
Abstract
Physical inactivity is a worldwide public health problem. Primary care physicians are in an excellent position to prescribe exercise and physical activity to their patients. This article discusses theories and methods of behavior change to help physicians motivate their patients to become more physically active. Calls to action for physicians are discussed.
‘Medical professionals must change the ways they counsel patients about exercise; exercise and physical activity are medicine and should be used as such.’
Physical inactivity is a worldwide public health problem. It is estimated that 6% to 10% of major noncommunicable diseases, including coronary heart disease, type 2 diabetes, and breast and colon cancers, are caused by physical inactivity. 1 In 2008, physical inactivity caused an estimated 9% of the 57 million premature deaths, or approximately 5.3 million. 1 In addition, research has indicated that low cardiorespiratory fitness is one of the strongest predictors of mortality.2-4
Primary care physicians are in an excellent position to discuss exercise and physical activity (PA) with their patients and to prescribe PA; however, many are not counseling their patients about these topics. 5 Physicians should talk with their patients about the strong evidence that PA can help reduce coronary heart disease, high blood pressure, stroke, metabolic syndrome, type 2 diabetes, breast and colon cancer, depression, and all-cause mortality. Additionally, physicians should base patient counseling on the research which shows that cardiorespiratory and muscular fitness can lead to improved bone health, improved cognitive function, increased functional health, and healthier body mass and composition.6,7
PA plays a critical role in disease management and quality of life. PA, along with dietary interventions, can help patients with type 2 diabetes better manage their disease. PA also leads to a reduction of hepatic fat accumulation commonly associated with type 2 diabetes. 8 PA has been shown in a meta-analysis to decrease the severity of sleep apnea, even when patients lost little or no weight. And when patients with sleep apnea increase their cardiorespiratory fitness, daytime sleepiness is reduced and sleep efficiency increases. 9 Promising evidence also indicates that exercise can improve anxiety symptoms. 6 When older adults participate in PA, the result is a delay in dependency and frailty and an increase in quality of life. 10
The current recommendations for physical activity indicate that it is important to avoid inactivity, and they note that even modest amounts of activity have health benefits. The recommendations for adults include either 150 minutes per week of moderate-intensity physical activity, 75 minutes of vigorous-intensity physical activity or some combination of the two. 6 It is recommended that children accumulate at least 60 minutes of moderate to vigorous physical activity a day. 6 It is not necessary to go to a fitness center many times a week or run marathons, although higher amounts of activity provide additional health benefits. An overall summary of the Physical Activity Guidelines for Americans 6 for aerobic PA is presented in Table 1. The guidelines also recommend resistance training to improve muscular strength of major muscle groups on at least 2 days per week.
