
Abstract
Objectives:
Little is known about how children’s health might be affected by parents’ participation in commercial weight loss programs. Given that more than 3.2 million people subscribe to just one commercial weight loss program, Weight Watchers, any secondary effects on children’s weight-related health behaviors (e.g. dietary behaviors, physical activity, and sedentary time) and body mass index from parent participation in commercial weight loss programs may have significant public health implications. This study examined the feasibility of conducting a study to assess such effects. Methods for recruitment and retention, and perceived acceptability and satisfaction among participants in small-scale preliminary study, were evaluated. Changes in body mass index and health behaviors among the parent–child dyads were also measured to test whether a larger-scale study would be warranted.
Methods:
This was an 8-week, pre–post observational feasibility study involving 20 parent–child dyads where both members had overweight or obesity. Physical and behavioral data were collected at baseline and 8 weeks from both members of the dyads. Parenting data were collected at the same time periods through parents’ self-report. Bivariate correlation was used to quantify the associations in changes for dyad members.
Results:
Feasibility goals for retention and perceived acceptability/satisfaction among participants were met. We reached approximately 80% of our enrollment goal. Parents showed a significant decrease in body mass index of 0.53 points (p < 0.05), while children showed a significant increase in raw body mass index (0.42, p < 0.05) and body mass index percentile (0.59, p < 0.05). However, correlation between changes in parent body mass index and changes in children body mass index percentile was positively correlated (r = 0.24, p = 0.31). A decrease in parent intake of total fat was associated with a decrease in the intake of fat in their children (r = 0.47, p < 0.05).
Conclusion:
Our findings support the viability of a larger-scale follow-up to assess the potential of using parent-only commercial weight loss program as a mechanism for improving health behaviors and body mass index in children with overweight or obesity.
Introduction
Childhood obesity has reached epidemic proportion in the United States. 1 Currently, about one out of five US children aged 6–11 years have obesity (17.5%), 1 putting those children at risk for type 2 diabetes, hypertension, hyperlipidemia, low self-esteem, depression, and/or sleep problems. Clearly, this epidemic has extremely significant public health implications.2–4 Parental role-modeling ranks highly among the factors known to influence obesity rates in children,5–8 and it is particularly consequential during early developmental periods when children are establishing key lifelong health behaviors. 9 For this reason, interventions that target parents’ weight-related health behaviors (e.g. dietary behaviors, levels of physical activity, and sedentary time (ST)) and body mass index (BMI) are considered helpful for enhancing healthy behaviors and reducing obesity in the young children of participants.10,11 A recent systematic review of randomized controlled trials (RCTs) reported that parent-only interventions positively influenced BMI outcomes in participants’ children aged 5–11. 12 Childhood obesity interventions also frequently involve parents and young children together;13,14 however, parent-only interventions may offer some logistical and cost advantages compared to parent–child interventions (e.g. it can be logistically challenging to get children to attend interventions along with their parents),15,16 and research has shown that parent-only and parent–child interventions each have similar effects on child BMI outcomes.10,12 There have been previous parent-only interventions that examine obesity-related outcomes in children as a result of changing some combination of parents’ health behaviors (e.g. dietary behaviors, physical activity) and parenting behaviors (e.g. parenting skills, parenting styles, monitoring, and parental support);17–25 however, to our knowledge, there has been little research examining changes in obesity-related outcomes in children resulting from parent interventions that target health behaviors only. As a step toward closing that gap in the existing literature, this study examines the feasibility of a study to assess children’s weight-related outcomes via interventions where their parents were enrolled in a commercial weight loss program (CWLP). Recruitment and retention methods, and perceived acceptability and satisfaction among participants who participated in a feasibility pilot, were assessed. Specific target goals were as follows: (1) enrolling 30 parent–child dyads during the study period; (2) retaining 80% of the enrolled parent–child dyads through the 8-week follow-up visit; (3) at least 80% of parent participants reporting that the survey questions and data collection processes were reasonable expectations for their children; and (4) at least 80% of parent and child participants reporting that they were satisfied with this study. Finally, weight-related outcomes (changes in BMI and changes in health behaviors) from the CWLP intervention were measured in both parents and their children at baseline and at 8 weeks to evaluate effect size (“the amount of change”) in the CWLP group and whether the changes were associated between dyad members. 26 Secondarily, we also assessed changes in parent/family support for children’s health behaviors and home environment variables, such as frequency of family eating out in a restaurant or eating ready-made fast food, frequency of parent exercising with their child, and frequency in unhealthy/healthy food available at home. We understood that the methodology and sample size of the feasibility test intervention would not have sufficient power to show statistically significant associations, but looked to test methods for a more powerful follow-up study and to assess whether an association in changes among dyad members might provide the grounds for a future investigation. The underlying hypothesis motivating this study was that there would be a positive association between changes in CWLP participants’ health behaviors/BMI and changes in their children’s health behaviors/BMI. We selected Weight Watchers (WW) for our intervention vehicle, as it is one of the most widely available CWLPs in the United States. 27 Furthermore, WW shows a good match with our study protocol that examines a variety of health behaviors because WW has a strong focus on changing overall health behavior changes rather than just changing diet behaviors (e.g. by providing prepared food to enrollees, as is the focus in some other CWLPs). Finally, WW has a track record of providing a highly standardized service to all of their members and WW International, Inc. conducts rigorous oversight of their programs to ensure consistent quality across different meetings throughout the United States. Given that the participants in our study would be attending WW meetings at different meeting sites and with different meeting leaders, those standardizing and quality control procedures would enhance the consistency of the intervention.
