
Abstract
Over the past few decades, researchers have been developing and refining psychological theories and models to provide solid behavioral frameworks for evidence-based research. Each year new theories and models are created; however, a select few appear to have withstood the test of time and continue to be frequently utilized in present-day research. The objectives of this review are to highlight these psychological theories and models and describe their application to various public health issues and behaviors. Descriptions and example applications of the following theories and models are described in this review: health belief model, theory of reasoned action/planned behavior, social cognitive theory, transtheoretical model, and socioecological model.
‘Change or action theories provide frameworks that guide the development of interventions, translate concepts to messages and strategies, and form a basis for evaluation.’
The application of psychological theories and models to health behavior change research, program development, and policy has become common over the past few decades. Theories and models provide structure for identifying and examining problems, choosing and developing appropriate interventions, and assessing results. These structures enable researchers and program developers to organize key variables related to desired health behavior changes or outcomes. 1 Theories and models are often described as being explanatory theories or change/action theories. Explanatory theories serve as a framework to discover why the problem exists, search for contributing factors, and help determine what can be changed. Change or action theories provide frameworks that guide the development of interventions, translate concepts to messages and strategies, and form a basis for evaluation.1,2
Similarities can be found among the frequently used theories and models; however, their differences set them apart from one other and make them relatively more or less useful as frameworks through which to understand and/or modify different types of health behaviors. A common similarity involves the overlap of key constructs. For example, the construct of self-efficacy, coined by Albert Bandura, refers to confidence in one’s abilities to successfully perform a particular behavior (ie, walk one mile despite barriers such as bad weather or a busy schedule).3,4 Although originally introduced in Bandura’s social cognitive theory (SCT), self-efficacy is also found as a construct within the health belief model (HBM), theory of reasoned action (TRA)/theory of planned behavior (TPB), and transtheoretical model (TTM). 1 Apart from constructs, most theories/models incorporate static individual differences (eg, demographic variables), dynamic individual differences (eg, mood/affect), and interpersonal factors (eg, social support), but the degree to which each of these variables is highlighted varies widely from one theory or model to another.
Comprehensive lists and descriptions of theories and models that have been used to guide health behavior research have been described extensively elsewhere.5,6 We focus here on a select few health behavior change theories commonly seen in the research literature, including the HBM, TRA/TPB, SCT, TTM, and socioecological model (SEM). This article serves as an overview of these theories and models with descriptions of their main components along with examples of their use in the literature. We organized the selected models and theories into three levels of focus: individual, interpersonal, and ecological. As the name suggests, individual level theories/models focus on the individual as the primary driver of change. Thus, their constructs fall within the individual’s realm of control. Interpersonal theories/models focus on the interaction between the individual and his or her relationships with others as the primary drivers of change. Their constructs include a combination of individual and interpersonal factors. Ecological models include components from the individual and interpersonal levels and also extend the focus of change outside of the person into the environment, acknowledging that a variety of factors outside of the individual’s direct control influence his/her behavior change processes and outcomes. As more evidence accumulates that the environment directly and indirectly influences individuals’ behavior, ecological theories/models have become increasingly popular frameworks to use in health behavior research that was previously dominated by individual-based theories/models.
