
Abstract
Stroke is a leading cause of disability in the US, often altering one’s ability to access and consume food. The aim of the present study was to characterize and evaluate predictors of stroke survivors’ diet quality (DQ). A cross-sectional evaluation of 2011-2018 National Health and Nutrition Examination Survey data is presented. Stroke survivors (n = 632) were matched for age, gender, and race with neurologically intact controls (n = 913). Food group intake, key nutrient intake, and Healthy Eating Index (HEI)-2015 scores were calculated from two 24-hour recalls and evaluated in relation to history of stroke, education, presence of a partner in the home, and income. Group differences in and predictors of DQ were evaluated with weighted independent samples t-tests and linear regression. Stroke survivors had lower intakes of vegetables, dairy, seafood and plant proteins, and unsaturated fats, and lower total HEI-2015 scores (P < 0.05). Having more education, a partner in the home, and higher income were overall positive predictors of DQ. DQ factors emphasized in heart-healthy diets were low in stroke survivors. Interventions may better address barriers to healthy eating post-stroke by incorporating educational, financial, and social support components.
“The food groups and nutrients consumed in lower amounts among stroke survivors are noteworthy when considering rehabilitation and future disease risk of stroke survivors.”
Introduction
Stroke is among the leading causes of death in the United States, yet the cohort of nearly 7 million stroke survivors often goes under-studied, whilst over half of survivors battle the effects of their inability to independently ambulate and function.1-4 The sequelae post-stroke alter health-related quality of life of stroke survivors in many ways,1-4 one of which may be the ability to obtain and prepare food. In fact, when comparing food insecurity in US adults with or without a history of stroke, Kim-Tenser et al 5 found stroke survivors to report an alarmingly high rate of food insecurity of 42%, compared to 17% in individuals without stroke. Furthermore, over half of acute stroke patients experience difficulty swallowing, known as dysphagia, which affects the types and textures of foods they are able to safely consume. 6 While dysphagia resolves in most stroke survivors, 11%–13% still experience some level of dysphagia 6 months post-stroke, significantly impacting their food and nutrient intake, particularly from animal protein sources, and risk for malnutrition and other conditions. 6
Malnutrition can refer to both overnutrition and undernutrition, but in the acute clinical setting, malnutrition typically refers to undernutrition characterized by weight loss, inadequate energy intake, muscle and fat loss, and/or fluid retention. 7 Malnutrition is associated with poorer rehabilitation outcomes of stroke patients, negatively impacting their health-related quality of life, as well as increased mortality 3-6 months post-stroke. 8 Furthermore, and potentially just as imperative, malnutrition is associated with increased stroke incidence, making it a concern for stroke re-occurrence in stroke survivors. 9
In chronic stroke survivors, dietary concerns are typically different than those in the acute setting, as individuals have often regained the ability to maintain an adequate energy intake, yet their ability to meet specific food group and nutrient requirements, that is, their diet quality, may be altered due to functional changes, as discussed previously. 10 Diet quality has been defined as the extent that a dietary pattern promotes health and reduces risk for chronic diseases. 11 In light of the role that diet quality plays in stroke survivors achieving the goals of stroke rehabilitation to improve functional mobility and decrease risk for stroke re-occurrence, it is important to understand the diet quality of stroke survivors. While evaluations of stroke survivors’ intake of individual macronutrients and some micronutrients have been published, 10 few studies have evaluated food group and nutrient intake of stroke survivors in comparison to the US Dietary Guidelines for Americans (DGAs), which provides a more comprehensive and realistic understanding of dietary intake that accounts for interaction between individual food groups and nutrients. Furthermore, potential predictors of diet quality of stroke survivors, such as income, the presence of a support person(s) in the form of a spouse or partner in the home, and education level, are largely unstudied.