The use of pre-existing CWLPs for addressing health behaviors and BMI in children is an important and novel component of the study design. By use of a widely available resource as the intervention delivery vehicle, successful completion of the proposed work may pave the way for developing easily scalable, community-based, family interventions.
Methods
Study overview
This was an 8-week, pre–post observational feasibility study involving 20 parent–child dyads, where the both members of the dyad had overweight or obesity. We collected data from all 20 dyads at baseline and at 8-week follow-up visits. The study followed participants in a CWLP (WW) intervention conducted in Portland, OR, in the United States from January 2016 to April 2017. The Institutional Review Board of Oregon Health & Science University (OHSU) approved the research materials on January 2016. Recruitment started on January 2016. The first dyad was enrolled on February 2016. The recruitment was ongoing throughout the study period with the CWLP intervention starting on an individual basis. The total recruitment period was from January 2016 until March 2017. The last dyad’s baseline visit was at the end of December 2016. All parent–child dyads provided written informed consent/assent.
Theoretical framework
This study was informed by family systems theory (FST).28,29 FST views the family as a unit comprising members who are intensely interconnected—supporting alternatives to approaches which treat family members in isolation from other family members. FST suggests that childhood obesity interventions do not need to involve children directly to be effective, and that interventions that target parents or other family members can also be quite effective. 29 Other previous parent-only interventions30–32 have also referenced this theory.28,29
Social cognitive theory (SCT)33,34 is also relevant to our study. SCT outlines the concept of “observational learning”—where children learn new behaviors through observing role models and through interaction with their environment.33,34 In line with SCT, and in combination with the principles of FST, this study is based on the viewpoint that interventions that lead to positive changes in parents’ health behaviors and positive changes in family health environment will ultimately facilitate healthy behaviors in children.
Recruitment
With support from WW International Inc., we recruited participants primarily at the CWLP meeting locations (e.g. four sites in Portland and two sites in Salem, OR). We gave brief face-to-face presentations at the CWLP weekly meetings once every 8–12 weeks. At each presentation, we distributed recruitment flyers. During the recruitment presentations, we shared a few examples of how parents’ participation in the CWLP might influence their children’s health behaviors (e.g. “When you learn new recipes at the CWLP (WW) meetings, it may make it easier for you to eat healthy and delicious food at home.”) to help parent enrollees to understand the purpose of our study. Potential participants provided contact information (i.e. name, email address, telephone number, availability/best window of time to reach, age of child, and preferred method of contact) on the “sign-up” sheets. Our teams then followed up with the CWLP participants who expressed interest. With assistance from the CWLP territory manager, we circulated a letter to the CWLP staff to help clarify the purpose of this study, study activities, our enrollment goals, and participant eligibility. We asked the CWLP staff to distribute flyers in between meeting times. Potential participants were invited to learn more by calling our toll-free telephone number or emailing us. On a bi-/tri-monthly basis, we re-visited the CWLP meeting locations to interact with their staff and give out thank-you cards and small fruit baskets to express appreciation for recruiting participants. Finally, we advertised our study with an advertisement posted on the OHSU website.