Individual Level
Health Belief Model
The HBM,7-9 depicted in Figure 1, was initially developed in the 1950s in attempt to understand and explain why many individuals were not participating in preventive health services (eg, tuberculosis screening), even when they were offered at no cost. The HBM proposes that the likelihood that individuals will engage in any given health behavior largely depends on their perceptions of the following variables: the severity of the illness(es) it helps prevent, their susceptibility to the illness(es), the benefits of engaging in the behavior, and the barriers to engaging in the behavior. According to the HBM, individuals are more likely to adopt the target health behavior if they believe the potential illness is serious, that they are highly susceptible to it, and that the benefits of engaging in the behavior outweigh the associated barriers. The construct “cues to action,” which are factors that prompt behavior change (eg, media campaigns, physician reminders), was later added to the model to increase its explanatory power (ie, statistical ability to accurately predict health behavior). Other factors, such as demographic characteristics (eg, age, race, ethnicity, gender) and psychosocial variables (eg, peer influence, mood/affect) also exert considerable influence over individuals’ decisions to engage in a specific health behavior according to the HBM. Self-efficacy, described as behavior-specific self-confidence,3,4 was also later added to the HBM in attempt to increase its ability to accurately predict health behavior. 10 These modified or extended versions of the HBM have been used in relatively recent research examining the model’s ability to predict short-term behaviors such as breast self-examinations and early diagnosis among women with a family history of breast cancer, 11 HPV vaccination initiation among adolescent girls in high-risk communities and undergraduate women, as well as A/H1N1 vaccination intention among higher education students.12-14 For example, Norman and Brain 15 applied an extended version of the HBM in their assessment of beliefs about breast cancer and breast self-examination among women with a family history of breast cancer. Results of their study suggested that interventions designed to enhance women’s breast self-examination self-efficacy, among other target behaviors stemming from HBM constructs, may encourage more appropriate and effective breast self-examination. 15
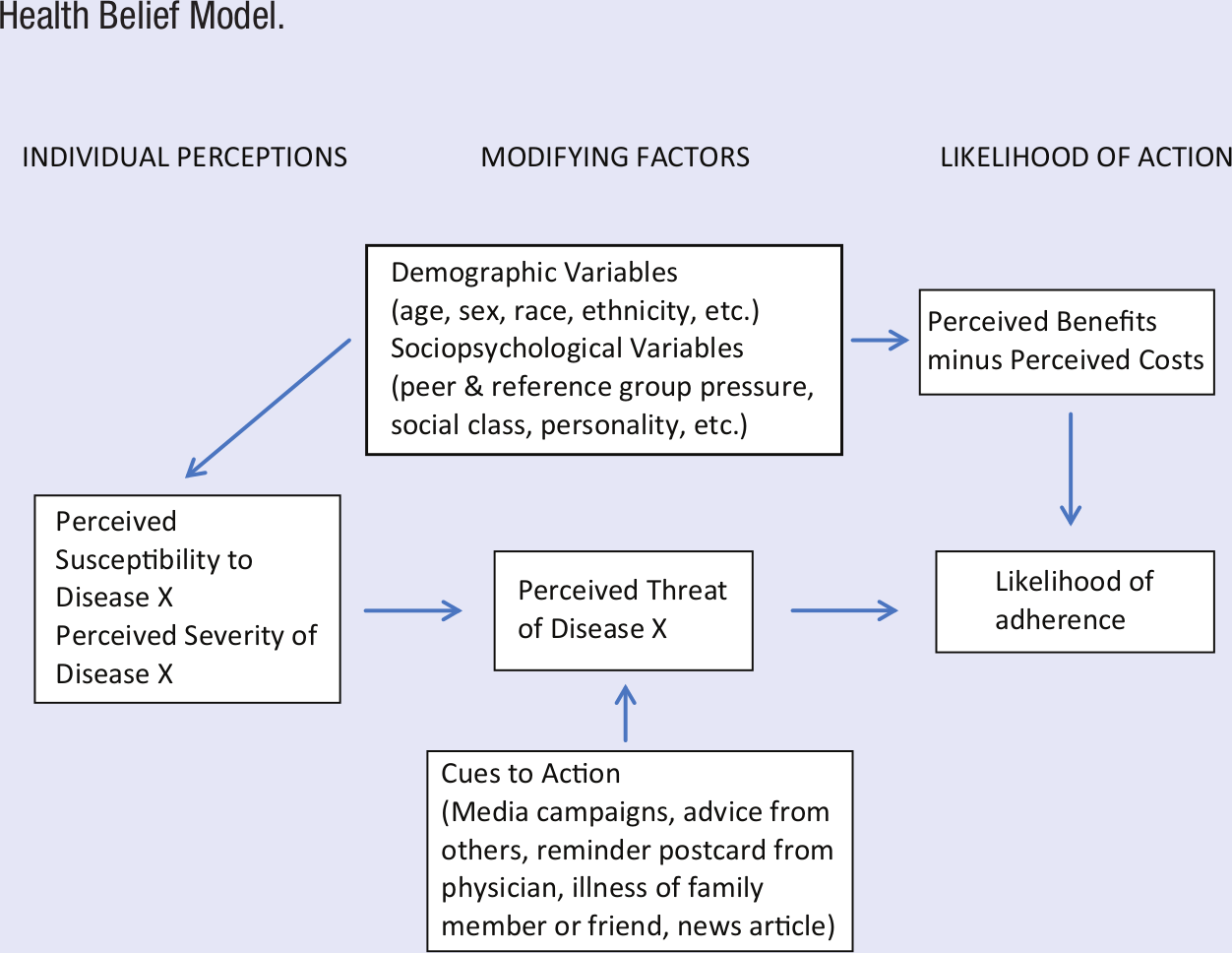
Health Belief Model.
The HBM has since been applied to longer term health behaviors and habits such as smoking cessation, contraceptive use, exercise, and dieting with some success.16-19 Hill et al 16 measured HBM constructs related to exercise behavior among older adults prior to and 6 months after discharge from the hospital. Results supported the utility of HBM constructs in the prediction of participants’ exercise behavior 6 months after discharge. 16
However, the HBM has received significant criticism and has not held up to rigorous scientific examination in longer term contexts. Specifically, a recent meta-analysis of studies using HBM constructs to longitudinally predict various health behaviors concluded that this model may not be particularly useful because 2 of its primary constructs (perceived severity and perceived susceptibility) only weakly predict long-term behavioral outcomes. 20
Although the HBM has been one of the most used models in health behavior research, 21 concerns about the model remain. For example, the relationships between the model’s constructs are not clearly delineated and measurements of certain constructs, such as cues to action, are not standardized.20,22 Moreover, whereas recent research supports the use of HBM as a predictive behavior model,23,24 other models (eg, TTM) have exhibited relatively stronger predictive ability of health behavior. 25 Thus, the HBM is found to be most useful when dealing with single or short-term behaviors (eg, receiving a flu vaccination) 20 and when it is used as an explanatory rather than an action/change model.
