
Abstract
Nutrition controversies abound, particularly in an age of vast information and technology. Scientific information is often disseminated so quickly, via news outlets or lay bloggers, that the factual details are left out and in-depth analysis is omitted. Our food supply and our environment are intertwined, yet from a public health standpoint there seems to be a disconnection between what our society wants, and what it may need, in terms of nutrition and disease prevention. We want our food supply to be safe, available, affordable, fresh, and tasty. We also want our environment to be minimally affected, animal rights to be upheld, and less waste to occur. We need to provide adequate nutrition that promotes health to a diverse population at a reasonable cost. This article will address some current nutrition controversies surrounding genetically modified organisms in our food supply, sugars, calories, and high-protein diets; as well as a recommendation for helping your patients choose a healthy diet and adopt healthy dietary behaviors is reviewed.
Keywords
‘While there is a plethora of nutrition misinformation circulated daily, I chose to focus on 4 areas that have received the focus of controversy and disagreement over the past few years . . . genetically modified organism (GMO) food, sugars, calories, and high-protein diets’
Our food supply and our environment are intertwined, yet from a public health standpoint there seems to be a disconnection between what our society wants and what it may need in terms of nutrition and disease prevention. We want our food supply to be safe, available, affordable, fresh, and tasty. We also want our environment to be minimally affected, animal rights to be upheld, and less waste to occur. In terms of public health, however, it comes down to more basic needs: adequate hydration and nutrition (adequate calories and essential nutrients) that improves health in a diverse population at a reasonable cost.
This is all easier said than done, and eating habits are much more complex than you may imagine. Within the context of “What is the best diet?” question comes nutrition controversies. While there is a plethora of nutrition misinformation circulated daily, I chose to focus on 4 areas that have received the focus of controversy and disagreement over the past few years, and will likely continue to get attention over the next few: genetically modified organism (GMO) food, sugars, calories, and high-protein diets.
As with almost anything controversial, there is often a great deal of emotional response to these topics. Fear of anything perceived as “unnatural” is common. Whether we realize it or not, we all bring personal bias to the table when it comes to both personal and cultural food preferences. 1 Our ideas of “the best diet” may also vary, and my goal is to help you understand the importance of healthy “eating” and not just the “healthiest diet,” as evidence shows there is more than one set of foods that may form the healthiest diets. 2
GMO Food
The World Health Organization (WHO) defines genetically modified organisms (GMOs) as organisms in which the genetic material (DNA) has been altered in a way that does not occur naturally. 3 It allows selected individual genes to be transferred from one organism into another, including between nonrelated species. The question on the minds of health professionals and consumers alike is, “Are they safe?” According to the International Food Information Council Foundation, GMOs are an extension of the type of food biotechnology development that has provided nectarines, tangerines, and similar advancements. Food biotechnology is the evolution of traditional agricultural techniques such as crossbreeding and fermentation. These types of foods have been safely consumed for over 15 years. Keep in mind that regulatory review is in place. The Food and Drug Administration and the Environmental Protection Agency, examine every GMO plant or animal feed supply for potential health risks and overall safety. The WHO states that current GMO foods on the market have passed risk assessments and are unlikely to present human risk. 3
The main issues of concern in regard to human safety are allergenicity, gene transfer, and outcrossing. 3 Protocols for allergen tests for GM foods have been evaluated by the Food and Agriculture Organization of the United Nations and the WHO. No allergic effects have been found relative to GM foods currently on the market. The WHO concludes that antibiotic resistant genes could be problematic, and while the gene transfer probability is low, use of technology without antibiotic resistance genes has been encouraged. Outcrossing is the movement of GM plants to conventional crops. Strategies should be put in place to reduce mixing, including a clear separation of the fields within which GM crops and conventional crops are grown. In general, there is a lack of human research, and rat studies have been inconclusive with regard to proving toxicity.3,4
In addition to safety, there is the question of necessity—Is GMO food technology necessary? This type of technology may help feed the planet as it increases yield with virus-resistant crop varieties. In less than 3 decades, the UN predicts that the world population will reach 9.6 billion people, and the US population is predicted to be over 430 million by the year 2050. 5 Considering the earth’s limited fertile land, plants engineered to grow where they could not survive in the past may serve our growing population. Virus-resistant crops can also provide higher yields and hardier plants.