Participants
To be eligible, dyads needed to meet the following inclusion criteria: (1) parents and children both with overweight or obesity (parent BMI ⩾ 25 kg/m2 and child’s BMI percentile ⩾ 85th); (2) children aged 6–12 years; (3) parents and children who were fluent in English (verbal and written); (4) parents who were primary caregivers and were about to enroll in or were currently enrolled in the CWLP; and (5) children who resided with the participating parents at least 5 days per week. Exclusion criteria included the following: (1) major medical conditions that contraindicated energy expenditure or moderate physical activity (e.g. orthopedic or joint problems, uncontrolled exercise–induced asthma, metabolic disorders); (2) use of prescribed weight loss drugs; (3) enrollment in a different or additional weight loss program; and (4) if participants were likely to move out of Oregon state within the next 12 months. We selected children aged 6–12 since (1) obesity often emerges in early childhood and tracks into early adolescence,35,36 and (2) health behaviors in children at these ages are heavily influenced by their parents and/or primary caregivers.37,38 Before age 6, it is very challenging to utilize any self-report questionnaires. 39 The upper age limit of 12 was chosen because after early adolescence the influence of caregivers is reduced (while the influence of others, primarily peers, is increased),40,41 and thus presumably the magnitude of the outcome measure might be lessened. We limited the study to participation in only one CWLP (WW) to minimize the potential for any cofounding effect due to variance across different CWLPs. Originally, exclusion criteria restricted participant’s prior involvement in the CWLP to less than 3–4 prior meetings. This exclusion was later dropped due to its limiting impact on potential participants (and is discussed further in the section “Limitations”).
Participants’ inclusion and exclusion criteria were assessed via self-report by phone or email (i.e. potential parent participants were asked to complete a self-screening questionnaire using a weblink we sent to them). If both parent and child were eligible, an in-person home visit was scheduled. Participants’ BMI inclusion criteria were reconfirmed by our study team during the initial in-person visit. If there was more than one child in the family, we asked the parent, “Please think about the child you spend the most time with …” and that child was the one included in the study. There were no families where both parents participated in the CWLP.
Intervention
All of the parent participants attended weekly in-person CWLP meetings for 8 weeks. The CWLP participants were enrolled in a well-known, CWLP that includes four major components: a food plan, an activity plan, a behavior modification plan, and group support. 42 At the CWLP meetings, participants were given information about weight management and had opportunity to consult with the CWLP staff. In addition, the CWLP participants are provided with access to Online Plus—an online program which allowed them to track their activity and food intake, and gave them access to additional CWLP online resources such as recipes and weight management strategies standard to this CWLP. In this study, we did not keep track of the WW components participants used or the frequency of use. We also did not control which weekly meetings participants attended; however, each CWLP meeting was held by the same designated meeting leader every week, and (as noted above) the specific CWLP used for the intervention, WW International, Inc., conducts meeting quality checks on a regular basis regarding the content conveyed to the participants.
Feasibility measures
The majority of the feasibility data (except for recruitment) were assessed at the end of the 8-week follow-up visit:
Recruitment and retention. Recruitment and retention of parent–child dyads were assessed by collecting data on the number of individuals who showed interest in our study, the number of individuals who became ineligible after screening, the number of potential participants who showed interest but did not respond to our contact for screening, the number of parent–child dyads who completed the baseline visit, and the retention rate through the 8-week follow-up visit.
Acceptability and satisfaction (parents). Participants’ perceived acceptability of and satisfaction with our study was assessed by asking a few questions during a follow-up visit: “Were the expectations of this study reasonable for your child (for example, reasonable in terms of intellectual abilities to answer survey questions? Data collection duration? Other?)?” “How satisfied were you with this study?” “How satisfied was your child with this study?” (from 1 = very dissatisfied to 5 = very satisfied), “What suggestions do you have to help us improve recruitment of participants for future studies?” and “Do you have any other thoughts, feedback, or suggestions for improving our study?”
Weight-related measures
Weight-related (primary and secondary) measures were obtained at participants’ homes twice during the study period (at baseline and at 8-week follow-up visit).