A deeper understanding of the current intake of stroke survivors compared to recommendations beyond individual macro- and micronutrients, as well as predictors of stroke survivors’ diet quality, is integral to the development of evidence-based, effective interventions aiming to improve stroke survivors’ diet quality and overall health-related quality of life and decrease future disease risk. Thus, the aim of the present study is to evaluate stroke survivors’ food group intake, nutrient intake, and diet quality measured by adherence to the Dietary Guidelines for Americans compared to matched neurologically intact controls in the US, as well as potential predictors of these dietary outcomes.
Methods
Participants
The study population included respondents of the National Health and Nutrition Examination Survey (NHANES), which is a series of cross-sectional surveys used to monitor and evaluate the health status of representative samples of the US population. 12 NHANES surveys approximately 5000 individuals each year, and the data is made publicly available in 2-year cycles. 12 Further information about the study population of NHANES is reported elsewhere. 12 The present study utilized data from the 2011-2018 NHANES cycles. All 2011-2018 NHANES participants with a history of stroke were included in the study sample, and neurologically intact controls matched to the stroke group based on age, gender, and race were also included. From this total sample, participants with two 24-hour recalls were included in the analyses. According to Department of Health and Human Services 45 CFR 46.102, this study does not constitute human subjects research.
Measures
Demographics, including age, gender, race, education level, family income to poverty ratio (ratio of family income to national poverty thresholds), marital status, as well as history of stroke and age of stroke occurrence, were collected as part of the NHANES household interview. 13 Trained NHANES interviewers guided participants in the completion of the household interview using a computer-based interview platform. 13 Anthropometrics, blood-based biomarkers, and dietary intake were measured as part of the Mobile Examination Center (MEC) examinations and interviews. 12 weight, height, and waist circumference were collected as part of the anthropometric exam, with body mass index (BMI) calculated as weight (kg)/(height [m])2. 13 Dietary intake was collected using 2, 24-hour recalls. 13 Trained interviewers conducted 24-hour recalls with participants in MECs. 13 2, non-consecutive 24-hour recalls were conducted using the Automated Multiple-Pass Method. 13 Recalls were conducted between 3 and 10 days apart, with the first recall conducted in person and the second conducted via phone. 13 Participants were provided with the USDA Food Model booklet to assist in portion size estimation. 13
Data Cleaning
Outliers in the dietary data, identified as total kilocalories being outside the 5th to 95th percentiles of intakes reported by adults in the NHANES (males: 650-5700 kcal; females: 600-4400 kcals), were removed. 14
Levels of marital status (married, widowed, divorced, separated, never married, and living with partner) were collapsed into 2 levels: presence of support person/partner in the home (married or living with partner), or absence of support person/partner in the home (widowed, divorced, separated, never married) to better capture any relationships between presence of a support person/partner and the outcomes of interest.
HEI Calculation
The Healthy Eating Index (HEI)-2015 total and component scores were calculated from the 2 24-hour recalls completed as part of the NHANES surveys.15-17 The HEI-2015 includes 13 components (total vegetables, greens and beans, total fruit, whole fruit, whole grains, refined grains, dairy, total protein foods, seafood and plant proteins, monounsaturated and polyunsaturated fatty acids, saturated fatty acids, sodium, and added sugars).
