medical school-based teaching kitchen, showed significant improvements in glycosylated hemoglobin, or A1c, which is a measure of average blood sugar, and blood pressure (BP) after cooking interventions compared to controls. 15 In addition, a few studies have demonstrated feasibility of a cooking classes in a clinical setting.16-19 Most recently, in 2021, their group completed an RCT with overweight patients and found similar positive experiences with the session in addition to observing weight loss in both the culinary intervention group and control group—which only received online nutrition resources. 20
Virtual platforms may expand the reach of culinary training to populations who may not otherwise have access to this resource. In our pilot program, we demonstrate how a virtual culinary medicine group can be integrated to a community clinic. Data regarding virtual cooking classes are emerging. Chef Rani Polak and his team have published the most on culinary medicine in the virtual space, outlining an 8–12 week curriculum of once-weekly, combined didactic and practicum sessions targeted at either healthcare professionals, health coaches, or patients. Their survey data were mostly positive, with participants finding the sessions educational and rating their confidence level with cooking at home increased after the virtual sessions.21-23
Since the target audience was those who working at our clinical sites, we decided to focus our virtual culinary instruction on preparing fresh and healthful snacks which one could bring to work and eat in place of the readily available and often highly processed vending machine and convenience store snacks.
Methods
Protocols for this study were approved by the University of Utah Institutional Review Board. The purpose of this study was to pilot the feasibility of hosting a virtual culinary medicine group visit with a cooking demonstration at a community medical clinic. The course was designed to be interactive, teaching basic nutrition knowledge and food preparation skills through simple recipes using common ingredients.
Participants were recruited from multiple clinics within the University of Utah Health System—primarily from the main place of work as the principal investigators—via email, flyers, and direct invitations by clinic staff and clinicians. Participants were included if they were over the age of 18 years, spoke English, and had access to an electronic device with videoconferencing capability. Other than meeting the inclusion criteria, there were no specific exclusion criteria. Participants were emailed a link to the class and completed an informed consent document to collect and analyze clinical data. Before the first class, participants were asked to fill out a survey containing questions about daily fruit and vegetable intake, and confidence preparing meals from fresh ingredients (See supplementary material).
We invited participants to attend a single session virtual culinary medicine class. We ran this same class 3 times from November 2020 to April 2021. A total of 29 participants attended. Each participant attended only once. The authors, trained in culinary medicine and dietetics, led the opening discussion about the health benefits of fiber, high quality protein, and flavoring foods with herbs and spices while minimizing the use of salt (i.e., flavor building). Two registered dieticians then performed a thirty-minute cooking demonstration showing how to quickly prepare healthful snacks—veggies and hummus, air popped popcorn flavored with herbs and spices, and a fruit and granola yogurt parfait—which can be taken to work and eaten in place of convenience foods. In the first cohort, participants were invited to follow along in their own kitchens, but few attempted and the interaction with our hardware was somewhat difficult, so in the second and third cohorts we focused on having a robust discussion and highlighting key components of the cooking demonstration from the dietitians. Throughout the class, participants were encouraged to ask questions, via the chat or audibly, which were addressed throughout the session. We had a final question and answer session during the last few minutes of the session. After the class, participants were emailed a post-class survey asking again about their confidence preparing meals from fresh ingredients and eliciting feedback about the course, a handout about flavor building, and recipes for the foods made in the class. (See supplementary material).
Surveys were adapted from previously administered internally developed surveys for the Culinary Medicine Student Course taught by faculty, including one of the authors (R. Doxey), at the University of Utah. These surveys assess health behaviors and confidence with culinary skills. These have not been externally validated.
Statistical Analysis was performed on the survey data comparing pre- and post-survey question: “How confident do you feel preparing snacks from fresh ingredients at home?” Participants rated their confidence on a Likert scale from 1 to 5, and a linear regression analysis used to determine a statistically significant change.