Primary outcome measures (parents and children)
BMI was calculated from the measurements of participants’ height and weight as recorded by our trained study members. Height was measured to the nearest 0.1 cm using a portable stadiometer (ShorrBoards, Weigh and Measure, LLC, Olney, MD, USA); Weight was measured in kilograms to the nearest 0.1 kg using an electronic portable scale (Health O Meter®, Pelstar, LLC, Alsip, IL, USA) with shoes taken off. If the difference between the 1st and 2nd measurements of weight was greater than 0.2 kg, we took additional measurements (sometimes up to 4) until the difference between any two measurements was 0.2 kg or less. Then those two measurements were averaged to determine a final weight. Height and waist circumference were measured using a similar procedure to reconcile for outlier measurements. For parents, BMI (kg/m2) was calculated and categorized into two weight status groups (overweight (⩾25 and <30) and obese (⩾30)). Two BMI measures were used for children: raw BMI score and BMI percentiles (calculated using the US Centers for Disease Control and Prevention sex- and age-specific Excel spreadsheet 43 ). Based on the BMI percentile data, children’s BMI is categorized as overweight (⩾85th and <95th percentile) and obese (⩾95th percentile). 44
Dietary behaviors were assessed by self-report. Parents completed the Block Food Screener (55 items) to briefly describe their fat, sugar, fruit, and vegetable intake. This questionnaire has been validated against the Block 100-item food frequency questionnaire, which has been known to be an accurate tool for measuring dietary intake in adults. 45 Children completed the Block Food Screener (41 items) that assesses children’s dietary intake over the past week, with the assistance of parent or caregiver as needed. 46 The Block Kids Food Screener has been validated: its usage has been highly correlated with actual intake when compared to the results of a 24-h dietary recall among children aged 10–17 years.46,47 It has been used for other studies including children aged 6–10 years, which applies to the current study participants.48–51
Physical activity was measured by ActiGraph Link (ActiGraph, LLC, Fort Walton Beach, FL, USA). 52 Participants were instructed to wear accelerometers during all waking hours except when bathing or swimming, for seven consecutive days. The minimum amount of accelerometer data that was considered acceptable was 3 days with at least 500 min of waking wear time for each of those days.53,54
Age-specific movement intensity thresholds were determined based on Freedson’s energy expenditure prediction equation for children 55 and Trioano’s energy equation for parents. 56 The activity intensity was defined in counts per minute (cpm). We defined ST as activity levels below 100 cpm for both parents and children, excluding periods of non-wear. 57 Non-wear time (i.e. at least 60 consecutive minutes of zero activity) was excluded for both parents and children. Using these definitions, an average proportion of time per day in sedentary and moderate-to-vigorous physical activity (MVPA), out of total time wearing the monitors, was calculated for each participant.
Secondary outcome measures (parents)
See Supplemental file 1 which provides samples of questions utilized in this study:
Parental self-efficacy for supporting children’s healthy behaviors was reported by parents using two scales: (1) self-efficacy for supporting children’s physical activity (four items) and (2) self-efficacy for children’s intake of fruits and vegetables (four items). 58 These measures were selected because they were directly related to our outcome variables of interest. The value of Cronbach’s alpha for those items ranged from 0.80 (physical activity) to 0.84 (fruits and vegetables).
Parent/family support for children’s healthy behaviors was measured using several metrics: (1) participating parental support for physical activity; (2) participating parent exercise together with the participating child; (3) family eating together; and (4) characteristics of how the family’s food was prepared. The first two aspects were assessed using Sallis’ Family Support for Exercise Questionnaire (Cronbach’s alpha = 0.78).59,60 Participating parental support for physical activity was assessed by a summed score of responses to five questions. Separately from this summed score, a response to “… done a physical activity or played sports with this child” was calculated. The last two aspects were assessed using two items of the revised family eating and activity habit questionnaires. 61 Each item was assessed separately to reflect parent/family support in the analysis.
Home environment variables were assessed using the Active Where? Parent-Child Survey I, which measures attributes of home, community, and school environments which have been shown to be correlated to children’s diet, physical activity, and ST.62–64 Only the home environment measures from the survey (i.e. 17 items for assessing the numbers of healthy/unhealthy food available at home; 13 items for assessing the numbers of electronic devices at home; and 14 items for assessing the number of pieces of physical activity equipment available in the child’s home) were included in this study.
Descriptive characteristics (parents)
Parents provided demographic data for themselves and their children (on sex, age, race/ethnicity, parental marital status, parental education level, and household income in the past 12 months). History of weight loss program participation was assessed with three questions (first two at baseline and the last one at the 8-week follow-up visit): (1) “How many WW meetings have you attended in the program in which you’re currently enrolled?” (2) “Prior to participating in WW this time, have you participated in any weight management program in the past such as WW or Jenny Craig?” and (3) “Since we met last time (about 2 months ago), how many WW meetings have you attended?”