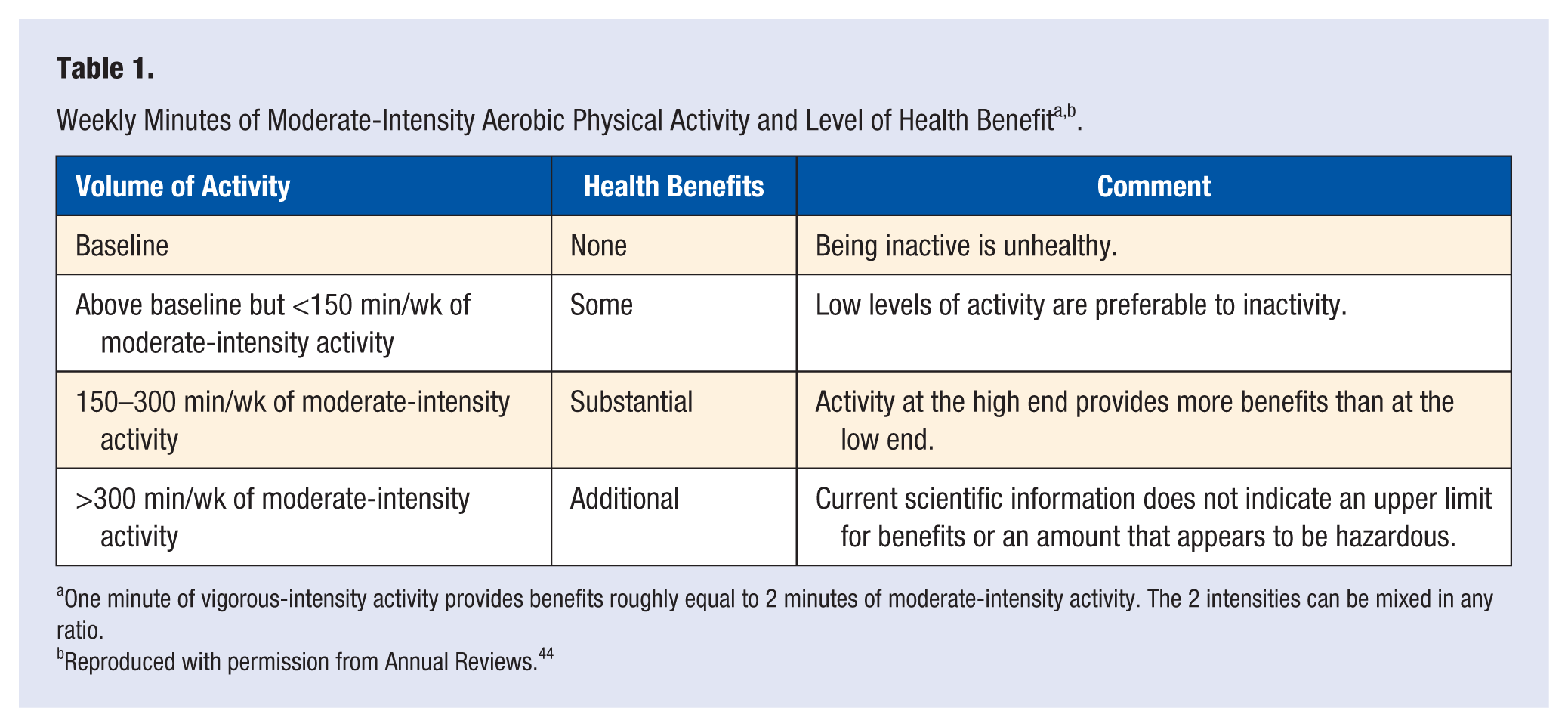
One minute of vigorous-intensity activity provides benefits roughly equal to 2 minutes of moderate-intensity activity. The 2 intensities can be mixed in any ratio.
Reproduced with permission from Annual Reviews. 44
Lifestyle Behavioral Change
Helping patients incorporate PA into their lifestyles is a behavioral intervention; for behavioral interventions to be the most effective, it is important to use a theoretical model to help influence and direct the behavior change. Some of the most effective theories used in behavior change models are social cognitive theory, the transtheoretical model, and the social ecological model. Using established theory and behavior change models and strategies can improve adherence to behavioral interventions.11,12
Social cognitive theory was introduced by Bandura 13 in 1986, and the theory and its constructs have been used effectively in behavioral interventions.11,14,15 Of the social cognitive theory constructs, those most widely used in PA behavior modification are those designed to help increase participants’ self-efficacy, rewards and reinforcements, and self-regulation. This theory has been very useful in establishing behavior change, and it is relatively easy to incorporate some constructs into a physical activity plan for patients. Working with patients to set goals, track their progress, and reward themselves for the changed behavior is all that is necessary to incorporate this theory into patient communication when motivating patients to increase PA.
The transtheoretical model uses self-efficacy, along with the stages of changes and processes of change, to help modify behavior.16,17 This theory helps to match the level of the intervention to the participant’s readiness for change and helps to meet people where they are in the process. Success with this model is achieved by moving a person from one level to the next over time, rather than completely adopting the behavior change all at once, although the eventual goal is for participants to reach the maintenance stage. The stages of change include precontemplation, contemplation, preparation, action, and maintenance (Table 2). Health professionals who are interested in using a stages of change approach to help their patients become more physically active should consult Motivating People to Be Physically Active. 18 In addition, Active Living Every Day 19 uses the transtheoretical model in workbook and web-based intervention formats for patients in a 12-week program. This book can help guide patients through the stages of change and help them incorporate PA into everyday life.
Transtheoretical Model: Stages of Change a .