Results
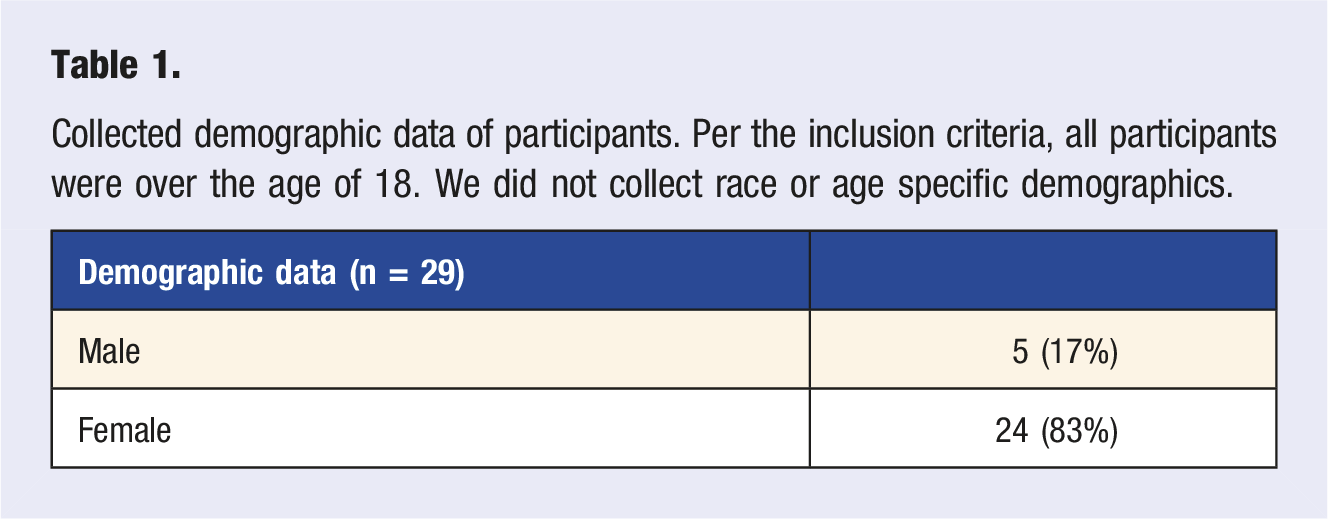
Collected demographic data of participants. Per the inclusion criteria, all participants were over the age of 18. We did not collect race or age specific demographics.
Pre-Class Survey
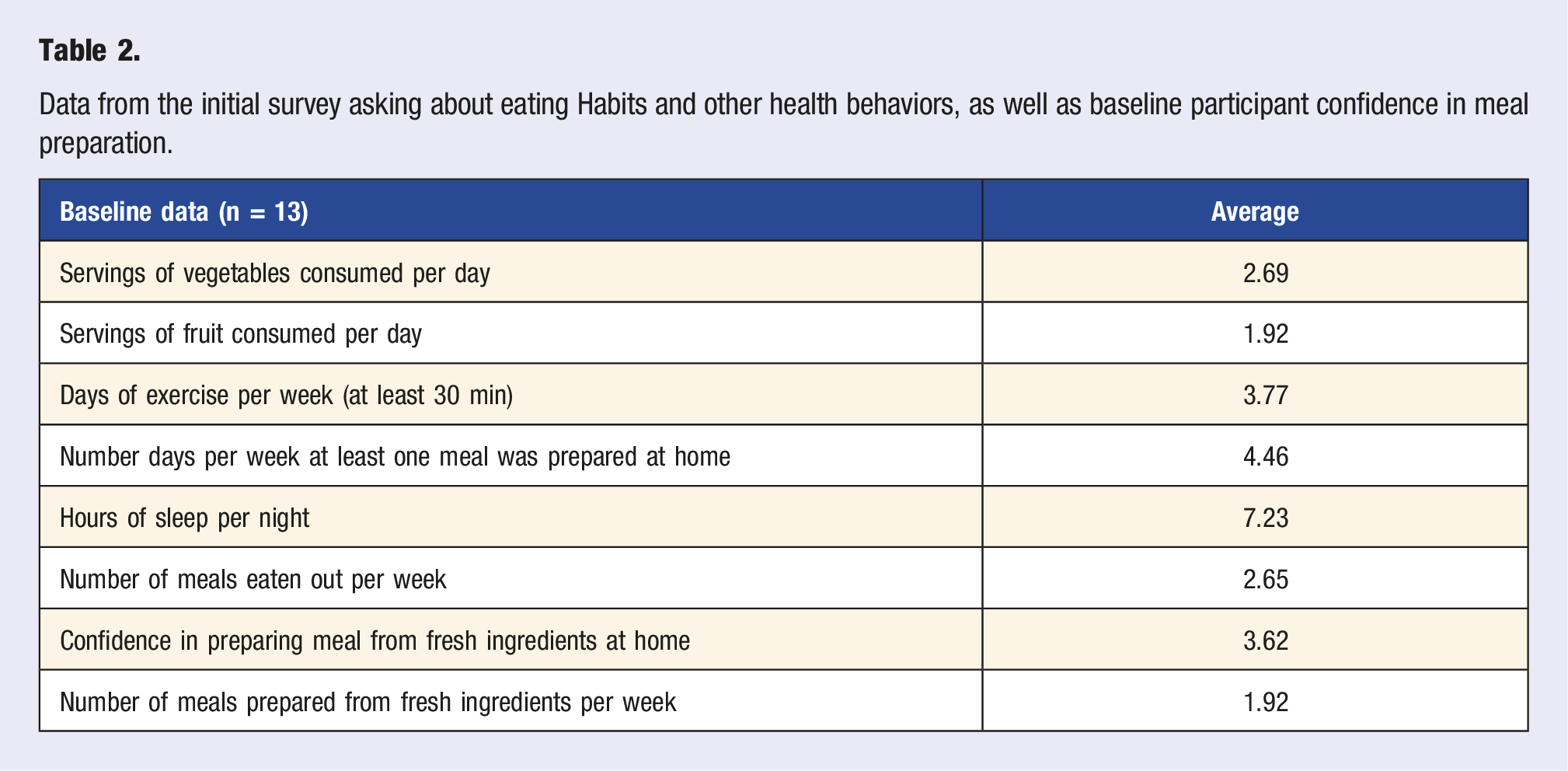
The pre-class survey results demonstrated that participants ate an average of 1.9 and 2.7 servings of fruits and vegetables per day, respectively. This is higher than averages reported in the US population of 1.0 serving of fruits and 2.3 servings of vegetables daily.24,25 Eleven of the thirteen participants (85%) filling out the pre-class survey reported eating at least 1 serving of fruits and 1 serving of vegetables daily.
Survey results showed that the participants ate at least 1 meal at home on average 4.4 days per week, but only an average of 1.9 meals per week were from fresh ingredients prepared at home. An average of 2.6 meals per week were from restaurants. Responses on cooking confidence in the pre-class survey ranged from 1 to 5 with an average of 3.6 on a 5-point Likert scale. The participants, on average, exercised for at least 30 min 3.76 days per week.
Post-Class Survey
Data from the initial survey asking about eating Habits and other health behaviors, as well as baseline participant confidence in meal preparation.
Confidence
Data from the post-class survey, assessing confidence in preparing meals, as well as estimate of future plans.