Statistical analysis
Participant characteristics at baseline were summarized using means and standard deviations, medians and ranges, or frequency with percentage as appropriate. Change variables from baseline to 8 weeks were calculated for parents’ and children’s BMI, health behaviors, parental self-efficacy, parent/family support for children’s healthy behaviors, and home environment. Due to our sample size, we used the t-distribution to calculate 95% confidence intervals (CIs) for the mean change. t-tests were used to assess significant changes over the 8 weeks. We used Spearman’s rho correlation to quantify the associations between changes in key parent and child outcomes as opposed to Pearson’s correlation, which assumes normal distribution of data as several change variables did not appear to be normally distributed. Exact p-values for Spearman’s rho cannot be calculated with ties, so significance status was verified using bias-corrected and accelerated (BCA) 95% CIs from 2000 bootstrapped replicates.65,66 We used Cohen’s effect size criteria for the correlation coefficient of 0.1 = small, 0.3 = medium, and 0.5 = large to describe effect size. 67 Data cleaning and analyses used SPSS version 24.0 (SPSS, Inc., Chicago, IL, USA) and R version 3.5.1 statistical software. 68
Results
In total, 25 eligible parent–child dyads participated in the baseline visit and 20 parent–child dyads remained and participated in the 8-week follow-up visit. The final analytic sample was 20 parent–child dyads. Out of the 20 parent–child dyads included in the sample, 15 dyads met the accelerometer data inclusion criteria (a minimum of 500 min of waking wear time for at least 3 days) and were included in the physical activity analysis. A sensitivity analysis showed that there were no significant differences between the original sample (n = 25 dyads) and the final sample (n = 20 dyads) with respect to demographics and weight-related health behavior variables at baseline.
Recruitment and retention
Initially, 112 potential participants showed interest in this study. Of that number, 43 potential participants did not respond to our contacts for screening. During the screening process, an additional 43 were excluded due to ineligibility. Of these 43 dyads, 28 were ineligible because the child did not have overweight or obesity. After the screening process, 26 dyads remained eligible. Of that number, one dyad did not respond to our contact to set up a baseline visit. Thus, we were able to recruit and complete the baseline data collection visit with 25 dyads (thus, we reached 83.3% of our enrollment goal of 30 dyads). Out of those 25 parent–child dyads, 20 dyads completed the follow-up visit (retention rate: 80%). Following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, 69 we included a flow diagram describing the overall recruitment and retention process (Figure 1) and the STROBE checklist (Supplemental file 2).

Flow diagram showing recruitment and retention of participants (dyads).
Acceptability and satisfaction
Overall, acceptability and satisfaction with the study was moderate to high: 100% of parent participants reported that the survey questions and the data collection processes were reasonable expectations for their children. In total, 90% of the parents were either very satisfied or satisfied with this study and 85% of the children were either very satisfied or satisfied with this study (children’s satisfaction was measured with respect to the data collection process only). The rest reported “neither satisfied nor dissatisfied.” Participants thought that our recruitment strategies could be improved by providing a referral bonus, recruiting participants via parent–teacher association meetings, or recruiting participants via websites (e.g. WW). Finally, several participants mentioned the difficulty of using activity monitor clips.
Sample characteristics
Baseline demographic characteristics of the study participants (n = 20) are displayed in Table 1. Mothers comprised 90.0% of the parents sampled, and girls comprised 75.0% of the children sampled. The majority of the participants were non-Hispanic White (75.0% for parents and 55.0% for children). The mean age of parents was 42.4 years and the mean age of children was 9.3 years. The majority of parent participants (75%) had a history of participating in a weight loss program in the past (prior to enrollment of this study). During their participation in the study, parents attended an average of 6.80 (95% confidence interval (CI): 6.04, 10.20) meetings in the 8 weeks between the baseline and follow-up. The majority of parent participants (13 out of the 20) used a component specific to the WW CWLP, the Online Plus program, at least once per month.
Participants’ characteristics (parent–child dyads N = 20).

SD: standard deviation; N/A: not applicable.
This information is presented as median (range). The numbers of Weight Watchers’ meetings attended at baseline by quartiles (25%, 50%, and 75%) were 3.5, 7, and 29, respectively. We note the highly skewed distribution of this variable.
Findings of change in BMI
Table 2 provides the baseline and change measures for BMI, health behaviors, parental self-efficacy, parent/family support for children’s healthy behaviors, and home environment from baseline to 8 weeks. Parents showed a significant decrease in the BMI of −0.53 points (p < 0.05), while children showed a significant increase in both raw BMI (0.42, p < 0.05) and BMI percentile (0.59, p < 0.05).
Changes in BMI, health behaviors, parental self-efficacy, parent/family support for children’s healthy behaviors, and home environment, from baseline to 8-week visit (parent–child dyads N = 20).