16
Each component is scored individually, and the scores for each component are totaled to provide an overall HEI-2015 score. Component scores range from 0-5 or 0-10, depending on the component, whilst the HEI total score can range from 0 to 100. Food group scores (total vegetables, greens and beans, total fruit, whole fruit, whole grains, refined grains, dairy, total protein foods, and seafood and plant proteins) were calculated by comparing cup or ounce equivalent intakes per 1000 kcal consumed to DGA recommendations. The fatty acid ratio score was calculated by comparing the ratio of unsaturated (monounsaturated and polyunsaturated) fat to saturated fat intake to DGA recommendations. Sodium score was calculated by comparing sodium intake per 1000 kcal to DGA recommendations. Lastly, saturated fat and added sugar scores were calculated by comparing percent of energy consumed from saturated fats and added sugars to standards (
Resting and Total Energy Expenditure
Resting and total energy expenditure were estimated as a comparison for reported energy intake. The Mifflin-St. Jeor equation was used to calculate resting energy expenditure (REE) in both groups per nutrition care guidelines, and a sedentary physical activity factor of 1.2 was used as an approximate estimate of energy expenditure from physical activity to calculate total energy expenditure (TEE). 18
Data Analysis
All statistical analyses were performed using SPSS version 29 19 and SAS OnDemand for Academics 20 and accounted for the complex sampling design of NHANES by utilizing weighted analyses according to published guidelines 21 to obtain a nationally representative sample. Sample weights were constructed from published 2 year weights to ensure accuracy of weighting for the combined 8 years of consecutive data included in this study. 21 Dietary sample weights were used for analyses. 21 Descriptive statistics (mean, standard error [SE], frequencies [%]) were used to characterize participant demographics, anthropometrics, and diet quality measures. Independent samples t-tests were used to identify any significant differences between stroke and neurologically intact groups, with alpha set at 0.05. Sufficient power was available with our sample size to detect a meaningful 10% difference in total HEI-2015 score between groups (power >0.95). 