Nonetheless, there continues to be misunderstanding and quickly drawn conclusions about the use and safety of GMO seed and foods. For instance, Bt-corn (Bacillus thuringiensis) garnered attention in popular mainstream media, misnamed “biotoxin corn.” Popular media has published stories that claim it causes an insects stomach to “explode.” This type of journalistic hysteria promotes fear and a lack of understanding about the products in question. The protein binds to the gut wall of the insect, and the insect stops feeding. The gut wall quickly breaks down and the insect dies. Bt-corn is actually a GMO using the Bt-bacterium (which is naturally occurring), and in turn it produces a protein that kills larvae, particularly the European corn borer. 6
Sugar
Sugars have been a hot button for several years now. In August 2013, even National Geographic magazine 7 had a photo of a cupcake on its cover with the headline: “Sugar: Why We Can’t Resist It.” Scientific American also published a story on the topic. 8 These stories discuss all sugars, but fructose and high-fructose corn syrup have been under the most scrutiny. Other caloric sweeteners (including agave nectar and honey) are often thought to be more “natural” and are overlooked as “problematic” sweeteners. The bottom line is, “Sugar is sugar.” There is no disagreement in the nutrition community that most people need to reduce their intake of sugars, but that is all sugars, regardless of type. Robert Lustig began a crusade against fructose in 2009 when he posted a lengthy YouTube video of one of his lectures on what he believes is the potential toxicity of fructose. It now has more than 4 million views. Others, such as journalist Gary Taubes, have written books reaching similar conclusions about the potential toxicity of sugar.
Much of the research that points to high fructose corn syrup as a potential dietary hazard actually uses pure fructose in methodology. In reality most people consume far less fructose than the amounts used in studies, particularly rat studies. High-fructose corn syrup is often singled out as the primary source of fructose in our food supply, when in fact sucrose currently holds that role. High-fructose corn syrup and sucrose are metabolized in nearly identical ways. 9 They deliver the same sugars, about 50% glucose and 50% fructose (see Figure 1), and affect metabolic markers for obesity and disease (insulin, glucose, and appetite hormones ghrelin and leptin) in a similar way. 10 There have been no human studies that show that high-fructose corn syrup is uniquely responsible for obesity. In fact, obesity rates continue to climb as high-fructose corn syrup use declines. 11