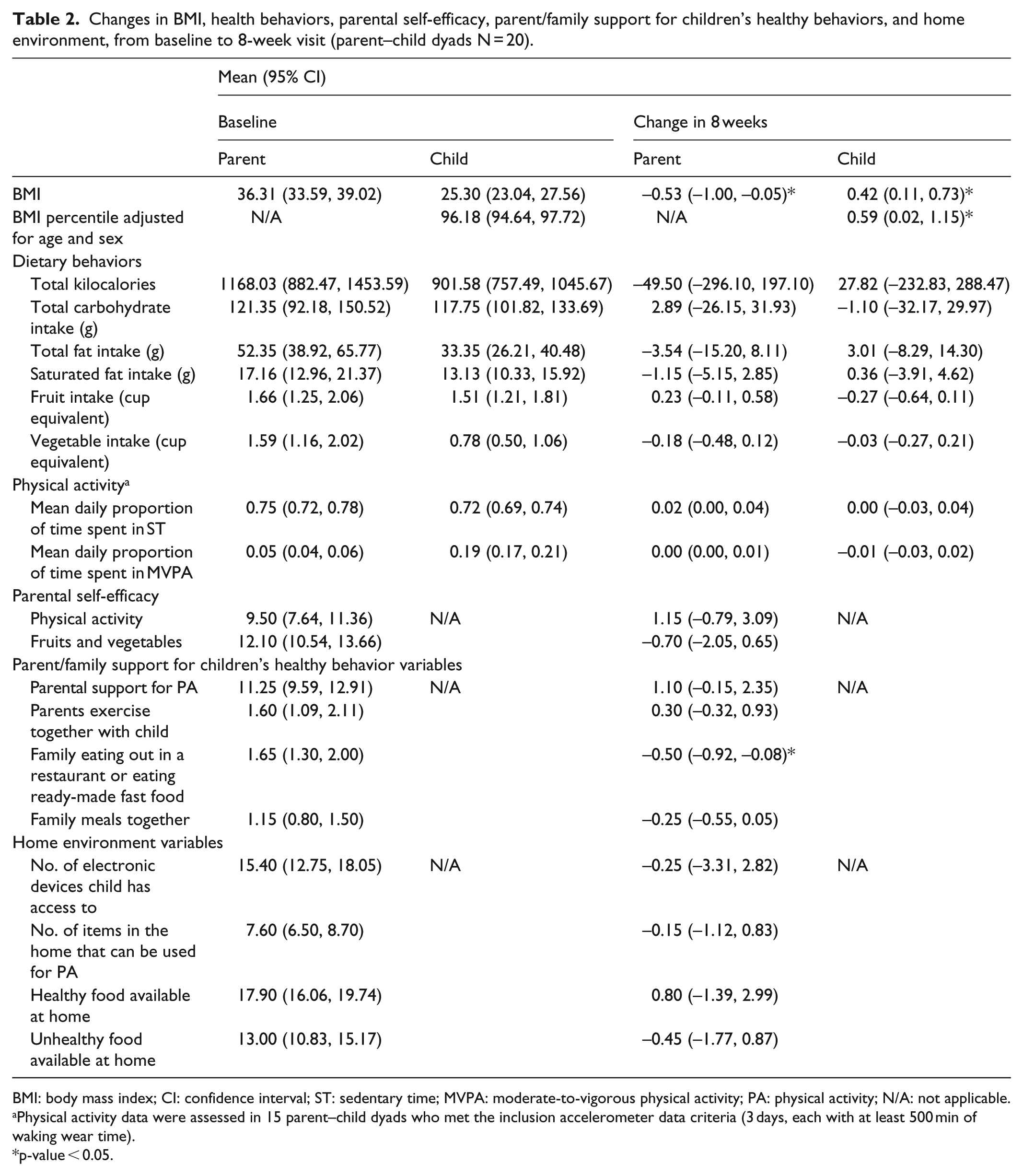
BMI: body mass index; CI: confidence interval; ST: sedentary time; MVPA: moderate-to-vigorous physical activity; PA: physical activity; N/A: not applicable.
Physical activity data were assessed in 15 parent–child dyads who met the inclusion accelerometer data criteria (3 days, each with at least 500 min of waking wear time).
p-value < 0.05.
Findings of change in weight-related health behaviors
The only significant behavior change that was noted with respect to parent/family support for children’s healthy behaviors was in the “frequency of family eating out in a restaurant or eating ready-made fast food.” There was a significant drop in the mean number of times families ate out by approximately 1.65 times per week (p < 0.05).
Findings of correlation in change values in parents and their children
Only one correlation was large enough to be significant. The change in parent’s total fat intake was positively correlated with the change in child’s total fat intake (r = 0.47, p < 0.05), implying that the larger the decrease in parental fat consumption, the larger the decrease in the child’s fat consumption. There were also positive correlations found between the changes in parent’s saturated fat intake and child’s saturated fat intake (r = 0.40) and the changes in total kilocalories parents and children consumed (r = 0.36) demonstrating additional medium effect sizes. Correlations between change in parent and child’s BMI percentiles were also positive although smaller (r = 0.24). Unexpectedly, the changes in parent and child’s fruit and vegetable consumption both showed small, non-significant, negative correlations (r = –0.11 and −0.05, respectively). All other key bivariate correlations between changes in parent and child measures, as well as BCA 95% CIs, are presented in Table 3.