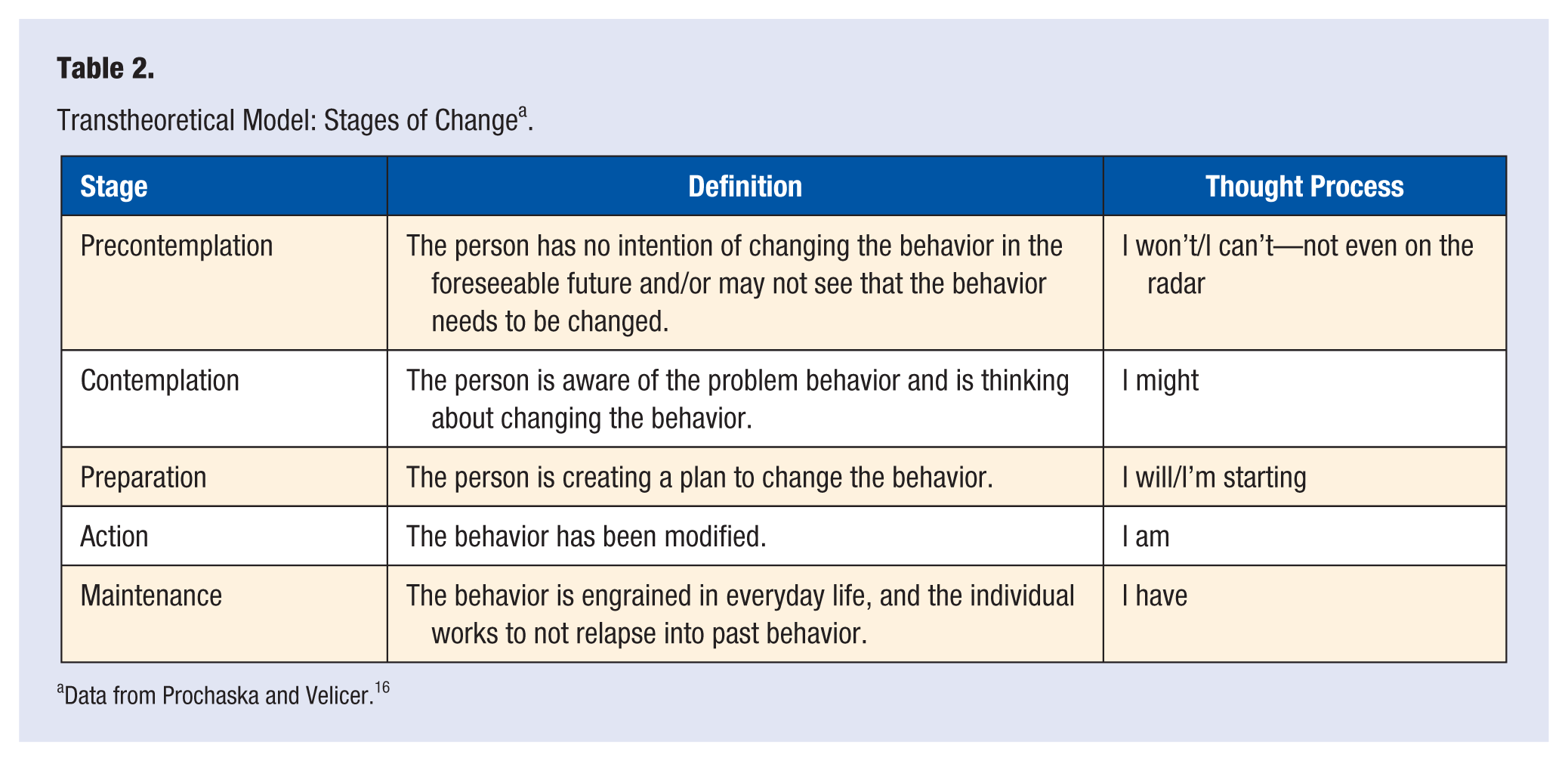
Data from Prochaska and Velicer. 16
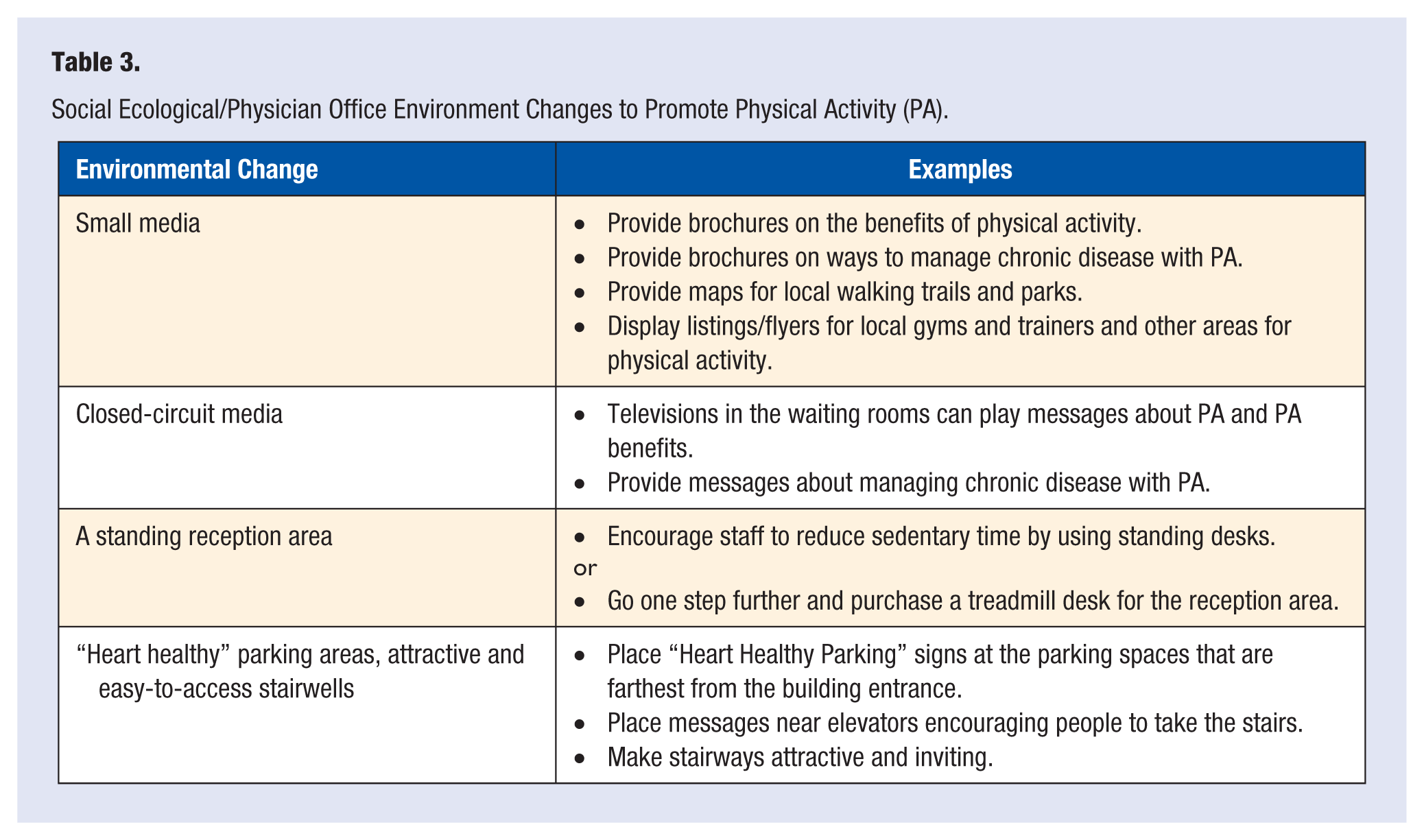
The final theory we will discuss is the social ecological20-22 approach, which includes considering changes in the environment. To see population-wide effects in behavior change, not only do individual interventions need to be implemented but efforts must be made to change the environment in which we live, work, play, and even go to the doctor. With the social ecological perspective, it is understood that behavior is influenced on multiple levels. The physician must ask what can be changed to influence the environment to encourage patients to make healthy choices (Table 3). For example, small media (ie, brochures, flyers, other information) encouraging PA can be displayed in the waiting room. Or signs to indicate “Heart Healthy Parking” can be placed in the farthest parking places at the office location (Figure 1). These small changes to the environment can help influence and motivate patients to increase their current level of PA.
Social Ecological/Physician Office Environment Changes to Promote Physical Activity (PA).

“Heart Healthy Parking” sign.
Other behavior change theory models do exist and can be effective for patients. What is important is to find the method that works best in the physician’s practice with the physician’s patients. Supporting behavior change with a theory-driven model and tested cognitive and behavioral strategies and methods will increase the odds of beneficial outcomes for patients.
How Will This Be Delivered?
When working with patients and advocating behavior change, practitioners should recognize that many times this will be a “two steps forward, one step back” type of process. Behavioral change is difficult and complex, and may factors influence it. When working to motivate patients to exercise, practitioners must first establish where