22 Weighted linear regression models were used to evaluate relationships of the outcomes of interest (food group intake, nutrient intake, HEI total and component scores) with independent variables (history of stroke, education level, poverty ratio, and presence of a partner in the home). Histograms, predicted probability (P-P) plots, and variance inflation factors were evaluated to confirm that linearity, normality, homoscedasticity, and independence of variables assumptions of linear regression were met. Post-hoc analyses for significant independent variables included calculation of estimated marginal means (EMM), beta coefficients, and pairwise comparisons where appropriate.
Results
Descriptive Participant Characteristics of Stroke Survivors and Neurologically Intact Controls.
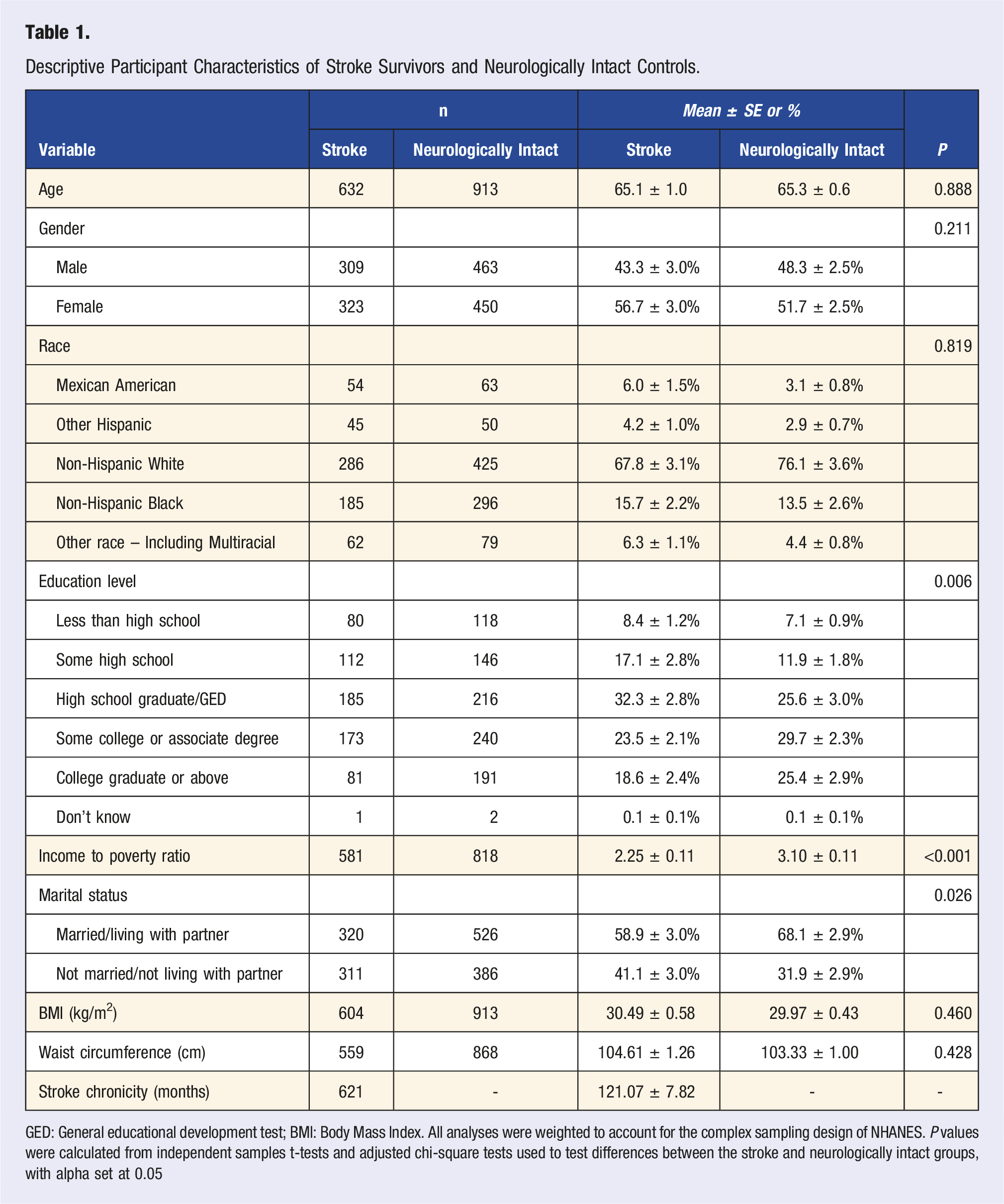
GED: General educational development test; BMI: Body Mass Index. All analyses were weighted to account for the complex sampling design of NHANES. P values were calculated from independent samples t-tests and adjusted chi-square tests used to test differences between the stroke and neurologically intact groups, with alpha set at 0.05
Anthropometrics
Anthropometrics are presented in Table 1. BMI and waist circumference were not significantly different between groups. Average BMI of stroke and neurologically intact individuals was 30.49 ± 0.58 kg/m2 and 29.97 ± 0.43 kg/m2, respectively, placing the average individual in both groups in the overweight category according to BMI.
Diet Quality
Food Group Intakes, Nutrient Intakes, and HEI Scores of Stroke Survivors and Neurologically Intact Controls.
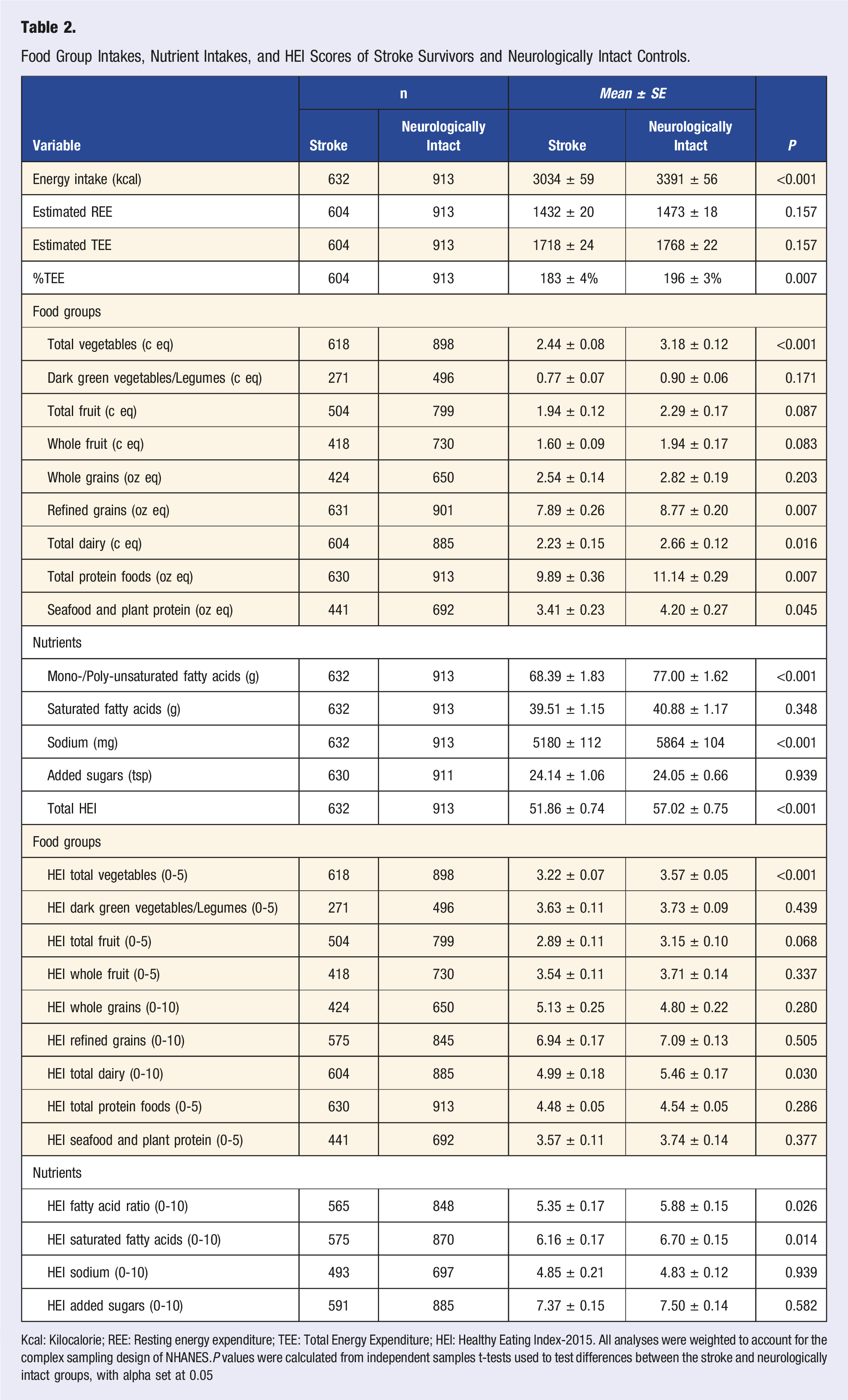
Kcal: Kilocalorie; REE: Resting energy expenditure; TEE: Total Energy Expenditure; HEI: Healthy Eating Index-2015. All analyses were weighted to account for the complex sampling design of NHANES.P values were calculated from independent samples t-tests used to test differences between the stroke and neurologically intact groups, with alpha set at 0.05
Relationship of Stroke and Demographics to Diet Quality Measures.

Kcal: Kilocalorie; GED: General Educational Development test; HEI: Healthy Eating Index-2015*Reference category for “stroke” categorical variable was “neurologically intact controls”; reference category for “education level” categorical variable was “college graduate or above”; reference category for “support person” categorical variable was “not married/not living with partner”