Theory of Reasoned Action and Theory of Planned Behavior
The TRA, depicted in Figure 2, was developed by Ajzen and Fishbein26,27 as a derivative of cognitive and social psychology. The TRA posits that individuals’ likelihood of engaging in a particular health behavior can be predicted by the strength of their intentions to engage in that behavior. Intentions represent a combination of one’s own attitudes toward the behavior and their “subjective norms.” According to the TRA, attitudes are formed by individuals’ beliefs about the consequences of the health behavior and the weight they place on those consequences (eg, belief that a regular exercise program will reduce the risk of cardiovascular disease). Likewise, subjective norms are products of individuals’ beliefs about others’ expectations of them regarding the behavior and their motivation to comply with those expectations. For example, if the friends of a teenager believe strongly that text messaging while driving is unsafe, then the teenager might be less likely to text while driving.
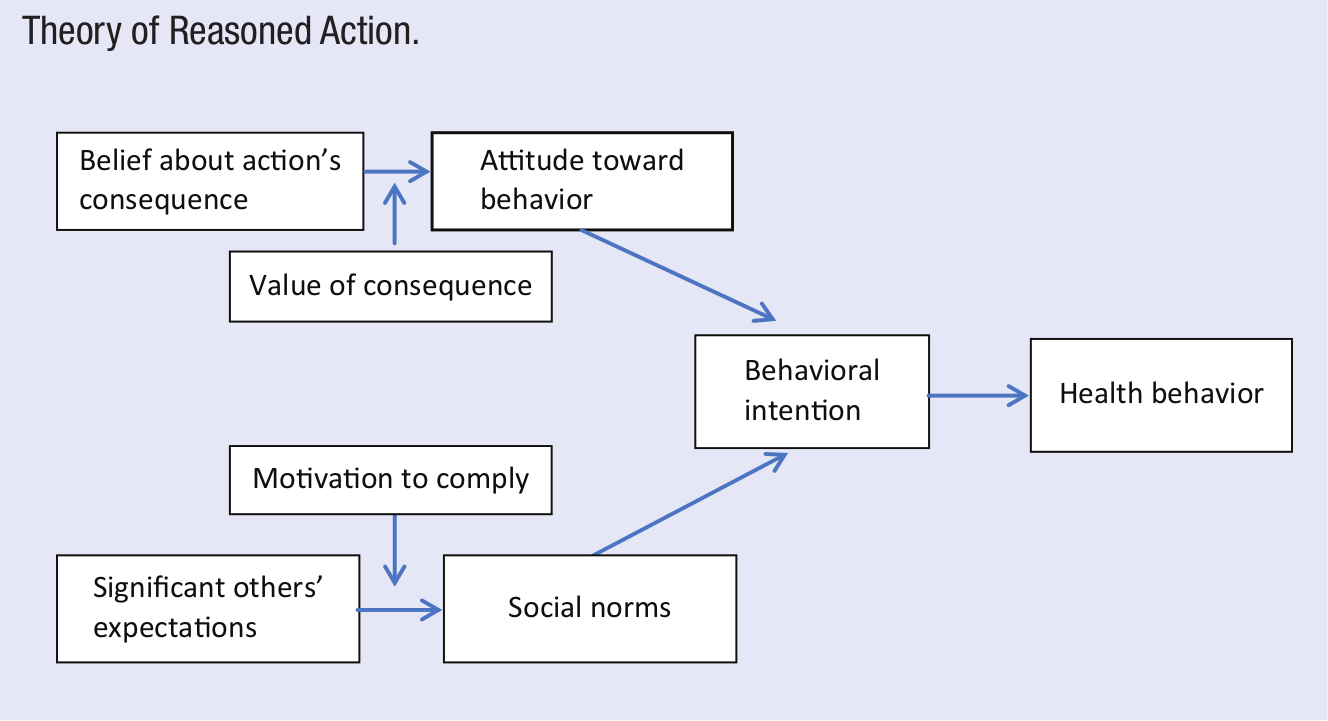
Theory of Reasoned Action.