Barriers
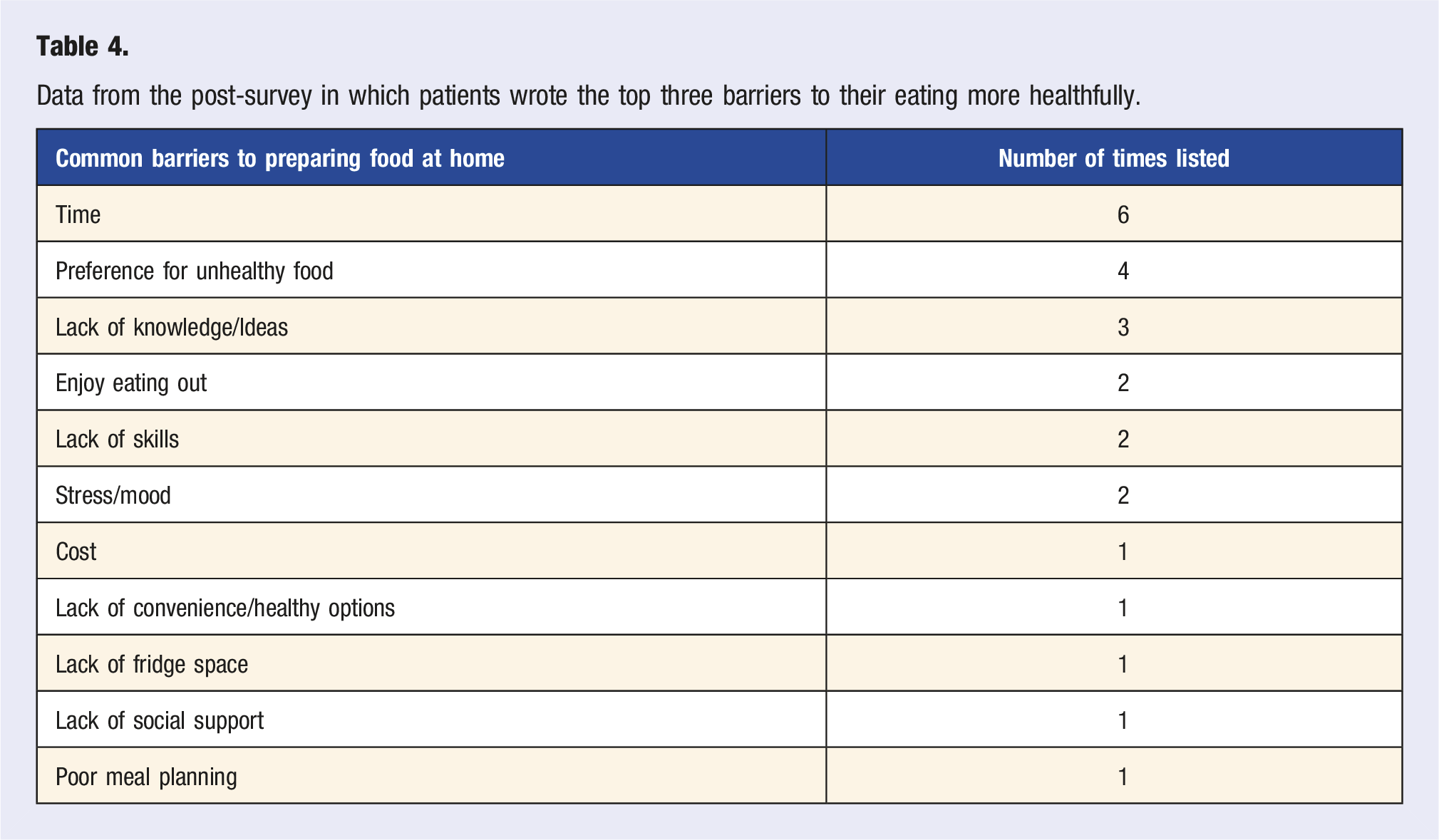
Data from the post-survey in which patients wrote the top three barriers to their eating more healthfully.
Cost
The recipes, all three snacks prepared, cost approximately $3.00 per serving.
Feedback
We also asked participants for narrative feedback regarding the class, which was very positive. Here are a few examples: “Concise info, easy recipes to follow what was going on, and good info for the everyday person.” “A mix of healthy and cooking. The science behind the food. It was well organized!” “I like the… education combined with tasty!” And, “the question and answer session was the most interesting.” Suggestions for improvement included recommendations on improving camera angles, microphone volume, and other technical aspects of the session. One participant also wanted to have an in-person class.
Discussion
Diet plays a major role in the development of chronic illness. Foods prepared at home are more likely to contain whole foods, less preservatives, and less refined sugars, making them an important treatment for people with chronic metabolic conditions and those at risk of developing metabolic disease.28-30 Individuals are more likely to prepare healthful foods at home, as confidence in their cooking abilities increases.31-33 However, lack of time, knowledge, and skill prevent many individuals from preparing meals at home. Through our healthy snacking virtual cooking class, we showed that simple culinary instruction via a videoconference platform trended toward increased confidence in participants’ culinary skills, and many felt confident that they would prepare healthful snacks and meals in the future.