Associations of key BMI and health behavior measures in parent–child dyads with overweight/obesity (parent–child dyads N = 20).

BCA 95% CI: bias-corrected and accelerated 95% confidence interval; P: parents; C: children; BMI: body mass index; ST: sedentary time; MVPA: moderate-to-vigorous physical activity; PA: physical activity.
These numbers were generated from 2000 bootstrapped replicates.
Physical activity data were assessed in the 15 parent–child dyads who met the inclusion accelerometer data criteria (3 days, each with at least 500 min of waking wear time).
p-value < 0.05.
Discussion
Given that we met or came close to meeting all of our feasibility and data collection goals, future studies in this area are warranted. The study met our goals in the areas of retention, perceived acceptability of the requirements of the participants, and perceived satisfaction with the study among the participants. We reached approximately 80% of our enrollment goal. Furthermore, we showed a positive association in change values regarding parents’ changes in health behaviors/BMI and children’s changes in health behaviors/BMI. Our outcomes suggest that “parent-only” interventions where parents are enrolled in a CWLP, such as WW, holds promise for addressing weight-related behavior changes among children with overweight and obesity. A larger-scale, longitudinal RCT is needed to confirm the generalizability of our findings. It should be noted that previous research on the impact on children from “parent-only” intervention, 10 and a recent systematic review of related RCTs, 12 showed that both parents and children’s BMI decreased as a result of “parent-only” interventions. Furthermore, previous research showed that parent–child dyads improved their dietary behaviors and/or physical activity.10,23,70
It is worth noting that we encountered a couple of recruitment challenges: (1) about 40% (43 out of 112) of the parents who initially showed interest in the study did not respond to our contacts for screening, and (2) among the 69 dyads who participated in the screening process, about 40% (28 out of 69) were ineligible because the child did not have overweight or obesity. Regarding the first point, we speculate that sometimes the children of the interested parent were not interested in participating, or that despite initial interest, parents felt they lacked time to participate in our study. These are barriers in recruitment for child obesity studies that have been mentioned by other researchers.71–73 Regarding the second point, we speculate that some parents were not fully aware of the technical definition of overweight and obese.
The relatively large number of dyads that were ruled ineligible because the children of interested parents did not have overweight or obesity suggests an interesting research question closely related to our original research question: Can interventions that enroll parents in CWLPs offer the potential for helping prevent childhood obesity by improving health behaviors and BMI in their children before they develop weight issues? Perhaps, the significant number of families ruled ineligible for our study reflects a preventive effect from parents’ existing enrollment in a CWLP. To address this research question, a longitudinal RCT could be conducted to compare the rates of children’s overweight/obesity in two groups: one with parent/child dyads where parents are enrolled in a CWLP and a control group with dyads where the parents are not enrolled in a CWLP.
Our retention and perceived acceptability and satisfaction among participants are similar to what can be found with other parent-only interventional research that targets obesity in their children.10,20,74 For example, Boutelle et al. 10 reported 76% and 73% retention rates at 3 (mid-intervention) and 6 (post intervention) months, respectively. West et al. 20 reported an 86% retention rate at 12 weeks (post intervention). The satisfaction rate among participants in this feasibility study of 85%–90% was similar to that reported in previous, similar studies.10,20,74 It is quite encouraging that 100% of the parent participants reported that the survey questions and the data collection processes were reasonable expectations for their children. While only 75% of parent–child dyads provided analysis-available data for physical activity, it is quite common that researchers do not receive completed accelerometer data in parent–child dyad studies.74,75
It may be that the unexpected direction of change in some of the key health behaviors and BMI variables, and the discrepancy between the direction of change and the positive associations in change value we found, were influenced by potential outliers or other factors such as small sample size, short study period, or the number of CWLP meetings participants attended prior to joining the study. When we examined the data in detail and excluded two outliers (where the child’s weight increased by 4–5 kg over the 8-week period), the mean change in child BMI percentile decreased from 0.59 (p = 0.01) to 0.27 (p = 0.15), and the correlation between changes in a parent’s BMI with changes in their child’s BMI percentile increased from 0.24 to 0.27. Also, we can speculate counterfactually that parent participation in a CWLP might have slowed down some children’s rate of increase in weight and BMI percentile, even as their weight and BMI values increased. In other words, perhaps without their parents’ participation in this study, children’s weight and BMI might have increased at a faster rate. We underline here that this study was not intended to have enough rigor to confirm the impact of enrolling parents in CWLP, but instead to examine the feasibility of conducting such an analysis. We consider the finding of associations in change value across all of the variables to be a reasonable counterbalance against the unexpected direction of change for some of the variables. A follow-up study with a larger sample and control group would clarify these questions.
