
Abstract
Childhood obesity continues to be a major public health concern in the United States. This work reviews the current understanding of the relationship between sleep duration and obesity among children and adolescents. A systematic search was conducted for papers published between January 2000 and July 2013 using keywords: (sleep) and (overweight or obesity or obese or body mass index or BMI or adiposity or body fat or fat) and (children or child or youth or teen or pediatric or adolescent or paediatric or childhood or adolescence or boy or girl). Reference lists of relevant articles and reviews or meta-analysis articles were checked to identify additional studies. Only empirical work and longitudinal studies that focused on children and adolescents were included in this review. The search identified 22 longitudinal studies. The majority of the reviewed studies support the presence of an inverse relationship between sleep duration and obesity. However, in some studies the relationship was not significant in adjusted analyses. Differences as a function of age and gender were also noted. Despite more than a decade of research, the debate on the association between sleep duration and obesity continues. Further research with repeated assessments, valid objective measures, and better control of potential confounding variables is warranted.
‘Studies conducted in the past decade have indicated the association of sleep deprivation and obesity.’
The rates of obesity among adolescents have tripled in the past 3 decades; currently more than one third of children and adolescents in the United States are overweight or obese. 1 Children and adolescents with a high body mass index (BMI) are more likely to become obese as adults2,3 and are at risk for many chronic conditions such as high cholesterol, hypertension, 4 diabetes,5,6 metabolic syndrome, liver disease, 7 and cancers, including breast and colorectal cancer. 8 Obesity prevention efforts should therefore begin early in life to prevent high-risk conditions later in adulthood.
Several behavioral, environmental, and genetic factors contribute to overweight and obesity. Physical inactivity and unhealthy diet often referred to as the “Big Two,” have been the primary focus of past obesity prevention programs. 9 However, recent studies have recognized other factors as possible causes of obesity.10,11 Some of these potential influences include microorganisms, endocrine disruptors, pharmaceutical iatrogenesis, reduced variability of ambient temperatures, increased maternal age, intrauterine effects, and sleep debt. 11 Among these factors, sleep deprivation has received considerable attention in the recent years.
An estimated 50 to 70 million Americans of all ages suffer from sleep problems. 12 Sleep needs may vary among individuals; however, it is recommended that 10- to 17-year-olds receive an average of 8.5 to 9.25 hours of sleep each night, 5- to 10-year-olds receive 10 to 11 hours of night sleep, and 1- to 3-year-olds receive 12 to 14 hours of sleep.13-15 However, research studies suggest that children and adolescents receive considerably less sleep than the recommended amount. In a national study, about 25% parents of 6- to 11-year-olds reported that their children did not receive adequate amount of sleep for their age. 16 A survey in Rhode Island found that 26% of high school students slept 6.5 hours or less and only 15% reported sleeping 8.5 hours or more on school nights. 17 Data from the 2007 Youth Risk Behavior Survey indicated that about 69% of high school students get less than 8 hours of sleep on school nights. 18 Moreover, the average sleep duration decreases by about 40 to 50 minutes from ages 13 to 19 years. 17 Increased academic demands, television watching, and social and recreational pressures may all contribute to decreased sleep duration during adolescence.17,19
Studies conducted in the past decade have indicated the association of sleep deprivation and obesity. The exact mechanism by which sleep deprivation may lead to obesity is not known; however, researchers have proposed several possible pathways, including the effect of sleep deprivation on hormones, energy expenditure, and health behaviors. Sleep has an effect on the sympathetic nervous system and/or hypothalamic hormones. 20 Sleep deprivation is associated with low levels of leptin and high levels of ghrelin, which influences appetite regulation.20-22 Sleep restriction is also associated with an increase in cortisol levels, which promote increased food intake and the accumulation of visceral fat in humans. 23 The second potential mechanism by which sleep restriction can contribute to obesity is by promoting behavior that causes weight gain. 24 Increased wakefulness may provide more time for eating in an obesogenic environment where food is readily available. 25 Often, lack of sleep is associated with sedentary activities like television watching, which might lead to weight gain due to increased snacking.26,27 Finally, sleep deprivation may lead to reduced energy expenditure. Sleep restriction has been linked with reductions in the thyroid-stimulating hormone (TSH). Since TSH stimulates basal metabolic rate, reductions in TSH can be associated with reduced resting metabolism. 24 Furthermore, people with chronic sleep restriction experience fatigue and daytime sleepiness, 28 which may decrease their motivation to engage in physical activity.25,29 It is also possible that these individuals might consume high-energy drinks and food to overcome fatigue. 24 Though majority of these studies have been conducted with adults, it is possible that similar mechanism influence the relationship between sleep and obesity among children and adolescents.