Energy
Average reported energy intake in the stroke and neurologically intact groups were 3034 ± 59 kcal and 3391 ± 56 kcal, respectively, which equated to 183% and 196%, respectively, of estimated total energy expenditure. When evaluated alongside history of stroke, education level, presence of a support person in the home, and income to poverty ratio were all significant predictors of energy intake (Table 3). Individuals with a support person in the home and with higher incomes had higher energy intakes, while individuals with no high school had significantly lower energy intakes (EMM: 2882
Food Groups
Stroke survivors’ intake of 5 of the ten food groups evaluated differed significantly from intake of neurologically intact controls (Tables 2 and 3). Stroke survivors had significantly lower intakes of total vegetables, refined grains, total dairy, total protein foods, and seafood and plant proteins (Tables 2 and 3). When evaluated alongside education level, presence of a support person in the home, and income to poverty ratio, history of stroke was a significant predictor of intake total vegetables, dark green vegetables/legumes, and refined grains (Table 3). Again, history of stroke was related to lower intakes of each of these food groups. Interestingly, while a lower income to poverty ratio was related to lower intakes of total vegetables, a lower income to poverty ratio was related to a higher intake of dark green vegetables and legumes. Having a support person in the home was also related to higher intakes of refined grains. Education level was related to intakes of both total fruits and seafood and plant proteins, with college graduates having higher intakes of both total fruits (EMM: 2.65
Nutrients
Stroke survivors’ intake of mono- and polyunsaturated fatty acids and sodium was significantly lower than intake of neurologically intact controls (Tables 2 and 3). Presence of a support person in the home and income to poverty ratio were also significant predictors of intakes of these nutrients, with individuals with a support person in the home and individuals with a higher income having higher intakes (Table 3). A support person and income to poverty ratio were also predictors of saturated fat intake, again, with individuals with a support person in the home and a higher income having higher saturated fat intakes (Table 3).