In this feasibility study, the pre-class survey revealed a wide range of confidence in culinary skills, suggesting that some were attending the class to improve their culinary skills, while others felt confident, but still wanted to learn more. While the increase in confidence in ability to cook at home was not statistically significant, the small sample size and pre-class distribution of cooking confidence greatly impacted the ability to achieve statistical significance. Despite this, the overall response from participants was very positive, as we saw from the narrative comments above.
This intervention demonstrates the feasibility of a virtual culinary instruction intervention to teach home-based snack preparation. Unlike traditional cooking classes that require special facilities, the virtual model requires less cooking equipment, using one portable demonstration cooking station vs several cooking stations, with participants using their own kitchen equipment. This also allows for a “practice like you play” model where participants are learning in their own cooking environment, relying on the kitchen tools and appliances they will have access to everyday. Participants are also required to shop for their own ingredients which could be a potential barrier to participation, though we kept the cost low, with all recipes combined costing around $3.00 per one serving of each. On the positive side, this allowed the participants the flexibility to make ingredient substitutions based on cost and preferences.
Limitations
There are several limitations to this study. The small sample size made it difficult to detect a statistically significant difference in confidence before and after the session, and as this was a pilot feasibility study, there was only one class session. Likely greater benefit would be derived from a series of classes and longitudinal follow-up. The measure of confidence was patient-reported with no objective measures used in the evaluation. In addition, despite the robust dialogue, few participants prepared food alongside the instructors, which contrasts with the high participation we typically see with in-person instruction. Lastly, this was a single-center trial, with trained and dedicated clinicians, and this may not be generalizable, especially in clinics with limited resources or fewer trained personnel. Confidience in culinary skils before and after the virtual cooking class.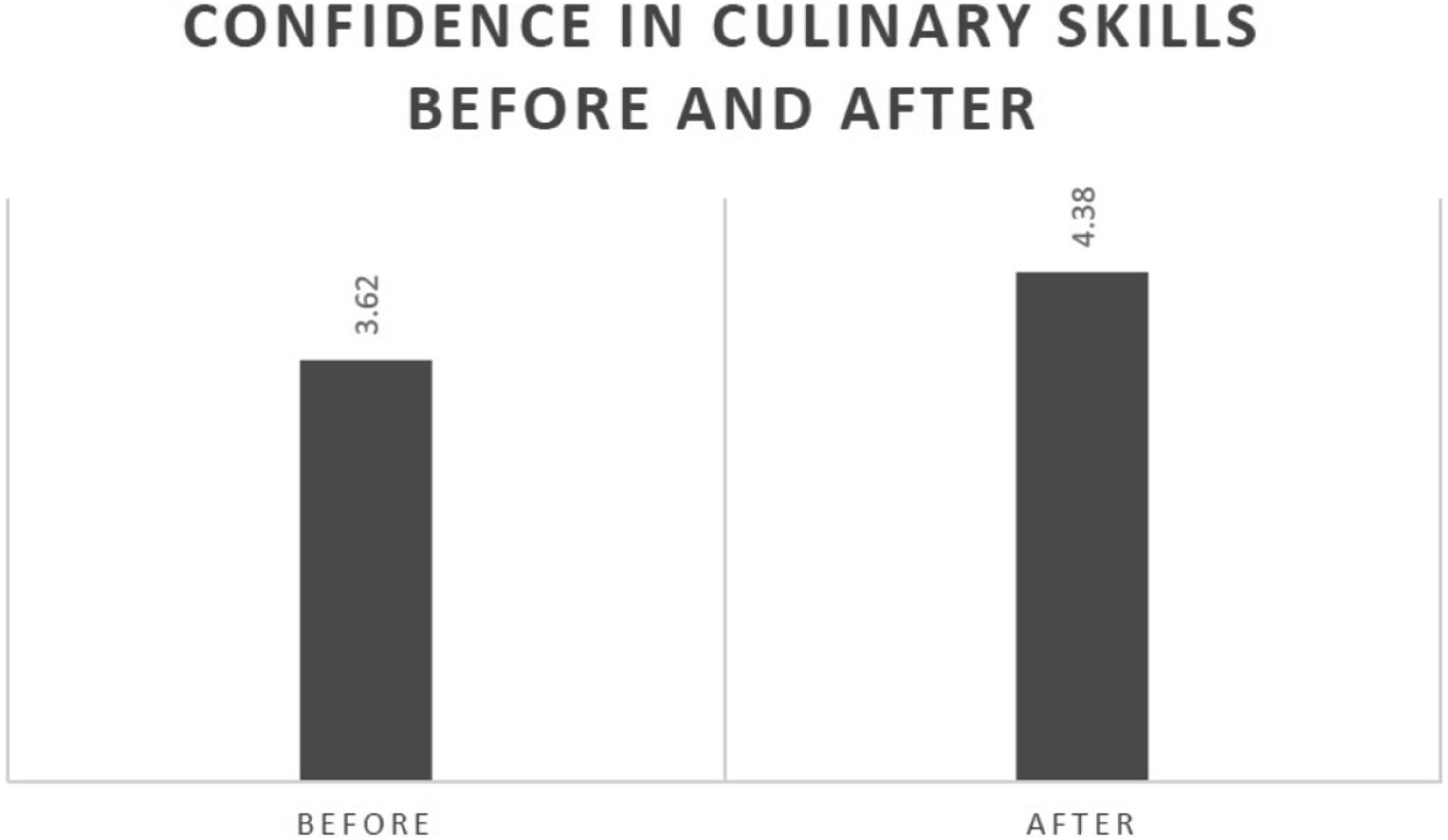
Conclusion