Several epidemiological studies have examined the association between sleep deprivation and obesity among children and adolescents. Some review articles have also been published on this topic. Magee and colleagues examined seven longitudinal studies conducted with children between 2004 and 2008; all 7 studies reported an association between short sleep duration and increased weight. 30 The most recent review article by Guidolin and Gradisar 31 included only 2 longitudinal studies with adolescents; both studies reported no significant associations. Several new studies have been published since then that examined the relationship between sleep duration and obesity, and some of the recent articles did not find any significant associations. The purpose of this review is to present the current understanding of the relationship between sleep duration and obesity among children and adolescents. Given the nature of cross-sectional studies, it is difficult to interpret whether sleep duration causes weight gain, or whether overweight/obese children have reduced sleep. Therefore, in this review we present only longitudinal studies among children and adolescents.
Methods
A systematic search was conducted using the PubMed, Academic Search Premier, ERIC, Health Source, and CINAHL databases for articles published between January 2000 through July 2013 using keywords: (sleep) and (overweight or obesity or obese or body mass index or BMI or adiposity or body fat or fat) and (children or child or youth or teen or pediatric or adolescent or paediatric or childhood or adolescence or boy or girl). Only empirical work that examined the longitudinal association between sleep duration and obesity among children and adolescents (ie, age of participants at baseline less than 18 years) was included. Articles that included a measure for weight and sleep duration were selected for review. Articles that examined sleep quality but not sleep duration were excluded. Studies on participants with obstructive sleep apnea, sleep disordered breathing, and other medical issues were excluded. Furthermore, articles in a language other than English and duplicate studies were also excluded. Reference list of relevant articles and reviews or meta-analysis articles were also checked.
Results
The search identified 22 longitudinal studies. Ten studies were conducted within the United States and another 12 studies conducted internationally in countries including Australia, Canada, Europe, Korea, and New Zealand (Table 1).
Longitudinal Studies Examining the Association Between Sleep Duration and Overweight/Obesity.
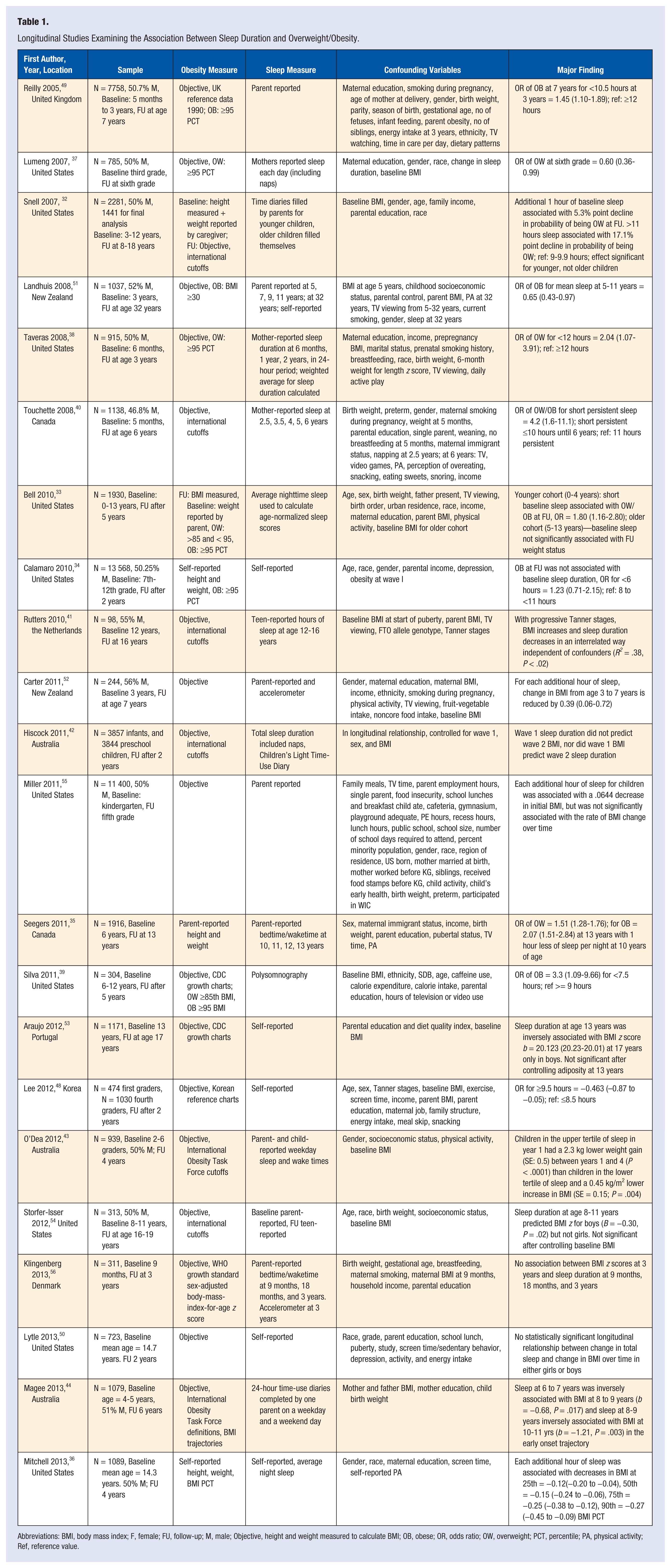
Abbreviations: BMI, body mass index; F, female; FU, follow-up; M, male; Objective, height and weight measured to calculate BMI; OB, obese; OR, odds ratio; OW, overweight; PCT, percentile; PA, physical activity; Ref, reference value.