In the midst of the unexpected findings, some of our findings regarding direction of change and positive association in change value were in line with what we expected based on our theoretical framework. Specifically, those findings, that is, (1) a significant decrease in the frequency of family eating out in a restaurant or eating ready-made fast food and (2) a positive correlation between the change in parent’s total fat intake and the change in child’s total fat intake—align well with the FST and the SCT. However, these preliminary findings should be validated in future, larger RCT studies.
Limitations
Several limitations of this study need to be taken into consideration. This observational study was relatively short (8 weeks), whereas the causal chain that was the premise for this study might be much longer. We deemed the 8-week period to be sufficient to establish the scope and feasibility of a 1-year follow-up pilot study. The relatively short study period might explain the lack of significant association and the small-to-moderate associations between some of the behavioral/environmental changes initiated by the study protocol and child’s BMI outcomes where past research has indicated larger associations.
Parents and children included in this study were predominantly mothers (90%) and girls (75%), respectively, which could limit the generalizability of the findings to all possible parent–child dyads (e.g. mother–son, father–daughter, and father–son dyads). Other demographic attributes of our sample may limit generalizability as well: our sample had a relatively high proportion of non-Hispanic Whites (~75%) and participants from high-income households (45%).
Study participants were volunteers recruited at CWLP multiple meeting locations potentially resulting in volunteer and self-selection bias as our sample might have been highly self-motivated to lose weight. Furthermore, as mentioned earlier, we recruited participants from multiple locations, so some variations may have occurred in how the content was conveyed to potential participants.
We allowed current CWLP (WW) members to participate in the study due to recruitment challenges we encountered. Our sensitivity analysis showed that the direction of the correlations is consistent between participants who attended only a few CWLP meetings prior to the enrollment in this study (N = 15) and the whole sample (n = 20). Future studies could be designed to test for the effect of prior CWLP participation more robustly.
This study used a single-group design and relied heavily on self-reported data; thus, further RCT research with a control group in community-based settings, and direct observations and/or using additional objective means for data collection would be warranted.
Finally, although the attrition was only 20%, a figure we deemed acceptable, future studies might benefit from follow-up with participants who dropped out, so as to assess how the intervention might be made more acceptable for participants.
Conclusion
Our assessment of recruitment and retention strategies, as well as the perceived acceptability and satisfaction with the study on the part of participants, provides support for the feasibility of building on this study to conduct a larger-scale follow-up study over a longer time frame. If such a larger study resolved some of the discrepancies in the current findings, it could establish the viability of enhancing children’s weight-related health behaviors through interventions that enroll their parents in widely accessible CWLP. Such interventions would potentially have an added benefit of incentivizing parents to enroll in weight loss programs by demonstrating that CWLP offer benefits not only to themselves, but to their children as well.
Supplemental Material
Supplemental_file2_STROBE_checklist_Aug212018 – Supplemental material for Assessing the feasibility of parent participation in a commercial weight loss program to improve child body mass index and weight-related health behaviors
Supplemental material, Supplemental_file2_STROBE_checklist_Aug212018 for Assessing the feasibility of parent participation in a commercial weight loss program to improve child body mass index and weight-related health behaviors by MinKyoung Song, Christopher S Lee, Karen S Lyons, Sydnee Stoyles and Kerri M Winters-Stone in SAGE Open Medicine
Supplemental Material
Supplementary_Material_Aug202018Revised – Supplemental material for Assessing the feasibility of parent participation in a commercial weight loss program to improve child body mass index and weight-related health behaviors
Supplemental material, Supplementary_Material_Aug202018Revised for Assessing the feasibility of parent participation in a commercial weight loss program to improve child body mass index and weight-related health behaviors by MinKyoung Song, Christopher S Lee, Karen S Lyons, Sydnee Stoyles and Kerri M Winters-Stone in SAGE Open Medicine
Footnotes
Acknowledgements
We acknowledge valuable support from Weight Watchers International, Inc. on advertising our study and recruiting participants. We also express our appreciation to John Hicks who oversaw the recruitment process and data collection under the supervision of Dr. Song; and especially to the parents and children who participated in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board of Oregon Health & Science University (OHSU) (STUDY00015075: Healthy Parents, Healthy Families).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an OHSU School of Nursing Innovations Small Grant.
Informed consent/assent
Written informed consent/assent from all study subjects and written parent permission of all the minor subjects were obtained before the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.