A single session, virtual culinary medicine class, focused on preparing healthy snacks is feasible in a community clinic setting, is well received by participants and may improve confidence in culinary skills in the home.
Richmond S. Doxey, Richard H. Wolferz, Kelly L. Stewart, Rachel Goossen, and Lindsey Imber
Supplemental Material
Supplemental Material - Building Flavor and Confidence in the Kitchen: A Pilot Virtual Cooking Class on Healthy Snacking
Supplemental Material for Building Flavor and Confidence in the Kitchen: A Pilot Virtual Cooking Class on Healthy Snacking by Richmond S. Doxey, Richard H. Wolferz, Kelly L. Stewart, Rachel Goossen, and Lindsey Imber in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Building Flavor and Confidence in the Kitchen: A Pilot Virtual Cooking Class on Healthy Snacking
Supplemental Material for Building Flavor and Confidence in the Kitchen: A Pilot Virtual Cooking Class on Healthy Snacking by Richmond S. Doxey, Richard H. Wolferz, Kelly L. Stewart, Rachel Goossen, and Lindsey Imber in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Building Flavor and Confidence in the Kitchen: A Pilot Virtual Cooking Class on Healthy Snacking
Supplemental Material for Building Flavor and Confidence in the Kitchen: A Pilot Virtual Cooking Class on Healthy Snacking by Richmond S. Doxey, Richard H. Wolferz, Kelly L. Stewart, Rachel Goossen, and Lindsey Imber in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Building Flavor and Confidence in the Kitchen: A Pilot Virtual Cooking Class on Healthy Snacking
Supplemental Material for Building Flavor and Confidence in the Kitchen: A Pilot Virtual Cooking Class on Healthy Snacking by Richmond S. Doxey, Richard H. Wolferz, Kelly L. Stewart, Rachel Goossen, and Lindsey Imber in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
We would like to acknowledge the support and assistance of Theresa Dvorak, RD and the Department of Nutrition and Integrative Physiology at the University of Utah. Also, we thank the Office of Wellness and Integrative Health at the University of Utah for the wellness seed grant which provided funding for consumables for this research. In addition, we would like to acknowledge the willing study participants who not only participated but gave us valuable feedback on this pilot program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Wellness Seed Grant from the Office of Wellness and Integrative Health at the University of Utah.
Supplemental Material
Supplementary material for this article is available on the online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.