HEI Scores
Stroke survivors had significantly lower HEI component scores for dairy, fatty acid ratio, and saturated fatty acids than their neurologically healthy counterparts (Tables 2 and 3). Total HEI score was alarmingly lower in stroke survivors, with an average score of 51.86
Discussion
This study provides insight into both food group and nutrient intakes of stroke survivors in the US compared to their neurologically intact counterparts. Overall, stroke survivors’ food group intake was lower than neurologically intact adults, placing them further away from meeting Dietary Guidelines for Americans recommendations as indicated by a significantly lower total Healthy Eating Index-2015 score. Income, measured by the family income to poverty ratio, and the presence of a partner/support person in the home were predictors of intake of several food groups and nutrients, highlighting potential areas of support to promote improved diet quality among stroke survivors.
Energy intake of stroke survivors was less than neurologically intact adults, yet it was still greater than estimated total energy expenditure. While actual energy needs likely differ from those estimated using Mifflin-St. Jeor and a general activity factor, the average BMI of the stroke survivors included in the present study (29.97 ± 0.43 kg/m2) was above what is generally considered a healthy range. In light of the high rates (∼30%–45%) of obesity among stroke survivors 23 and the known impact of obesity on functional mobility and disease risk, including re-occurrence of stroke among stroke survivors,24-26 attention to energy intake is warranted as part of weight management and lifestyle intervention efforts among stroke survivors.
The food groups and nutrients consumed in lower amounts among stroke survivors are noteworthy when considering rehabilitation and future disease risk of stroke survivors. Intake of many components of a Mediterranean dietary pattern, including vegetables, seafood and plant proteins, and unsaturated fatty acids such as olive oil, were all lower among stroke survivors compared to neurologically intact adults. The Mediterranean diet is well-supported for its promotion of heart health, including stroke prevention.27-31 Mediterranean diet-focused programming for stroke survivors has been pilot tested, 32 yet opportunities remain for further testing, dissemination, and implementation of lifestyle interventions that promote a Mediterranean dietary pattern among stroke survivors. The Dietary Guidelines for Americans provides food group recommendations that align with a Mediterranean dietary pattern that may be helpful for development of such interventions. 33 Furthermore, some resources exist on adapting a Mediterranean dietary pattern to incorporate local and cultural foods, 34 increasing the attainability and sustainability of the dietary pattern for stroke survivors.