Research examining the TRA has demonstrated that it is most useful at predicting behaviors under volitional or perceived control 28 ; however, some behaviors are not entirely within an individual’s control. For example, an individual may have the desire to consume a healthy diet, yet because of living in a food desert (ie, limited access to fresh fruits and vegetables) the individual may feel unable to make the desired behavior change. Therefore, Ajzen 29 proposed an extension of the TRA called the theory of planned behavior, or TPB, in an attempt to better predict health behaviors. The TPB incorporates TRA constructs and adds a construct called perceived behavioral control, which is defined as individuals’ perceptions of their ability to perform a given behavior. 29 The TPB’s perceived behavioral control construct is similar to the concept of self-efficacy3,4 and defined in terms of control beliefs (the presence or absence of perceived facilitators and barriers associated with a given behavior) and perceived power (the impact of these facilitators and barriers).
Unlike the HBM, the TRA and TPB clearly delineate the relationships between their individual constructs. As a result, research examining the predictive abilities of these theories has generally supported each of them as a whole. 25 However, a major concern about TRA/TPB is that they do not incorporate any constructs that allow for affective/emotional or psychosocial variability, 30 which has also been a noted concern with the HBM. 31 Some have proposed extended versions of the TPB to more thoroughly account for the components that are missing from the model, including past behavior, self-identity, and additional social influence variables (group norms, family social support, friends’ social support, and social provisions) without much greater success in the results. 32 Furthermore, these theories do not take into account the fact that some behaviors are so habitual that they are not subject to planning or reasoning (eg, years spent driving a car without wearing a seatbelt). 33 In these cases, even the strongest of intentions are not likely powerful enough to overcome the automatic nature of well-established habits. 30
Although the TRA and TPB have received less attention in health behavior research than some of the newer models in recent years, they consistently rank among the most used theories in the field and demonstrate considerable predictive value.34-38 The TRA and/or TPB have been used as guiding frameworks for assessing, understanding, and influencing behavior change in diverse populations with a variety of health behaviors. Some studies have used these theories for preventive measures, such as female condom use among Chinese sex workers 39 and alcohol consumption among early adolescents and young adults.40,41 Others have used the TRA/TPB frameworks for drug-related issues such as HIV-negative methamphetamine users 42 and quality of nurse care for addictive drug users. 43 Zamboanga et al 40 used TRA constructs to explore mediators related to adolescents’ drinking behavior. Specifically, they measured how participants’ perceptions of their peers’ alcohol use influenced their outcome expectancies and valuations (ie, perceptions of expectancies to be good or bad). Results demonstrated that participants who perceived that their peers approve of alcohol use and regularly consume alcohol were more likely to have a positive history of lifetime alcohol use. 40
Furthermore, with the growing prevalence of obesity, researchers have also used these theories to better understand dietary and physical activity behaviors: family meal frequency among adolescents, 44 fruit and vegetable consumption, 45 social ideological influences on food consumption and physical activity, 46 and physical activity maintenance, 47 among others. A recent study by Hunt and Gross 35 tested the validity of TPB in the prediction of exercise adherence in bariatric patients at various time points, ranging from preoperative to more than 1 year postoperative. TPB measures assessed attitudes toward regular exercise, affective attitude (ie, enjoyment of physical activity), subjective norms, and perceived behavioral control. The International Physical Activity Questionnaire was used to assess exercise behavior. Perceived behavioral control, subjective norms, and attitudes toward exercise predicted exercise intention and self-reported behavior; perceived behavioral control was the best predictor. 35