A number of methodological differences were noted among the reviewed articles. Studies varied in their methods to collect data for BMI calculations. Objectively measured height and weight was used to calculate BMI in most of the studies, but in others height and/or weight information was obtained via self-report.32-36 Studies also differed in the classification used to define overweight/obesity. Studies conducted in the United States used the 2000 Centers for Disease Control and Prevention (CDC) growth charts to calculate the BMI percentiles,33,34,37-39 whereas the majority of studies conducted outside the United States used the international cutoff points.40-44 The CDC growth charts were developed with data from the 5 national health examination surveys in the United States. 45 The international cutoffs were developed using the survey data from 6 countries (Brazil, Great Britain, Hong Kong, the Netherlands, Singapore, and the United States). 46 The use of CDC versus international cutoffs can result in an absolute difference of 0% to 13% in the prevalence of overweight and obesity. 47 Some other studies used their country-specific growth charts. For example, Lee et al 48 used the Korean growth charts and another study used the UK reference charts. 49 Furthermore, the differences in the classification of obesity status and the reference group used in the analyses could affect the relationship between sleep duration and obesity in the reviewed articles. For example, studies by Silva et al 39 and Bell and Zimmerman 33 analyzed the odds of being overweight (ie, BMI >85 kg/m2) and obese (BMI >95 kg/m2) compared with a reference group of normal weight participants (BMI <85 kg/m2), whereas, Calamaro et al 34 analyzed the odds of being obese (BMI >95 kg/m2) compared with a reference group of participants with BMI <95 kg/m2. Including overweight participants in the reference group could affect the relationship between sleep and weight status.
The definition of short sleep duration differed among the reviewed articles, but seemed appropriate for the age-group examined in the studies. For example, Taveras et al 38 used <12 hours as short sleep duration for 6-month-olds, Reilly et al 49 used <10.5 hours for children 5 months to 3 years old, Silva et al 39 used <7.5 hours for 6- to 12-year-olds, and Calamaro et al 34 used <6 hours for 7th to 12th graders. Most of the studies used parental and/or self-reported measure for sleep. Only one study used the polysomnographic assessment for sleep. 39 Two studies included naps in the total sleep time.37,42 However, no specific patterns were observed in the relationship between sleep and obesity based on these different sleep assessment techniques (Table 1). Finally, studies varied in the number and type of covariates controlled in the analyses. Most studies controlled for the demographic factors such as age, gender, and socioeconomic conditions; however, they varied in relation to the health-related behaviors such as dietary intake, sedentary habits, and physical activity. Very few studies controlled for puberty,35,41,48,50 which is an important determinant of obesity among adolescents.
The reviewed studies used baseline sleep duration to predict overweight/obesity at a follow-up and thus can support a causal association between sleep and obesity. Most of these longitudinal studies indicated that short sleep duration is a risk factor for overweight/obesity.* The relationship was significant even after controlling for baseline weight status. Some of the studies have baseline data from the first year of life and follow up data until early childhood.38,40,49 The longest longitudinal study to date was performed in New Zealand, where average sleep duration at 5 to 11 years of age was used to predict obesity in adulthood. 51 The authors found that, with every one-hour increase in the sleep duration in childhood, the risk of obesity was reduced by 35% at 32 years of age. 51
The longitudinal relationship between sleep duration and obesity in the reviewed articles varied as a function of age. In the study by Bell and Zimmerman 33 a significant association between sleep and obesity was seen only for younger children (0-4 years at baseline). Among older children (5-13 years), short sleep duration at baseline was not associated with weight gain at a 5-year follow-up. Similar results were found in the study by Snell et al. 32 Some gender differences were also observed. Two reviewed studies noted the relationship between sleep duration and obesity among boys, but not among girls.53,54
Some recently published studies (n = 7) did not support a longitudinal relationship between sleep duration and obesity.34,42,50,55,56 Using data from the National Longitudinal Study of Adolescent Health, Calamaro et al 34 found that short sleep among 7th to 12th graders was not associated with obesity at a 2-year follow-up. Two studies that examined the sleep duration of infants and obesity 2 to 3 years later did not find any significant association.42,56 Miller et al found a concurrent relationship between sleep duration and obesity among children; however, the longitudinal association was not significant. 55 Similarly, Lytle et al 50 did not find any significant association between change in sleep duration and obesity risk in their longitudinal study of school children. Arauja et al 53 in Portugal and Storfer-Isser et al 54 in the United States found significant associations between baseline sleep duration and follow-up BMI z scores; however, the associations were not significant after controlling for baseline body composition.