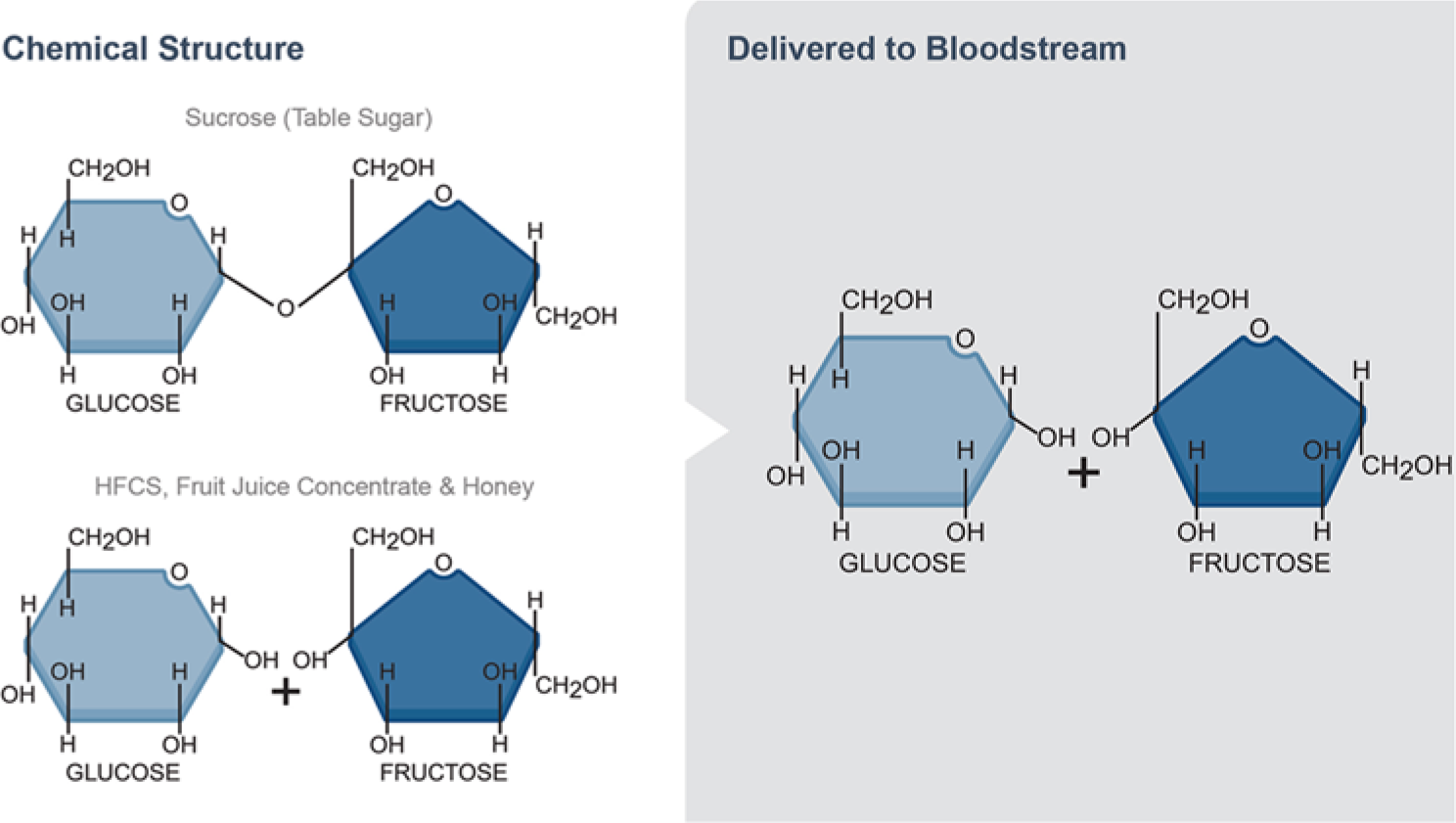
Chemical Structures of Sucrose and High-Fructose Corn Syrup.
Calories
Another controversial topic that has emerged is the answer to the question: Is a calorie a calorie? We know that a calorie is defined as the amount of heat required to raise the temperature of 1 g of water 1°C. There have been various opinions about this concept, and some feel that some foods should be labeled “bad” while others are labeled “good.”
In terms of public health and wellness, a calorie is a calorie, and total energy intake does matter. Based on food availability data, calorie intake has potentially increased by about 458 calories from 1970 to 2010. 11 Flour and cereal products account for 37% of the increase while added fats contribute 53%. Sugars provided 7%, and 3% is contributed by all other foods. While one can argue over the minutia of the laws of thermodynamics 12 —if calorie intake does not match metabolic output, weight gain generally occurs, usually in the form of adipose tissue.
Debates have emerged that argue it is just a question of what type of food is eaten, but it is also important to recognize the portion sizes of foods. Larger portions add more calories to the diet as well. There is no question that portion sizes of common foods (particularly carbohydrate foods such as bagels or muffins, but beverage cup sizes as well) have become increasingly larger since the 1970s. The size of a 2013 bagel has more than doubled that of the 1990 bagel for instance. Portion sizes of other bakery items, such as brownies, cinnamon buns, or cookies, have also become distorted. What appears to be a single portion is actually 3 portions or more.
So is it the carbohydrate food, or the portion? In a study of 811 adults given 4 different reduced diets, weight loss was achieved regardless of the balance of macronutrients. The 4 diets provided various percentages of calories from fat, protein, and carbohydrate, and despite the variances, clinically meaningful weight loss resulted. 13 At the 6-month mark, participants had lost an average of 7% of their initial body weight, but did regain some weight at the 12-month mark. By 2 years, however, weight loss remained similar, whether assigned the 15% or the 25% protein diets (3.0 and 3.6 kg, respectively). For the carbohydrate variances (65% vs a low carb 35%) weight loss was similar as well (2.9 and 3.4 kg, respectively). Among the 80% of participants who completed the trial, the average weight loss was 4 kg; 14% to 15% of the participants had a reduction of at least 10% of their initial body weight. Satiety, hunger, satisfaction with the diet, and attendance at group sessions were similar for all diets.