The Dietary Approaches to Stop Hypertension (DASH) diet is another evidence-based dietary pattern for maintenance of healthy blood pressure through decreased intake of sodium and increased intake of potassium, calcium, and magnesium from vegetables, fruits, whole grains, and low-fat or fat-free dairy. 35 While stroke survivors had significantly lower sodium intakes than neurologically intact adults, average intake (5180 ± 112 mg) was still significantly higher than DGA recommendations of no more than 2300 mg sodium per day. 33 Thus, stroke survivors are similar to the neurologically intact population in their need for reduced sodium intake; and incorporating strategies for reducing sodium into lifestyle interventions for stroke survivors is warranted. In addition, total dairy intake was significantly lower in stroke survivors and below recommendations. 33 While dairy is not the only source of calcium, it is difficult to meet calcium recommendations without dairy or calcium-fortified dairy alternatives. With calcium needs increasing with age for maintenance of bone health, and many stroke survivors being at increased fall risk due to neurological and muscular changes post-stroke, dairy or calcium-containing alternatives are a high-priority food group for stroke survivors.3,33 Furthermore, many forms of dairy, including milk and yogurt, are good sources of protein, another nutrient lower in stroke survivors but important for maintenance and building of muscle mass during stroke rehabilitation. 8
Income was a significant predictor of many of the important food groups and nutrients discussed previously, including vegetables, unsaturated fatty acids, and saturated fatty acids. While it is well-known that a higher income decreases barriers to healthy eating, 36 it is important to consider strategies to decrease stroke survivors’ income barriers to adequate food group and nutrient intake. As stated previously, stroke survivors experience high rates of food insecurity. 5 However, minimizing financial barriers to healthy eating does not guarantee improved diet quality, as evidenced by some of the present study’s results indicating that those with higher income to poverty ratios had higher intakes of sodium, saturated fat, and refined grains. Kim-Tenser et al 5 also found lower education, as well as lower income to poverty ratio and nonmarried status, to be predictors of food insecurity in stroke populations. The present study also found absence of a partner in the home, which was experienced by nearly half of the sample of stroke survivors, was another predictor of many dietary measures, including intake of unsaturated fatty acids. Physical limitations post-stroke that often impair stroke survivors’ ability to grocery shop, cook, and even eat, combined with the absence of a partner in the home and limited income, may be a perfect storm for poor rehabilitation outcomes and health-related quality of life among stroke survivors. Multicomponent interventions that include education and counseling on healthy eating as well as social and environmental supports may be needed to effectively address diet quality concerns among stroke survivors.
While average income of stroke survivors in the present study was above the poverty threshold, the average income was outside the eligibility requirements for many federal food assistance programs, as eligibility for most food assistance programs requires income to be 130%–185% of the poverty threshold 37 ; and average income of stroke survivors in the present study was 219% of the poverty threshold. Stroke survivors may “fall through the cracks” of federal food assistance programs for these reasons, leaving them to rely on more local programs like Meals on Wheels 38 that often have limited resources and waiting lists for eligible participants.
As stated previously, presence of a partner/support person in the home was a significant predictor of several diet quality measures. While there are clearly other sources of social support both inside and outside the home besides a spouse/partner, presence of a partner in the home is a simple indicator of in-home support that has been consistently measured throughout NHANES cycles and can be valuable given the common physical limitations that ensue post-stroke. 39 The role of a partner in stroke survivors’ diet quality highlighted in this study emphasizes the importance of incorporating partners in nutrition-related interventions aiming to improve stroke survivors’ diet quality. Furthermore, for the nearly 50% of stroke survivors that may not have a partner in the home according to this study sample, developing and disseminating interventions that provide social support to stroke survivors is imperative to optimizing diet quality. 40
Stroke was not a significant predictor of many HEI component scores, but history of stroke, along with education level and presence of a support person in the home, were significant predictors of total HEI score. Average total HEI of stroke survivors was 51.86 ± 0.74 compared to 57.02 ± 0.75 in neurologically intact adults. Average total HEI score among US adults is 58, and among US adults 60+ years old, average total HEI is 61. 33 The disparity between total HEI scores in neurologically intact adults and the stroke survivors included in this study is alarming, especially considering the importance of diet quality for stroke recovery, rehabilitation, and prevention of stroke re-occurrence. Theoretically, an “optimal” total HEI score is 100, as this maximum score indicates adherence to an individual’s food group and nutrient recommendations, including recommended limits for saturated fats, added sugars, and sodium, found in the Dietary Guidelines for Amercians.16,41 While it is expected that an individual will not meet all dietary recommendations at all times, in order to optimize health and prevent disease, meeting a majority of dietary recommendations as evidenced by a total HEI score close to 100 is the goal. The 51.86 average total HEI score of the stroke survivors in our sample indicates that, on average, barely half of their food group and nutrient recommendations are met, again, highlighting the nutritional concern these findings raise for this population. Stroke rehabilitation therapy traditionally focuses on exercises to promote functional mobility and reduce post-stroke disability, while post-stroke nutrition care may include brief inpatient nutrition education on a heart-healthy diet and an outpatient nutrition counseling session, at most, with a registered dietitian. Given the results of this and similar studies that highlight disparities in diet quality and its predictors among stroke survivors,5,39 incorporation of additional nutrition care for stroke survivors in traditional stroke rehabilitation therapy is warranted. In addition, development and dissemination of evidence-based interventions that target diet quality predictors like income and social support are imperative to improve quality of life among the large cohort of stroke survivors living in the US.