Interpersonal Level
Social Cognitive Theory
Social cognitive theory is one of the most robust health behavior change theories.5,48 It evolved from social learning theory5,49 and originally focused on observational learning, or learning by watching others’ behavior (also called modeling), and the reinforcements (both positive and negative, internal and external) that help determine whether or not one will repeat the behavior. Updated by Bandura and colleagues, the SCT posits that behavior change is influenced by internal individual factors (eg, cognitive, affective, biological), as well as the social and physical environment. The model is reciprocal 1 in that each of these factors affects the others in a continuous, dynamic feedback loop called reciprocal determinism (Figure 3). 5
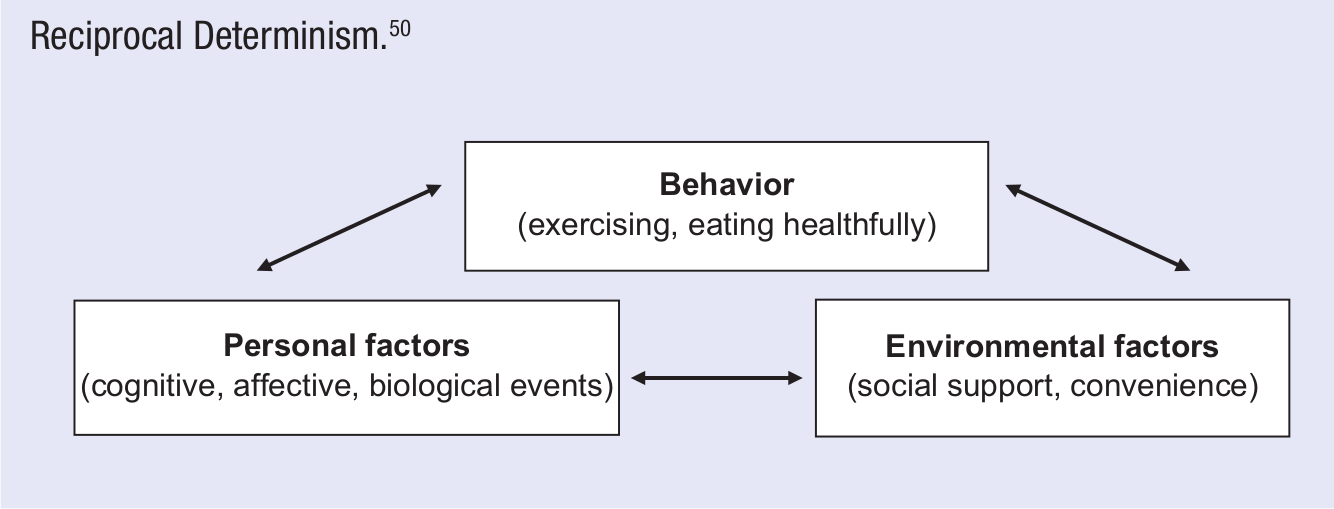
Reciprocal Determinism. 50
Self-efficacy is the main construct of the SCT 51 and, as mentioned previously in this article, a powerful predictor of behavior change that has been incorporated into numerous social and behavior science theories.5,48 Self-efficacy beliefs have been strongly associated with actual performance of a diverse range of health behaviors.52,53 According to Bandura, self-efficacy can be increased through mastery experiences, social modeling, improving physical and emotional states, and verbal persuasion. 48 Mastery experience is gained through succeeding in attainable, yet increasingly challenging health behavior change goals and is considered to have the strongest influence on self-efficacy beliefs.5,48,54 Modeling, as previously discussed, can be accomplished by watching others perform the desired behavior; it is especially effective when relatable peers perform the behavior. Finally, maintaining an optimal level of physiological intensity (ie, excited but not overly anxious) for performing the specific behavior can increase self-efficacy. Optimal intensity can often be accomplished by using relaxation techniques and positive self-talk as well as receiving encouragement from others.5,48,54
Self-regulation strategies are also used to enhance confidence for behavior change and typically begin with self-monitoring, or systematically observing one’s current health behaviors. 48 Data are collected with pedometers, food diaries, smoking logs, or other tools, depending on the health behavior being targeted. These objective data can then be reviewed to determine how specific health behaviors might be improved and to identify incremental and long-term behavior change goals. For example, an Internet-based physical activity intervention using self-monitoring techniques (eg, pedometers and step logs) identified select SCT constructs (perceived environment, outcome expectancies, social support, and enjoyment) as predictors of increased physical activity among participants at 12-month follow-up. 55 Overlapping to a degree with the concept of mastery experience, self-regulation may also include establishing rewards for individuals meeting behavior change goals and enlisting social support from family and friends for performing target behaviors. 48
Another important determinant of behavior according to the SCT is outcome expectancies. 5 This construct, defined as the influence that the outcomes anticipated from a health behavior exert on one’s willingness to perform this behavior, makes intuitive sense and has been supported in numerous research studies. 56 SCT posits that a health behavior is more likely to be performed if positive outcome expectancies are present, whereas negative outcome expectancies reduce the likelihood of the health behavior. For example, individuals will be much more inclined to run a mile if they anticipate that doing so will energize them rather than cause them to feel sore. The relative value of the anticipated outcome also plays an important role in this decision-making process. For example, an individual may view a positive anticipated outcome of smoking a cigarette (feeling more relaxed) as less important than a negative anticipated outcome (smelling like smoke) and thus decide accordingly to forgo the cigarette.