the patient is with his or her own ideas about exercise. Does the patient know exercise is important but cannot seem to find the time to do it? Or is he or she not even aware of how beneficial exercise can be? The simple technique of motivational interviewing (MI) can be used to discover the patient’s current stage of change as well as motivate him or her to make changes. MI is considered a collaborative conversation between practitioner and patient, designed to elicit change and overcome apathy toward change.23,24
When working with patients toward behavior change, physicians and other health professionals should focus on several areas. Help patients solve problems: Why can’t they exercise? Is it a lack of time, lack of fun, or lack of support? Suggest ways to overcome these barriers. Recommend that the patient set a goal, and show him or her how to monitor progress. Encourage the patient to find a reasonable reward for achieving the goal: for example, a massage after a month of regular exercise, a trip to the zoo with a friend, a new pair of exercise shoes. Help the patient establish a social support system. This involves identifying, asking for, and using social support: For example, the patient could ask to join a neighbor during her morning walk. Social support has been shown to be one of the most important factors in maintaining a regular PA program, for everyone from children to older adults.25-30
Working with patients is essential, as is referring them to other professionals for further and more in-depth counseling for behavior change. Behavior change counseling takes time that the busy physician may not have on a daily basis. Build a referral base of practitioners who specialize in PA interventions and behavior change, such as exercise specialists and counselors. Refer patients to a professional within their budget: Don’t send a Medicaid patient to an expensive fitness center.