Limitations
While this study does use a nationally representative sample, it is not without limitations. First, not all available NHANES data were used. Due to variations in data collected in the NHANES cycles between 1999 and 2010, the independent and dependent variables of interest for the present study were only consistently collected after 2010.12,13 In addition, the onset of the COVID-19 pandemic limited the dietary data collected and available from the 2019-2020 cycle, limiting our dataset to 2011-2018.12,13 Furthermore, while utilizing a spouse/partner in the home is a good measure of in-home support, it is understood that there are other sources of social support missed by using this measure alone. Again, social support has been assessed through different measures across the NHANES cycles. Since marital status has been consistently measured across the NHANES cycles and is a measure of in-home support, an important form of support for many stroke survivors who have physical limitations post-stroke, 3 marital status was chosen as a social support predictor for this study. Additionally, though the Mifflin-St. Jeor predictive energy equation is supported for estimating resting energy expenditure in the stroke population, 18 the sedentary physical activity factor used to estimate total energy expenditure in this study has limited accuracy compared to an objective measure of actual physical activity level, which was not collected as part of the NHANES surveys. Furthermore, the sample sizes of the stroke survivor and neurologically intact groups were not the same due to differences in the number of participants who completed 2 24 hour recalls in each group. However, the 2 groups still did not differ in the characteristics for which they were matched (age, gender, race). The food group and nutrient intakes calculated from the 24-hour recalls were also not representative of usual intake according to the National Cancer Institute Method, which does introduce the limitation of intra-individual variation of dietary intake. However, only participants who completed both 24-hour recalls were included in the analyses to mitigate this limitation. It is also important to note that type of stroke and stroke severity may have differing impacts on many of the predictors and outcomes evaluated in this study. However, NHANES does not collect information on stroke type and severity. Still, this study highlights areas that may warrant further investigation among samples of the stroke population. Lastly, due to the cross-sectional nature of the NHANES dataset, no causation between stroke and diet quality outcomes can be inferred from this study.
In conclusion, a large cohort of stroke survivors are living in the US; and while stroke has many implications for functional mobility and capacity to obtain and prepare food, diet quality and its predictors among stroke survivors is largely unstudied. The present study aimed to evaluate stroke survivors’ food group intake, nutrient intake, and adherence to the US Dietary Guidelines compared to matched neurologically intact controls, as well as potential predictors of these dietary outcomes. Stroke survivors’ food group intake, especially those food groups part of evidence-based heart-healthy dietary patterns like the Mediterranean and DASH diets, was lower than neurologically intact adults. Stroke survivors had lower total Healthy Eating Index-2015 scores than their neurologically intact counterparts and lower than the national average, highlighting the need for interventions targeting diet quality in stroke survivors. Having a higher income and a partner in the home were positive predictors of stroke survivors’ intakes of several food groups and nutrients. Dietary interventions in stroke survivors may benefit from incorporating financial and social support components to better address the barriers to healthy eating in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.