High-Protein Diets
High-protein diets continue to be a popular weight loss method, but as the Sacks study 13 suggests, dietary composition of carbohydrate, fat, and protein does not significantly affect successful weight loss. The National Academy of Science recommends 0.8 g of protein per kilogram body weight. The Recommended Dietary Allowance for adult (age 19-70+) females is 46 g per day, and for males it is 56 g daily. Protein needs to increase significantly during stress such as surgery or trauma, but for most healthy individuals, 0.8 to 1.2 grams per kilogram body weight, is all that is required for normal muscle function and repair.
Protein is found in all animal tissue, with beef, pork, fish, or poultry providing 7 g of protein per ounce. Eggs and dairy products also offer significant protein, and nuts, seeds, vegetables, and grains provide plant proteins. Popular high-protein diets include the Atkins Diet, South Beach Diet, and the most current trend, the Paleo Diet. While each varies in detail, each is heavy on protein, generally providing about 25% of calories from protein. Some are higher in fat, and some research has shown that a lower fat, high-protein plan results in less adverse changes in biomarkers for disease. 14
While high-protein diets are generally successful in promoting weight loss due to the calorie deficit that is created, there may be some benefit to this regime in those prone to metabolic syndrome 15 although it is certainly not the only effective dietary regime. 16 The foods and food groups that these diets often eliminate, however, is of concern. Minerals such as calcium, vitamin D, magnesium, and phosphorus, as well as B vitamins and fiber, may be deficient.
Summary
We are left with the question: What should I eat? There are many ways to eat, and many foods and beverages to choose from that can result in a healthy diet that reduces disease risk. Rather than focus on an ingredient, or one food, it may be better to focus on the entire diet and eating behaviors and patterns. 2 As health professionals interested in wellness and disease prevention, we may be better served forming consensus on the “healthiest eating behaviors”17-19 as opposed to the “healthiest diet.”
Healthy eating may include behaviors such as the following:
Normal eating patterns providing the energy to support daily activity
Ability to choose a variety of health foods, and small to moderate portions of not-so-healthy foods
Self-awareness of eating cues (hunger and satiety)
Self-awareness of emotional eating situation or cues
Balance and moderation with food and activity, and all aspects of our lives (stress management)
The USDA 20 and the American Heart Association 21 agree on some basic points regarding “the best diet”:
Calories support activity (ie, calories in = calories out)
Balanced for protein (10% to 35%), carbohydrate (45% to 65%), and fat (20% to 30%)
Low in saturated fat (<7%)
Adequate in “healthy fats” (polyunsaturated, monounsaturated—provision of omega 3 and omega 6 fatty acids)
Moderate in sodium (1500-2300 mg)
Adequate in fiber (less refined grains; about 24 g fiber daily)
Low in sugar (IOM guideline is <25% daily calories, AHA is 100-150 kcal/day)
The following list suggests goals you may recommend to help patients develop healthier eating habits:
Recommend a diet and exercise journal
Recommend consistent eating schedules to avoid excessive hunger, and ensure balanced nutrition
Suggest ways to add more fruits and vegetables into the diet
Suggest they include more whole grains and less refined grains, but reduce portions of most bread/grain products
Slow down. Pay attention to satiety cues
Schedule more activity into daily life, and plan some additional physical activity (exercise) at least 3 days a week
While there is no complete definition for normal eating, 19 there is some consensus about helping patients achieve their dietary goals.22,23 While many physicians are attempting to provide nutrition counseling, employing the help of a registered dietitian/nutritionist (RDN) can help a physician’s practice become more effective in terms of diet-related issues such as weight management, diabetes, or cardiovascular nutrition. 24 Evidence supports a long-term approach, particularly in the area of weight management.3,25