Physicians can use new technologies to improve and enhance behavioral modifications. Many physician offices already use phone calls, e-mails, and text messages for appointment reminders; this technology can also help patients stay on track with their PA goals and help them to remain motivated. Text messaging with appointment reminders, feedback, and monitoring has been shown to improve compliance with health behaviors and can help improve patients’ health. 31 In a randomized controlled trial for weight loss that included the use of text messages, those who received text messages as part of the intervention lost an average of 2.88 kg more than the control group, and 92% of the intervention group in this study would recommend the intervention to a friend. 32 Along with text messaging, apps for smart phones can help improve patients’ health. Cowan et al 33 reported in 2013 there were 127 iPhone apps in the “health and fitness” category. Many of the apps used theoretical approaches and could be used to support behavior change. 33 Schoffman et al 34 reported similar findings for pediatric apps for weight loss; many of these apps also used theoretical approaches and could help support behavior change. 34 For those who prefer a simpler approach to PA, physicians can recommend or give to patients a pedometer or accelerometer. Research has shown that simply using pedometers helps people increase their physical activity by 2491 steps per day. 35 Pedometers and/or accelerometers can help patients set goals and monitor progress.
Physicians must help patients find a way to be accountable for efforts to improve their health. Helping patients set reasonable goals and establish a system for recording and reporting goal progress can help them to maintain progress. Using technology to track and monitor daily, weekly, and monthly progress will allow patients to see their health improvements.
Calls to Action
Although adding PA interventions or other disease prevention approaches to a busy medical practice seems daunting, physicians and their staffs can make some changes fairly easily that will make a significant difference for patients. These include using exercise as a vital sign, recommending exercise as well as drugs, using technology to support behavior change, and changing the environment.
It is time to start using exercise as a vital sign. Train staff who take vital signs to ask patients about their current level of PA and calculate each patient’s amount (minutes per week) of moderate physical activity. Use this number to assess each patient’s compliance with the Physical Activity Guidelines for Americans and provide appropriate counseling. Adding this information to a patient’s electronic medical record will increase tracking and follow-up. 36 Widespread adoption of exercise as a vital sign could go a long way to improving the population’s health.36-40
It is time to start recommending exercise in the same way that drugs or other therapies are recommended. Evidence supports the role of physicians in promoting PA to patients and indicates that patients can significantly increase PA levels when directed to by their primary care physicians.41,42 According to a recent report, evidence indicates that exercise is equal to drug therapies in prevention of coronary heart disease, treatment of diabetes, poststroke rehabilitation, and treatment of heart failure. 42 When considering the potential negative side effects of drugs versus the positive side effects of PA, exercise clearly is the better choice for many patients. Research shows that when physicians included behavior change strategies and provided written materials, patients did increase their physical activity. 43
It is time to start using technology to support health. Technology continues to change rapidly, so find the type of technology that fits each patient and his or her intended behavior change. The simpler the technology is to use and the easier to track progress, the more effective it will be.
It is time to start changing the environment. Table 3 presents ways to ecologically incorporate PA into the medical practice. Changing the environment can have lasting effects on the population in the practice, not only the patients but also the staff. A healthy work environment can lead to a happier and healthier workforce.
Conclusion
Physical activity is essential for a healthy life, and even small bouts of exercise can increase longevity and quality of life. Medical professionals must change the ways they counsel patients about exercise; exercise and physical activity are medicine and should be used as such.
Behavior change can be difficult and complex, but if it is approached in a theoretical way, with tested cognitive and behavioral strategies, patients can change their behaviors and improve their health. Patients should not seek perfection but rather should aim for some level of improvement. The medical community needs to adopt a disease prevention model, 38 and implementing PA interventions with patients is a prime way to accomplish this task. 39
Footnotes
Acknowledgements
We thank Gaye Christmus for editorial assistance. Steven Blair receives book royalties from Human Kinetics (Champaign, Illinois) for Active Living Every Day.