Social cognitive theory offers a comprehensive model of the behavior change process. Some critics suggest that this model is overly broad and has not been tested as a whole in the way other theories are routinely examined. 48 Rather, studies have shown that specific SCT concepts (eg, self-efficacy) are associated with behaviors, but such research does not confirm the entire theory. Nevertheless, the SCT provides a strong foundation for health promotion research and practice and has been successfully applied to a variety of health behaviors (eg, cardiovascular disease,57-61 cancer screening, 62 tobacco use,63-68 alcohol use,49,69-71 diet,72,73 obesity,74-76 physical activity,56,72,73,77-79 diabetes prevention, 80 condom use,81,82); in a wide range of ages (eg, children,73,83-85 teens, 70 college students, 86 elderly 78 ); in underserved populations (eg, African Americans, 64 Latinas,74,80 low-income individuals73,74); and in several different countries (mostly in the United States, but also in China, 81 Sweden, 73 the United Kingdom, 87 and Australia 78 ). For example, a notable Web-based intervention used social cognitive components (social support, self-efficacy, outcome expectations, and self-regulation) to gain a better understanding of the demographic, behavioral, and psychosocial influences of participants involved in an online intervention addressing nutrition and physical activity. 88 Results revealed that participants’ high self-efficacy and outcome expectancy levels did not translate into health behavior change and self-regulatory behaviors, seemingly due to their simultaneous low levels of perceived social support. They concluded that although high self-efficacy may be associated with healthier lifestyles, low levels of social support may serve as a barrier to behavior change that is difficult to overcome. 88
Transtheoretical Model
The TTM is an integrative model of behavior change developed from many different psychological theories, such as SCT 50 and learning theory.49,89 DiClemente et al 90 first described this model after noting that people vary in terms of motivational readiness to quit smoking and move through specific stages of motivational readiness along the path to behavior change. 91 The 5 stages of change that form the core of the TTM are
Precontemplation, in which change is not being considered
Contemplation, in which change is being considered
Preparation, in which an individual takes small steps toward change
Action, in which the health habit has been recently adopted
Maintenance, in which the change has been sustained for ≥6 months
This model is considered cyclical, accounting for people’s tendency to move back and forth through these stages of change. Individuals may lose resolve and abandon new behavior patterns, feel guilty, lose confidence, and revert to their previous routines, with probable recycling through the earlier stages of precontemplation or contemplation. For example, an individual may adopt a regular exercise routine and then regress back to the precontemplation stage after becoming severely ill. Thus, numerous cycles through the stages often happen before an adopted health behavior becomes a habit.92,93
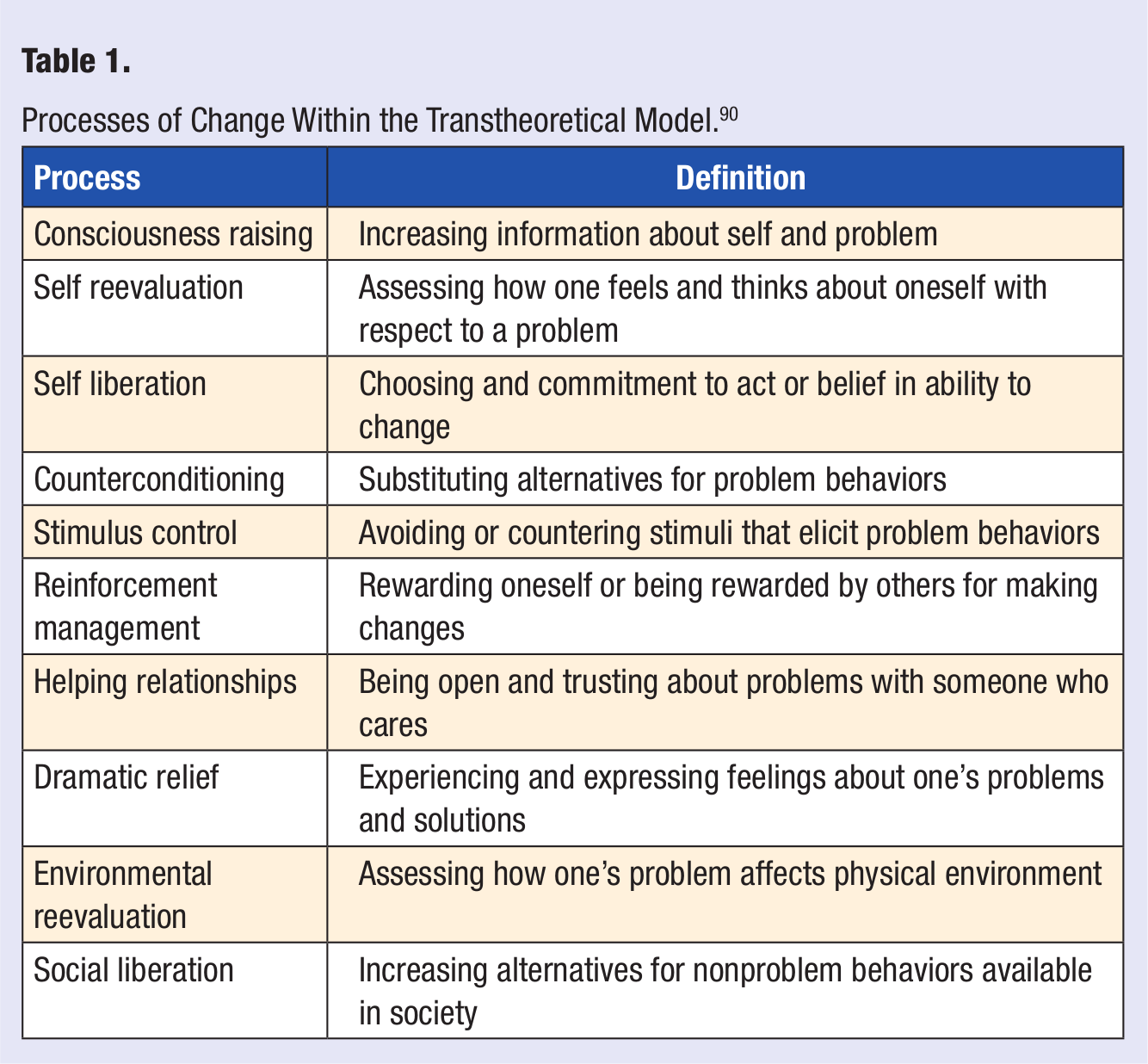
The cognitive and behavioral strategies and techniques that people use to advance through these stages of change are described as processes of change (see Table 1). The TTM posits that people use different processes of change at different stages in the change process and are likely to benefit from interventions developed specifically for their level of motivational readiness and most relevant to their current information needs.5,93 For example, to help move individuals from precontemplation to contemplation, processes such as consciousness raising and dramatic relief should be attempted, whereas people in the action stage are more likely to find contingency management, counter conditioning, and stimulus control helpful. 92
Processes of Change Within the Transtheoretical Model. 90
Theoretical constructs, such as self-efficacy and decisional balance, also play important roles in the adoption and maintenance of health behaviors according to the TTM.5,92,93 The decisional balance construct comes from Janis and Mann’s decision-making theory 94 and involves weighing the perceived advantages and disadvantages of behavior change when deciding whether to adopt a new health behavior. Table 2 lists examples of perceived benefits (the “pros”) and perceived costs (the “cons”) of physical activity. Subtracting total standardized cons scores from total standardized pros scores derives a standardized “decisional balance” score. 95 Decisional balance has been shown to vary as a function of stages.91,95,96 Early stages (precontemplation and contemplation) are associated with higher ratings of disadvantages (cons) and lower ratings of advantages (pros) of change, whereas later stages (action and maintenance) are associated with lower ratings of disadvantages (cons) and higher ratings of advantages (pros) of change. 92