Discussion
We conducted a comprehensive review of longitudinal studies examining the relationship between sleep duration and obesity among children and adolescents. This study represents an updated and expanded review from earlier work.30,31 The current review includes more recently published longitudinal studies and those specifically focused on children and adolescents. A total of 22 studies were reviewed. The majority (n = 13) of the reviewed studies support an inverse relationship between sleep duration and obesity. Two studies found a significant association for younger children but not for older children.32,33 However, seven longitudinal studies did not find the relationship between sleep duration and obesity to be significant in the adjusted analyses, especially after controlling for baseline body composition.34,42,50,53-56 This raises the question of publication bias in the earlier years of research in this field. Since we did not include unpublished papers, it is possible that we may have missed studies with nonsignificant findings.
The reviewed articles used different methodological approaches, including informants, collection and measurement of BMI and sleep, and used different covariates, which makes comparison of studies difficult. Comparing studies across the different developmental periods, we observed that findings differed as a function of age and gender. Five studies used baseline data from infants; two of these studies did not find significant relationship.42,56 Three42,54,55 of the 14 studies that reported data on children and six32-34,50,53,54 of the 10 studies that reported data on adolescents did not find significant association between the sleep duration and overweight/ obesity. Two studies noted positive associations among boys but not among girls.53,54 These age and gender differences might be because of the physiological changes during puberty; however, more empirical research is needed to examine these physiological changes, including the effect on the sympathetic nervous system and hypothalamic hormones. Studies are needed that examine developmental variables such as puberty in the association between sleep and obesity. Pubertal development is associated with prominent changes in the body composition with attainment of more body fat in girls and more lean body mass, skeletal mass, and muscle mass in boys. 57 Moreover, these changes in body composition occur several years earlier in girls than in boys. 57 Without controlling for these developmental changes, the association between sleep duration and obesity may be biased. Whether this relationship varies as a function of age and gender or is related to the pubertal growth needs further exploration. Longitudinal studies with repeated assessments from early childhood to late adolescence may help to identify the critical window of development when sleep duration is a risk or protective factor for obesity. It is also possible that factors such as sleep quality, and shift in sleep times (ie, late bed and wake-up times) may play a role along with sleep duration. Furthermore, the role of daytime nap and catch-up sleep over weekends and holidays needs to be explored.
Obesity is caused by a number of complex and interrelated factors. The efficacy of an obesity prevention program targeting a single factor is relatively small. 58 Therefore, interventions that focus only on diet and/or physical activity have shown moderate success.59,60 Under these circumstances, the role of short sleep in the obesity epidemic if supported can have great public health implications. However, it is important to realize that improving sleep alone will not be sufficient to reverse the obesity epidemic. The significance of adequate sleep does not undervalue the role of diet and physical activity. However, promoting adequate sleep along with the dietary and physical activity interventions may improve the efficacy of current programs. The Institute of Medicine has recently recommended the promotion of age-appropriate sleep duration as a measure of childhood obesity prevention. 61 Short sleep duration in children and adolescents is primarily due to modifiable lifestyle factors. Parents, caregivers, and health care providers can help children to maintain good sleeping practices. Assessment of sleep patterns can be incorporated as a routine practice during clinic visits. Educational materials recommending the required amounts of sleep and methods to achieve it can be provided by primary care providers to parents and children. Parental monitoring may improve sleep habits among children and adolescents. Parents can be encouraged to put their younger kids to bed early. Setting rules about television and computer time can facilitate early bedtimes among adolescents.
Despite more than a decade of research, the debate on the causal association between sleep duration and obesity continues. To validate these relationships, longitudinal studies with repeated assessments, long-term exposure, measures of body composition, valid objective measures of sleep duration and sleep quality, and better control of confounders, including pubertal development, are required. 62 Finally, the gold standard, randomized clinical trials, in which obese children and adolescents are encouraged to sleep for adequate hours, may more definitively establish causal pathways.