Pros (Advantages) and Cons (Disadvantages) of Increasing Exercise Behavior. 95
Although the TTM originated in the addictions research field, it has since been applied to numerous health behaviors (eg, fruit and vegetable consumption,97,98 weight control, 99 eating disorders, 100 alcohol and drug use, 101 condom and oral contraceptive use,102,103 sunscreen use, 104 medical compliance, 105 cervical cancer and mammography screening,106,107 cardiovascular risk reduction, 108 stress management, 109 intimate partner violence,110,111 and exercise,112-115); in diverse populations (eg, college students, 116 African American adolescents,97,98,117 patients with severe mental illness, 118 tuberculosis, 119 HIV, 120 and multiple sclerosis 105 ); and in many countries (eg, Australia, 72 Mexico, 121 Taiwan, 107 Nepal, 120 and Malaysia 119 ).
Papandonatos et al 114 assessed the TTM constructs self-efficacy, decisional balance, and processes of change as mediators of change in the context of a motivationally tailored physical activity promotion intervention for sedentary adults. Results revealed that processes of change and self-efficacy, but not decisional balance, predicted increases in physical activity. 114 Gillespie and Lenz 108 used the TTM to design a health-related intervention tool for a cardiovascular risk reduction program, which provides a patient-centered plan related to several behaviors (eg, diet, exercise, sleep success, etc). Patients are given a “readiness to change” questionnaire to determine their baseline stage of change and a “confidence to change” questionnaire to evaluate their change-related self-confidence. Using the results of these assessments, practitioners are able to tailor the lifestyle medication program by identifying key target behaviors (eg, exercise) and setting achievable goals specific to the individual.
Despite the TTM’s support, several criticisms of this model have been raised.122,123 For example, the complexity of health behaviors is an issue when considering stage-based behavior change theories. Staging algorithms typically ask about physical activity or diet in general, but motivational readiness for change may vary for subcategories not fully captured by these algorithms (eg, interested in walking and vegetable consumption but not strength training or reducing fat intake). The TTM also focuses on stage progression as a significant outcome, but this is not always associated with actual behavior change.124,125 Nevertheless, the TTM has been a highly influential theoretical framework composed of a number of useful organizing constructs that have been shown to be meaningfully related in empirical data and psychometric studies.
Ecological Level
Socioecological Model
In more recent years, psychological theories and models have increasingly incorporated the broader contexts that affect health behaviors, recognizing that these external factors are often as influential as internal factors. Socioecological models, or SEMs,126-128 are based on 4 fundamental principles that are critical to understanding their application to health behavior change: (a) the environmental and personal factors that influence health behavior dynamically interact with each other; (b) environments are multidimensional and complex; (c) people are multidimensional and complex, and intervention designs should consider both the individual and the groups with which the individual is affiliated; and (d) people–environment interactions exert multiple levels of influence, such that individuals often modify their settings, and settings influence individuals. The socioecological framework suggests that both person-focused and environment-focused strategies can be applied to health behavior change. 127 For example, person-focused strategies may include preventive screening programs, individual counseling, or participation in lifestyle interventions. Environmental strategies include both geographic (eg, mixed use communities) and sociocultural aspects (eg, integrating target health behaviors into organizational structures/cultures).
The SEM has recently grown in popularity, particularly in the public health realm. The SEM differs from more traditional psychological models in that it explicitly incorporates not only the individual’s immediate external influences (eg, interpersonal relationships) but also more peripheral factors (eg, community, environment). Furthermore, rather than predicting a specific order or direction in which influences exert themselves, the SEM depicts the individual in the center of increasingly broader circles of influence, which interact with one another in an ongoing process (see Figure 4). 126

Socioecological Model. 126
The SEM has been applied in assessment and intervention research on a variety of health behaviors and/or in diverse populations.129-131 A noteworthy approach by Donenberg et al 131 examined the effects of multiple influences (peer, family, partner, and mental health) on sexual behavior among children attending therapeutic day schools (ie, schools that provide health risk education and address mental health issues). Results of self-reported surveys revealed that sexual behaviors were predicted by peer influence (which was also reflective of family dysfunction) and conduct problems among both males and females. 131 This example demonstrates how examining multiple levels of influence within the SEM can increase our level of understanding of factors that may influence health risks.
Socioecological model–framed studies include chronic diseases (eg, obesity132,133 and diabetes self-management 134 ), dietary and exercise behaviors,135-137 physical activity assessment in various populations,137-139 health care access (eg, access and use of oral health services 140 ), and interventions conducted through organizations (eg, church-based health promotion interventions 141 ) and within communities (eg, community-based participatory research 142 ), among others. One study examined the social ecological influences (social, environmental, and behavioral) of oral health service access and use among low-income Latino children. 140 Face-to-face interviews of Latino mothers regarding their children’s dental health revealed that (a) initial dental care was affected by the mother’s beliefs regarding the importance and benefits of preventive oral health, (b) household income and availability of oral health services were associated with planned dental visits, and (c) regular dental visits were more likely if the mother believed they were necessary and if she reported good communication with the dental provider. 140
As with all of the aforementioned theories and models, some challenges arise in the application of the SEM to health behavior change interventions. Because the model is exceptionally comprehensive, its application is inherently complex. For example, addressing the SEM’s multiple levels of influence, including regional (eg, neighborhoods), structural (eg, physical environment), and institutional (eg, government, worksite, family) factors, on health behaviors is challenging due in large part to limitations on control over these external variables. Also, additional research is required to help determine which of the model’s multiple components are critical in the behavior change process. Despite its complexity, the SEM appears to be a promising model for an increasingly transdisciplinary scientific community.
Summary
In this article, we summarized only a few of the numerous psychological theories and models that guide health behavior change interventions. We chose to focus on some of the most frequently used models and theories in the literature as well as to represent the range of general categories by which they are organized (ie, individual, interpersonal, ecological). Over the past few decades, the fields of behavioral medicine, public health, and medicine (among others) have been gradually shifting from a sole focus on the individual to a progressively greater focus on the local and, to a growing extent, global environment in which the individual resides.1,126 Although this shift recognizes and better accounts for the increasingly globalized world that undoubtedly influences individuals’ behavior more than ever before, these new ecological theories and models are quite complex and somewhat generic.126-128 Their numerous and relatively broadly defined variables are often difficult to measure, rendering these models as a whole difficult to assess. However, they relieve individuals of at least some of the overwhelming amount of personal responsibility placed on them by the individual and, to a somewhat lesser but still considerable degree, interpersonal theories and models, which explicitly or implicitly assert that individuals should engage in target health behaviors regardless of the external barriers they may face. Moreover, the health problems and challenges for which health behavior change interventions are designed have also shifted from primarily acute and/or short-term illnesses (eg, deadly viruses and infections) to predominantly chronic diseases (eg, cardiovascular disease and diabetes). As mentioned previously in the article, one-time or short-term problems appear to be adequately addressed by the individual-focused theories and models (HBM, TRA/TPB), whereas interventions for longer term problems are often more appropriately designed using interpersonal (and presumably ecological) frameworks (SCT, TTM, SEM).
Many other theories not included in this article also incorporate key concepts that help explain and predict health behaviors. Perhaps the 2 biggest challenges facing the various disciplines involved in health behavior change research are (a) to match specific goal health behaviors with the theories and models that incorporate the most relevant and appropriate constructs to design and implement effective interventions and (b) to systematically incorporate and account for the wide range of ecological factors that clearly influence health behavior to an increasingly greater extent in the modern, global world.
Footnotes
Acknowledgements
We would like to acknowledge Emma Claire Jones for her assistance with the extensive list of references for this article.